

Abstract
Metacarpophalangeal pattern profile (MCPP) was determined on 16 Prader-Willi patients. Chromosome analysis of 14 patients showed an interstitial deletion of the long arm of chromosome 15 in seven subjects and normal chromosome results for the remaining individuals. Two separate and distinguishable hand profiles for each group based on the chromosome findings were identified. Correlation studies confirmed the homogeneity of the chromosome deletion group relative to the Prader-Willi individuals with normal chromosomes. Discriminant analysis of Prader-Willi versus normal individuals produces a function of three MCPP variables plus age which may provide a useful tool for diagnosis.
Keywords: Chromosome 15 deletion, correlation studies, discriminant analysis, metacarpophalangeal pattern profile (MCPP), Prader-Willi syndrome subgroups
Prader-Willi syndrome was first described in 1956 (Prader et al. 1956) and by now over 300 cases have been reported. This condition, generally sporadic in occurrence, is characterized by infantile hypotonia, early childhood obesity, mental deficiency of varying degrees, small hands and feet, and hypogonadism. Diagnosis of the condition may be difficult, particularly in the younger patient. Therefore, quantitative methods based on clinical or physical attributes in this disorder may be helpful.
Metacarpophalangeal pattern profile (MCPP) analysis is an evaluation of the hand skeleton based on a comparison of 19 tubular bone lengths to normal bone length standards, as described by Poznanski et al. (1972a) and Garn et al. (1972). The method provides a quantitative assessment of the amount and direction of dimensional alteration in the hand skeleton, relative to normal. MCPP analysis has previously been utilized in the evaluation of numerous syndromes (Poznanski et al. 1972b, 1973, Poznanski 1974, Escobar & Bixler 1977, Halal & Preus 1979) for which characteristically abnormal pattern profiles have been demonstrated.
We have recently derived a method of MCPP analysis for 16 patients diagnosed with Prader-Willi syndrome to evaluate the potential of this technique to serve as an additional diagnostic criterion of this condition.
Materials and Methods
(1) MCPP data: Postero-anterior hand radiographs were obtained for 16 patients whose clinical features [(neonatal hypotonia, neonatal feeding problems, delayed developmental milestones, mental retardation, obesity (in 75% of our patients), small hands and feet, hypogonadism, and chromosome 15 deletions (in 50% of our patients)] were consistent with the diagnosis of Prader-Willi syndrome. The diagnosis of Prader-Willi syndrome was made by at least two physicians on more than one occasion. This group included 10 males and 6 females ranging in age from 2 weeks to 24 years, with a mean age of 11.1 years.
The metacarpophalangeal bone lengths of each patient were measured with a Boley gauge and compared to bone length standards (appropriate for age and sex) published by Garn (Garn et al. 1972 – white Americans, age 2 years to adulthood) and Poznanski (Poznanski 1974–Gefferth Hungarian sample, birth to 15 months). Through these comparisons, Z score values for the 19 bones of each patient were obtained (Z score = observed bone length minus mean bone length divided by the standard deviation associated with the particular age and sex of normal standards). The MCPP for a given patient is, therefore, the set of 19 Z scores, which may be plotted on a graph or subjected to various statistical methods for study and comparison with the MCPP of other patients, or groups of patients (Poznanski et al. 1972a).
(2) Correlation studies: A “mean” pattern profile, based on the average Z score for each bone, of 16 patients was derived (Poznanski et al. 1972a, Garn et al. 1972). The pattern of each patient was compared to this mean pattern via a correlation program which produces a Pearsonian r value (correlation coefficient).
(3) Discriminant analysis: A forward step-wise method of discriminant analysis (Enslein et al. 1977) was performed on the 19 Z scores and the age of individuals from two groups: the 16 patients with Prader-Willi syndrome and a control group of 41 normal subjects whose hand radiographs were randomly obtained from the records of Indiana University School of Dentistry, Department of Orthodontics. Age was considered as a possible discriminating variable after it was found in the Prader-Willi group that age was negatively correlated with each of the 19 Z score variables, thus indicating a slowing down in hand bone growth relative to normal individuals, as has been noted by Smith (1976). The sample of 41 normals included 17 males and 24 females, with an age range of 9.5 to 18 years and a mean age equal to 13.1 years.
(4) Prometaphase chromosome analysis of 14 Prader-Willi individuals was also performed and seven individuals had an interstitial deletion of the long arm of chromosome 15 (bands q11 to q13), consistent with the deletion reported by Ledbetter et al. (1981). Detailed chromosome analysis will be published elsewhere. Seven individuals had normal chromosomes. In order to identify differences, if any, in the hand profile, a second series of correlation and discriminant analyses was undertaken between the two groups of Prader-Willi individuals.
Results
The mean pattern profile based on the 16 patients with Prader-Willi syndrome is essentially flat without obvious vertical deviations (Fig. 1). The mean Z scores fall between −1 and −2.5. Any Z score of −0.5 or lower is significantly different from zero; therefore each hand bone is significantly shorter at the 5% level. From the profile, it appears that the distal hand bones are shorter than the proximal bones. The mean Z scores of the two groups of Prader-Willi individuals based on the chromosome results (deletion or non-deletion) showed two separate distinguishable profiles (Fig. 1). When the curves are 1.1 or further apart for our sample size, then we are justified in concluding that the deleted and non-deleted groups differ at the 5% level. A larger separation of the two profiles exists when comparing the metacarpals, proximal and middle phalanges but an overlap of the distal phalanges also exists.
Fig. 1.
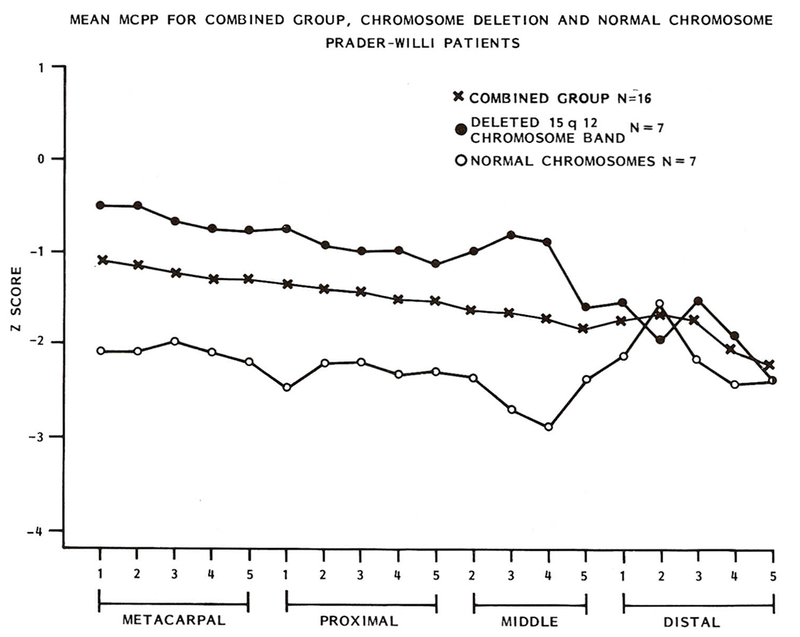
Mean MCPP for combined group, deletion and non-deletion Prader-Willi individuals. Subgroup profiles resemble mirror images.
After applying the correlation program to assess similarity between the mean pattern and each of the 16 individual patterns, ten of 16 individuals had a significant positive correlation. Next, the correlation of individual patterns of each member and their group mean pattern (deletion or non-deletion) was assessed. All members of the deletion chromosome group and four of seven non-deletion members had a significant correlation (Table 1).
Table 1.
Correlations between Prader-Willi individual’s MCPP and its group mean MCPP based on chromosome 15 findings
| Age | Sex | Correlation |
|---|---|---|
| Group 1. Normal chromosome 15 | ||
| 24 years | M | 0.37 |
| 7 years | F | 0.43* |
| 1 year | M | 0.14 |
| 14 years | F | 0.63* |
| 12 years | M | 0.56* |
| 12 years | M | 0.20 |
| 15 years | F | 0.47* |
| Group 2. Chromosome 15 deletion | ||
| 12 years | M | 0.67* |
| 2 weeks | F | 0.39* |
| 22 years | F | 0.78* |
| 22 years | F | 0.80* |
| 9 years | M | 0.89* |
| 8 months | M | 0.82* |
| 5 years | M | 0.83* |
= Significant correlation at 5% level for one-tailed test.
Discriminant analysis of the normal and combined deletion and non-deletion Prader-Willi groups resulted in a discriminant function based on 3 of the 19 MCPP variables plus age. In the discriminant analysis, patients with Prader-Willi syndrome were distinguished from the normal control group at an overall correct classification rate of 100% for our sample (Fig. 2). The three MCPP variables in the discriminant function were the Z scores representing: (1) the 5th distal phalanx (X19), (2) the 2nd metacarpal (X2) and (3) the 5th middle phalanx (X14).
Fig. 2.
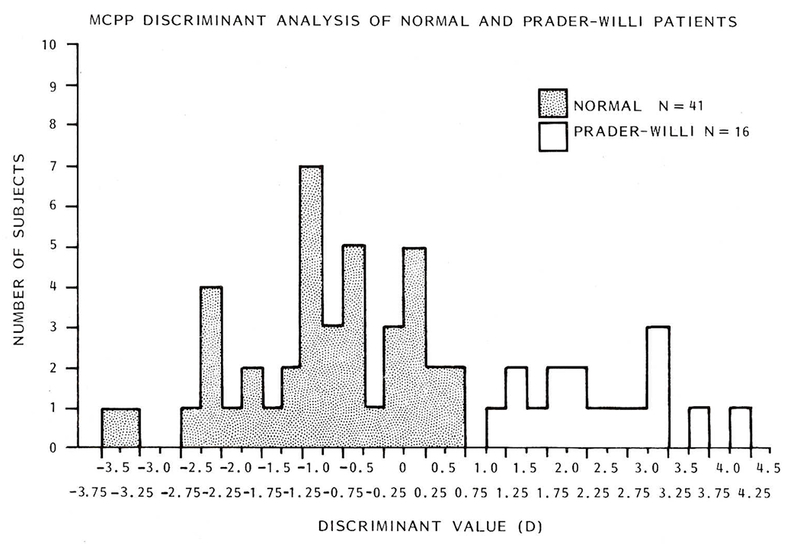
Histogram depicting normal and Prader-Willi classification by discriminant analysis. D = 1.062 + 0.581 (X2) − 0.613(X14) − 0.917(X19) − 0.108(age in years).
Discriminant analysis of deletion and non-deletion chromosome Prader-Willi groups resulted in a discriminant function based on 3 of the 19 MCPP variables, through which the individuals with a chromosome deletion were distinguished from the individuals with normal chromosomes at an overall correct classification rate of 100% from the sample of this study (Fig. 3). In contrast to the results for normal individuals versus Prader-Willi patients, age never entered into the discriminant function. The three variables comprising the discriminant function were the Z scores, representing: (1) the 4th middle phalanx (X13), (2) the 3rd distal phalanx (X17) and (3) the 5th middle phalanx (X14).
Fig. 3.
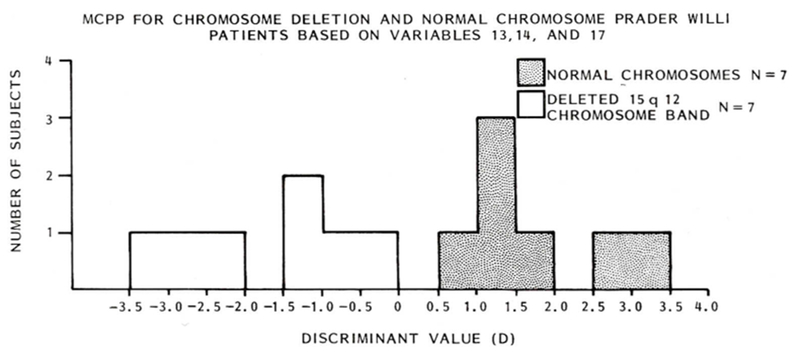
Histogram depicting deletion and non-deletion Prader-Willi classification by discriminant analysis. D = −0.761 − 2.408(X13) + 0.724(X14) + 1.265(X17).
Discussion
Poznanski (1974) has previously described the subjective radiological impression of small hand size in patients with Prader-Willi syndrome. The mean pattern profile based on our 16 cases confirms this impression in quantitative terms. Interestingly, when the Prader-Willi patients were divided according to the chromosome findings, two distinctly different patterns emerged. The correlations in the deletion chromosome group suggest a pattern of homogeneity which contrasts with an apparent residual heterogeneity in the non-deletion group.
The discriminant analysis results suggest that effective classification of Prader-Willi patients compared to normal individuals based on MCPP data is possible. Two of the three discriminating variables between the normal and Prader-Willi individuals are the middle and distal phalanges of the fifth finger. On physical examination, it appears that individuals with the Prader-Willi syndrome have an overall small hand size and the fifth finger is shorter in relationship to the other digits. We are encouraged by the discrimination between the Prader-Willi chromosome groups which supports the suggestion of subgroups made by previous investigators (Forssman & Hagberg 1964, Laurance 1967, Ledbetter et al. 1980). Additional testing is in progress to prove the reliability of the classification method. It is important: (1) to assess the incidence of false positive or false negative results using additional patients, and (2) to test the method’s power to distinguish patients with Prader-Willi syndrome not only from a normal sample, but from patients affected with other conditions featuring small hands and/or a generally similar phenotype. The initial observations presented in this report suggest the potential of MCPP analysis as another diagnostic tool in the evaluation of patients in whom Prader-Willi syndrome is suspected.
Acknowledgments
The authors acknowledge use of the facilities of Computing Services, IUPUI. The authors wish to thank Drs. P. I. Bader and R. S. Wappner for allowing us to obtain hand radiographs from Prader-Willi patients they have been following. This study was supported in part by PHS-5T32 GM07468 (MGB) and by Oral-Facial Genetics Training Grant DE 7043-05 (SGK and FJM).
References
- Enslein K, Ralston A & Wilf HS (eds.) (1977). Statistical Methods For Digital Computers. New York, John Wiley and Sons, pp. 76–95. [Google Scholar]
- Escobar V & Bixler D (1977). The acrocephalosyndactyly syndromes: A metacarpophalangeal pattern profile analysis. Clin. Genet 11, 295–305. [DOI] [PubMed] [Google Scholar]
- Forssman H & Hagberg B (1964). Prader-Willi syndrome in boy of 10 with prediabetes. Acta paediat. 53, 70–78. [DOI] [PubMed] [Google Scholar]
- Garn SM, Hertzog KP, Poznanski AK & Nagy JM (1972). Metacarpophalangeal length in the evaluation of skeletal malformation. Radiology 105, 375–381. [DOI] [PubMed] [Google Scholar]
- Halal F & Preus M (1979). The hand profile in de Lange syndrome: Diagnostic criteria. Amer. J. med. Genet 3, 317–323. [DOI] [PubMed] [Google Scholar]
- Laurance BM (1967). Hypotonia, mental retardation, obesity and cryptorchidism associated with dwarfism and diabetes in children. Arch. Dis. Child 42, 126–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ledbetter DH, Riccardi VM, Youngbloom SA, Strobel RJ, Keenan BS, Crawford JD & Louro JM (1980). Deletion (15q) as a cause of the Prader-Willi syndrome (PWS). Amer. J. hum. Genet 32, 77A. [Google Scholar]
- Ledbetter DH, Riccardi VM, Airhart SD, Strobel RJ, Keenan BS & Crawford JD (1981). Deletions of chromosome 15 as a cause of the Prader-Willi syndrome. New Engl. J. Med 304, 325–329. [DOI] [PubMed] [Google Scholar]
- Poznanski AK, Gam SM, Nagy JM & Gall JC Jr. (1972a). Metacarpophalangeal pattern profiles in the evaluation of skeletal malformations. Radiology 104, 1–11. [DOI] [PubMed] [Google Scholar]
- Poznanski AK, Garn SM, Gall JC Jr. & Stern AM (1972b). Objective evaluation of the hand in the Holt-Oram syndrome. Birth Defects: Original Article Series Vol. VIII, No. 5, 125–131. [Google Scholar]
- Poznanski AK, MacPherson RI, Gorlin RJ, Garn SM, Nagy JM, Gall JC Jr., Stern AM & Dijkman DJ (1973). The hand in otopalatodigital syndrome. Ann. Radiol 16, 203–209. [PubMed] [Google Scholar]
- Poznanski AK (1974). The Hand in Radiological Diagnosis. Philadelphia, W. B. Saunders Co., pp. 29–35. [Google Scholar]
- Prader A, Labhart A & Willi H (1956). Ein Syndrom von Adipositas, Kleinwuch, Kryptorchismus und Oligophrenie nach Myatonieratigem Zustand im Neugeborenenalter. Schweiz, med. Wschr 86, 1260–1261. [Google Scholar]
- Smith DW (1976). Recognizable Patterns of Human Malformation. Philadelphia, W. B. Saunders Co., pp. 106–107. [Google Scholar]