

Abstract
Background.
This study examined alternative models for how negative and positive urgency influence the relationship between depressive symptoms and alcohol and cannabis use in a community sample
Methods.
Participants included adults (n = 675; age = 42.57, SD = 15.66; 65.0% female; 74.2% White) in the community sample from the Rockland Project by the Nathan Kline Institute. Path analyses were conducted
Results.
Negative urgency was a unique mediator in the relationship between depressive symptoms and problematic alcohol use (β =.121, 95% CI = .060 – .182) and problematic cannabis use (β =.120, 95% CI = .060 – .179). Negative and positive urgency significantly moderated the relationship between depressive symptoms and problematic cannabis use (negative urgency: β = .092, 95% CI = .040 – .145; positive urgency: β = .070, 95% CI = .022 – .119), such that the relationship was positive at high levels and negative at low levels of urgency. The patterns and levels of the relationships between depressive symptoms and cannabis use differed between negative and positive urgency. Neither urgency trait moderated the relationship between depressive symptoms and problematic alcohol use.
Conclusions.
Despite being strongly related, negative and positive urgency have distinct roles in the relationship between depressive symptoms and problematic alcohol and cannabis use. Previous finding with younger samples that do not include both traits in the model at time generalize and at other times do not replicate, which warrants the continued examination of how these traits impart risk across the lifespan.
Keywords: negative urgency, positive urgency, alcohol use, cannabis use, depression
1. Introduction
Depression, and alcohol and cannabis use disorders are prevalent in the general population, with lifetime prevalence rates of 16.6% (Kessler et al., 2012, 2005), 29.1% (Grant et al., 2015), and 6.3% (Hasin et al., 2016) respectively. Depression frequently co-occurs with both alcohol and cannabis use disorders (Grant et al., 2015, 2004; Hasin et al., 2016); understanding factors influencing the relationship between depressive symptoms and problematic alcohol and cannabis use is important for prevention and intervention.
Negative and positive urgency (i.e., the tendency to act rashly under extreme negative and positive emotions, respectively) are impulsive personality traits that are prime candidates that may influence the relationship between depressive symptoms and problematic alcohol and cannabis use. First, positive and negative urgency are implicated in depression (Berg et al., 2015; Carver et al., 2013; Marmorstein, 2013). Importantly, in a longitudinal study, urgency (i.e., the higher order construct of urgency traits) at elementary school predicted higher levels of depressive symptoms 12 months later (Smith et al., 2013), suggesting that urgency is a risk factor for the development of or increase in depressive symptoms over time. Second, negative and positive urgency are implicated in both alcohol and cannabis use, but do show some specific patterns across use subtypes (Coskunpinar et al., 2013; VanderVeen et al., 2016): Both urgency traits are related to problematic alcohol use, but not frequency of use (Coskunpinar et al., 2013); both urgency traits are related to cannabis use, only positive urgency is related to problematic cannabis use (VanderVeen et al., 2016). Also, depression is more strongly related to heavy alcohol and cannabis use, than light use (Alati et al., 2005; Lev-Ran et al., 2014).
Despite these findings, the research examining the interrelationship among urgency traits, depression, and alcohol and cannabis use is relatively small. Research in young adults and adolescents indicates that negative urgency plays a mechanistic role in explaining the relationship between depressive symptoms and alcohol use, such that higher depressive symptoms are related to higher negative urgency, which in turn, is related to greater alcohol use (Gonzalez et al., 2011; Pang et al., 2014). One study failed to replicate this with cannabis use (Pang et al., 2014). Research in young adults also suggests that positive urgency may moderate the relationship between depressive symptoms and alcohol use, such that depressive symptoms are associated with negative alcohol-related consequences in individuals with higher positive urgency, but not in those with lower positive urgency (Karyadi and King, 2011).
Together, though these constructs appear to be interrelated, there are significant gaps that we address. First, it is important to include both negative and positive urgency simultaneously in these models. Negative and positive urgency are highly intercorrelated (r’s ~ .5–.8 across studies); models only including one or the other fail to account for the general effect of urgency and lack specificity with regards to valence (i.e., positive or negative emotions), which might explain inconsistencies in the literature. Second, there is a great need to examine the generalizability of these relationships among the general population. The majority of research has been conducted in adolescents and young adults; the findings might not generalize to older, more heterogeneous adult samples (Argyriou et al., 2018). A recent measurement invariance study supported the validity of examining urgency across the adult lifespan, making it possible to examine negative and positive urgency in adults with a wide age range (Argyriou, Um, Wu, & Cyders, under review).
In the current study, we test a series of competing, although not mutually exclusive, mediation and moderation models suggested by theory and previous empirical data to better understand the relationship among urgency, depressive symptoms, and problematic alcohol and cannabis use. First, we test concurrent mediation models in which positive and negative urgency are mediators of the relationship between depressive symptoms and alcohol or cannabis use (as supported by Gonzalez et al., 2011; Pang et al., 2014). Although personality traits, such as urgency, are thought to be more stable attributes, they do change across the lifespan (Argyriou et al., 2018; Littlefield et al., 2016, 2009) and have been shown to change in response to depressive symptoms (Riley et al., 2016). Given that depressive symptoms are often experienced repeatedly throughout life, the idea that one’s personality changes in response to this, explaining the relationship between such symptoms and alcohol and cannabis use, is viable (Littlefield et al., 2016, 2012, 2009). Second, we test moderation models examining negative and positive urgency as moderators of the relationship between depressive symptoms and problematic alcohol and cannabis use (as supported by Karyadi and King, 2011). This model is also viable – urgency traits are theorized to influence risk-taking behaviors, such as alcohol and cannabis use, under extreme emotional states. Previous literature suggests that individuals with depression experience more daily negative emotions and are more reactive to pleasant events in their daily life (Bylsma et al., 2011; Peeters et al., 2003), which provides an ideal context in which negative and positive urgency to operate. It may be that depressive symptoms are more stronlgy tied to alcohol and cannabis use among those high in urgency traits.
We examine these models in a large community-based sample of adults aged 18 – 71 in order to characterize these relationships in the general population using path analyses in structural equation modeling (SEM). Examining both mediation and moderation models enables the differentiation of important pathways in which urgency plays distinct roles in imparting risk for problematic alcohol and cannabis use. We test the effect of one urgency trait, while accounting for the other urgency trait, due to the high shared variance between them and in order to provide more specificity in these model patterns.
2. Materials and Methods
2.1. Data
The de-identified data were extracted from the publicly available, large-scale community sample from the Rockland County, NY collected through the Rockland Project by the Nathan Kline Institute (Nooner et al., 2012). The community sample closely resembled U.S. demographics and therefore, exclusion criteria were minimal to maximize representativeness. Any individual who was willing to participate within the age range (between 6 – 85) was enrolled in the study (i.e., there were no other inclusion or exclusion criteria), and recruitment bias was controlled with zip code-based recruitment with efforts to avoid over-representation of any community to match the representation of Rockland County that resembles U.S. demographics. The Institutional Review Board at the Nathan Kline Institute and Montclair State University approved the study and informed consent was obtained from participants; the current analysis was exempt from human subject review.
2.2. Participants
Our sample included 675 participants who were 18 years or older (mean age = 42.57 years, SD = 15.66; 65.0% female; 74.2% White; see Table 1). All participants included completed measures used in this study as a part of Rockland Project protocol. We included all individuals from the Rockland data who were 18 years old or older and who completed measures of key constructs (i.e., depressive symptoms, urgency traits, and problematic alcohol and cannabis use).
Table 1.
Participant characteristics (n = 675)
| Mean (SD; range) or % | |
|---|---|
| Demographics | |
| Age | 42.57 (15.66; 18 – 71) |
| 18–30 years | 30.7% |
| 31–60 years | 54.4% |
| Over 61 years | 15.0% |
| Gender | |
| Female | 65.0% |
| Male | 35.0% |
| Ethnicity | |
| White | 74.2% |
| Black | 16.7% |
| Asian | 4.9% |
| American Indian | 1.2% |
| Other ethnicities | 3.0% |
| Marital Status | |
| Married | 40.7% |
| Widowed | 1.8% |
| Divorced or separated | 15.3% |
| Never Married | 40.3% |
| Household Income | |
| Less than $34,999 | 19.9% |
| $35,000 – $99,999 | 36.4% |
| $100,000 or more | 42.1% |
| Education Level | |
| Less than high school | 1.5% |
| High school diploma | 10.5% |
| Partial college | 30.5% |
| College degree | 29.2% |
| Graduate degree | 25.6% |
| Occupation | |
| Unskilled workers, students, & housewives | 11.6% |
| Semi-skilled workers & small business owners | 44.0% |
| Administrators, professionals, & business proprietors | 42.0% |
| Urgency | |
| Negative Urgency | 1.97 (0.56; 1.00 – 3.83) |
| Positive Urgency | 1.52 (0.50; 1.00 – 3.71) |
| Depression symptoms | |
| BDI-II, total score | 6.14 (7.06; 0.00 – 44.00) |
| Minimal depression (0–13) | 87.6% |
| Mild depression (14–19) | 6.7% |
| Moderate depression (20–28) | 3.6% |
| Severe depression (29–63) | 1.8% |
| Substance use | |
| Alcohol | |
| No lifetime alcohol use | 13.5% |
| ASSIST alcohol involvement | 4.02 (4.47; 0 – 34) |
| Lower risk | 93.0% |
| Moderate risk | 5.8% |
| High risk | 0.2% |
| Age of first use* | 17.07 (3.64) |
| Years of use* | 17.83 (16.00) |
| Cannabis | |
| No lifetime cannabis use | 35.6% |
| ASSIST cannabis involvement | 2.11 (4.87; 0 – 39) |
| Lower risk | 82.9% |
| Moderate risk | 16.6% |
| High risk | 0.5% |
| Age of first use* | 17.87 (4.06) |
| Years of use* | 5.99 (9.53) |
Notes. BDI-II = Beck Depression Inventory-II; ASSIST = Alcohol, Smoking and Substance Involvement Screening Test;
includes individuals who reported lifetime use
2.3. Measures
2.3.1. UPPS-P Impulsive Behavior Scale (UPPS-P; Lynam et al., 2006)
The UPPS-P is a 59-item self-report assessment of five distinctive impulsive personality traits. Only negative and positive urgency subscales were used in this study. Responses range from 1 (agree strongly) to 4 (disagree strongly). Items were reverse scored and means were calculated per scoring instructions so that higher scores indicate higher urgency. Both negative urgency (Cronbach’s α = .87) and positive urgency (Cronbach’s α = .91) showed excellent reliability in the current sample.
2.3.2. Beck Depression Inventory-II (BDI-II; Beck, Steer, & Brown, 1996)
BDI-II is a 21-item self-report questionnaire assessing depressive symptoms. Responses range from 0 to 3 and higher total scores indicate greater depressive symptoms. The reliability of BDI-II in the current sample was excellent (Cronbach’s α = .91). Depressive symptoms (a continuous variable) was chosen rather than a dichotomous diagnosis (yes/no depression) to increase variability and thus increase predictive power.
2.3.3. Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST; Heslop, Ross, Osmond, & Wynaden, 2010)
The ASSIST is a screening measure for problematic substance use developed by the World Health Organization. A set of 8 items assesses problematic substance use (tobacco, alcohol, cannabis, cocaine, stimulants, sedatives and sleeping pills, hallucinogens, inhalants, opioids and other drugs). The first item assesses lifetime use of a given drug. If lifetime use is present, the following items assess frequency, craving, health/social/legal/financial problems, failure to perform daily responsibilities, expression of concern from friends/relatives/others, and failure to cut down the drug use over the past three months. The total subscale scores range from 0 to 39. Alcohol and cannabis subscales that were used in the current study showed acceptable reliability (Cronbach’s α = .77 for alcohol; Cronbach’s α = .61 for cannabis). Other substances were not included due to low base rates of lifetime use (< 25% of the sample), with even lower rates of non-zero subscale total scores.
2.4. SEM Statistical Analysis Plan
First, we conducted a confirmatory factor analysis estimated using maximum likelihood (ML) in Mplus8 (Muthén and Muthén, 2017) with two latent variables (negative and positive urgency) to examine the model fit before constructing the full path model. Because urgency items are ordinal (1 = agree strongly to 4 = disagree strongly), we parceled items to create four indicators in each latent factor with a mean of three or four items to make them continuous and suitable for ML (Little et al., 2002). The model fit was evaluated using Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Standardized Root Mean Square Residual (SRMR) (Hu and Bentler, 1999) because the χ2 statistic is sensitive to a large sample size (Kline, 2016).
Next, we conducted a SEM path analysis estimated using ML that identified latent and observed variables while covarying for age, gender, and race. We defined two latent variables using the negative and positive urgency parcels as indicators by fixing the loading of the first parcel in each factor to 1. The BDI total scores and ASSIST problematic alcohol and cannabis use subscale scores were included as observed variables. We examined pathways from depressive symptoms to the urgency traits to problematic alcohol and cannabis use in a concurrent (i.e., cross-sectional) model.
Finally, two SEM moderation analyses estimated with ML were conducted using Mplus8 (Muthén and Muthén, 2017). We defined variables as described above. In each model, one urgency trait was considered as a moderator in the relationship between depressive symptoms and problematic alcohol and cannabis use, while controlling for the effects of the other trait. The interaction was probed at three levels of each urgency trait, at 1 SD below the mean (low), at the mean, and at 1 SD above the mean (high). Because Mplus does not produce traditional model fit indices for latent variable interactions, we evaluated the model fit using the two step procedure suggested by Maslowsky and colleagues (2015). First, traditional model fit indices are obtained from a model without the interaction. Second, the models with and without the interaction are compared using a log-likelihood ratio test that calculates a log-likelihood difference value, D. This test statistic is approximately distributed as χ2 with the degree of freedom (df) of 1 (as there is one additional free parameter in our model with interaction) to determine the significance. If the test is significant (p < .001), the model without interaction has a significant loss of fit relative to the model with interaction.
Results
3.1. Preliminary analyses
The preliminary analysis was conducted using SPSS (IBM Corp, 2016). The variables were normally distributed except problematic cannabis use, which exceeded skewness (< 3) and kurtosis (< 10) guidelines (Kline, 2016). Therefore, log-transformed problematic cannabis use scores were used in the subsequent analyses. Missing race categorical data (0.00005% of data) were missing at random and were imputed with the mode of all sample. Missing continuous data (0.00005% of data) were missing at random and were imputed using Full Information Maximum Likelihood (FIML) in Mplus8 (Muthén and Muthén, 2017). The initial relationships among study variables and demographic variables were examined with Pearson’s correlation analyses. Sample characteristics are presented in Table 1; relationships among variables are described in Table 2.
Table 2.
Bivariate correlations
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1 Age | |||||||
| 2 Female sex | 0.12** | ||||||
| 3 Non-white race | −0.26** | −0.10** | |||||
| 4 NUR | −0.13** | −0.01 | −0.07 | ||||
| 5 PUR | −0.20** | −0.17** | 0.06 | 0.69** | |||
| 6 BDI-II total score | −0.01 | 0.03 | −0.05 | 0.43** | 0.27** | ||
| 7 ASSIST-Alcohol | −0.03 | −0.07 | −0.17** | 0.21** | 0.14** | 0.11** | |
| 8 ASSIST-Cannabis | −0.27** | −0.19** | 0.06 | 0.22** | 0.19** | 0.11** | 0.19** |
Notes. Female sex coded as 1: Male sex coded as 0; Non-white race coded as 1: White race coded as 0; NUR = negative urgency; PUR = positive urgency; BDI-II = Beck Depression Inventory; ASSIST = Alcohol, Smoking, and Substance Involvement Screening Test
p < .05
p < .00
3.2. SEM Analyses
3.2.1. Mediation models
The model fit of the confirmatory factor analysis of the two urgency traits was good (χ2(19) = 105.220, p < .001; RMSEA = .082, CFI = .979, TLI = .970, SRMR = .033). The model fit of the concurrent path model using negative and positive urgency as mediators was good (χ2(61) = 221.597, p < .001; RMSEA = .062, CFI = .965, TLI = .951, SRMR = .059; Table 3, Figure 1). There were significant indirect effects of depressive symptoms on problematic alcohol and cannabis use via negative urgency (β = .121, 95% Confidence Interval (CI) = .060 – .182; β = .120, 95% CI = .060 – .179, respectively), but not via positive urgency (β = −.023, 95% CI = −.056 – .010; β = −.026, 95% CI = −.058 – .007, respectively). Greater depressive symptoms were related to higher negative urgency (β = .466, 95% CI = .412 – .519), and higher negative urgency was related to higher problematic alcohol and cannabis use (β = .260, 95% CI = .133 – .386; β = .257, 95% CI = .134 – .379, respectively). However, positive urgency was a significant mediator in the relationship between depression and alcohol and cannabis use when negative urgency was not included concurrently in the model (Fit indices: χ2(23) = 71.092, p < .001; RMSEA = .056, CFI = .980, TLI = .966, SRMR = .066; β = .028, 95% CI = .008 – .049; β = .025, 95% CI = .005 – .045, respectively). Greater depression symptoms were related to higher positive urgency (β = .284, 95% CI = .223 – .344) and higher positive urgency was related to higher problematic alcohol and cannabis use (β = .099, 95% CI = .031 – .168; β = .089, 95% CI = .021 – .156, respectively). The patterns of results remained unchanged for negative urgency as a mediator when positive urgency was not included concurrently in the model
Table 3.
SEM concurrent mediation analyses
| X | M | Y | Indirect Effects (standardized β) |
Standardized SE |
95% CI |
|---|---|---|---|---|---|
| Depressive symptoms → Urgency traits → Problematic use | |||||
| Fit Indices: χ2(61) = 221.597, p < .001; RMSEA = .062, CFI = .965, TLI = .951, SRMR = .059 | |||||
| Depressive symptoms | Negative urgency | Problematic alcohol use | .121 | .037 | .060 – .182* |
| Problematic cannabis use | .120 | .036 | .060 – .179* | ||
| Positive Urgency | Problematic alcohol use | −.023 | .020 | −.056 – .010 | |
| Problematic cannabis use | −.026 | .020 | −.058 – .007 | ||
| Problematic alcohol use | |||||
| Direct effects | Depressive symptoms | .008 | .044 | −.064 – .080 | |
| Covariate effects | Age | −.049 | .039 | −.113 – .016 | |
| Gender | −.084 | .038 | −.147 – −.022* | ||
| Race | −.179 | .038 | −.242 – −.115* | ||
| Problematic cannabis use | |||||
| Direct effects | Depressive symptoms | .025 | .042 | −.045 – .095 | |
| Covariate effects | Age | −.227 | .037 | −.288 – −.165* | |
| Gender | −.171 | .037 | −.231 – −.111* | ||
| Race | −.002 | .038 | −.064 – .061 | ||
Figure 1.

SEM path analysis of the indirect effect of depressive symptoms on problematic use through negative and positive urgency.
3.2.2. Moderation models
First, the model without the interaction between negative urgency and depressive symptoms was estimated. This model fit the data well (χ2(55) = 153.538, p < .001; RMSEA = .052, CFI = .978, TLI = .966, SRMR = .026). Next, the model with the interaction was compared with the model without. The log-likelihood difference value, D = 33.956 with a df of 1, was significant (p < .001) indicating the model with the interaction had a better fit than the model without the interaction. The relationship between depressive symptoms and problematic alcohol use was not significantly moderated by negative urgency (β = −.014, 95% CI = −.067 – .038; Table 4). The relationship between depressive symptoms and problematic cannabis use was significantly moderated by negative urgency (β = .092, 95% CI = .040 – .145; Table 4, Figure 2). The relationship between depressive symptoms and problematic cannabis use was significantly negative at the low level (B = −.012, 95% CI = −.020 – −.003), was unrelated at the mean (B = −.002, 95% CI = −.007 – .002), and significantly positive at the high level of negative urgency (B = .007, 95% CI = .002 – .012). The moderation analysis was also conducted without controlling for positive urgency; the pattern of results remained unchanged.
Table 4.
SEM moderation analysis: Relationship between depression and problematic alcohol and cannabis use moderated by negative urgency
| Predictor | Standardized b | Standardized SE | 95% CI |
|---|---|---|---|
| Problematic Alcohol Use | |||
| Intercept | 1.237 | .132 | 1.019 – 1.445* |
| Depression Symptoms | .019 | .050 | −.063 – .101 |
| Negative Urgency | .272 | .081 | .139 – .404* |
| Positive Urgency | −.079 | .073 | −.198 – .041 |
| Interaction: Negative Urgency x Depression Symptoms |
−.014 | .032 | −.067 – .038 |
| Age | −.044 | .039 | −.109 – .020 |
| Gender | −.092 | .039 | −.156 – −.029* |
| Race | −.171 | .039 | −.235 – −.107* |
| Problematic Cannabis Use | |||
| Intercept | 1.441 | .121 | 1.241 – 1.640* |
| Depression Symptoms | −.045 | .049 | −.125 – .035 |
| Negative Urgency | .194 | .079 | .063 – .324* |
| Positive Urgency | −.126 | .071 | −.242 – −.009* |
| Interaction: Negative Urgency x Depression Symptoms |
.092 | .032 | .040 – .145* |
| Age | −.226 | .037 | −.288 – −.165* |
| Gender | −.178 | .037 | −.239 – −.117* |
| Race | .007 | .038 | −.056 – .070 |
Figure 2.

Conditional effects of depressive symptom severity on problematic cannabis use, moderated by negative urgency
The model with the interaction between positive urgency and depressive symptoms was estimated. The log-likelihood difference value, D = 31.092 with a df of 1, was significant (p < .001) indicating the model with the interaction has a better fit than the model without. The relationship between depressive symptoms and problematic alcohol use was not significantly moderated by positive urgency (β = −.016, 95% CI = −.065– .033; Table 5). However, the relationship between depressive symptoms and problematic cannabis use was significantly moderated by positive urgency (β = .070, 95% CI = .022 – .119; Table 5, Figure 3). The relationship between depressive symptoms and problematic cannabis use was significantly negative at the low level (B = −.009, 95% CI = −.017 – −.001), was unrelated at the mean (B = −.001, 95% CI = −.005 – .003), and significantly positive at the high level of positive urgency (B = .008, 95% CI = .002 – .014). The moderation analysis was also conducted without controlling for negative urgency; the results remained unchanged.
Table 5.
SEM moderation analysis: Relationship between depression and problematic alcohol and cannabis use moderated by positive urgency
| Predictor | Standardized b | Standardized SE | 95% CI |
|---|---|---|---|
| Problematic Alcohol Use | |||
| Intercept | 1.238 | .132 | 1.020 – 1.456* |
| Depression Symptoms | .016 | .046 | −.060 – .092 |
| Negative Urgency | .257 | .079 | .128 – .386* |
| Positive Urgency | −.061 | .083 | −.198 – .076 |
| Interaction: Positive Urgency x Depression Symptoms |
−.016 | .030 | −.065 – .033 |
| Age | −.044 | .039 | −.109 – .020 |
| Gender | −.092 | .039 | −.155 – −.029* |
| Race | −.171 | .039 | −.235 – −.108* |
| Problematic Cannabis Use | |||
| Intercept | 1.434 | .122 | 1.234 – 1.635* |
| Depression Symptoms | −.012 | .045 | −.086 – .062 |
| Negative Urgency | .282 | .076 | .157 – .408* |
| Positive Urgency | −.198 | .081 | −.332 – −.064* |
| Interaction: Positive Urgency x Depression Symptoms |
.070 | .029 | .022 – .119* |
| Age | −.228 | .037 | −.289 – −.166* |
| Gender | −.176 | .037 | −.238 – −.115* |
| Race | .009 | .038 | −.053 – .072 |
Figure 3.
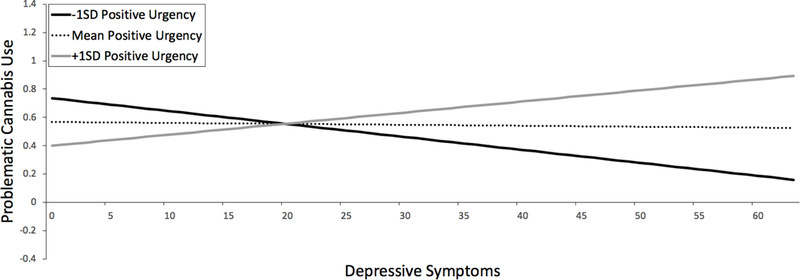
Conditional effects of depressive symptom severity on problematic cannabis use, moderated by positive urgency
Discussion
The present study sought to examine alternative models concerning how positive and negative urgency influence the relationship between depressive symptoms and problematic alcohol and cannabis use. We tested a series of concurrent path analyses using community adults with a wider age range than previous work and we also tested for effects of one urgency trait, while controlling for the other trait, in order to determine specificity in trait effects. Our study found that 1) negative, but not positive, urgency significant mediated the relationship between depressive symptoms and both problematic alcohol and cannabis use; 2) both negative and positive urgency significantly moderated the relationship between depressive symptoms and problematic cannabis use with diverging patterns; and 3) negative and positive urgency did not moderate the relationship between depressive symptoms and problematic alcohol use.
The current study supports and extends previous findings that negative urgency is a mediator between depressive symptoms and alcohol use in young adults (Gonzalez et al., 2011) and adolescents (Pang et al., 2014) to a community adults with a wider age range. Unlike in an adolescent sample (Pang et al., 2014), negative urgency mediated the relationship between depressive symptoms and problematic cannabis use. This supports that negative urgency is a prime candidate mechanism for the relationship between depressive symptoms and problematic alcohol and cannabis use.
Importantly, the current study examined negative and positive urgency in the same model, thus further solidifying the role of negative urgency in the relationship between depression and alcohol and cannabis use even after controlling for the effect of positive urgency. Interestingly, positive urgency did not exert any unique mediational effect, over and above the effect of negative urgency. However, when negative urgency was not included as a covariate, positive urgency did emerge as a significant mediator, suggesting trait specific effects that are only captured when both traits are included in the model. This suggests discriminant validity between negative and positive urgency for depressive symptom effects. Negative and positive urgency are highly correlated (r = 0.69, p < .001, in the current sample). However, given that ~90% of the variance in negative and positive urgency is reliable, this correlation magnitude suggests that about 45% of the variance in each trait is reliable and unshared with the other trait. This supports the notion that, although highly related, these two traits are indeed distinct and show important differential patterns with behaviors of risk.
Interestingly, the moderation effects tested in the present study indicate that the relationship between depressive symptoms and problematic cannabis use is moderated by both negative and positive urgency, both while controlling for the effect of the other urgency trait and without the other trait included in the model. The relationship between depressive symptoms and problematic cannabis use was significantly positive at high levels and negative at low levels of each urgency trait. Interesting, however, the intercepts in these models varied, such that positive urgency showed a crossover interaction that negative urgency did not (although the slope patterns were similar across the traits). The crossover of effects occurred at a BDI score of 20, indicative of moderate depression. Studies may fail to show a relationship between positive urgency and problematic cannabis use if depression levels are low in the sample, whereas effects might be more easily detected for negative urgency across the range of depression symptom levels.
These findings corroborate findings suggesting that higher urgency is associated greater marijuana-related problems in young adults (Dvorak and Day, 2014), but do not replicate specificity findings in a meta-analysis showing only higher positive urgency as related to greater negative cannabis use consequences in adolescents (VanderVeen et al., 2016). The results from our adult sample suggest that both negative and positive urgency are important in increasing the effect of depressive symptoms on problematic cannabis use. Interestingly, and inconsistent with previous findings (Karyadi and King, 2011), positive and negative urgency did not moderate the relationship between depressive symptoms and problematic alcohol use, suggesting such a moderation might be specific to young adult samples and that such an effect should be viewed as more tenuous in samples with a wider age range. Additionally, the pattern might be more robust for problematic use, rather than general use of alcohol and cannabis (see Coskunpinar et al, 2013 and VanderVeen et al., 2016, for two reviews on this topic that reach a similar conclusion).
The current study has some limitations. First, the measures for negative and positive urgency, depression, and alcohol and cannabis use were self-report measures. Second, we conducted SEM path analyses using cross-sectional data, so the concurrent mediation findings cannot establish a causal relationship and these should be replicated in future longitudinal work. Third, our community sample was predominantly White and female, which may limit generalizability of findings. Fourth, our community sample has a wide age range and did not examine the age-specific effects, although we did covary for age. A recent study using the same sample suggests age moderation effects in the relationship between urgency and problematic cannabis, but not alcohol, use (Argyriou et al., under review). The pattern of these results suggested more robust relationships between urgency and cannabis use among younger females (for negative urgency) and older females (for positive urgency) (Argyriou et al., under review), thus somewhat explaining differential results in the current study as compared to previous work in primarily young samples. Finally, our community sample includes adults with varying severity of depressive symptoms and problematic alcohol and cannabis use with the majority of individuals indicating minimal depressive symptoms or use of alcohol or cannabis.
4. Conclusions
In conclusion, our findings suggest that, despite being strongly related to each other, negative and positive urgency have distinct patterns of risk in influencing the relationship between depressive symptoms and alcohol and cannabis use. At times, these patterns mirror previous findings in adolescent and young adult samples (e.g., Gonzalez et al., 2011; Pang et al., 2014) and in studies in which both traits were not included in the model; however, at other times the patterns are quite different than previous work (e.g., Karyadi and King, 2011; Pang et al., 2014). We propose that continued examination of negative and positive urgency in samples with a wider age range is warranted to better understand how these traits change and impart risk across the lifespan.
Footnotes
Declarations of interest: none
References
- Alati R, Lawlor DA, Najman JM, Williams GM, Bor W, O’Callaghan M, 2005. Is there really a “J-shaped” curve in the association between alcohol consumption and symptoms of depression and anxiety? Findings from the Mater-University Study of Pregnancy and its outcomes. Addiction 100, 643–651. doi: 10.1111/j.1360-0443.2005.01063.x [DOI] [PubMed] [Google Scholar]
- Argyriou E, Um M, Carron C, Cyders MA, 2018. Age and impulsive behavior in drug addiction: A review of past research and future directions. Pharmacol. Biochem. Behav 164, 106–117. doi: 10.1016/j.pbb.2017.07.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Argyriou E, Um M, Cyders MA, n.d. Measurement invaraince of the UPPS-P Impulsive Behavior Scale across age and sex [DOI] [PubMed]
- Beck AT, Steer RA, Brown GK, 1996. Beck Depression Inventory-II (BDI-II) San Antonio, TX. [Google Scholar]
- Berg JM, Latzman RD, Bliwise NG, Lilienfeld SO, 2015. Parsing the Heterogeneity of Impulsivity: A Meta-Analytic Review of the Behavioral Implications of the UPPS for Psychopathology. Psychol. Assess 27. doi: 10.1037/pas0000111 [DOI] [PubMed] [Google Scholar]
- Bylsma LM, Taylor-Clift A, Rottenberg J, 2011. Emotional reactivity to daily events in major and minor depression. J. Abnorm. Psychol 120, 155–167. doi: 10.1037/a0021662 [DOI] [PubMed] [Google Scholar]
- Carver CS, Johnson SL, Joormann J, 2013. Major depressive disorder and impulsive reactivity to emotion: Toward a dual-process view of depression. Br. J. Clin. Psychol 52, 285–299. doi: 10.1111/bjc.12014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coskunpinar A, Dir AL, Cyders M. a., 2013. Multidimensionality in Impulsivity and Alcohol Use: A Meta-Analysis Using the UPPS Model of Impulsivity. Alcohol. Clin. Exp. Res 37, 1441–1450. doi: 10.1111/acer.12131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dvorak RD, Day AM, 2014. Marijuana and self-regulation: Examining likelihood and intensity of use and problems. Addict. Behav 39, 709–712. doi: 10.1016/j.addbeh.2013.11.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzalez VM, Reynolds B, Skewes MC, 2011. Role of impulsivity in the relationship between depression and alcohol problems among emerging adult college drinkers. Exp. Clin. Psychopharmacol 19, 303–313. doi: 10.1037/a0022720 [DOI] [PubMed] [Google Scholar]
- Grant BF, Goldstein RB, Saha TD, Chou SP, Jung J, Zhang H, Pickering RP, Ruan WJ, Smith SM, Huang B, Hasin DS, 2015. Epidemiology of DSM-5 Alcohol Use Disorder: Results from the National Epidemiologic Survey on Alcohol and Related Conditions - III. JAMA Psychiatry 72, 757–766. doi: 10.1001/jamapsychiatry.2015.0584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grant BF, Stinson FS, Dawson DA, Chou SP, Dufour MC, Compton WM, Pickering RP, Kaplan K, 2004. Prevalence and Co-Occurrence of Substance Use Disorders and Independent Mood and Anxiety Disorders on Alcohol and Related Conditions. Arch. Gen. Psychiatry 61, 807–816. [DOI] [PubMed] [Google Scholar]
- Hasin DS, Kerridge BT, Saha TD, Huang B, Pickering R, Smith SM, Jung J, Zhang H, Grant BF, 2016. Prevalence and correlates of DSM-5 cannabis use disorder, 2012–2013: Findings from the national epidemiologic survey on alcohol and related conditions-III. Am. J. Psychiatry 173, 588–599. doi: 10.1176/appi.ajp.2015.15070907 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heslop K, Ross C, Osmond B, Wynaden D, 2010. ASSIST: The alcohol, smoking and substance involvement screening test (ASSIST): Manual for use in primary care, World Health Organization. doi: 10.1007/s11469-013-9428-3 [DOI] [Google Scholar]
- Hu L, Bentler PM, 1999. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J 6, 1–55. [Google Scholar]
- IBM Corp, 2016. SPSS, Version 24.0
- Karyadi KA, King KM, 2011. Urgency and negative emotions: Evidence for moderation on negative alcohol consequences. Pers. Individ. Dif 51, 635–640. [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE, 2005. Lifetime prevelance and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey replication. Arch. Gen. Psychiatry 62, 593–602. doi: 10.1001/archpsyc.62.6.593 [DOI] [PubMed] [Google Scholar]
- Kessler RC, Petukhova M, Sampson NA, Zaslavsky AM, Wittchen H-U, 2012. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res 21, 169–184. doi: 10.1002/mpr.1359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB, 2016. Principles and practices of structural equation modeling, 4th ed. The Guilford Press, New York. [Google Scholar]
- Lev-Ran S, Roerecke M, Le Foll B, George TP, McKenzie K, Rehm J, 2014. The association between cannabis use and depression: A systematic review and meta-analysis of longitudinal studies. Psychol. Med 44, 797–810. doi: 10.1017/S0033291713001438 [DOI] [PubMed] [Google Scholar]
- Little TD, Cunningham WA, Shahar G, Widaman KF, 2002. To Parcel or Not to Parcel : Exploring the Question, Weighing the Merits. Struct. Equ. Model 9, 151–173. doi: 10.1207/S15328007SEM0902 [DOI] [Google Scholar]
- Littlefield AK, Sher KJ, Wood PK, 2009. Is “maturing out” of problematic alcohol involvement related to personality change? J. Abnorm. Psychol 118, 360–374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Littlefield AK, Stevens AK, Ellingson JM, King KM, Jackson KM, 2016. Change in negative urgency, positive urgency, and sensation seeking across adolescence. Pers. Individ. Dif 90, 332–337. doi: 10.1016/j.paid.2015.11.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Littlefield AK, Vergés A, Wood PK, Sher KJ, 2012. Transactional models between personality and alcohol involvement: A further examination. J. Abnorm. Psychol 121, 778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynam DR, Smith GT, Whiteside SP, Cyders MA, 2006. The UPPS-P: Asessing five personality pathways to impulsive behavior Purdue University, West Lafayette, IN. [Google Scholar]
- Marmorstein NR, 2013. Associations between dispositions to rash action and internalizing and externalizing symptoms in children. J. Clin. Child Adolesc. Psychol 42, 131–138. doi: 10.1080/15374416.2012.734021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maslowsky J, Jager J, Hemken D, 2015. Estimating and interpreting latent variable interactions: A tutorial for applying the latent moderated structural equations method. Int. J. Behav. Dev 39, 87–96. doi: 10.1177/0165025414552301.Estimating [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO, 2017. Mplus User’s Guide, Eighth ed. Los Angeles CA. doi: 10.2307/2234838 [DOI] [Google Scholar]
- Nooner KB, Colcombe SJ, Tobe RH, Mennes M, Benedict MM, Moreno AL, Panek LJ, Brown S, Zavitz Stephen TT, Li Q, Sikka S, Gutman D, Bangaru S, Schlachter R, Kamiel SM, Answer AR, Hinz CM, Kaplan MS, Rachlin AB, Adelsberg S, Cheung B, Khanuja R, Yan C, Craddok CC, Calhoun V, Courtney W, King M, Wood D, Cox CL, Kelly AMC, Di Martino A, Petkova E, Reiss PT, Duan N, Thomsen D, Biswal B, Coffey B, Hoptman MJ, Javitt DC, Pomara N, Sidtis JJ, Koplewicz HS, Castellanos XF, Leventhal BL, Milham MP, 2012. The NKI-Rockland sample: A model for accelerating the pace of discovery science in psychiatry. Front. Neurosci 6, 1–11. doi: 10.3389/fnins.2012.00152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pang RD, Farrahi L, Glazier S, Sussman S, Leventhal AM, 2014. Depressive symptoms, negative urgency and substance use initiation in adolescents. Drug Alcohol Depend 144, 225–230. doi: 10.1016/j.drugalcdep.2014.09.771 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peeters F, Nicolson NA, Berkhof J, Delespaul P, deVries M, 2003. Effects of daily events on mood states in major depressive disorder. J. Abnorm. Psychol 112, 203–211. doi: 10.1037/0021-843X.112.2.203 [DOI] [PubMed] [Google Scholar]
- Riley EN, Rukavina M, Smith GT, 2016. The reciprocal predictive relationship between high-risk personality and drinking: An 8-wave longitudinal study in early adolescents. J. Abnorm. Psychol 125, 798–804. doi: 10.1037/abn0000189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith GT, Guller L, Zapolski TCB, 2013. A Comparison of Two Models of Urgency: Urgency predcits both rash action and depression in youth. Clin. Psychol. Sci 1, 266–275. doi: 10.1177/2167702612470647 [DOI] [PMC free article] [PubMed] [Google Scholar]
- VanderVeen JD, Hershberger AR, Cyders MA, 2016. UPPS-P model impulsivity and marjiunana use behaviors in adolescents: A meta-analysis. Drug Alcohol Depend 168, 181–190. doi: 10.1016/j.drugalcdep.2016.09.016 [DOI] [PubMed] [Google Scholar]