

Abstract
A 3-month-old-male infant presented with enlargement of head since birth. Clinical and radiological evaluation revealed congenital hydrocephalus, corpus callosum agenesis, prosencephalic cyst, and cranial vault deficiency with supernumerary nostril on the left side. Right ventriculoperitoneal shunt (Chhabra shunt) surgery was performed. The patient did well postoperatively. Parents of the patient have been counseled for repair of supernumerary nostril. Congenital hydrocephalus with corpus callosum agenesis is rare. Furthermore, supernumerary nostril is a very rare anomaly with <40 cases reported in the literature till date. To the best of our knowledge, congenital hydrocephalus, corpus callosum agenesis, prosencephalic cyst, and cranial vault deficiency associated with supernumerary nostril have not been reported till date. We herein briefly review the pertinent literature and describe the embryopathogenesis of this rare association. We propose that this association is a neurocristopathy.
Keywords: Association, congenital hydrocephalus, corpus callosum agenesis, neural crest, prosencephalic cyst, supernumerary nostril
Introduction
Congenital hydrocephalus is not a rare entity. Its management is operative, either by placement of ventriculoperitoneal (VP) shunt or third ventriculostomy.[1] Supernumerary nostril is one of the rarest congenital nasal anomalies. It is characterized by a nose-like structure arising from the dorsum nasi or ala. It has been described by a few reports in the previous literature.[2,3] Hydrocephalus with corpus callosum agenesis is also rare.[4] Herein, we present a 3-month-old-male infant with congenital hydrocephalus, corpus callosum agenesis, prosencephalic cyst, and cranial vault deficiency associated with supernumerary nostril. This association has not been reported till date. Neural crest cells contribute in the development of nasal placode and face, meninges, anterior skull base, and forebrain. We propose that this association is due to aberration in the migration and development of embryonic neural crest cells and should be ascribed as neurocristopathy. We also briefly review the pertinent literature and embryopathogenesis of this rare association.
Case Report
A 3-month-old-male infant weighing 7 Kg presented with enlargement of head since birth. The patient was born full term by elective cesarean section to a 26-year-old mother (Gravida 1, Para 1). There was no history of consanguinity. Mother was hypothyroid, not receiving thyroxin with markedly raised levels (TSH 34.51 mIU/ml), and anemic (Hb 8 g %). Serological tests such as TORCH, Venereal Disease Research Laboratory, HIV, and HBsAg were negative. She had not received iron-folic acid tablets periconceptually. There was no history of infection, teratogen ingestion, and drug abuse or radiation exposure. There was no family history of congenital anomalies. The antenatal diagnosis of hydrocephalus was made at 26 weeks of gestation. The repeat antenatal ultrasonography (USG) performed at 34 weeks showed hydrocephalus with dilated lateral and third ventricles with thinned cerebral cortex and nonvisualization of fourth ventricle. His birth weight was 2745 g and head circumference was 41 cm. Postnatally, he developed physiological jaundice which was managed expectantly and was discharged with an advice for pursuing operative intervention for hydrocephalus. Milestones of the baby were delayed.
Clinical examination revealed enlarged head with nonpulsatile and bulging anterior fontanel, engorged scalp veins, and presence of sunset sign. The head size of the patient was 50 cm and skull vault appeared deficient superiorly and in the occipital region [Figure 1]. An accessory opening arising from the left nostril was present, with an internal diameter measuring 3 mm and external of 7 mm [Figure 2]. No active bleeding or discharge was observed. The ipsilateral normal left nostril (opening) was placed medially, appeared small (slit like) as compared to right nostril [Figure 2]. It was completely separate from the accessory cavity by thick bridge of skin encompassing cartilage. On probing with 6 French fine tubing, the accessory nasal cavity was blind ending (1.5 cm in depth), without any communication to the ipsilateral nasal cavity [Figure 2]. The right nostril was normal. Rest of the nasal cavity structure was normal. There was no columellar deviation.
Figure 1.
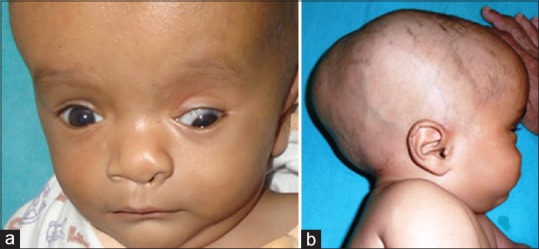
Clinical photographs revealing (a) frontal bossing and sunset sign, (b) enlarged head with bulging anterior fontanel, engorged scalp veins, skull vault appearing deficient superiorly and in the occipital region
Figure 2.

Clinical photographs (a) frontal view showing accessory nostril above the left nostril, (b) worm's-eye view showing accessory nostril above and lateral to the left nostril, (c) probing with 6 French fine tube revealing blind ending accessory nasal cavity (1.5 cm in depth)
Radiological Considerations
USG of the brain suggested severe hydrocephalus with ventricular hemispheric ratio (VHR) of 0.49. The computed tomography (CT) head showed gross hydrocephalus, with dilatation of lateral and third ventricles, agenesis of corpus callosum, prosencephalic cyst (left occipital horn), thin cortical mantle, without significant periventricular ooze, and small fourth ventricle [Figure 3]. Laboratory investigations revealed white blood cell total count of 8000 mm3, hemoglobin 9.3 g/dl, and pack cell volume 29.3%, with normal renal and liver functions.
Figure 3.
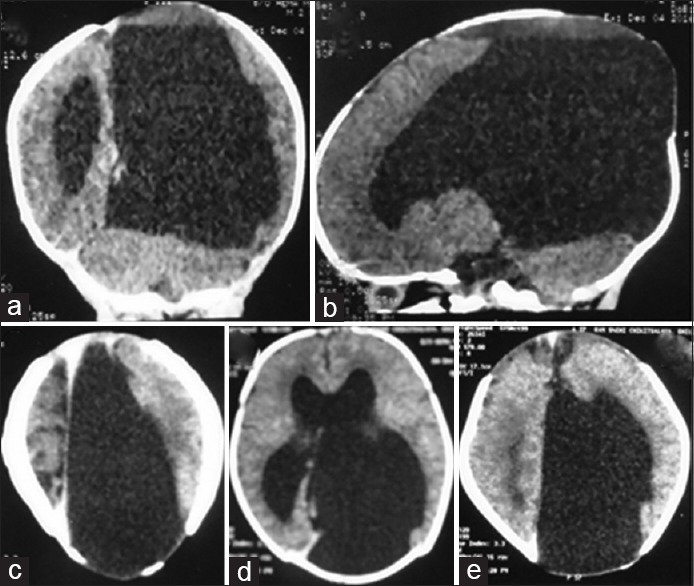
The computed tomography head (a-coronal; b-sagittal; and c,d,e-axial images) showing gross hydrocephalus, dilatation of lateral and third ventricles, agenesis of corpus callosum, thin cortical mantle, without significant periventricular ooze, and small fourth ventricle
Right low pressure VP shunt (Chhabra shunt) surgery was performed owing to the marked sutural diastasis and thinned out cerebral cortex. Endoscopy of the nasal cavity revealed that accessory opening did not communicate with the ipsilateral normal nasal cavity. Parents of the patient have been counseled for repair of supernumerary nostril. Postoperative skull X-ray (anterior-posterior and lateral view) at 6-week follow-up showed shunt positioned well [Figure 4]. Axial and coronal CT head with three-dimensional reconstruction was performed for assessment of hydrocephalus and anatomy of the cranium and nose, which revealed shunt functioning well, decreasing VHR [Figure 5], deficiency of skull vault superiorly, and in the occipital region [Figure 6]. There was the presence of supernumerary nostril on the left side with the presence of septum/cartilage between the two abnormal cavities on left side, and the rest of the nasal cavity was normal [Figure 7]. The child improved clinically and was doing well on follow-up. The patient is being evaluated by a pediatric neurologist to improve developmental and social outcomes.
Figure 4.
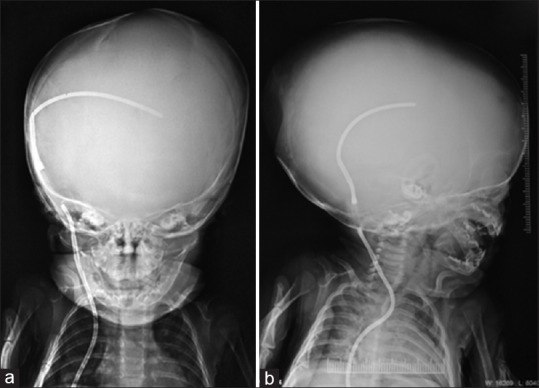
Postoperative Skull X-ray (a-AP and b-lateral views) showing properly placed shunt
Figure 5.
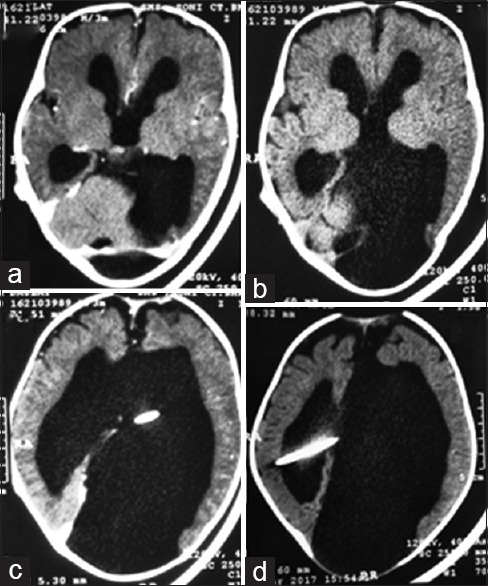
Postoperative computed tomography brain (a and b- axial images) showing gross hydrocephalus, with dilatation of lateral and third ventricles, agenesis of corpus callosum and left occipital horn cyst; (c and d- axial images) VP shunt properly placed in lateral ventricle
Figure 6.
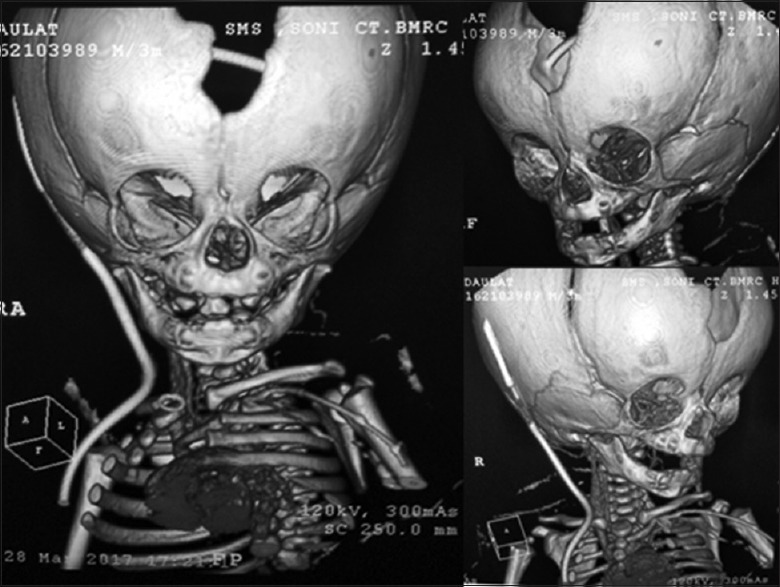
Computed tomography head with three-dimensional reconstruction revealing deficiency of skull vault superiorly and in the occipital region and mild angulation and widening of left nasal bone
Figure 7.
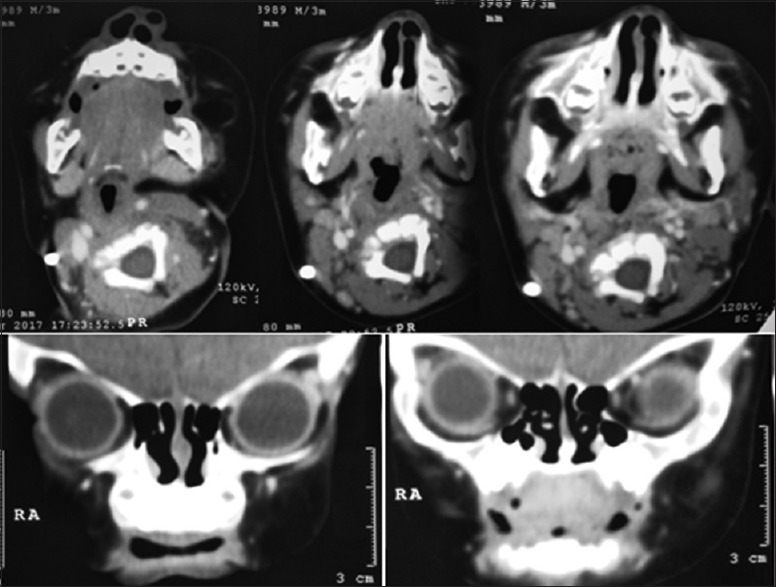
Computed tomography face showing the presence of supernumerary nostril on left side with the presence of septum/cartilage between the two abnormal cavities on left side; normal appearing rest of the nasal cavity
Discussion
Congenital hydrocephalus is not an uncommon condition managed by a pediatric surgery services. Its incidence is 0.2–0.5/1000 live births, whereas its etiology remains obscure.[1] It can be associated with variety of physiological and pathological conditions.[1]
Corpus callosum is the most prominent commissural connection between the cortical hemispheres. It is the largest connective structure in the brain with 190 million axons that transfer information between the two cerebral hemispheres.[4] Corpus callosum agenesis encompasses complete absence as well as partial absence of the corpus callosum. In some percentage of cases, cause is genetic, but in approximately 75% cases, cause is obscure.[4,5] Hydrocephalus with corpus callosum agenesis is rare; various syndromes have been ascribed but none with the presence of supernumerary nostril.[4,5,6]
Supernumerary nostril is also known as triple nostril or accessory nostril. It is a very rare congenital anomaly of duplication resulting from embryological defects with <40 cases reported after its first description by Lindsey in 1906.[2,3] It includes additional nostril with or without accessory cartilage. It can be unilateral (mostly) or bilateral, which may or may not communicate with the normal nasal cavity on the ipsilateral side. The external opening of the accessory nostril may be situated above or at the same level or below the normal nostril. It may be situated lateral or medial to the normal nostril.[2] In most of the cases, the supernumerary nostril was located on the left side and above the normal nostril (as seen our case).[2]
Associated congenital deformities are seen in 45% of the patients, among them craniofacial malformations are the most common.[2,7] Reported anomalies are incomplete facial cleft,[8] ipsilateral congenital cataract and microcornea,[9] congenital double columella,[2] patent ductus arteriosus, central incisor fusion, severe sensorineural deafness,[10] ipsilateral/contralateral naso-ocular cleft, cleft palate and lip, hypoplastic heminose, congenital auricular hypoplasia, esophageal atresia, imperforate anus, frontonasal dysplasia,[2] dermoid cyst at the contralateral nasomaxillary groove,[2] and congenital adrenal hyperplasia with clitoromegaly.[11] Furthermore, anophthalmia of the contralateral eye with multiple hemangiomas of head and chest have been reported.[12] More than half of the cases of supernumerary nostril reported in the literature are from Asian continent, with significant contribution from India and China.[2,3,7,8,9,10,11,12]
The differential diagnoses of supernumerary nostril are proboscis lateralis, basal encephalocele, meningocele, nasal dermoid, nasal glioma, and nasolacrimal duct duplication.[2,3,7,8,9,10,11,12] Among all the differential diagnoses, proboscis lateralis closely resembles the supernumerary nostril. Furthermore, associated brain and cranial vault anomalies are seen in 19% of the patients with proboscis lateralis.[13] Anomalies of forebrain (prosencephalon) such as holoprosencephaly have been reported with proboscis lateralis.[14] In our case, both cranial vault defect and hydrocephalus were present.
The principle of surgery for supernumerary nostril consists of complete removal of soft tissue along with the cartilage between the normal and false nostril. This is followed latter by rhinoplasty for the nostril asymmetry.[3,8,10]
Hydrocephalus, agenesis of the corpus callosum, and cleft lip/palate have been reported by fetal autopsies and molecular analyses in a series.[5] Numerous neurodevelopmental disorders are associated with corpus callosal agenesis.[6,15] A rare case of serious cerebral malformations including corpus callosum aplasia, prosencephalic cyst, internal carotid canal, and facial malformations, associated with cholesteatoma without the presence of supernumerary nostril, has been reported.[6] However, congenital hydrocephalus, corpus callosum agenesis, prosencephalic cyst, and cranial vault deficiency associated with supernumerary nostril have not been reported till date.
Embryology of Facial Development and Brain to Appreciate the Association
The face develops from five facial primordia appearing as prominences around the stomatodaeum (primitive mouth) between 4th and 8th week of gestation. During early 4th week of gestation, the frontonasal process is formed from the developing forebrain, and it appears as downward projection overlapping upper part of stomatodaeum. There is a single median frontonasal process and paired maxillary and mandibular process. These prominences are produced by the cephalic neural crest cells (transient and multipotent progenitors that give rise to several cell types) migrating into the branchial arches during the 4th week of gestation.[16] Surface ectoderm on both sides of the frontonasal process becomes thicker and forms nasal placode. The center of the nasal placode sinks to form a nasal groove and finally forms a nasal pit. Simultaneously, horseshoe-shaped lateral and medial nasal process develops on both sides of the nasal groove. Later, the nasal pit gets deeper and becomes nasal sacs which in turn move into the middle due to merging of medial nasal prominence of both sides along with lateral nasal process and maxillary process. Finally, nasal sacs form nasal cavity and nostrils. The lateral nasal process forms the ala of the nose, and the medial nasal process contributes in forming nasal septum. Maxillary process forms the external opening of the primitive nasal cavity and the upper lip. Thus, nose receives contribution from frontonasal process, lateral and medial nasal process of right and left side, and also maxillary process.[16]
Furthermore, the region of the eye is first seen as an ectodermal thickening which is called as lens placode, appearing on the ventrolateral side of the frontonasal process, lateral and cranial to the nasal placode. The development of eye starts at the angle between lateral nasal process and maxillary process.[16]
Lindsay proposed the theory of dichotomy by atavism or parallel evolution for explaining supernumerary nostril. Erich supported Linsday's theory and postulated that if the accessory nasal pit is located too laterally, the fusion of the lamina is not affected, which leads to the formation of a supernumerary nostril.[17] Reddy and Rao hypothesized that the extra nostril arose as a result of an accessory placode or pit. An accessory nasal placode may be present either above or below the normal nasal placode.[18] Nakamura and Onizuka hypothesized that a localized defect in the lateral nasal process is the cause of accessory nostril.[19] They hypothesized that, during the proliferation of mesenchymal cells in the lateral nasal process, a concavity or fissure appears in this area accidentally which divides it into two segments, resulting in nasal duplication.[19] Sinha et al. speculated that cause is anomaly in the development of the nasal placodes, with a defect in the migration of cells from frontal prominence leading to developmental anomalies of lens and nasal placodes.[9] Kashyap and Khan ascribed the presence of alar cartilage from the accessory nostril to be due to fissuring of lateral nasal process, thereby creating a duplication of segments.[20]
This, “fissuring of the lateral nasal process” during development is the most accepted and cited theory by various authors.[19,20,21] This theory may explain the presence of supernumerary nostril occurring in isolation but fails to explain the anomalies associated which are present in significant (45%) percentage of patients and also presence of hydrocephalus as seen in our case. The presence of associated anomalies in supernumerary nostril cases may be due to early significant embryological interruption.
In addition to the development of face, neural crest cells contribute to the development of meninges, anterior skull base, and forebrain.[5,6,15] The meninges and medial neocortex use a cascade of signals to regulate corpus callosum development.[15] Furthermore, other associated anomalies mentioned in previous reports and also in our case may be explained by the role of neural crest in the formation of craniofacial skeleton, cornea, development of eye, odontoblasts (dentin producing cells of teeth), adrenal gland, cardiac septa, otic placode and inner ear development, cardiac septa formation, connective tissue, blood vessels, and development of brain and meninges.[15,22]
A rare case of quadruple or four nostrils has been reported recently. Three nostrils lined up about what would correspond to the nasal dorsum, whereas the fourth nostril was situated in the right supraciliary area.[23]
We propose that the presence of supernumerary nostril in association with congenital hydrocephalus, corpus callosum agenesis, prosencephalic cyst, and cranial vault deficiency could be due to an aberration in the migration and development of neural crest cells into the branchial arches, brain, and cranial vault. Thus, our case should be ascribed as neurocristopathy. As nasal placodes are produced by the cephalic neural crest cells, there may be an abnormal additional migration of these cells and depending on their destination, additional nasal placode (s) would be produced, resulting in formation of supernumerary nostril. This theory could also explain the presence of supernumerary (quadruple or four nostrils) nostrils in a newborn reported from Mexico.[23]
In conclusion, the presence of congenital hydrocephalus, corpus callosum agenesis, prosencephalic cyst, and cranial vault deficiency associated with supernumerary nostril is extremely rare. Aberration in the migration and development of embryonic neural crest cells may explain this association. Genetic and embryological research would help in understanding and preventing the rare anomalies in future.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We are sincerely thankful to residents and nursing staff of Department of Paediatric Surgery, SMS Medical College, Jaipur, for helping in our endeavor.
References
- 1.Venkataramana NK. Hydrocephalus Indian scenario – A review. J Pediatr Neurosci. 2011;6:S11–22. doi: 10.4103/1817-1745.85704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sah BP, Bhandary S, Pokharel A, Shilpakar SL, Chettri ST, Paudel D. Supernumerary nostril associated with dermoid cyst: A rare case report and review of literature. Am J Med Case Rep. 2014;2:52–4. [Google Scholar]
- 3.Choi BE, Ko SO, Shin HK. Supernumerary nostril: A case report. Maxillofac Plast Reconstr Surg. 2016;38:43. doi: 10.1186/s40902-016-0090-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Paul LK, Brown WS, Adolphs R, Tyszka JM, Richards LJ, Mukherjee P, et al. Agenesis of the corpus callosum: Genetic, developmental and functional aspects of connectivity. Nat Rev Neurosci. 2007;8:287–99. doi: 10.1038/nrn2107. [DOI] [PubMed] [Google Scholar]
- 5.Schoner K, Kohlhase J, Müller AM, Schramm T, Plassmann M, Schmitz R, et al. Hydrocephalus, agenesis of the corpus callosum, and cleft lip/palate represent frequent associations in fetuses with Peters’ plus syndrome and B3GALTL mutations. Fetal PPS phenotypes, expanded by dandy walker cyst and encephalocele. Prenat Diagn. 2013;33:75–80. doi: 10.1002/pd.4012. [DOI] [PubMed] [Google Scholar]
- 6.Berio A, Piazzi A. Serious cerebral malformations (corpus callosum aplasia, prosencephalic cyst), internal carotid canal and facial malformations due to neural crest abnormalities, associated with choleosteatoma. Minerva Pediatr. 2007;59:403–8. [PubMed] [Google Scholar]
- 7.Franco D, Medeiros J, Faveret P, Franco T. Supernumerary nostril: Case report and review of the literature. J Plast Reconstr Aesthet Surg. 2008;61:442–6. doi: 10.1016/j.bjps.2006.04.007. [DOI] [PubMed] [Google Scholar]
- 8.Pan XY, Aung T, Yin GQ. Inverted supernumerary nostril together with tessier 3 incomplete cleft: A Rare congenital deformity case report. Aesthetic Plast Surg. 2015;39:574–7. doi: 10.1007/s00266-015-0501-0. [DOI] [PubMed] [Google Scholar]
- 9.Sinha R, Das S, Sikder B, Ray S, Bit UK. Supernumerary nostril with congenital cataract. Ear Nose Throat J. 2005;84:716–718. 9. [PubMed] [Google Scholar]
- 10.Xu Y, Fan F. Supernumerary nostril together with patent ductus arteriosus, central incisor fusion and severe sensorineural deafness. Int J Pediatr Otorhinolaryngol Extra. 2013;8:59–60. [Google Scholar]
- 11.Ciloglu S, Duran A, Buyukdogan H, Yigit AK. Supernumerary nostril: Congenital adrenal hyperplasia with a rare congenital anomaly. Ann Maxillofac Surg. 2014;4:193–4. doi: 10.4103/2231-0746.147133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Holmes EM. Congenital triple nares. Arch Otolaryngol. 1950;52:70–3. doi: 10.1001/archotol.1950.00700030089009. [DOI] [PubMed] [Google Scholar]
- 13.Belet N, Belet U, Tekat A, Küçüködük U. Proboscis lateralis: Radiological evaluation. Pediatr Radiol. 2002;32:99–101. doi: 10.1007/s00247-001-0602-6. [DOI] [PubMed] [Google Scholar]
- 14.Demyer W, Zeman W, Palmer CG. The face predicts the brain: Diagnostic significance of median facial anomalies for holoprosencephaly (arhinencephaly) Pediatrics. 1964;34:256–63. [PubMed] [Google Scholar]
- 15.Choe Y, Siegenthaler JA, Pleasure SJ. A cascade of morphogenic signaling initiated by the meninges controls corpus callosum formation. Neuron. 2012;73:698–712. doi: 10.1016/j.neuron.2011.11.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sadler TW. Langman's Medical Embryology. 10th ed. Philadelphia, Pa, USA: Lippincott Williams & Wilkins; 2006. pp. 1–226. [Google Scholar]
- 17.ERICH JB. Nasal duplication. Report of case of patient with two noses. Plast Reconstr Surg Transplant Bull. 1962;29:159–66. [PubMed] [Google Scholar]
- 18.Reddy KA, Rao AK. Triple nostrils: A case report and review. Br J Plast Surg. 1987;40:651–2. doi: 10.1016/0007-1226(87)90164-0. [DOI] [PubMed] [Google Scholar]
- 19.Nakamura K, Onizuka T. A case of supernumerary nostril. Plast Reconstr Surg. 1987;80:436–41. doi: 10.1097/00006534-198709000-00018. [DOI] [PubMed] [Google Scholar]
- 20.Kashyap SK, Khan MA. Supernumerary nostril: A case report and review. Int J Morphol. 2009;27:39–41. [Google Scholar]
- 21.Mishra LK, Pradhan SK, Gupta S, Sahoo S. Supernumerary nostril: Report of a rare case and a review of the literature. Plast Surg Case Stud. 2015;1:55–6. [Google Scholar]
- 22.Trainor PA, Melton KR, Manzanares M. Origins and plasticity of neural crest cells and their roles in jaw and craniofacial evolution. Int J Dev Biol. 2003;47:541–53. [PubMed] [Google Scholar]
- 23.Aparicio-Rodríguez JM, Urzaiz E, Rodríguez-Peralta S, San MB, Zepeda-Olivera S, Chatelain-Mercado S. A rare four supernumerary nostril: A female case report at the hospital Para El Niño Poblano, México. J Asian Sci Res. 2013;3:493–505. [Google Scholar]