

Dear Editor,
A 55-year-old man was diagnosed with the end-stage heart failure. He was enrolled in the waitlist of heart transplantation. The patient was scheduled for heart transplantation as the donor heart became available. Anesthesia induction was uneventful. Right radial artery was cannulated for invasive pressure monitoring and pulmonary artery catheter sheath was introduced into the right internal jugular vein. After midline sternotomy and adequate heparinization, aortic and bicaval cannulation was performed to establish cardiopulmonary bypass. The recipient heart was removed, and the donor heart was inserted in its place using bicaval anastomosis technique. During weaning from cardiopulmonary bypass, Swan-Ganz catheter was inserted into the sheath already in the right internal jugular vein. The balloon of the catheter was inflated after inserting 20 cm length of the catheter. As the catheter was further advanced even beyond 40 cm, right ventricular waveform was not observed. Transesophageal echocardiography neither revealed catheter in the right atrium nor in inferior vena cava. Where the catheter was floating could not be ascertained echocardiographically. Azygos and innominate vein palpation by the surgeon did not find malposition of the catheter.
The catheter entered superior vena cava (SVC) cannula instead of right atrium during the insertion process. As the patient was on partial bypass during weaning, drain from SVC cannula was observed to be decreased. Careful examination of the cannula revealed the Swan-Ganz catheter with inflated balloon [Figure 1].
Figure 1.
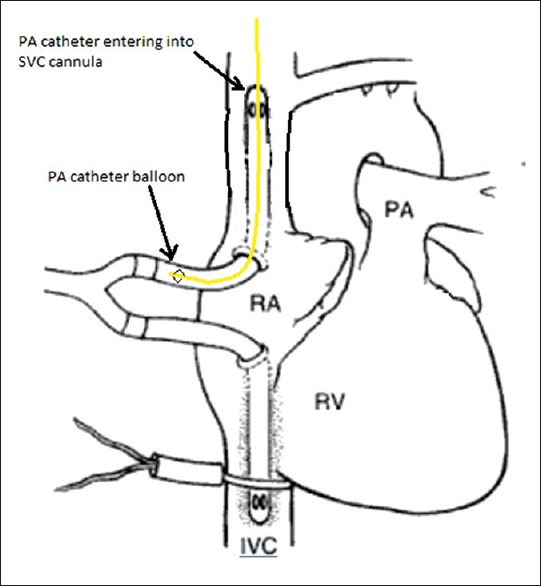
Schematic diagram illustrating passage of pulmonary artery catheter into superior vena cava cannula
Swan-Ganz catheter is a balloon tip, flow directed catheter which travels from SVC, right atrium to right ventricle, and then pulmonary artery. Cardiac output and hemodynamic parameters obtained using the catheter guides the management of the patient. However, it can potentially causes complications during insertion such as arterial puncture and pneumothorax. Apart from arrhythmia and right bundle branch block, misplacement and intracardiac knotting can also occur. Inadvertent insertion of the catheter into carotid artery, pericardium, coronary sinus, hepatic vein, and azygos vein have also been reported.[1,2,3,4]
During cardiac transplantation, it is very essential to monitor pulmonary artery pressure and right ventricular function. Invasive monitoring of pulmonary artery pressure and pulmonary vascular resistance by Swan-Ganz catheter can guide weaning from cardiopulmonary bypass. Transesophageal echocardiographically is able to rule out malposition of the catheter in coronary sinus, intracardiac knotting, in inferior vena cava, or hepatic vein, as was done in the present case. Even azygos and innominate vein placement of the catheter can be suspected by palpating the vein in an open chest. However, it is very unusual and unreported misplacement of Swan-Ganz catheter floating into SVC cannula.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Cardwell ME, Winter B. Pericardial placement of a pulmonary artery catheter. Anaesthesia. 1998;53:290–2. doi: 10.1046/j.1365-2044.1998.00281.x. [DOI] [PubMed] [Google Scholar]
- 2.Baciewicz FA, Nirdlinger MA, Davis JT. An unusual position of a Swan-Ganz catheter. Intensive Care Med. 1987;13:211–2. doi: 10.1007/BF00254707. [DOI] [PubMed] [Google Scholar]
- 3.Davis MS. Hepatic vein obstruction due to Swan-Ganz catheter placement. Chest. 1994;106:603–5. doi: 10.1378/chest.106.2.603. [DOI] [PubMed] [Google Scholar]
- 4.Park SK, Gil NS, Kim A, Ryu HG. A misplaced and entrapped pulmonary artery catheter. Korean J Anesthesiol. 2013;64:380–1. doi: 10.4097/kjae.2013.64.4.380. [DOI] [PMC free article] [PubMed] [Google Scholar]