

Abstract
Objectives
The current study set out to examine the links between contact frequency with one’s social network and cognitive health in later life. It assessed both direct and indirect pathways and the possible role of ethnicity in the effect of the social network on cognitive function.
Method
We used data from adults aged 50 and above, which was collected in Israel as part of the Survey of Ageing, Retirement and Health (SHARE). A moderated mediation analysis was conducted to test the direct and indirect associations between contact frequency and cognitive function, as well as the moderation of these associations by population group. Three population groups were examined – veteran-Jews, Arabs and immigrants from the former Soviet Union.
Results
Contact frequency with the close social milieu was found to be directly positively related to cognitive function. The association was also mediated by depressive symptoms, such that frequent contacts were linked to cognitive health via reduced depressive symptoms. This indirect link differed, however, among the three population groups.
Conclusion
Contact frequency is important for cognitive health in the second half of life, and it operates both directly and by decreasing depressive symptoms. However, these links are not found among all ethnic groups and may, therefore, depend on the culture and social norms of each group and the meaning attributed to social ties.
Keywords: Psychosocial and cultural aspects, depression, cognitive functioning
Introduction
A growing body of evidence shows that older adults embedded in resourceful social networks exhibit better cognitive performance than their more socially disengaged peers (Charles & Carstensen, 2010). Specifically, persons who report frequent contact with their social networks tend to function better cognitively (Seeman et al., 2011; Wang, He, & Dong, 2015; Zunzunegui, Alvarado, Del Ser, & Otero, 2003) and experience less cognitive decline (Zunzunegui et al., 2003), although this association is not always found (Gow, Corley, Starr, & Deary, 2013; Holtzman et al., 2004). However, while many studies examine the existence of such an association, there is a scarcity in research regarding the mechanisms underlying this relationship (Bielak, 2010).
Contact frequency is commonly assumed to impact cognitive health in old age directly, an assumption represented by the ‘use it or lose it’ theory. This perspective suggests that frequent engagement with others provides ‘cognitive exercise’ which stimulates the mind and preserves cognitive functions (Hertzog, Kramer, Wilson, & Lindenberger, 2009; Hultsch, Hertzog, Small, & Dixon, 1999). Cognitive stimulation may be achieved by navigating social cues, organizing social gatherings and engaging in complex social discourse (Bielak, 2010; Kim & Kim, 2014). Such encounters can also enhance cognitive reserve, which allows people to tolerate brain pathology without showing clear behavioral symptoms (Bennett, Schneider, Tang, Arnold, & Wilson, 2006).
However, the direct pathway of impact presents only a partial explanation of the effect of social contacts on cognitive health. In addition to offering mental stimulation, interacting with others can improve cognitive health by reducing psychological stress and improving one’s mental health. Berkman and colleagues (2000) proffer a conceptual model of a cascading social process, in which engagement with meaningful others can affect cognitive health through mediators such as psychological distress. Although this suggested mechanism has been brought up as a possible explanation of the associations between social networks and cognitive health, there is little research directed at its empirical examination (Fratiglioni, Paillard-Borg, & Winblad, 2004). Therefore, it has been suggested that studies need to further investigate such specific mechanisms (Berkman et al., 2000; Bielak, 2010). A step in that direction was made by a study which demonstrated an indirect effect of social and leisure activities on cognitive health through psychological stress (McHugh Power, Tang, Lawlor, Kenny, & Kee, 2018). Nonetheless, that inquiry did not differentiate social activities from non-social leisure activities, leaving questions about the specific pathways of social interactions unanswered. Consequently, the current study will examine both the direct and indirect pathways from contact frequency to cognitive health.
An important additional aspect of this association is its manifestation in different cultural contexts. Studies regarding social contacts and cognition usually focus on older adults from Western cultures and do not differentiate between diverse population groups (Gow et al., 2013; Holtzman et al., 2004; La Fleur & Salthouse, 2016. For an exception see Wang et al., 2015). This lack in the literature is meaningful as the associations in question may not be universal and may, indeed, be influenced by socio-cultural factors (Bielak, 2010). For example, minority group members, who tend to have lower social status and less access to resources, also generally perform worse cognitively than persons belonging to the majority culture (Lee et al., 2012; Ng, Niti, Chiam, & Kua, 2007).
Minority group members also differ in the characteristics of their social environment. Research regarding African-Americans shows that they usually have smaller and more familial social networks, compared to their white counterparts, and they contact them more frequently (Ajrouch, Antonucci, & Janevic, 2001). People who emigrate in late life may face an even greater risk of having relatively restricted social networks due to language and cultural barriers and, hence, they rely mostly on adult children (Diwan, 2008; Wong, Yoo, & Stewart, 2005). Moreover, minority groups have unique beliefs, norms and expectations from this environment (Wong et al., 2005), which may influence the manner in which their social networks impact their cognitive health. It is possible, therefore, that under such different social norms and expectations, engagement with close others portends different outcomes for one’s cognitive health.
Israel provides a particularly relevant setting in which to investigate the associations between contact frequency and cognitive health in minority groups, due to its multi-cultural and multi-ethnic population. The older cohort in Israel can be divided into three main groups – veteran-Jews, new immigrants from the Former Soviet Union (FSU), and Arab Israelis. The majority group is composed of Hebrew-speaking veteran-Jews, that is, those who were either born in Israel or immigrated to it (except for the recent FSU immigrants who are presented next). The FSU immigrants came to Israel in a mass immigration wave in the early 1990s and currently form 19% of the older population. They underwent the immigration process at a relatively older age than immigrants do in general. They also tend to be more educated but have a lower income compared to the veteran-Jews (Ayalon, Heinik, & Litwin, 2010). Moreover, they are more likely to have fewer children living close by and to report having less contact with their children (Litwin, 2006).
The Arab population consists of 12% of the older population in Israel (Brodsky, Shnoor, & Be’er, 2017). They are mostly Muslim, speak Arabic and on average tend to be relatively disadvantaged on all socioeconomic indicators (i.e. education, income, and employment status). They are less healthy and more depressed compared to the majority group, although they tend to perceive their health as better (Khalaila, 2017; Khalaila & Litwin, 2014). There are some indications of a higher rate of dementia in an Arab Israeli rural community of three villages (Bowirrat, Treves, Friedland, & Korczyn, 2001) and data shows that Arab Israelis exhibit poorer reading skills (Central Bureau of Statistics, 2017). They also have a more traditional lifestyle and larger households (Central Bureau of Statistics, 2017), although they share their personal problems with others less often (Baron-Epel, 2009) and it is unclear whether they have more or less contacts with family and friends (Baron-Epel, 2009; Litwin, 2006).
Previous research suggests that among Israeli adults from different population groups, social relationships vary in their effects on physical health and well-being. Such inquiry provides some indication that among the Israeli minority groups, social factors are associated to a lower extent with mental and self-rated health (Baron-Epel, 2009; Baron-Epel, Weinstein, Haviv-Mesika, Garty-Sandalon, & Green, 2008), although there are other findings that show no group differences in the influence of social networks on quality of life (Damri & Litwin, 2016). Moreover, it is as yet unclear whether these trends extend to cognitive health. Building upon these findings and the literature explored above, the current study explores group differences in relation to cognitive health. Specifically, it considers both the direct and the indirect pathways from social contacts to cognitive performance among older adults from the three main population groups in Israel. We address four hypotheses:
Contact frequency with the members of one’s social network is positively associated with cognitive health.
Contact frequency with the network members is also indirectly linked with cognitive health. That is, contact frequency is associated with mental health, which is related to higher cognitive health among older adults.
The direct effects of contact frequency on cognitive health are smaller among minority groups.
The indirect effects of contact frequency on cognitive health through mental health are smaller among minority groups.
Methods
The study uses data from SHARE-Israel, the Israeli component of the Survey of Health, Aging and Retirement in Europe (Börsch-Supan et al., 2013). The survey provides extensive information on a variety of domains in a nationally representative sample of Israelis aged 50 and above and their spouses of any age (Litwin, 2009). Questionnaires were administered using computerized interviews, conducted in the three main languages spoken by older adults in Israel – Hebrew, Arabic and Russian. The current study is based on data collected in 2015 (Börsch-Supan, 2017).
The analytical sample consisted of all respondents aged 50 and above. We excluded participants whose ethnicity, as reported by the survey agency, did not match their language interview (e.g. Arab Israelis who chose to be interviewed in Hebrew). Respondents were also excluded if they had a diagnosis of Alzheimer’s disease, dementia or any other serious memory impairment. The final analytical sample numbered 1,718 participants, who completed the assessment tools for cognitive performance.
The main analysis was conducted on 1,348 participants who had full information on all the study variables. We compared these participants to those who were not included in the main analysis due to missing information, using t-test analyses for continuous variables and chi-square tests for factors. Effect sizes were assessed using ’, Cramer’s V, and Cohen’s d for χ2 and t-tests, respectively. Small, medium and large effects were considered for values of 0.1, 0.3, and 0.5 respectively for φ and Cramer’s V, and for values of 0.2, 0.5, and 0.8, respectively, for Cohen’s d. Participants with missing information were more likely not to have a partner (φ = 0.86), not to participate in social activities (φ = 0.74), more likely to be veteran-Jews and less likely to be FSU immigrants (Cramer’s V = 0.91). They did not differ in terms of age, years of education, gender, cognition score, depressive symptoms and self-rated health.
Measures
Dependent variable
Cognitive performance was assessed via a composite measure based on three cognitive tests of immediate recall, delayed recall and fluency (Adam, Bonsang, Grotz, & Perelman, 2013). The immediate and delayed recall tasks are known as episodic memory tasks that evaluate short-term verbal learning and memory and information retention (Cheke & Clayton, 2013). In the immediate memory task, the interviewer reads aloud a list of ten words and asks the respondent to recall as many as he or she can. In the delayed recall task, the respondent is asked to repeat these words 5–10 min later. The scores for each of these tests range from 0–10. Verbal fluency, a measure of executive function and language ability (Henry, Crawford, & Phillips, 2004), was measured by asking respondents to name as many animals as they can in one minute. Due to outliers in a small number of cases, scores greater than 45 were re-coded as 45. The composite measure of cognition was constructed by averaging the standardized scores of these three indicators.
Independent variable
Social networks were measured in SHARE-Israel for the first time in 2015. They were assessed using a novel name-generator approach which maps individuals’ social milieu from their subjective perspective. Respondents are asked to name up to seven persons with whom they discuss important matters, and are subsequently asked to provide more information about these confidants and about the relationship with them (Litwin, Stoeckel, Roll, Shiovitz-Ezra, & Kotte, 2013). We focused on the question about the contact frequency with the social network members, which had seven response options ranging from ‘Daily’ to ‘Never.’ Contact frequency with the social network in the current analyses was calculated as the average score of the contact with the social network members, and it was re-coded such that higher scores meant more frequent contact.
Mediator
The current study also examined whether contact frequency was associated with cognitive health indirectly, through mental health. This construct was captured by means of depressive symptoms, assessed using the EURO-D scale. The scale was developed in order to measure late life depressive symptoms across European countries and has been shown to have good validity and internal consistency (Castro-Costa et al., 2008). It consists of 12 binary items inquiring about different depressive symptoms: depressed mood, pessimism, suicidality, guilt, sleep, interest, irritability, appetite, fatigue, concentration, enjoyment and tearfulness. Scores range from 0 to 12, with higher scores indicating greater symptoms severity. Internal reliability was measured by Kuder-Richardson’s ρ and was .75.
Covariates and moderators
Cognitive performance in later life is influenced by a variety of socio-economic and health variables, such as age, education, gender, marital status, social activities and physical health (Agrigoroaei & Lachman, 2011; Litwin & Stoeckel, 2015). We therefore included these factors as covariates in the analyses. Age was used as a continuous variable and gender as a dummy variable (1 = Men, 2 = Women). Participants were further divided into having a partner (being married or in a registered partnership) or not having a partner (never married\divorced\widowed). Education was measured by years of education. Social activities were assessed using a set of questions about engaging in such undertakings as going to social clubs and educational courses. The measure of social activities was re-coded into a dichotomous variable indicating participation in any activity or no participation at all. Self-assessed health was measured on a 5-point Likert scale, which was reverse coded such that a higher score indicated better perceived health. The populations groups were veteran-Jews, Arabs and FSU immigrants. They were identified based on language of interview and an additional variable created during data cleaning, which confirmed population group status based on information from the interviewers. Respondents were assigned to a population group and included in the analyses only if they were identified by both variables.
Data analyses
First, descriptive statistics were employed to calculate the means and standard deviations of the continuous variables and the percentage and frequency of the categorical variables. In the second stage, bivariate analyses were performed to examine the association between cognitive health and the study variables, using independent t-tests for factors and Pearson tests for continuous variables.
Next, we employed mediation and moderated mediation analyses to test the study hypotheses (Preacher & Hayes, 2008). Hayes (2012) suggests using PROCESS model 10, which simultaneously tests mediation effects and moderated mediation effects. This model allows the indirect effects of the independent variable (X) on a dependent variable (Y) through a mediator (M) to be moderated by two moderators (W and Z). In the current study, this method calculates the mediating effect between the independent variable (X; contact frequency) and the dependent variable (Y; cognitive performance) through a mediator (M; depressive symptoms) at several values of the two dummy moderators (W: Arabs vs. veteran-Jews; and Z: FSU immigrants vs. veteran-Jews). All models also accounted for the covariates.
The first hypothesis, of a direct association between contact frequency and cognitive health was analyzed by assessing the direct effect of the independent variable (contact frequency) on the dependent variable (cognitive performance). The second hypothesis, regarding an indirect effect through depression, was assessed by adding the mediator (depressive symptoms) to the analysis of the total effect. These analyses were conducted while controlling for covariates and moderators, using the PROCESS mediation model 4 (Hayes, 2012; Preacher & Hayes, 2008).
The second stage referred to the moderated mediation effects, using PROCESS model 10 (Hayes, 2012). This model tests the moderation of the direct and indirect effects. The third hypothesis was examined via an interaction of population groups with contact frequency, with cognitive performance as the outcome variable. The fourth hypothesis suggested that the indirect effect through depression varies by population groups, and was therefore tested as an interaction of population groups with contact frequency, with depressive symptoms as the outcome variable. A significant interaction, were it to be found, can indicate that the groups differ in the way that contact frequency impacts cognitive health through depression.
The total effect, conditional indirect and direct effects were calculated through bootstrapping set at 5,000 samples. Confidence intervals were calculated using this method by sorting the lowest to highest of these 5,000 samples of the original dataset, yielding a 95-percentile confidence interval. All analyses were run using SPSS 20.0 with PROCESS statistical program (Hayes, 2012). All estimated effects reported by PROCESS are unstandardized regression coefficients.
Results
Table 1 displays the descriptive characteristics of the study sample. It shows that the average contact frequency with the social network was 6.4, which indicates that the respondents contacted their social network members between daily and several times a week. They also reported an average of 2.5 depressive symptoms. As the cognitive performance indicator is based on standardized scores, its mean value is around zero, by design. Almost three quarters of respondents were veteran-Jews, followed by FSU immigrants and Arabs, respectively. Table 1 also shows that women were a majority in the sample. The mean age was almost 70 and the average years of education were over 12. Three quarters of the participants had partners. About half participated in social activities, and they rated their health as ‘good’ (3 on a scale of 1–5).
Table 1.
Descriptive statistics of the study variables (N = 1,718).
| Variables | Valid N (%) | Mean (S.D) | Range | |
|---|---|---|---|---|
| Independent variable | ||||
| Contact frequency | 6.4 (0.8) | 1–7 | ||
| Dependent variable | ||||
| Cognitive performance | 0.0016 (0.9) | 2.38–2.09 | ||
| Mediator | ||||
| Depression score | 2.5 (2.4) | 0–12 | ||
| Covariates | ||||
| Gender | Men | 718 (41.8) | ||
| Women | 1000 (58.2) | |||
| Age | 68.9 (9.2) | 50–105 | ||
| Education | 12.6 (4.3) | 0–25 | ||
| Ethnicity | Veteran-Jews | 1196 (71.8) | ||
| Immigrants from the | 285 (17.1) | |||
| Former Soviet Union (FSU) | ||||
| Arabs | 184 (11.1) | |||
| Marital status | No partner | 419 (25.4) | ||
| Has partner | 1233 (74.6) | |||
| Social activities | No | 867 (51.8) | ||
| Yes | 808 (48.2) | |||
| Self-rated health | 3.0 (1.1) | 1–5 |
Table 2 presents the bivariate tests of the study variables with cognitive performance as the dependent variable. It shows that respondents who contacted their social network more often also functioned better cognitively. Higher depressive symptoms, on the other hand, were associated with worse cognitive health. An ethnic difference in cognitive health was also found and the results revealed that the FSU immigrant and Arab groups had lower cognitive performance than the veteran-Jews group. Further ANOVA analyses showed that the highest cognitive performance was reported by veteran Jews (Mean = 0.09, SD = 0.9), followed by FSU immigrants (Mean = −0.26, SD = 0.8) and Arabs (Mean = −0.33, SD = 0.7) [f (2, 1777) = 34.3, p = 0.001] (data not shown).
Table 2.
Bivariate tests of covariates and mediator with cognitive performance (N = 1,718).
| Variables | Cognitive function
|
|||
|---|---|---|---|---|
| Mean (S.D) | Test | p.value | ||
| Contact frequency | r = 0.08 | 0.001 | ||
| Depression score | r = −0.50 | 0.001 | ||
| Gender | Female | −0.02 (0.8) | t = 1.09 | 0.30 |
| Male | 0.03 (0.8) | |||
| Age | r = −0.44 | 0.001 | ||
| Education | r = 0.35 | 0.001 | ||
| Ethnicity_Arabs | Jews | 0.03 (0.8) | t = 6.01 | 0.001 |
| Arabs | −0.32 (0.7) | |||
| Ethnicity_FSU | Jews | 0.04 (0.9) | t = 5.83 | 0.001 |
| FSU | −0.26 (0.7) | |||
| Marital status | Has partner | 0.11 (0.9) | t = −7.86 | 0.001 |
| No partner | −0.30 (0.8) | |||
| Social activities | Yes | 0.17 (0.8) | t = −8.05 | 0.001 |
| No | −0.15 (0.9) | |||
| Self-rated health | r = 0.41 | 0.001 | ||
The analyses also revealed that advanced age was negatively correlated with cognitive performance, while educational level was positively correlated. Gender was not associated with cognition. Married respondents showed greater cognitive performance than those with no partner. Cognitive health was also greater among respondents involved in social activities and among those reporting better health.
Direct and indirect effects
We first tested whether contact frequency was associated with cognitive health, while controlling for covariates (see Figure 1). The results indicated a significant total direct effect (path C) of contact frequency on cognitive performance (B = 0.11, t (1348) = 3.71, p = 0.001, 95% CI = 0.05, 0.17; Adjusted R2 = 0.32). We then examined whether that direct effect was mediated by depressive symptoms, while controlling for the background variables. After adding depressive symptoms as a mediator, the direct effect of contact frequency decreased, albeit remaining significant (path C′; with mediator) (B = 0.07, t (1348) = 2.49, p = 0.01, 95% CI = 0.01, 0.12, Adjusted R2 = 0.39). The indirect effect was also significant, indicating that frequent contact with the social network was related to improved cognition also through reduced depressive symptoms, which contributed 7 percent to the explained variance in cognitive performance, after the contribution of the covariates.
Figure 1.
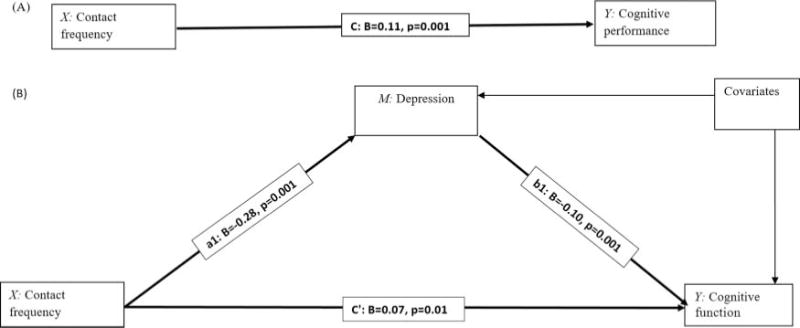
The mediation model depicting direct and indirect effects of contact frequency (X) on cognitive performance (Y) tested in the current study, controlling for covariates. Notes: Graphic A depicts the total effect (C) of contact frequency (X) on cognitive performance (Y). Graphic B depicts the direct effect (C′) of contact frequency (X) on cognitive performance (Y) after including a mediator (M: depression). Values represent unstandardized regression coefficients.
Moderation by ethnicity
We next examined whether the direct and indirect effects of contact frequency on cognitive performance vary by population group (Table 3). The first model in Table 3 focused on the direct effect of contact frequency on cognition and its interaction with population groups. It indicated a significant direct effect of contact frequency on cognitive performance even after including the other study variables. However, the population group variables were not associated with cognitive performance, after controlling for the different covariates, and they also did not significantly interact with contact frequency. That is, there were no significant differences in cognitive performance between the ethnic groups, and the direct association between contact frequency and cognitive performance was not conditional on ethnicity. The analysis also revealed that cognitive performance was negatively associated with depression, such that persons who reported more depressive symptoms had worse cognitive health. Additionally, better cognitive performance was associated with younger age, more years of education, participation in social activities and good self-rated health, while no significant associations were found for gender and marital status.
Table 3.
Direct and indirect effect of contact frequency on cognitive performance through depression conditionally in ethnicity (N = 1,348).
| Path: Predictor | Dependent variable model (Y = Cognitive function)
|
Adj R2 (p.value) | |||
|---|---|---|---|---|---|
| B | SE | t | p | ||
| Constant | 1.10 | 0.22 | 4.90 | 0.001 | 0.40 (0.001) |
| Contact frequency (X) | 0.05 | 0.28 | 2.01 | 0.04 | |
| Ethnicity_Arabs | 0.06 | 0.08 | 0.67 | 0.49 | |
| Ethnicity_FSU | −0.05 | 0.05 | −1.01 | 0.31 | |
| Contact frequency X Ethnicity_Arabs | −0.09 | 0.12 | −0.78 | 0.42 | |
| Contact frequency X Ethnicity_FSU | −0.11 | 0.07 | −1.47 | 0.14 | |
| Depressive symptoms | −0.10 | 0.01 | −10.34 | 0.001 | |
| Covariates | |||||
| Gender | −0.01 | 0.03 | −0.08 | 0.93 | |
| Age | −0.02 | 0.01 | −10.08 | 0.001 | |
| Marital status | 0.01 | 0.04 | 0.11 | 0.90 | |
| Education years | 0.04 | 0.01 | 7.95 | 0.001 | |
| Social activities | 0.17 | 0.03 | 4.37 | 0.001 | |
| Self-rated health | 0.08 | 0.02 | 3.92 | 0.001 | |
|
Mediator variable model (M = Depressive symptoms) | |||||
| Path: Predictor | B | SE | t | p | Adj R2 (p.value) |
|
| |||||
| Constant | 5.02 | 0.65 | 7.60 | 0.001 | 0.30 (0.001) |
| Contact frequency (X) | −0.28 | 0.08 | 3.40 | 0.001 | |
| Ethnicity_Arabs | 0.06 | 0.21 | 0.28 | 0.77 | |
| Ethnicity_FSU | 0.40 | 0.17 | 2.29 | 0.02 | |
| Contact frequency X Ethnicity_Arabs | 1.29 | 0.26 | 4.90 | 0.001 | |
| Contact frequency X Ethnicity_FSU | 0.49 | 0.21 | 2.25 | 0.02 | |
Notes: Value labels of categorical variables: ethnicity_Arabs (0 = Jews and FSU immigrants, 1 = Arabs); ethnicity_FSU (0 = Jews and Arabs, 1 = Former Soviet immigrants), gender (0 = male, 1 = female); Marital status (0 = no partner, 1 = has partner); Social activities (0 = no, 1 = yes). The mediator model also controlled for gender, age, marital status, education years, social activities and self-rated health.
Table 3 also shows the effects of the study variables on the depression measure. This analysis is meant to examine whether the population groups moderate the indirect effects of contact frequency through depressive symptoms. As may be seen, contact frequency was negatively associated with the depression score. The FSU group was likely to have more depressive symptoms than the veteran-Jews group, but no difference was found between Arabs and Jews in depression scores. Additionally, the interaction of contact frequency with population groups was significant. It revealed that both Arabs and FSU immigrants differed from the veteran-Jews in the associations between contact frequency and depression.
A simple moderation analysis was next conducted to explore the effect of the contact frequency—ethnicity interaction on depression (using PROCESS 2016, model 1). Figure 2 displays the results of the interaction. It shows that only among the veteran-Jews was frequently contacting the social network associated with less depressive symptoms. Among the Arab respondents, on the other hand, more frequent interaction was related to a higher depression score. For the FSU immigrants, this association was not significant. These results imply that the three population groups differ in their psychological pathways from contact frequency to cognition. That is, among the veteran-Jews, contacting the social network is related to lowered depression, which in turn is related to better cognition. Among the Arabs, frequent contact is related to more depressive symptoms, which are associated with worse cognition. For the FSU immigrants, contact frequency is not related to cognitive health through mental health, but only in a direct link.
Figure 2.
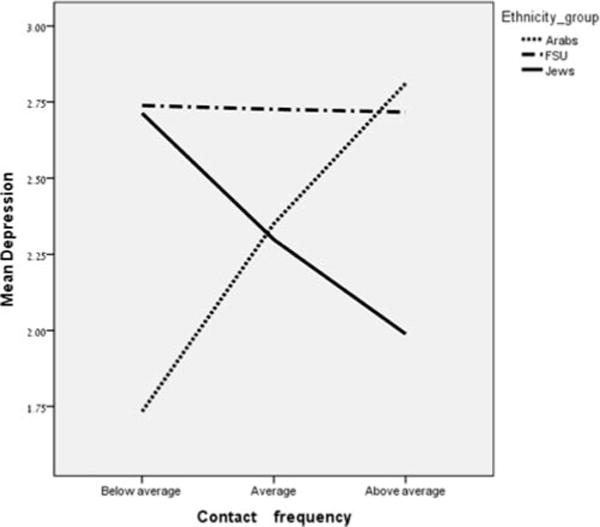
Relationship between contact frequency and depression score for different population groups (veteran-Jews, FSU immigrants and Arabs), controlling for covariates.
We note that the social network module was first introduced to SHARE-Israel in 2015, and therefore it is difficult to fully capitalize on the rich longitudinal data available. Still, previous waves assessed cognitive health in SHARE-Israel. We conducted a supplementary analysis that controlled for cognitive health from the previous wave, collected in 2013. This analysis was performed as a supplementary analysis (Supplementary Table 1), as it reduced the sample size in a significant way due to between-wave attrition. The results are similar to those conducted with the 2015 sample, with the only difference being that the interaction of FSU immigrants with depressive symptoms was no longer significant. This analysis may partly help disentangle the potential reciprocal effects of contacts and cognition and indicate that contact frequency impacts cognitive performance even when controlling for earlier cognition.
Discussion
The present study investigated the links between social contacts and cognitive performance in later life, while paying special attention to the mechanisms and cultural context of this association. First, the results showed that adults who contact their social milieu more frequently also have better cognitive health. In addition to that direct linkage, the association was also mediated by depressive symptoms. Those who more frequently contacted their social milieu had better mental health, which in turn was linked to a better cognitive state. Last, the cultural context in which these social contacts occurred was related to their impact on cognition, as the mediation effect was found to differ among the population groups in Israel. Frequent contact was related to cognition through lower depression only among the veteran-Jews, the majority population. Among the Arab Israelis, greater contact frequency was associated with greater depressive symptoms. For the FSU immigrants, on the other hand, contact frequency was not related to depressive symptoms and impacted cognition only directly.
Overall, our first hypothesis was supported, as contact frequency with the social network was found to be beneficial for the cognition of older adults. In accordance with the ‘use it or lose it’ theory, frequently engaging in social interactions may operate as a form of mental exercise and maintain cognitive abilities (Hultsch et al., 1999). This result helps clarify previous inconsistent findings regarding this association (Gow et al., 2013; La Fleur & Salthouse, 2016; Seeman et al., 2011; Wang et al., 2015), and supports the premise of a positive association between the two constructs.
Additionally, we found that contact frequency not only impacts cognition directly, it can act on cognitive health through a psychological avenue by lowering depression, in accordance with our second hypothesis. Moreover, after adding this indirect link to the model, the direct association shrank (albeit remaining significant). This indicates that part of the direct impact of social contacts on cognitive health is explained by their effect on mental health. Frequently contacting close others may provide various emotional benefits, such as a sense of belonging (Baumeister & Leary, 1995), and these close others can also provide advice and assistance in coping with stressful events (Cohen & Wills, 1985). Lower depression has important implications for cognition, perhaps through hindering neurodeteriorative changes that can affect cognition (Hertzog et al., 2009). Showing such mediation is an important addition to the understanding of the means through which social networks affect cognition (Bielak, 2010).
One of this study’s main goals was to explore the cultural context of the relationship between social networks and cognitive health. The results indicate that indeed, cultural status can influence the way that social ties affect cognition in later life. Contact frequency was directly and positively related to cognitive health in all the population groups, contradictory to the third hypothesis. Nevertheless, the indirect link varied among the different groups, in partial accordance with our last hypothesis (#4), as we summarize next. It seems that only among the veteran-Jews, was contact with meaningful others associated with cognition through reduced depressive symptoms.
In contrast, among the Arab Israelis, social contacts were related to cognition through elevated depressive symptoms. A possible explanation for this finding is that members of this population group contact their very close network members mainly when bad or urgent events occur. Contacts with the wider circle, on the other hand, have been found elsewhere to occur in relation to more general pleasant occurrences or when daily intergenerational transfers of money or time are carried out (Lavee & Katz, 2003). As noted earlier in the article, the current study mapped only the close social networks and secondary ties were not considered. An additional possible explanation is that Arab Israelis provide more caregiving to family members, and the increased contact frequency reflects greater caregiving burden (Khalaila & Cohen, 2016; Khalaila & Litwin, 2011). Among Arab Israelis, therefore, social contacts may have two contradictory effects (Baron-Epel, 2009). They can act as a form of mental stimulation, but may also be negatively related to cognition by signaling stress or caregiving burden. This tendency may be related to this group’s more collectivist worldview, which emphasizes interdependence and can lead to frequent contacts with close familial ties despite interpersonal tensions (Oyserman, 1993; Singelis, Triandis, Bhawuk, & Gelfand, 1995). Future studies should examine this premise in other collectivist cultures.
Finally, FSU immigrants’ social contact frequency did not impact their cognitive performance through depression. It could be that among this population, social ties have a different, more instrumental, function and thus exert only a direct influence on cognitive health, without having a moderating effect on depressive symptoms. For example, the interaction of FSU immigrants with their children may revolve around practical tasks that relieve the children of their domestic workload (Khvorostianov & Remennick, 2015). This result echoes previous findings in which the FSU immigrants’ quality of life wasn’t influenced by support exchanges with their social environment (Damri & Litwin, 2016) and their contact frequency was not associated with mental health (Baron-Epel, 2009). However, it is still unclear which aspects of this group’s culture lead to this pattern of results, and this premise should be examined in future research.
Taken together, the findings from the present study indicate that it is important to understand the context in which social contacts occur and the meanings attributed to them to better assess their impact on cognitive health. Moreover, the findings underscore the necessity of understanding the different characteristics of minority groups in order to comprehend their unique pathways to cognition. These pathways may be direct or indirect, and cultural norms can influence the indirect avenues, possibly even resulting in opposite directions of influence.
The current study has a few potential limitations that should be addressed in future research. Due to the complexity of the model, the outcome variable was composed of an aggregate score of cognition, combining several cognitive tests. While this provides a valuable indication of cognitive status, future research may expand upon different cognitive skills, as there are documented differences in various cognitive tasks among the population groups in Israel (Ayalon et al., 2010). Another limitation may concern the possibility of slight differences in the translations of the cognitive measures, from English into three different languages: Hebrew, Arabic, and Russian. It might be, for example, that the different words used in the recall tasks differ in their frequency of use within the three languages. The SHARE project employs various measures to avoid such translation effects, but differences may still occur, as in every cross-cultural study. We took an additional measure to minimize such biases by leaving out participants whose language of interview did not match their declared group, such as Arabs who were interviewed in Hebrew.
An additional possible limitation is that of reverse causation, given the cross-sectional nature of the current analyses. The option of a reverse direction of influence is suggested by the health selection hypothesis, which maintains that cognitive limitations affect social relationships due to reduced social functioning and diminished social reciprocity (Liao, Muniz-Terrera, Head, & Brunner, 2017). Although empirical evidence doesn’t generally provide support for this hypothesis (Ertel, Glymour, & Berkman, 2008; Hertzog et al., 2009), it should be considered when interpreting the results. This possibility could not be addressed in the current investigation since only one wave of data was collected in Israel. However, it may be examined in the future following the collection of additional waves of data. Additionally, it should be noted that some respondents were not included in the final analysis due to missing information and they differed in several attributes from those participants who were eventually included.
The current study examined the role of social contacts in relation to cognition, a topic in need of better understanding. However, we note that additional social variables may be relevant to cognitive health, such as loneliness and positivity of relationships. Future studies may expand the current findings by examining the role of other social factors in relation to cognitive performance.
Despite these limitations, the present study nevertheless makes an important contribution. It highlights the positive association between frequently contacting one’s social milieu and cognitive performance among older people. However, it goes beyond merely describing this association and underscores its complex nuances. It shows that depression is an important mediating factor, and that the meaning and significance attributed to social contact may vary among different population groups. Practitioners working with older people may benefit from more carefully considering the function of social contact in different cultures. Moreover, they should develop culturally relevant interventions aimed at improving their older patients’ cognitive health, considering the unique role of social contacts in each culture.
Supplementary Material
Acknowledgments
Funding for this research, from the Bader Philanthropies, Inc., is gratefully acknowledged.
Funding
This paper uses data from SHARE Wave 6 (DOI: 10.6103/SHARE.w6.600). The SHARE data collection has been primarily funded by the European Commission through FP5 (QLK6-CT-2001–00 360), FP6 (SHARE-I3: RII-CT-2006–062 193, COMPARE: CIT5-CT-2005–028 857, SHARELIFE: CIT4-CT-2006–028 812) and FP7 (SHARE-PREP: N° 211 909, SHARE-LEAP: N° 227 822, SHARE M4: N° 261 982). Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740–13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG4553–01, IAG_BSR06–11, OGHA_04–064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see www.share-project.org).
Footnotes
Supplemental data for this article can be accessed at https://doi.org/10.1080/13607863.2018.1459472
Disclosure of interest
The authors report no conflicts of interest.
References
- Adam S, Bonsang E, Grotz C, Perelman S. Occupational activity and cognitive reserve: Implications in terms of prevention of cognitive aging and Alzheimer’s disease. Clinical Interventions in Aging. 2013;8:377–390. doi: 10.2147/CIA.S39921. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agrigoroaei S, Lachman ME. Cognitive functioning in midlife and old age: Combined effects of psychosocial and behavioral factors. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences. 2011;66B(S1):i130–i140. doi: 10.1093/geronb/gbr017. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ajrouch KJ, Antonucci TC, Janevic MR. Social networks among blacks and whites: The interaction between race and age. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences. 2001;56(2):S112–S118. doi: 10.1093/geronb/56.2.S112. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Ayalon L, Heinik J, Litwin H. Population group differences in cognitive functioning in a national sample of Israelis 50 years and older. Research on Aging. 2010;32(3):304–322. doi: 10.1177/0164027509356875. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron-Epel O. Differences in the association between social support and mental health in a multi-cultural population in Israel. International Journal of Mental Health Promotion. 2009;11(4):5–14. doi: 10.1080/14623730.2009.9721795. Retrieved from . [DOI] [Google Scholar]
- Baron-Epel O, Weinstein R, Haviv-Mesika A, Garty-Sandalon N, Green MS. Individual-level analysis of social capital and health: A comparison of Arab and Jewish Israelis. Social Science & Medicine. 2008;66(4):900–910. doi: 10.1016/j.socscimed.2007.10.025. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Baumeister R, Leary M. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychological Bulletin. 1995;117(3):497–529. Retrieved from http://doi.org/0033-2909. [PubMed] [Google Scholar]
- Bennett DA, Schneider JA, Tang Y, Arnold SE, Wilson RS. The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: A longitudinal cohort study. Lancet Neurology. 2006;5(5):406–412. doi: 10.1016/S1474-4422(06)70417-3. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: Durkheim in the new millennium. Social Science & Medicine. 2000;51(6):843–857. doi: 10.1016/S0277-9536(00)00065-4. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Bielak AAM. How can we not “lose it” if we still don’t understand how to “use it”? unanswered questions about the influence of activity participation on cognitive performance in older age - A mini-review. Gerontology. 2010;56(5):507–519. doi: 10.1159/000264918. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 6. Release version: 6.0.0. SHARE-ERIC Data set. 2017 doi: 10.6103/SHARE.w6.600. Retrieved from . [DOI]
- Börsch-Supan A, Brandt M, Hunkler C, Kneip T, Korbmacher J, Malter F, Zuber S. Data resource profile: The Survey of Health, Ageing and Retirement in Europe (SHARE) International Journal of Epidemiology. 2013;42(4):992–1001. doi: 10.1093/ije/dyt088. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowirrat A, Treves TA, Friedland RP, Korczyn AD. Prevalence of Alzheimer’s type dementia in an elderly Arab population. European Journal of Neurology. 2001;8(2):119–123. doi: 10.1046/j.1468-1331.2001.00183.x. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Brodsky J, Shnoor Y, Be’er S, editors. The 65+ Population in Israel: Statistical Abstract 2016. Jerusalem: Myers-JDC-Brookdale; 2017. [Google Scholar]
- Castro-Costa E, Dewey M, Stewart R, Banerjee S, Huppert F, Mendonca-Lima C, Prince M. Ascertaining late-life depressive symptoms in Europe: An evaluation of the survey version of the EURO-D scale in 10 nations. The SHARE project. International Journal of Methods in Psychiatric Research. 2008;17(1):12–29. doi: 10.1002/mpr.236. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Central Bureau of Statistics. Society in Israel Report No 9. Jerusalem: Central Bureau of Statistics; 2017. [Google Scholar]
- Charles ST, Carstensen LL. Social and emotional aging. Annual Review of Psychology. 2010;61:383–409. doi: 10.1146/annurev.psych.093008.100448. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheke LG, Clayton NS. Do different tests of episodic memory produce consistent results in human adults ? Learning & Memory. 2013;20(9):491–498. doi: 10.1101/lm.030502.113. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychological Bulletin. 1985;98(2):310–357. Retrieved from http://psycnet.apa.orgjournals/bul/98/2/310. [PubMed] [Google Scholar]
- Damri N, Litwin H. Minority population group status and QOL change: The case of older Israelis. European Journal of Ageing. 2016;13(4):299–309. doi: 10.1007/s10433-016-0396-x. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diwan S. Limited English proficiency, social network characteristics, and depressive symptoms among older immigrants. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences. 2008;63B(3):S184–S191. doi: 10.1093/geronb/63.3.S184. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Ertel KA, Glymour MM, Berkman LF. Effects of social integration on preserving memory function in a nationally representative US elderly population. American Journal of Public Health. 2008;98(7):1215–1220. doi: 10.2105/AJPH.2007.113654. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fratiglioni L, Paillard-Borg S, Winblad B. An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurology. 2004;3(6):343–353. doi: 10.1016/S1474-4422(04)00767-7. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Gow AJ, Corley J, Starr JM, Deary IJ. Which social network or support factors are associated with cognitive abilities in old age ? Gerontology. 2013;59(5):454–463. doi: 10.1159/000351265. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Hayes AF. PROCESS [Macro] 2012 Retrieved from http://afhayes.com/introduction-to-mediation-moderation-and-conditional-process-analysis.html.
- Henry JD, Crawford JR, Phillips LH. Verbal fluency performance in dementia of the Alzheimer’s type: A meta-analysis. Neuropsychologia. 2004;42(9):1212–1222. doi: 10.1016/j.neuropsychologia.2004.02.001. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Hertzog C, Kramer AF, Wilson RS, Lindenberger U. Enrichment effects on adult cognitive development. Psychological Science in the Public Interest. 2009;9(1):1–65. doi: 10.1111/j.1539-6053.2009.01034.x. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Holtzman RE, Rebok GW, Saczynski JS, Kouzis AC, Wilcox Doyle K, Eaton WW. Social network characteristics and cognition in middle-aged and older adults. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences. 2004;59(6):P278–P284. doi: 10.1093/geronb/59.6.P278. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Hultsch DF, Hertzog C, Small BJ, Dixon RA. Use it or lose it: Engaged lifestyle as a buffer of cognitive decline in aging ? Psychology and Aging. 1999;14(2):145–263. doi: 10.1037//0882-7974.14.2.245. Retrieved from http://psycnet.apa.orgjournals/pag/14/2/245. [DOI] [PubMed] [Google Scholar]
- Khalaila R. Socioeconomic status, health behaviors, obesity and self-rated health among older Arabs in Israel. Journal of Cross-Cultural Gerontology. 2017;32(1):115–130. doi: 10.1007/s10823-016-9301-5. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Khalaila R, Cohen M. Emotional suppression, caregiving burden, mastery, coping strategies and mental health in spousal caregivers. Aging & Mental Health. 2016;20(9):908–917. doi: 10.1080/13607863.2015.1055551. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Khalaila R, Litwin H. Does filial piety decrease depression among family caregivers ? Aging & Mental Health. 2011;15(6):679–686. doi: 10.1080/13607863.2011.569479. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Khalaila R, Litwin H. Changes in health behaviors and their associations with depressive symptoms among Israelis aged 50+ Journal of Aging and Health. 2014;26(263):401–421. doi: 10.1177/0898264313516997. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khvorostianov N, Remennick L. Immigration and generational solidarity: Elderly Soviet immigrants and their adult children in Israel. Journal of Intergenerational Relationships. 2015;13(1):34–50. doi: 10.1080/15350770.2015.992758. Retrieved from . [DOI] [Google Scholar]
- Kim EY, Kim KW. A theoretical framework for cognitive and non-cognitive interventions for older adults: Stimulation versus compensation. Aging & Mental Health. 2014;18(3):304–315. doi: 10.1080/13607863.2013.868404. Retrieved from . [DOI] [PubMed] [Google Scholar]
- La Fleur CG, Salthouse TA. Which aspects of social support are associated with which cognitive abilities for which people? The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2016;72(6):1006–1016. doi: 10.1093/geronb/gbv119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lavee Y, Katz R. The family in Israel: Between tradition and modernity. Marriage & Family Review. 2003;35(1/2):193–217. doi: 10.1300/J002v35n01. Retrieved from . [DOI] [Google Scholar]
- Lee HB, Richardson AK, Black BS, Shore AD, Kasper JD, Rabins PV. Race and cognitive decline among community-dwelling elders with mild cognitive impairment: Findings from the Memory and Medical Care Study. Aging & Mental Health. 2012;16(3):372–377. doi: 10.1080/13607863.2011.609533. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liao J, Muniz-Terrera G, Head J, Brunner EJ. Dynamic longitudinal associations between social support and cognitive function: A prospective investigation of the directionality of associations. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences. 2017;0(0):1–11. doi: 10.1093/geronb/gbw135. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Litwin H. Social networks and self-rated health: A cross-cultural examination among older Israelis. Journal of Aging and Health. 2006;18(3):335–358. doi: 10.1177/0898264305280982. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Litwin H. Understanding aging in a Middle Eastern context: The SHARE-Israel survey of persons aged 50 and older. Journal of Cross-Cultural Gerontology. 2009;24(1):49–62. doi: 10.1111/j.1747-0285.2012.01428.x.Identification. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Litwin H, Stoeckel KJ. Social network, activity participation, and cognition: A complex relationship. Research on Aging. 2015;38(1):76–97. doi: 10.1177/0164027515581422. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Litwin H, Stoeckel K, Roll A, Shiovitz-Ezra S, Kotte M. Social network measurement in SHARE Wave 4. In: Malter F, Borsch-Supan A, editors. SHARE Wave 4: Innovations & Methodology. Munich: MEA – Max-Planck-Institute for Social Law and Social Policy; 2013. pp. 18–37. [Google Scholar]
- McHugh Power J, Tang J, Lawlor B, Kenny RA, Kee F. Mediators of the relationship between social activities and cognitive function among older Irish adults: Results from the Irish Longitudinal Study on Ageing. Aging & Mental Health. 2018;22(1):129–134. doi: 10.1080/13607863.2016.1233935. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Ng TP, Niti M, Chiam PC, Kua EH. Ethnic and educational differences in cognitive test performance on mini-mental state examination in Asians. The American Journal of Geriatric Psychiatry. 2007;15(2):130–139. doi: 10.1097/01.JGP.0000235710.17450.9a. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Oyserman D. The lens of personhood: Viewing the self and others in a multicultural society. Journal of Personality and Social Psychology. 1993;65(5):993–1009. [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40(3):879–891. doi: 10.3758/BRM.40.3.879. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Seeman TE, Miller-Martinez DM, Stein Merkin S, Lachman ME, Tun Pa, Karlamangla AS. Histories of social engagement and adult cognition: Midlife in the U.S. study. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences. 2011;66(Suppl 1):i141–i152. doi: 10.1093/geronb/gbq091. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singelis TM, Triandis HC, Bhawuk DPS, Gelfand MJ. Horizontal and vertical dimensions of individualism and collectivism: A theoretical and measurement refinement. Cross-Cultural Research. 1995;29(3):240–275. doi: 10.1177/106939719502900302. Retrieved from . [DOI] [Google Scholar]
- Wang B, He P, Dong B. Associations between social networks, social contacts, and cognitive function among Chinese nonagenarians/centenarians. Archives of Gerontology and Geriatrics. 2015;60(3):522–527. doi: 10.1016/j.archger.2015.01.002. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Wong ST, Yoo GJ, Stewart AL. Examining the types of social support and the actual sources of support in older Chinese and Korean immigrants. International Journal of Aging & Human Development. 2005;61(2):105–121. doi: 10.2190/AJ62-QQKT-YJ47-B1T8. Retrieved from . [DOI] [PubMed] [Google Scholar]
- Zunzunegui MV, Alvarado BE, Del Ser T, Otero A. Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences. 2003;58(2):S93–S100. doi: 10.1093/geronb/58.2.S93. Retrieved from . [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.