

Abstract
Patients with non‐small cell lung cancer (NSCLC) harboring common mutations of the epidermal growth factor receptor (EGFR) are sensitive to EGFR‐tyrosine kinase inhibitors (TKI). Although forms of EGFR harboring single uncommon mutations such as G719X or L861Q are thought to be less sensitive to EGFR‐TKI, the efficacy of these drugs in patients with double uncommon mutations has remained unclear. We here present an NSCLC patient found to be positive for double uncommon EGFR mutations (G719X and L861Q) by clinical genomic sequencing analysis of a pleural effusion specimen who showed a durable response to the EGFR‐TKI afatinib. The sensitivity of EGFR with single or double uncommon mutations to afatinib and the EGFR‐TKI erlotinib was also evaluated in vitro with a visual assay based on HEK293 cells transiently transfected with expression plasmids for yellow fluorescent protein (YFP)‐tagged fragments of the EGFR intracellular domain (ICD). Whereas forms of EGFR with double uncommon mutations were more sensitive to erlotinib than were those with single uncommon mutations, those with single or double uncommon mutations were similarly sensitive to afatinib, consistent with the patient's clinical outcome. Our data support the notion that afatinib is the most suitable EGFR‐TKI for NSCLC harboring uncommon mutations of EGFR. Furthermore, the YFP‐EGFR‐ICD assay is potentially applicable to prediction of EGFR‐TKI efficacy in patients with such mutations.
Keywords: afatinib, double uncommon mutations, epidermal growth factor receptor, erlotinib, YFP‐EGFR‐ICD assay
1. INTRODUCTION
Approximately 40% of Asians with non‐small cell lung cancer (NSCLC) harbor somatic mutations in the kinase domain of the epidermal growth factor receptor (EGFR).1 Deletions in exon 19 (Ex19del) and a point mutation in exon 21 (L858R) account for approximately 90% of all EGFR mutations and are referred to as “common mutations.” Patients who harbor these common mutations manifest a marked response to EGFR‐tyrosine kinase inhibitors (TKI), whereas those positive for uncommon EGFR mutations are thought to be less sensitive to these drugs. The frequency of such uncommon mutations among individuals with EGFR‐mutated NSCLC has been estimated at 4%‐13%.1
A recent clinical study showed that not only NSCLC patients with common mutations but also those with uncommon mutations of EGFR responded to afatinib, an irreversible, second‐generation EGFR‐TKI.2 Most double EGFR mutations are combinations of common and uncommon mutations, with double uncommon mutations being relatively rare.3 It has, thus, remained unclear whether patients with double uncommon mutations differ in their sensitivity to EGFR‐TKI compared with those with single mutations. We here describe an NSCLC patient with double uncommon mutations of EGFR who showed a marked response to afatinib. To investigate the sensitivity of EGFR harboring single or double uncommon mutations to EGFR‐TKI, we performed an in vitro assay based on the expression of yellow fluorescent protein (YFP)‐tagged fragments of the EGFR intracellular domain (YFP‐EGFR‐ICD).
2. MATERIALS AND METHODS
Plasmids encoding YFP‐tagged fragments of EGFR‐ICD containing single or double mutations were generated as described previously.4, 5, 6 Constructs were confirmed by DNA sequencing. HEK293 cells (5.0 × 104 per well) were seeded in 24‐well plates, transfected for 30 hours with 500 ng of plasmid DNA with the use of Lipofectamine 3000 (Thermo Fisher Scientific, Waltham, MA, USA),5 and then exposed to erlotinib (Cayman Chemical, Ann Arbor, MI, USA) or afatinib (Selleck Chemicals, Houston, TX, USA) in culture medium at 37°C for 6 hours. The distribution of YFP‐EGFR‐ICD fluorescence was then examined with a BZ‐8100 fluorescence microscope (Keyence, Osaka, Japan). The proportion of cells with fibril‐like structures was scored for 100 cells for each condition.
3. RESULTS
3.1. Case report
A 43‐year‐old Japanese man with a smoking history of 30 pack‐years presented with chest discomfort and was diagnosed with stage IV (cT2aN0M1a) adenocarcinoma of the lung. Genomic analysis of a pleural effusion specimen revealed the presence of double uncommon EGFR mutations (G719X in exon 18 and L861Q in exon 21). Computed tomography (CT) revealed a 24‐mm nodule in the lower left lobe of the lung and left pleural effusion. Treatment with afatinib was initiated at 40 mg daily. After 1 month, a CT scan showed a prominent reduction in the size of the nodule in the lower left lobe and the disappearance of left pleural effusion (Figure 1A, B). The patient's serum concentration of carcinoembryonic antigen (CEA) had decreased from 162.6 to 7.3 ng/mL at 5 months after the onset of afatinib treatment (Figure 1C). At the time of writing of this report, the patient had continued to receive afatinib without dose reduction for 10 months and showed sustained tumor shrinkage.
Figure 1.
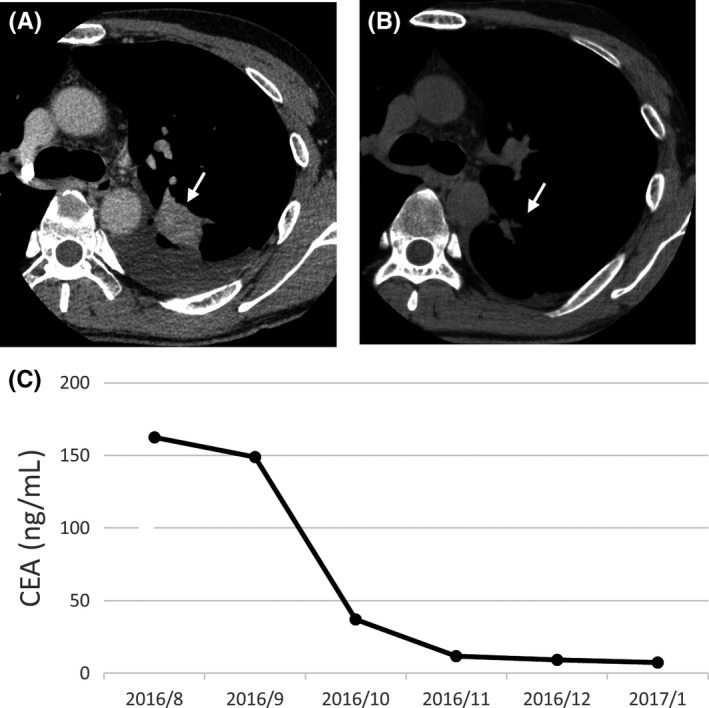
Clinical course of the patient. A, B, Computed tomography scans of the chest showing the primary mass (arrow) in the lower left lobe of the lung immediately before (A) and 1 month after (B) the onset of afatinib treatment. C, Time course (year/month) of serum CEA concentration from the onset of afatinib treatment
3.2. Sensitivity of epidermal growth factor receptor with double uncommon mutations to epidermal growth factor receptor‐tyrosine kinase inhibitors
To evaluate the sensitivity of EGFR mutants to EGFR‐TKI, we adopted an assay based on cells expressing YFP‐EGFR‐ICD. YFP‐EGFR‐ICD fusion proteins form fibril‐like structures on exposure to EGFR‐TKI in a manner that is thought to reflect sensitivity to these drugs. Consistent with our previous findings,5, 6 the formation of such fibril‐like structures was observed in HEK293 cells transfected with an expression plasmid for an Ex19del mutant of EGFR and then exposed to 100 nmol/L erlotinib or 10 nmol/L afatinib, whereas such an effect was not apparent in cells expressing EGFR (Ex19del) with an additional TKI resistance‐conferring T790M mutation (Figure 2). We then investigated the effects of EGFR‐TKI on cells expressing EGFR with single (G719A, G719S or L861Q) or double (G719A/L861Q or G719S/L861Q) uncommon mutations. In the case of erlotinib, EGFR (G719A) formed fibril‐like structures in a concentration‐dependent manner between 100 and 500 nmol/L, whereas the G719S and L861Q mutants did so at drug concentrations between 50 and 200 nmol/L. In contrast, the G719A/L861Q and G719S/L861Q double mutants formed complete fibril‐like structures in the presence of erlotinib at 50‐100 nmol/L (Figure 3A, B). These results thus suggested that EGFR with double uncommon mutations is more sensitive to erlotinib compared with EGFR harboring the corresponding single uncommon mutations and that erlotinib sensitivity is dependent on the type of uncommon mutation. In the case of afatinib, both single and double mutants formed fibril‐like structures in the presence of 5.0 nmol/L drug concentration (Figure 3C, D), suggesting that both types of mutant EGFR are similarly sensitive to afatinib.
Figure 2.
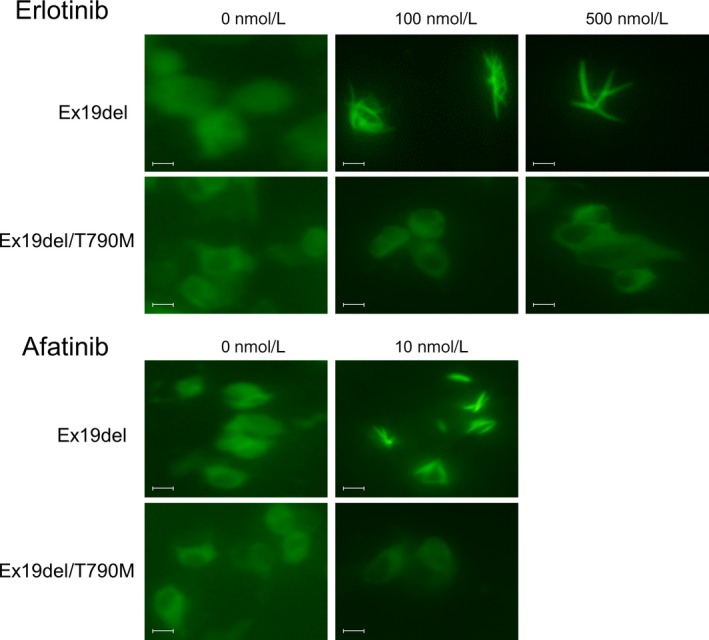
Sensitivity of Ex19del and Ex19del/T790M mutant forms of epidermal growth factor receptor (EGFR) to EGFR‐tyrosine kinase inhibitors. HEK293 cells expressing yellow fluorescent protein‐EGFR‐intracellular domain mutants were exposed to erlotinib or afatinib at the indicated concentrations for 6 h, after which the cells were examined by fluorescence microscopy. Scale bars, 10 μm
Figure 3.
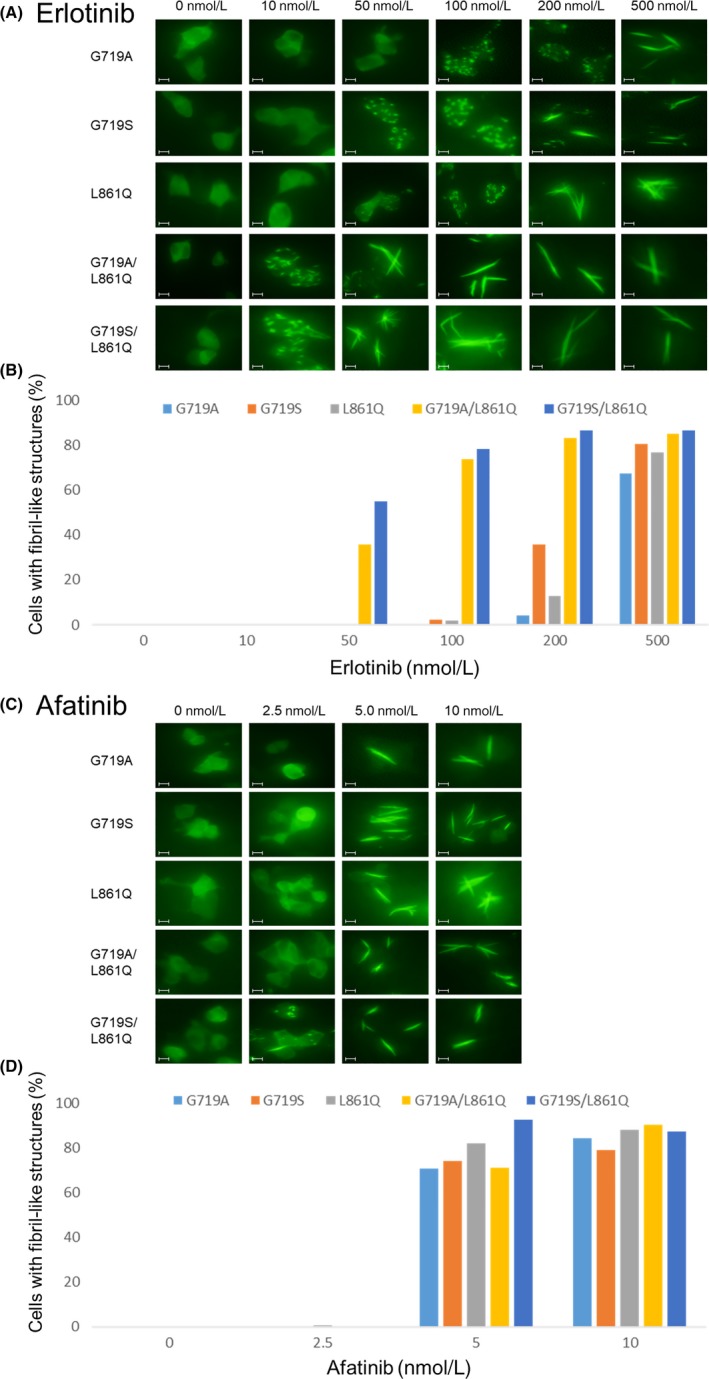
Sensitivity of epidermal growth factor receptor (EGFR) with single or double uncommon mutations to EGFR‐tyrosine kinase inhibitors. A, C, HEK293 cells expressing G719A, G719S, L861Q, G719A/L861Q or G719S/L861Q mutant forms of yellow fluorescent protein‐EGFR‐intracellular domain were exposed to erlotinib (A) or afatinib (C) at the indicated concentrations for 6 h and then examined by fluorescence microscopy. Scale bars, 10 μm. B, D, Proportion of cells with fibril‐like structures for cells exposed to erlotinib (B) or afatinib (D) as in (A) and (C), respectively
4. DISCUSSION
Previous clinical reports have found that patients with NSCLC harboring uncommon mutations of EGFR tend to be less sensitive to reversible (first‐generation) EGFR‐TKI compared with those positive for common EGFR mutations.7 However, subset analysis of the LUX‐Lung 3 and LUX‐Lung 6 trials showed that the objective response rate for the second‐generation EGFR‐TKI afatinib was 77.8% and 56.3% in patients with G719X or L861Q mutations of EGFR, respectively.2 In vitro studies found that EGFR with a single G719X mutation was more sensitive to second‐generation than to first‐generation or third‐generation EGFR‐TKI, and that EGFR with a single L861Q mutation was sensitive to both second‐generation and third‐generation EGFR‐TKI.1, 7 These data thus suggest that afatinib is the most appropriate EGFR‐TKI for NSCLC harboring uncommon mutations of EGFR. However, the efficacy of afatinib in patients with double uncommon mutations of EGFR has not been clear.
As far as we are aware, the successful treatment of only 1 other patient with double uncommon mutations of EGFR with afatinib has been previously reported.8 In that report, the inhibitory effect of afatinib on the receptor mutant (L858M/L861Q) was confirmed by immunoblot analysis of EGFR phosphorylation. In our assay, the concentration of erlotinib capable of inducing formation of fibril‐like structures by EGFR with uncommon mutations was dependent on the type and number of mutations. However, the concentration dependence of fibril formation induced by afatinib was similar for EGFR with single or double uncommon mutations. The present and previous8 studies thus indicate that afatinib is a satisfactory treatment option for NSCLC patients with double uncommon mutations of EGFR.
We examined the sensitivity of EGFR mutants to EGFR‐TKI with the use of an assay based on YFP‐EGFR‐ICD expression. Assays based on measurement of cell viability or immunoblot analysis of EGFR phosphorylation have been widely adopted for evaluation of EGFR‐TKI sensitivity. However, these assays require a homogeneous population of stably transfected cells, the generation of which is time‐consuming. In contrast, the YFP‐EGFR‐ICD assay allows both the use of transiently transfected cells and quantitative measurement of EGFR activity on a single‐cell basis. We previously investigated the EGFR‐TKI sensitivity of EGFR harboring common or single uncommon mutations with this assay and found that the results reflected the clinical outcome.5 The increasing application of genomic sequencing to NSCLC patients is likely to reveal new combinations of EGFR mutations. A simple cellular assay such as that based on YFP‐EGFR‐ICD expression will, thus, be required to evaluate the effects of EGFR‐TKI on such mutant forms of the receptor.
In conclusion, we here presented the case of a patient harboring double uncommon mutations of EGFR who showed a marked response to afatinib treatment. The efficacy of afatinib for EGFR harboring such double mutations was confirmed with an assay based on YFP‐EGFR‐ICD expression.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
Kimura S, Tanaka K, Harada T, et al. Sensitivity of epidermal growth factor receptor with single or double uncommon mutations to afatinib confirmed by a visual assay. Cancer Sci. 2018;109:3657–3661. 10.1111/cas.13787
REFERENCES
- 1. Kobayashi Y, Mitsudomi T. Not all epidermal growth factor receptor mutations in lung cancer are created equal: perspectives for individualized treatment strategy. Cancer Sci. 2016;107:1179‐1186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Yang JC, Sequist LV, Geater SL, et al. Clinical activity of afatinib in patients with advanced non‐small‐cell lung cancer harbouring uncommon EGFR mutations: a combined post‐hoc analysis of LUX‐Lung 2, LUX‐Lung 3, and LUX‐Lung 6. Lancet Oncol. 2015;16:830‐838. [DOI] [PubMed] [Google Scholar]
- 3. Kim EY, Cho EN, Park HS, et al. Compound EGFR mutation is frequently detected with co‐mutations of actionable genes and associated with poor clinical outcome in lung adenocarcinoma. Cancer Biol Ther. 2016;17:237‐245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. de Gunst MM, Gallegos‐Ruiz MI, Giaccone G, Rodriguez JA. Functional analysis of cancer‐associated EGFR mutants using a cellular assay with YFP‐tagged EGFR intracellular domain. Mol Cancer. 2007;6:56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Furuyama K, Harada T, Iwama E, et al. Sensitivity and kinase activity of epidermal growth factor receptor (EGFR) exon 19 and others to EGFR‐tyrosine kinase inhibitors. Cancer Sci. 2013;104:584‐589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Harada T, Lopez‐Chavez A, Xi L, Raffeld M, Wang Y, Giaccone G. Characterization of epidermal growth factor receptor mutations in non‐small‐cell lung cancer patients of African‐American ancestry. Oncogene. 2011;30:1744‐1752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Banno E, Togashi Y, Nakamura Y, et al. Sensitivities to various epidermal growth factor receptor‐tyrosine kinase inhibitors of uncommon epidermal growth factor receptor mutations L861Q and S768I: what is the optimal epidermal growth factor receptor‐tyrosine kinase inhibitor? Cancer Sci. 2016;107:1134‐1140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Saxon JA, Sholl LM, Janne PA. EGFR L858M/L861Q cis mutations confer selective sensitivity to afatinib. J Thorac Oncol. 2017;12:884‐889. [DOI] [PMC free article] [PubMed] [Google Scholar]