

Abstract
Background:
Asthma is a chronic and complex lung disease that is not completely understood. It involves airway inflammation, reversible airflow obstruction, and bronchial hyperresponsiveness. The most common symptoms are recurrent wheezing, chest tightness, shortness of breath, and coughing.
Objective:
The Asthma Insights and Management study gathered information on the burden of asthma in the Gulf region (United Arab Emirates, Kuwait, Saudi Arabia) and Russia.
Methods:
This was a cross-sectional, multinational, noninterventional, two-phase study that collected data from patients ages ≥ 12 years, through interviews and a survey questionnaire. Phase 1 consisted of survey questions focused on estimating the asthma prevalence in the community. Phase 2 was designed to assess the level of asthma control, asthma-related perceptions and behaviors, and presentation patterns. Data were summarized by using descriptive analyses.
Results:
Analysis of data of 711 patients revealed that the prevalence of asthma among patients who lived in the community was 7.9% and that 66% subjectively perceived their asthma as being controlled. However, 97% of the patients' asthma were partially controlled or uncontrolled based on the Global initiative for Asthma control classification. Troubling symptoms were daytime coughing (33.3%) and shortness of breath (20.3%). With respect to medications for asthma, 76.2% of the patients reported the use of quick relief medication and 80.8% of maintenance medication during the past 4 weeks. Asthma exacerbation in the past year was reported by 40% of adults and adolescents in the study.
Conclusion:
The results showed that a significant proportion of the patients experienced bothersome symptoms and that many had a lack of knowledge about asthma control and treatment recommendations, which indicated that there is a need for improvements in patient education and asthma care in the Gulf and Russia regions.
Keywords: Activity, asthma, control, exacerbations, function, GINA classification, Kuwait, Middle East, the Gulf, Russia
Asthma is a chronic lung disease that involves airway inflammation, reversible airflow obstruction, and bronchial hyperresponsiveness. The most common symptoms are recurrent wheezing, chest tightness, shortness of breath, and coughing. The development of asthma is complex and not completely understood by scientists.1 A number of risk factors for asthma have been described: (1) a positive family history of asthma, (2) passive smoking (prenatally and postnatally), (3) prematurity (including pulmonary infections, respiratory distress syndrome, and bronchopulmonary dysplasia, (4) early viral respiratory infections (such as respiratory syncytial virus–bronchiolitis), (5) male gender, (6) early lung function abnormalities, and (7) an atopic constitution.2 Asthma most often starts in childhood but can affect people of all ages.
The Global Asthma Report 20143 indicates that 334 million people have asthma and that 14% of children and 8.6% of young adults (18–45 years) experience asthma symptoms. Some studies reported the prevalence of asthma in Saudi Arabia, which presented highly variable results, ranging from 15.5%4 of school children with a diagnosis of asthma to 4.05%5 among the general population. Across the United Arab Emirates, the prevalence of asthma has been estimated to be 8–10%,6 whereas, in Russia, its prevalence among adults is estimated to be 7.4–10.6%,7,8 and, in Kuwait, the prevalence is estimated to be 12.3%.8
Most studies are focused on the prevalence in childhood, and there is limited knowledge on the prevalence of asthma in adults due to a scarcity of population-based surveys in this age group as well as the difficulties in distinguishing asthma from other chronic respiratory conditions. Several articles highlight asthma as frequently underdiagnosed; diagnosed patients are inadequately controlled despite receiving treatment.9–13 The poor control of asthma symptoms affects not only patients' health-related quality of life but also reflects an increased use of health-care resources compared with patients with well-controlled asthma.14–16 Moreover, older patients with asthma incur higher morbidity and mortality than younger patients, which increases the direct medical cost of their management.17–20
Asthma Insights and Management (AIM) surveys have been conducted in different regions worldwide,14,15,21–23 including Europe, the United States, Australia, China, and Hong Kong, where surveys were conducted through telephone interviews, whereas, in Latin America and some Asia Pacific countries, surveys were conducted through face-to-face interviews. The questionnaire objectively measured the patients' perception of asthma control based on the Global Initiative for Asthma (GINA) guidelines,24 which classifies patients' asthma as controlled, partially controlled, or not controlled. The percentage of patients with controlled asthma was highly variable across the countries within the study.
In the Gulf and in Russia, there is a lack of reliable estimates of disease prevalence and understanding of the status of the management of patients with asthma is poor. In the United Arab Emirates, 96% of the patients reported that their asthma was well or completely controlled in a question that assessed subjective perception, but the percentage dropped to 70% when the level of control was assessed by using objective measures (according to the Asthma Control Test score).25,26 A cross-sectional study conducted in adult patients with asthma who attended primary care clinics at three major hospitals in Riyadh, Saudi Arabia, found that, when using the Asthma Control Test, 58.9% of men and 77.0% of women had uncontrolled asthma.27
This study aimed at gathering information on the burden of asthma in the Gulf region (United Arab Emirates, Kuwait, Saudi Arabia) and in Russia. More specifically, the study objectives were (1) to estimate the prevalence of asthma among patients living in the community as reported by the patients, (2) to assess the level of control of asthma patients living in the community as reported by the patients, (3) to document the asthma-related patient perceptions and behaviors, and (4) to assess the asthma presentation patterns as reported by the patients.
METHODS
Study Design
The AIM study is a noninterventional study conducted in the United Arab Emirates, Kuwait, Saudi Arabia, and Russia, as a two-phase population-based survey. This survey had a first phase, which identified patients who self-reported asthma and who were invited to take part in the second phase of the survey. The latter consisted of both demographic data collection and a detailed interview regarding the symptoms and treatment for their asthma and how it impaired their quality of life.
Study Population
The study population consisted of patients ages ≥ 12 years and who lived in the community. The patients must have had a self-reported asthma diagnosis and had been taking asthma medication or experienced an asthma attack or symptoms at the time of or within the previous 12 months of the survey. An initial screening interview was conducted in randomly selected households to estimate the prevalence and to identify patients to be interviewed. Only patients who provided informed consent or provided both assent and representative's consent were considered for interview.
Data Collection
The survey section (phase 1) consisted of a maximum of eight questions focused on the household characteristics and on the identification of those patients diagnosed with asthma. Phase 2 data were collected during a face-to-face interview, which lasted ∼35 minutes, between December 1, 2016, and February 2, 2017, by using the AIM questionnaire, which was available in Arabic and Russian languages. Interviews were designed to assess the burden of asthma (short- and long-term symptoms; functional impact; and health-care utilization, such as health-care provider visits and use of asthma medications), and to assess patients' beliefs about the appropriate use of medications for asthma control. The patients were also asked to assess their (or their child's) productivity on a scale of 0–100% on both typical days and on days when their asthma was at its worst. Sociodemographic data were also collected from the patient, such as gender, age, smoking status, education level, and diagnosis of nasal allergies. Asthma exacerbation was defined as an episode of asthma symptoms more frequent or more severe than normal.
Statistical Analysis
Because the study was exploratory in nature, no formal sample-size estimation was performed. It was expected that 700 patients would be interviewed: 200 patients in the United Arab Emirates, 100 patients in Kuwait, 150 patients in Saudi Arabia, and 250 patients in Russia. All data were analyzed, which comprised all patients screened and interviewed. Descriptive analyses were performed by using count and frequency (n [%]) for categorical variables, mean ± standard deviation (SD), and median (interquartile range) for continuous variables. Before the descriptive analysis, the data were examined for potential skewness and influential outliers, which were handled appropriately as required (e.g. use of non-parametric methods, dropping of outliers, etc). The prevalence of asthma was estimated from the proportion of patients who reported the diagnosis in the sample, with 95% confidence intervals. Descriptive statistics were drawn on observations with non-missing data, and missing data was not replaced with substituted values. Data were presented for the overall subject population by country. All statistical analyses were performed by using SAS 9.1 software or a later version (SAS Institute, Cary, NC).
Ethical Considerations
Eligible patients were included in the study after providing written institutional ethics review boards approved informed consent and assent, if required. This study was also designed, implemented, and reported in accordance with the Guidelines for Good Pharmacoepidemiology Practices of the International Society for Pharmacoepidemiology and with the ethical principles laid down in the Declaration of Helsinki.28 The study was approved by the following institutional ethics review boards: Research Ethics Committee, Prince Sultan Military Medical City, Riyadh, Kingdom of Saudi Arabia, Ministry of Health, Kuwait, Research Ethics Committee, Zayed Military Hospital, Abu Dhabi, United Arab Emirates, and local ethics committee (Or Pharmnadzor), Saint Petersburg, Russia.
RESULTS
Description of the Overall Study Population
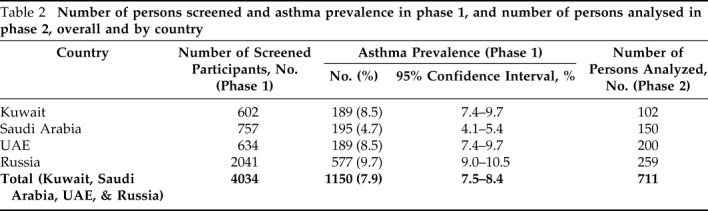
Overall, 4034 persons were screened in phase 1, all countries combined. The study population (phase 2) consisted of 711 eligible patients for whom data were analyzed: 102 eligible patients in Kuwait, 259 in Russia, 150 in Saudi Arabia, and 200 in the United Arab Emirates. Of the 711 patients from all countries, 408 were men (58.3%), and the mean ± SD age was 39 ± 15.6 years. Other information on the sociodemographic characteristics of all the patients is presented in Table 1.
Table 1.
Sociodemographic characteristics of all the patients
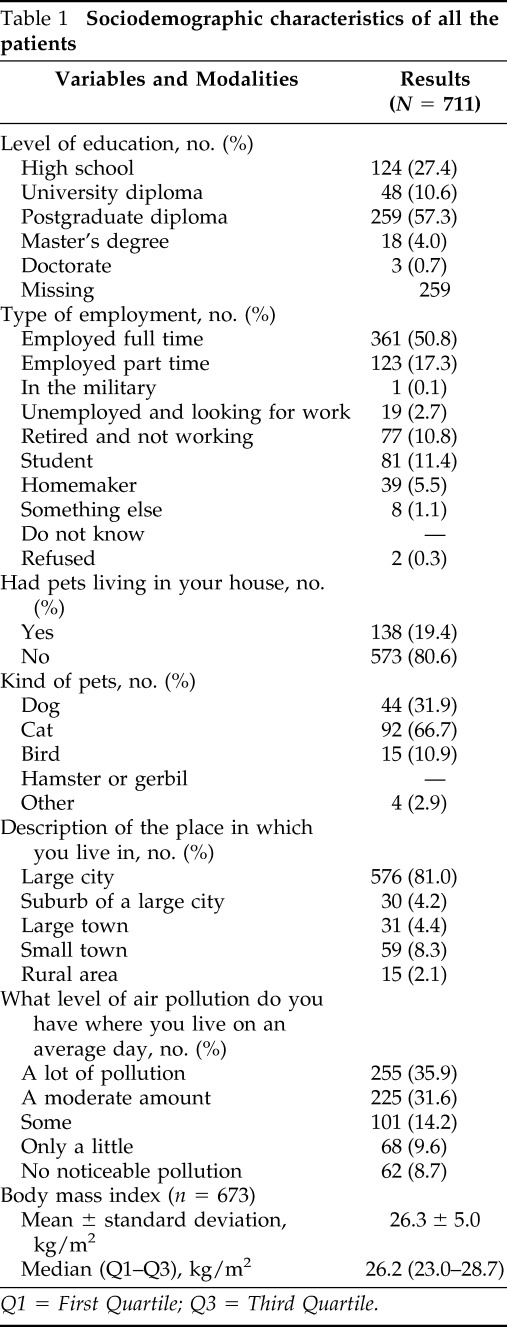
Q1 = First Quartile; Q3 = Third Quartile.
Patient-Reported Prevalence of Asthma Among Patients Who Lived in the Community
The overall patient-reported prevalence of asthma was 7.9%, 95% confidence interval 7.5–8.4%. Asthma prevalence per country is displayed in Table 2.
Table 2.
Number of persons screened and asthma prevalence in phase 1, and number of persons analysed in phase 2, overall and by country
Level of Asthma Control in Patients Who Lived in the Community as Perceived by Patients and Based on GINA Criteria
Almost two-thirds of the 711 patients (66%) from all the countries perceived their asthma as being completely or well controlled (Fig. 1); however, 97% had partially controlled or uncontrolled asthma based on the GINA control classification.24 Over the past 12 months, more than half of the 711 patients (62.6% [n = 445]) had an asthma episode that prevented playing or exercising. In the past 4 weeks, 708 patients experienced asthma symptoms approximately twice per week (median 2 [interquartile range 1–3]), and 499 of 711 (70.2%) reported a cough, wheezing, shortness of breath, or chest tightness during the day. Approximately one-fourth (26.7% [n = 133]) of 499 patients experienced such symptoms at least twice a week, with an average of four times a day (median 2 [interquartile range 2–4]).
Figure 1.

Patients who perceived their asthma as completely or well controlled in the past 4 weeks.
Also, in the past 4 weeks, 385 of 711 patients (54.1%) were awakened by coughing, wheezing, shortness of breath, or chest tightness during the night, and 90 of 385 patients (23.4%) reported these symptoms occurring at night at least twice a month. However, fewer than half of the patients (46% [249/541; 170 with missing data]) had a cough, wheezing, shortness of breath, or chest tightness during exercise, play, or physical exertion in the past 4 weeks, with 72 of 249 (28.9%) having had these symptoms during exercise, play, or physical exertion at least twice a week. More than half of the patients reported that their asthma did not cause them to miss work or school and that the average of missed days was approximately 8 (median 4 [interquartile range 2–7]) in the past year.
Description of Asthma-Related Perceptions and Behavior
Across all the countries, 498 patients (70%) reported daytime symptoms in the past 4 weeks, whereas 384 patients (54%) reported nighttime symptoms and 249 (35%) described symptoms during exercise. Among those, the highest frequencies of daytime symptoms during exercise (either daily or most days) was recorded in Kuwait (36% [n = 37] patients and 20% [n = 21], either daily and most days, respectively). In parallel, Russia had the highest frequency of nighttime symptoms (nightly or most nights), with 68 patients (26%).
The most troubling symptoms were coughing (223 patients [33.3%]) and shortness of breath during the day (136 patients [20.3%]), followed by being awakened at night by coughing (73 patients [10.9%]) and by shortness of breath (69 patients [10.3%]). The least troubling symptoms were coughing up phlegm (61 patients [9.1%]), chest tightness (55 patients [8.2%]), and wheezing or whistling in the chest (53 patients [7.9%]). Asthma's interference in the patients' life, including asthma-related activity limitations in all the countries is summarized in Fig. 2. A majority (62%) indicated that sport and recreation activities were limited, and almost half of the patients (47%) indicated that normal physical exercise was limited.
Figure 2.

The percentage of patients who reported limitation of specific activities (a lot or some) in all countries (N = 711).
All the patients were using prescription medication for quick relief from asthma symptoms: 76.2% used it within the past 4 weeks, and 42.5% used it on a daily basis. The most frequently used medication form was inhalers (72.9% over-the-counter medication; 67.1% prescribed medication), followed by nebulizer (40.4% and 45.9%, over-the-counter medication and prescribed medication, respectively). Further details on the use of quick-relief medication are given in Supplemental Table 1. Of the 711 patients, 574 (80.8%) reported that the most recent use of a prescription medication for long-term maintenance was within the past 4 weeks. More than half of the patients used this medication in the form of an inhaler (59.1%,), followed by a nebulizer (46.%). More details on the use of prescription medication for long-term maintenance are given in Supplemental Table 2.
Description of Asthma Patterns as Reported by Patients
More than half of the patients reported that their asthma was worse outdoors (55.3% [n = 393]), whereas 43 patients (6%) said their asthma was worse indoors. Among different triggers, tobacco smoking was the most commonly reported trigger (53.7% [n = 382]), followed by viruses or cold (43.7% [n = 311]), changes in weather (43.2% [n = 307]), dust (41.8% [n = 297]), chemicals (37.1% [n = 264]), and fumes and odors (36.8% [n = 262]). Perfume (27% [n = 192]), pollution (23.2% [n = 165]), and pollen (18.6% [n = 132]) were also described as triggers that worsened asthma symptoms. Asthma exacerbation in the past year was reported by 40% of adults and adolescents in our study.
DISCUSSION
This cross-sectional and multinational study aimed to gather information on the burden of asthma in the Gulf and Russia regions. The study showed that the patient-reported prevalence of asthma among patients who lived in the community was 7.9%. This was higher compared with a Saudi general population study5 but in line with earlier results from the United Arab Emirates6 and Russia,7,8 and was lower than the reported prevalence in Kuwait.8 Of the 711 patients, 66% perceived their asthma as being completely or well controlled; however, 97% of the patients had just partially controlled or not controlled asthma based on GINA control classification.24 The first finding was in line with global results, which indicated that a median of 67% (range, 27–88%) of patients perceived their asthma as completely and/or well controlled.29 However, globally, a slightly higher proportion, 9% (range, 0–29%), of the patients had well-controlled asthma when using criteria from asthma guidelines.24,29 In the study conducted in Saudi Arabia, however, the proportion of patients that perceived their asthma as uncontrolled was much higher (58.9% of men and 77.0% of women versus 44% in the current study).26
Troubling symptoms were daytime coughing (33.3%) and shortness of breath (20.3%). With respect to medications for asthma, 76.2% of the patients reported the use of quick-relief medication and 80.8% of the patients used maintenance medication during the past 4 weeks. Nearly two of five adults and adolescents with asthma in the Gulf and Russian regions reported asthma exacerbations in the past year, which was consistent with the findings of Asthma Insight and Management in Europe and Canada.30 The fact that patients perceived their asthma as controlled while it actually was not, showed that patients exhibited a lack of knowledge about asthma control. Furthermore, the fact that > 40% of the patients used quick-relief medication on a daily basis, which is contrary to guideline recommendations,24,29 showed a lack of knowledge of treatment recommendations. This was similar to findings in other regions.29
Some study limitations should be borne in mind in the data interpretation of this cross-sectional study. First, data collected were based on self- and/or patient-reported outcomes, which could be limited due to social acceptance of reporting one's symptoms (social desirability bias)31 and recall bias (e.g., patients could be alluding to asthma that occurred in the past yet subsided after a certain age). Social desirability is a phenomenon that restricts the extent to which the study patients will “speak their minds.” It is associated with patients' predisposition to give more socially acceptable answers to a questionnaire and the fact that people do not always “know their minds.”32 In addition, the probability of recall bias cannot be excluded because the patients' self-reported subjective experience of asthma in a past time frame, which could produce distortions in the accuracy or completeness of the retrieved recollections.
CONCLUSION
The results showed that a significant proportion of patients experienced bothersome symptoms and that many had a lack of knowledge about asthma control and treatment recommendations, which indicated a need for improvements in patient education and asthma care.
ACKNOWLEDGMENTS
We thank all persons who participated in the study.
Footnotes
The study was sponsored and funded by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc.
K. Tunceli and E. Urdaneta are employed at Merck & Sharp Dohme Corp. (MSD) and Kaan Tunceli has stock (options) in MSD. The remaining authors have no conflicts to declare pertaining to this article
Supplemental data available at www.IngentaConnect.com
REFERENCES
- 1. Subbarao P, Mandhane PJ, Sears MR. Asthma: epidemiology, etiology and risk factors. CMAJ. 2009; 27:E181–190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Nafti S, Taright S, El Ftouh M, et al. Prevalence of asthma in North Africa: the Asthma Insights and Reality in the Maghreb (AIRMAG) study. Respir Med. 2009; 103(Suppl 2):S2–11. [DOI] [PubMed] [Google Scholar]
- 3. Al Ghobain MO, Al-Hajjaj MS, Al Moamary MS. Asthma prevalence among 16- to 18-year-old adolescents in Saudi Arabia using the ISAAC questionnaire. BMC Public Health. 2012; 12:239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Nahhas M, Bhopal R, Anandan C, Elton R, Sheikh A. Prevalence of allergic disorders among primary school-aged children in Madinah. Saudi Arabia: two-stage cross-sectional survey PLoS One. 2012; 7:e36848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Moradi-Lakeh M, El Bcheraoui C, Daoud F, et al. Prevalence of asthma in Saudi adults: findings from a national household survey, 2013. BMC Pulm Med. 2015; 15:77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Alsowaidi S, Abdulle A, Bernsen R. Prevalence and risk factors of asthma among adolescents and their parents in Al-Ain (United Arab Emirates). Respiration. 2010; 79:105–111. [DOI] [PubMed] [Google Scholar]
- 7. Emelyanov G, Fedoseev G, Sergeeva N, et al. The Prevalence of Asthma and Allergic Rhinitis Among Adults in St. Petersburg, Russia. J Allergy Clin Immunol. 2004;113(2)(Suppl):S321 https://www.jacionline.org/article/S0091-6749(04)00696-7/fulltext Accessed October 3, 2018. [Google Scholar]
- 8. The International Union Against Tuberculosis and Lung Disease. The Global Asthma Report 2011. Paris, France: The International Union Against Tuberculosis and Lung Disease; 2011. [Google Scholar]
- 9. Gonzalez-Garcia M, Caballero A, Jaramillo C, Maldonado D, Torres-Duque CA. Prevalence, risk factors and underdiagnosis of asthma and wheezing in adults 40 years and older: A population-based study. J Asthma. 2015; 52:823–830. [DOI] [PubMed] [Google Scholar]
- 10. Martins P, Rosado-Pinto J, do Céu Teixeira M, et al. Under-report and underdiagnosis of chronic respiratory diseases in an African country. Allergy. 2009; 64:1061–1067. [DOI] [PubMed] [Google Scholar]
- 11. Porsbjerg C, Sverrild A, Stensen L, Backer V. The level of specialist assessment of adult asthma is influenced by patient age. Respir Med. 2014; 108:1453–1459. [DOI] [PubMed] [Google Scholar]
- 12. Tomita K, Hanaki K, Hasegawa Y, et al. Underrecognition of the severity of asthma and undertreatment of asthma in a rural area of Japan. J Asthma. 2005; 42:689–696. [DOI] [PubMed] [Google Scholar]
- 13. van Schayck O. Global strategies for reducing the burden from asthma. Prim Care Respir J. 2013; 22:239–243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Gold L, Smith N, Allen-Ramey F, Nathan RA, Sullivan SD. Associations of patient outcomes with level of asthma control. Ann Allergy Asthma Immunol. 2012; 109:260–265.e2. [DOI] [PubMed] [Google Scholar]
- 15. Gold LS, Thompson P, Salvi S, Faruqi RA, Sullivan SD. Level of asthma control and health care utilization in Asia-Pacific countries. Respir Med. 2014; 108:271–277. [DOI] [PubMed] [Google Scholar]
- 16. Price D, Fletcher M, van der Molen T. Asthma control and management in 8,000 European patients: the REcognise Asthma and LInk to Symptoms and Experience (REALISE) survey. NPJ Prim Care Respir Med. 2014; 24:14009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Bauer BA, Reed CE, Yunginger JW, Wollan PC, Silverstein MD. Incidence and outcomes of asthma in the elderly. A population-based study in Rochester. Minnesota. Chest. 1997; 111:303–310. [DOI] [PubMed] [Google Scholar]
- 18. Enright PL, McClelland RL, Newman AB, Gottlieb DJ, Lebowitz MD. Underdiagnosis and undertreatment of asthma in the elderly. Cardiovascular Health Study Research Group. Chest. 1999; 116:603–613. [DOI] [PubMed] [Google Scholar]
- 19. Huss K, Naumann PL, Mason PJ, et al. Asthma severity, atopic status, allergen exposure and quality of life in the elderly persons. Ann Allergy Asthma Immunol. 2001; 86:524–530. [DOI] [PubMed] [Google Scholar]
- 20. Yáñez A, Cho S, Soriano J, et al. Asthma in the elderly: what we know and what we have yet to know. World Allergy Organ J. 2014; 7:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Gold LS, Montealegre F, Allen-Ramey FC, et al. Level of asthma control and healthcare utilization in Latin America. Allergy. 2013; 68:1463–1466. [DOI] [PubMed] [Google Scholar]
- 22. Rabe KF, Vermeire PA, Soriano JB, Maier WC. Clinical management of asthma in 1999: the Asthma Insights and Reality in Europe (AIRE) study. Eur Respir J. 2000; 16:802–807. [DOI] [PubMed] [Google Scholar]
- 23. Thompson PJ, Salvi S, Lin J, et al. Insights, attitudes and perceptions about asthma and its treatment: findings from a multinational survey of patients from 8 Asia-Pacific countries and Hong Kong. Respirology. 2013; 18:957–967. [DOI] [PubMed] [Google Scholar]
- 24. Global Initiative for Asthma. Global Strategy For Asthma Management And Prevention, 2018. Available from https://ginasthma.org/download/832 Accessed October 3, 2018.
- 25. Hassan Mahboub BH, Santhakumar S, Soriano JB, Pawankar R. Asthma insights and reality in the United Arab Emirates. Ann Thorac Med. 2010; 5:217–221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Schatz M, Sorkness CA, Li JT, Marcus P, Murray JJ, Nathan RA, et al. Asthma control test: Reliability, validity, and responsiveness in patients not previously followed by asthma specialists. J Allergy Clin Immunol 2006;117:549–556. [DOI] [PubMed] [Google Scholar]
- 27. Torchyan AA. Asthma control in Saudi Arabia: gender implications. Allergy Asthma Proc. 2017; 38:47–53. [DOI] [PubMed] [Google Scholar]
- 28. International Society for Phamacoepidemiology. Guidelines for Good Pharmacoepidemiology Practices (GPP). Revision 3: June 2015. Available from https://www.pharmacoepi.org/resources/policies/guidelines-08027 Accessed October 3, 2018.
- 29. Nathan RA, Thompson PJ, Price D, et al. Taking aim at asthma around the world: Global results of the Asthma Insight and Management Survey in the Asia-Pacific Region. Latin America, Europe, Canada, the United States. J Allergy Clin Immunol Pract. 2015; 3:734–742.e5. [DOI] [PubMed] [Google Scholar]
- 30. Abt SRBI Inc. The Asthma Insight and Management in Europe and Canada (EUCAN AIM) survey 2010: a multi-country survey of asthma patients: SRBI, 2010. Available from http://www.takingaimatasthma.eu/docs/EUCAN_AIM_Highlights.pdf Accessed October 3, 2018.
- 31. Akhtar-Danesh N, Landeen J. Relation between depression and sociodemographic factors. Int J Ment Health Syst. 2007; 1:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Psychometric Resource Center. Bias in Interviewing and Self Report Questionnaires, 2017. Available from http://www.psychometric-assessment.com/bias-in-interviewing-and-self-report-questionnaires Accessed October 3, 2018.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.