

A 75-year-old man underwent surveillance colonoscopy after polypectomy at another institution. Colonoscopy revealed a laterally spreading tumor involving a diverticulum in the ascending colon. He was referred to our hospital for further examination and treatment.
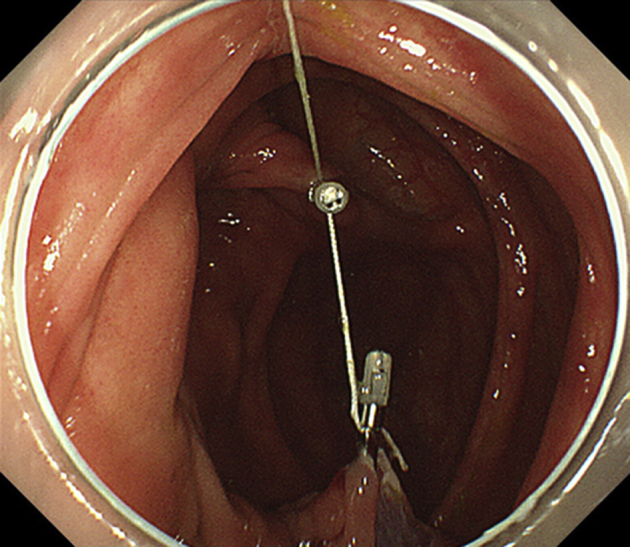
Colonoscopy at our institution revealed a laterally spreading tumor (LST) involving a diverticulum in the posterior wall of the ascending colon (Figure 1, Figure 2). The lesion was a granular-nodular mixed-type LST, and the Japanese Narrow-band Imaging Expert Team classification was type 2A (ie, no evidence of invasion). Therefore, we performed endoscopic resection instead of surgical intervention.
Figure 1.

Colonscopic view showing a laterally spreading tumor in the ascending colon.
Figure 2.

Colonscopic view showing involvement of the polyp with a diverticulum.
The procedure was performed with continuance of aspirin therapy because the patient had a history of abdominal aortic aneurysm, aortic dissection, and myocardial infarction and had undergone coronary-artery bypass graft surgery. Because it was difficult to remove the lesion involving the diverticulum by conventional EMR, we performed traction-assisted colonic endoscopic submucosal dissection using a clip-and-line to facilitate efficient submucosal dissection (Video 1, available online at www.VideoGIE.org).1, 2
After injection of a sufficient amount of hyaluronic acid, a mucosal incision was performed on the diverticular side of the tumor and then on the anal side by use of a FlushKnife BT (DK2618JB15; Fujifilm Medical, Tokyo, Japan). We then grasped the anal side of the tumor with the clip-and-line. However, it was impossible to create a flap because of interference from the anal fold of the colon (Fig. 3).
Figure 3.

During traction-assisted endoscopic submucosal dissection, creating a flap was difficult because of interference from the anal fold of the colon.
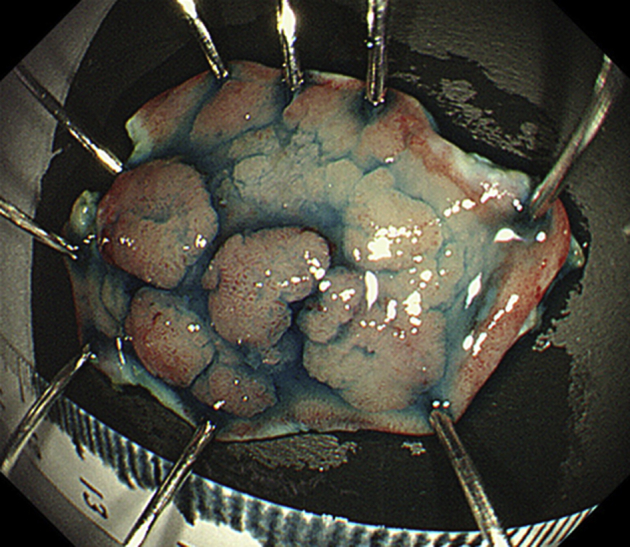
Another clip was added to the bottom of the cecum to create a “pulley” (Fig. 4),3, 4, 5 so that pulling the line with appropriate tension, depending on the situation, enabled good visibility of the submucosal layer (Fig. 5). Considerably better visibility of the submucosal layer was afforded by traction on the line, and the tumor was resected en bloc in 29 minutes (Fig. 6).
Figure 4.
The addition of another clip to the bottom of the cecum to create a “pulley.”
Figure 5.

Achievement of considerably better visibility of the submucosal layer.
Figure 6.
En bloc resection of the tumor in 29 minutes.
A small muscle defect was seen at the location of the diverticulum in the mucosal defect (Figure 7, Figure 8), and the entire mucosal defect was completely closed with clips (Fig. 9). After the line was cut with scissors forceps, the lesion was retrieved through the anus. Prophylactic antibiotics were prescribed for 4 days after the procedure. Oral feeding commenced on day 3 postoperatively, and the patient was discharged on day 6. Pathologic examination of the lesion showed high-grade dysplasia with negative margins.
Figure 7.

Mucosal defect present after endoscopic submucosal dissection.
Figure 8.

Small muscle defect at the location of the diverticulum in the mucosal defect.
Figure 9.

Complete closure of the entire mucosal defect with clips.
Disclosure
All authors disclosed no financial relationships relevant to this publication.
Supplementary data
Pulley traction-assisted colonic endoscopic submucosal dissection affording good visibility of submucosal layer.
References
- 1.Yamasaki Y., Takeuchi Y., Hanaoka N. A novel traction method using an endoclip attached to a nylon string during colonic endoscopic submucosal dissection. Endoscopy. 2015;47:E238–E239. doi: 10.1055/s-0034-1391868. [DOI] [PubMed] [Google Scholar]
- 2.Shichijo S., Yamasaki Y., Takeuchi Y. Case of colonic adenoma involving a diverticulum resected by a traction-assisted endoscopic submucosal dissection technique. Dig Endosc. 2017;29:729–730. doi: 10.1111/den.12904. [DOI] [PubMed] [Google Scholar]
- 3.Li C.H., Chen P.J., Chu H.C. Endoscopic submucosal dissection with the pulley method for early-stage gastric cancer (with video) Gastrointest Endosc. 2011;73:163–167. doi: 10.1016/j.gie.2010.08.041. [DOI] [PubMed] [Google Scholar]
- 4.Oyama T. Counter traction makes endoscopic submucosal dissection easier. Clin Endosc. 2012;45:375–378. doi: 10.5946/ce.2012.45.4.375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rieder E., Makris K.I., Martinec D.V. The suture-pulley method for endolumenal triangulation in endoscopic submucosal dissection. Endoscopy. 2011:E319–E320. doi: 10.1055/s-0030-1256774. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Pulley traction-assisted colonic endoscopic submucosal dissection affording good visibility of submucosal layer.