

Abstract
Affective volatility (i.e., variability) is typically conceptualized as a marker of poor mental and behavioral health. The current research challenges this notion. Among individuals who typically experience low positive affect (PA), vacillation between bouts of joy and marked anhedonia may be associated with better behavioral health relative to a restricted range of PA experience. We therefore tested the hypothesis that mean levels of PA captured via an 8-day intensive repeated Ecological Momentary Assessment (EMA) would moderate the association of EMA-measured PA variability with behavioral health measured at intake among working mothers (N = 202) with young children—an population at risk for experiencing repeated stress- and reward-induced PA changes. Mixed Effect Location Scale Modeling parsed variance in PA mean and variability, which were used in subject-level regression models of associations with depressive symptoms, anxiety, and alcohol use. PA mean moderated the associations of PA variability with depressive symptoms (Interaction: β=.20, p=.02) and alcohol consumption frequency (Interaction: β=.22, p=.02). PA variability and depressive symptom and alcohol consumption levels were positively associated at higher PA mean levels, whereas PA variability was inversely associated with depressive symptom and alcohol consumption at low mean PA. PA mean × variability interactions were not significant for anxiety and binge drinking. We conclude that: (1) intensive longitudinal modeling of affect mean × variability interaction effects may provide incremental information in psychopathology research; (2) PA volatility does not unilaterally indicate poor behavioral health; and (3) a nuanced perspective on the role of PA volatility may benefit clinical services for working mothers.
Keywords: Mixed Effect Location Scale Model, Ecological Momentary Assessment, Positive Mood, Depression, Alcohol
Positive affect—the experience of pleasant emotions—is crucial to mental health and subjective well-being (Fredrickson & Losada, 2005). Positive affect promotes resource building and goal pursuits (Elliot & Thrash, 2002), creative thinking and problem solving (Isen, Daubman, & Nowicki, 1987), and resiliency (Cohn, Fredrickson, Brown, Mikels, & Conway, 2009). Deficits in positive affect have been implicated in a number of behavioral conditions, including depression, anxiety-related problems, and substance use (e.g., Garfield, Lubman, & Yücel, 2014; Pizzagalli, 2014), and are considered to be both drivers and consequences of psychopathology (Stanton & Watson, 2014). Consequently, a tendency to typically experience higher levels of positive affect (on average, usual) is characteristically considered to be an indicator of positive mental health.
Importance of Characterizing Individual Differences in Mean Level and Volatility in State Positive Affect in Mental Health Research
While the personality literature shows that individuals possess long-term propensities toward experiencing positive affect in a variety of situations (i.e., “trait” positive affect; Lyubomirsky, King, & Diener, 2005), a given level of positive affect experienced at a momentary time point (i.e., ‘state’ positive affect) is a dynamic construct. For most (but not all) populations, positive affect fluctuates within-individuals across time in response to momentary pleasant events, stressors, or other stimuli (Caspersen, Pereira, & Curran, 2000; Dunton et al., 2014). One’s typical within-person variability in state positive affect experience across time (i.e., affective volatility) can be considered as a source of between-person variation (Dunton et al., 2014; Hedeker, Mermelstein, & Demirtas, 2012). Hence, recent conceptualizations of individual differences in state positive affect highlight two distinct sources of inter-individual variation: (1) mean level across time independent of volatility; and (2) volatility (i.e., variability) across time independent of mean level (see Figure 1).
Figure 1. An example of inter-individual differences in mean levels and volatility in EMA ratings of positive affect.
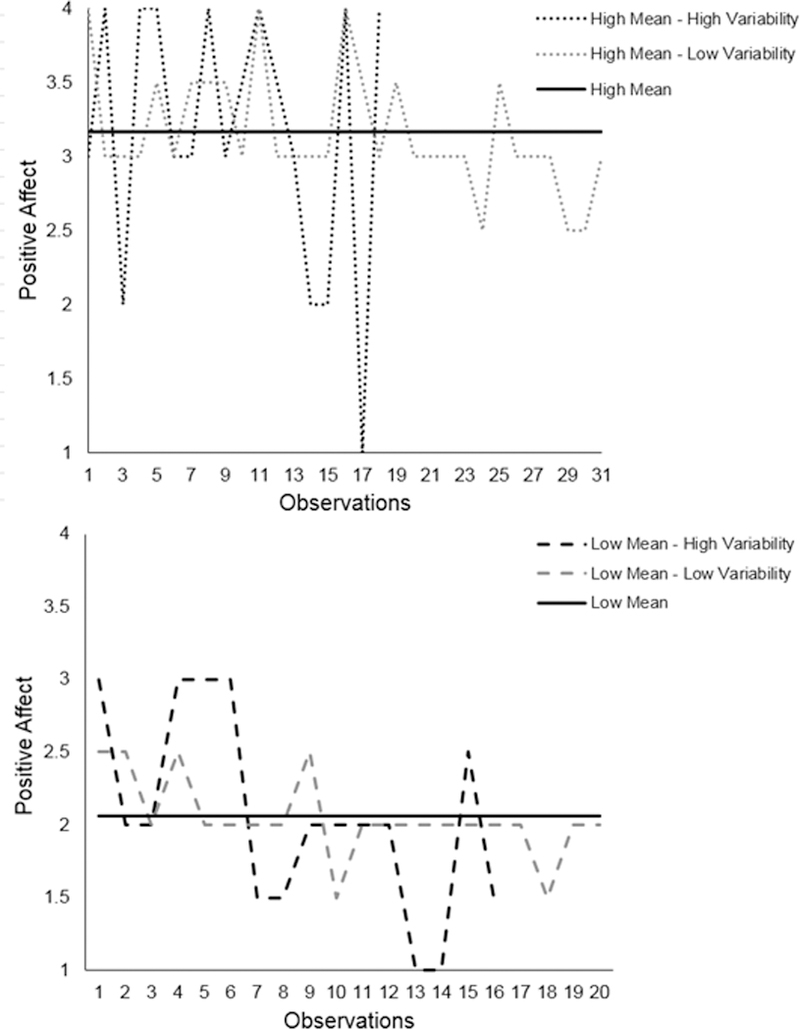
The top panel displays EMA ratings of positive affect for two individuals with relatively high mean levels of positive affect but different degrees of variability in positive affect. The bottom panel displays EMA ratings of positive affect for two individuals with relatively low mean levels of positive affect but different degrees of variability in positive affect.
Lack of Consensus of Whether Positive Affect Volatility Signifies Good or Poor Mental Health
While there is a general consensus regarding the benefits of high mean levels of positive affect, whether greater variability in positive affect is indicative of adaptive or maladaptive behavioral functioning is not clear (e.g., Gruber, Kogan, Quoidbach, & Mauss, 2013; Kashdan & Rottenberg, 2010; Kuppens, Allen, & Sheeber, 2010). Volatility in positive affect may represent maladaptive functioning, as reflection of: (1) a frailty of the affective processing system indicative of hyper-sensitivity to the effects of subtle changes in external and internal states on affect, or (2) an endogenous propensity toward affective vacillation that may be context independent. Gruber et al. (2013) found that day-to-day intraindividual variability in positive affect was associated with greater depression and anxiety symptoms among two non-clinical samples, suggesting that positive affective volatility may be a marker of poor emotional health. Alcohol consumption levels have also been positively associated with variability in positive affect in non-clinical populations, which could be explained by an aggregation of episodes of alcohol use that cause or result from momentary changes in positive affect states or by a shared set of risk factors that contribute to affective volatility and lability to alcohol use (Gottfredson & Hussong, 2013).
Variability in positive affect has also been argued to be an indicator of adaptive psychological functioning among healthy adults and may reflect emotional flexibility or the ability to respond flexibly to changing circumstances (Kashdan & Rottenberg, 2010). Changes in positive affect in response to perceived shifts within the environment spur action to adaptively respond to dynamic contexts. Affective variability may also signal the capacity to express changes in emotion and is considered the healthy standard compared to restricted positive affect range, such as in the case of anhedonia whereby individuals are insensitive to the effects of rewarding environmental cues on positive affect (Kuppens et al., 2010). In a study of normal and clinically depressed adults, Lawton et al. (1996) found that individuals with major depression displayed significantly less variability in daily ratings of positive affect compared to individuals with mild or no depressive symptoms. Such findings raise the possibility that diminished positive affect volatility may be an indicator of a dormant affective processing symptom.
Conflicting evidence and conceptualizations of whether fluctuations in positive affect are adaptive or maladaptive to mental health could be explained by vital moderators. We propose what we feel is an intuitive candidate moderator of the association between positive affect variability and mental health—one’s mean level of state positive affect collapsed across time and instances.
Mean Level of State Positive Affect as Candidate Moderator of the Association of Positive Affect Volatility with Emotional Symptomatology and Alcohol Consumption
Variability in positive affect may be an indicator of adaptive psychological functioning within the subpopulation of individuals with low mean levels of positive affect. Amongst those with low mean levels of positive affect, volatility signifies responsiveness to changing contextual factors and the ability to experience higher than mean levels of positive affect. People with low mean and high variability positive affect may vacillate between experiencing temporary states of marked anhedonia and momentary states of joy. Such a pattern of affective experience may signal a non-dormant affective processing system that is responsive to contexts. For such individuals, perhaps the cumulative effects of brief states of joy may have lasting effects that counterpoise states of marked anhedonia to protect against emotional symptomatology, such as depression and anxiety, and satiate urges to consume alcohol to enhance positive affect. By contrast, people with low mean positive affect with little volatility reflects a chronic restricted affect state of low-to-moderate levels of positive affect without temporary bouts of joy or brief episodes of marked anhedonia. Such individuals may not reap the protective benefits of momentary episodes of joy and thus be more prone to depression and anxiety symptoms and possess a drive to consume alcohol for affect enhancement.
Amongst individuals with higher mean levels of positive affect, lower affective volatility may indicate psychological stability and a constant level of adaptive positive affect with little or no temporary bouts of affective deficiency. If periods of positive affective deficiencies represent vulnerability to psychopathology or maladaptive emotion-regulation behaviors, such as alcohol consumption, high-mean/low-variability positive affect populations may be resilient to behavioral conditions. For high-mean positive affect individuals, high variability in positive affect may represent affective vacillations between extreme states of joy and temporary periods of moderate or lower positive affect that could suggest episodes of feeling less satisfied with life. High-mean/high-variability positive affect populations could also capture those with a propensity toward other illnesses characterized by repeated states of high positive affect and reward seeking (e.g., mania, attention deficit hyperactivity disorder, substance use problems; Gruber, Johnson, Oveis, & Keltner, 2008).
Methods for Characterizing Mean Affect, Affect Volatility, and their Interaction as Correlates of Mental Health
To the best of our knowledge, no prior study has examined whether mean affect moderates the association between affective volatility and mental health problems. Real-time data capture strategies such as Ecological Momentary Assessment (EMA) are designed to repeatedly assess momentary experiences and events as they occur naturally within the content of everyday life (Stone & Shiffman, 1994). Such an approach yields a relatively large number observations within each subject otherwise known as intensive longitudinal data. Intensive longitudinal designs whereby samples provide repeated reports of momentary affective states multiple times per day provide a rich data source for modeling variance in person-level mean and variability parameters across time (Hedeker, Mermelstein, & Demirtas, 2008; Hedeker et al., 2012; Penner, Shiffman, Paty, & Fritzsche, 1994). While person-level mean and variability estimates in state affect are non-redundant sources of variance, they have been shown to be moderately correlated with one another (Hedeker et al., 2008, 2012). Hence, statistical controlling for the covariance between mean and variability parameters is important to understand their unique effects as well as their interactive effects. Mixed effect location scale modeling incorporates a log linear structure for determinants of both the between- and within-subject variance (Hedeker et al., 2008; Hedeker & Nordgren, 2013). More importantly, this modeling approach includes a random subject effect for the within-subject variance specification (Hedeker et al., 2008). This allows the within-subject variance to vary at the subject level which can then be modeled as a person-level predictor, along with traditional predictors such as person-level mean (Hedeker & Nordgren, 2013). Therefore mixed-effects location scale models have useful applications where interest centers on the joint modeling of the mean and variance structure.
Women with Small Children are A Population Liable to Experience Affective Volatility and Mental Health Problems
Mothers of small children represent a particularly vulnerable population for experiencing affective volatility and mental health problems. First, women are more likely to experience more intense affective states (Carstensen, Pasupathi, Mayr, & Nesselroade, 2000) and greater affective lability (Carstensen et al., 2011) compared to men. Beyond that, mothers typically represent the primary care givers for children (Bianchi, 2000) and may be more susceptible to experiencing the emotional highs and low associated with parenthood (Rutherford, Wallace, Laurent, & Mayes, 2015). For example, data from the American Time Use Survey indicated that mothers experience greater momentary well-being (i.e., greater momentary feelings of happiness and lower momentary feelings of sadness and stress) when they are with their child(ren) compared to times when they are not with their child(ren); however, mothers reported greater momentary feelings of stress and fatigue compared to fathers (Musick, Meier, & Flood, 2016).
Women in their childbearing years are also more susceptible to experiencing mental health problems such as depression or anxiety disorders. Globally, depression is second only to HIV/AIDS in terms of total disability among women aged 15 to 44 years and in the United States depression is the leading cause of non-obstetric hospitalization among women age 18 to 44 years (Kendall-Tackett, 2016). Moreover, nearly one-third of adults between the ages of 18 and 44 have experienced an anxiety disorder and women are 60% more likely than men to experience an anxiety disorder over their lifetime (Kessler et al., 2005). The presence of mental health issues among mothers is important given its implications for the development of psychopathology among children (e.g., Cummings & Davies, 1994).
The Present Study
In this secondary analysis of a community sample of mothers with small children, the present report utilized intensive repeated measures positive affect data collected from an EMA observation period as well as data from questionnaire measures of depressive symptoms, anxiety, and alcohol use administered at an intake visit. We test the hypothesis that the association between intraindividual variability of positive affect with depressive symptoms, anxiety, and alcohol consumption would be moderated by mean levels of positive affect, such that the association between positive affect volatility and mental health would trend toward a positive direction at higher mean affect level and trend toward a negative direction at a lower mean affect level. A two-stage approach employing mixed effect location-scale modeling (Hedeker & Nordgren, 2013) was used to simultaneously model mean levels of and intraindividual variability in positive affect and their interactive associations with subject-level indicators of mental health.
Methods
Study Overview
This secondary data analysis was conducted among mothers from the Mothers’ and Their Children’s Health Study (MATCH). MATCH uses ecological momentary assessment in addition to other sampling techniques to understand the effects of parental stress on children’s physical activity and eating behaviors at the within-day level that contribute to children’s long‐term obesity risk (Dunton et al., 2015). Though the primary aims of the MATCH study are different from the aims of the present study, the present study represents an opportunity to maximize the information contained in EMA data from MATCH that aligned with our a priori, novel research questions.
Participants
Participants were mothers of children attending public elementary schools and afterschool programs in the greater Los Angeles metropolitan area. Inclusion was based on the following criteria: (1) the child was in 3rd-6th grade; (2) the mother had ≥50% custody of the child; and (3) mother and child were able to read English or Spanish. Exclusion was based on the following criteria: either mother or child (1) currently taking medications for thyroid function or psychological conditions (2) health issues that limit physical activity, (3) enrolled in special education programs (3) currently using oral or inhalant corticosteroids for asthma, (4) pregnancy, (5) child classified as underweight by a BMI percentile < 5% adjusted for sex and age and (6) mothers who work 2+ weekday evenings per week or 8+ hours on any weekend day.
Procedures
Mothers interested in participating in the study were screened for eligibility by phone. Eligible mothers and their children were asked to attend an in-person data collection session. At this session, mothers completed a paper-and-pencil questionnaire, anthropometric assessments, and received instructions for smartphone-based EMA protocol which they are asked to complete over the next eight days. As part of the EMA protocol mothers received random prompts through an auditory signal on the smartphone to complete a brief electronic questionnaire up to 8 times per day (8 questionnaires on weekend days occurring between 7:00am and 9:30pm, 4 questionnaires on weekdays occurring during non-school hours between 3:00pm and 9:30pm). Each electronic questionnaire consisted of up to 31 questions about mother’s current affect, behaviors, context, and parenting practices and took approximately 3 minutes to complete. If participants did not respond to the initial auditory signal, participants were re-prompted two additional times at three-minute intervals. If participants did not answer the brief electronic questionnaire within 10 minutes of the initial auditory signal, the questionnaire became inaccessible until the next prompt. At the same time, children answered EMA prompts on a similar schedule but those data are reported elsewhere (Dunton et al., 2016).
EMA data were collected through a custom software application (app) for smartphones running the Android operating system (Google Inc., Mountainview, CA). Participants without a compatible smartphone or not wishing to use their own smartphone for the study were loaned a Motorola MotoG (Motorola Mobility, Chicago, IL) smartphone. Mothers who owned compatible Android smartphones were given the option to complete the EMA surveys directly from their personal phones (11% of participants chose this option). Mothers were given the option to use the app in English or Spanish (6% of mothers chose Spanish). All study procedures were approved by the University of Southern California’s Institutional Review Board (HS-12–00446).
Measures
Positive affect.
Mother’s positive affect was assessed through EMA. Items assessing positive affect were based on the circumplex model (i.e., valence and arousal) of the Positive and Negative Affect Schedule (Watson, Clark, & Tellegen, 1988) with response options on a 4-point Likert scale ranging from 1 (not at all) to 4 (extremely). Positive affect was assessed with two items (i.e., “Right before the phone went off, how HAPPY were you feeling?”, “Right before the phone went off, how CALM/RELAXED were you feeling?”). These items were selected to capture positive activated affect (e.g., happy) and positive-deactivated affect (e.g., calm), while limiting participant fatigue and burden typically associated with EMA protocols. Responses to the domains of positive affect through EMA were internally consistent (Ω = 0. 68), so a composite score was created by averaging the responses together.
Mental Health.
Depression was assessed using the 20-item Center for Epidemiologic Studies Depression Scale (CESD; Radloff, 1977). Participants were asked how often they felt a particular way in the past week (e.g., “I felt that I could not shake off the blues even with the help of friends and family”) on a scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time). The 20-item measure is designed to assess symptoms of depression including dysphoria, anhedonia, appetite, sleep, thinking/concentration, guilt, fatigue, agitation, and suicidal ideation. Responses displayed a high level of internal consistency (α = .92) and were summed. For secondary analysis, three subscales (somatic, negative affect, and interpersonal symptoms) that were identified by a recent meta-analysis of the factor structure of the CESD, which is consistent with Radloff’s (1977) original four-factor structure, were also derived (Shafer, 2006). Anxiety was assessed using the 20-item State-Trait Anxiety Inventory, a validated measure of anxiety in adults (Spielberger, 1989). Participants were asked to indicate how often they felt a particular way in the past week (e.g., “I felt inadequate”) on a scale ranging from 1 (almost never) to 4 (almost always). Responses were internally consistent (α = .92) and summed to create a composite score. Frequency of drinking occasions over the past month was assessed using a single item (i.e., “How often during the past month did you have a drink containing alcohol?”) (Johnston, O’Malley, Bachman, & Schulenberg, 2010). Response options included: “never”, “monthly or less”, “2–4 times per month”, “2–3 times per week”, and “4 or more times per week”. Responses were the recoded to provide the following numeric values for number of drinking occasions in the past month: 0 (never), 1 (monthly or less), 3 (2–4 times per month), 10 (2–3 times per week), and 16 (4 or more times per week). Binge drinking in the past month was assessed with a single-item (i.e., “During the past month, how often did you have six or more drinks in one occasion?”) (Johnston et al., 2010). Mothers indicated that they had engaged in at least one binge drinking occasion were coded as 1, whereas mothers who did not indicate binge drinking in the past month were coded as 0.
Demographic characteristics.
Mothers completed paper-and-pencil questionnaires assessing age, ethnicity, household type, employment status, education level, and annual household income (some participants [n =73] were asked about their income in 2012 which occurred one to two years prior to participation in the study).
Data Analysis
This study employed a two-stage data analysis approach. The first stage used mixed effect location scale modeling to estimate a subject’s mean (location) and variability (scale), and the second stage integrated these estimated location and scale effects into a subject-level linear or logistic regression (Hedeker & Nordgren, 2013). The first stage model was executed using the MIXREGLS program (for more details on this modeling approach see Hedeker & Nordgren, 2013). Specifically, in the first stage, an empty model with no covariates was tested to disaggregate the within-subject (WS) mean level as well as between-subject (BS) and WS variances in positive affect (i.e., a momentary prompt-level outcome) (Hedeker & Nordgren, 2013). In the second stage, a subject’s mean level and variability in momentary positive affect (estimated in the first stage model) as well as the interaction between their mean level and variability in positive affect were used to predict subject-level aspects of mental health (i.e., depression, anxiety) and health risk behaviors (i.e., volume of alcohol consumption, binge drinking). Four separate second stage models were tested, one for each subject-level outcome of interest. All second stage models were tested as linear regression models, except for the model with binge drinking as the outcome in which a logistic regression was tested in the second stage. Positive affect variables (both mean level and variability in) were standardized along with maternal mental health and frequency of alcohol consumption variables to facilitate the comparison of results between models. The binge drinking variable was not standardized because these variables were dichotomized and thus had a meaningful zero.
Subject-level covariates (i.e., age, ethnicity, household type, employment status, education level, annual household income, and number of children) to include in the second stage model were screened based on significant bivariate correlations with subjects’ mean level and variability in positive affect as well as study outcomes (p < 0.05). As a result, adjusted second stage models controlled for income quartiles (i.e., $0-$34,999, $35,000-$74,999, $75,000-$104,999, $105,000+), household type (single-parent vs dual-parent/multigenerational) and education (college vs no college).
Resampling.
Resampling was conducted as an additional step to strengthen confidence in the estimates of the original model. Resampling accounts for the fact that the first-stage analysis generates subject-level random effects as estimated quantities, which are then used as predictors in the second-stage analysis. As estimated quantities, these estimates can have varying degrees of uncertainty (Carsey & Harden, 2013). For example, if a particular subject does not have many observations in the first-stage analysis, their random effect estimates will have more uncertainty relative to a subject that has many observations. Therefore, for each subject, the random effects were resampled 100 times to generate random effects estimates (and standard errors) the random effects were resampled. These resampled data were then used to rerun the second-stage modeling procedure 100 times. Results were then averaged for the coefficients and standard errors across the resamples.
Results
Data Availability and Participant Characteristics
There were 202 mothers enrolled in the study at baseline. Of those, 11 mothers provided no positive affect data across the EMA protocol (2 due to malfunction and 9 due to non-response). Of mothers providing EMA data on positive affect (n = 191), mothers answered an average of 78.2% (range 3.4% – 100%) of delivered EMA prompts. Additionally, due to missing demographic information (n = 7) as well as incomplete paper-and-pencil questionnaire data regarding outcomes of interest, the final analytic sample sizes for each series of models ranged from 171 (anxiety) - 184 (drinking) participants. Of participants providing valid EMA data and demographic information, mother’s age ranged from 24 to 57 years (M = 40.9 years, SD = 6.2). Approximately half of mothers identified as Hispanic or Latina (49.2%). The majority of mothers were a part of two-parent households (62.8%) while 23.6% of mothers were single-parents and 13.6% were apart of multigenerational households. Sixty percent of mothers reported attending attended college. More than half of the sample reported working full-time (56.4%). Median annual household income in the sample ranged between $65,000 and $74,999.
On average, mothers reported relatively low-to-moderate levels of depressive symptoms (M = 7.9 on a 0 to 60 scale; SD = 8.3) and anxiety (M = 37.1 on a 20 to 80 scale; SD = 9.5). Participants reported approximately 4 drinking occasions, on average, within the past month (M = 3.9 occasions; SD = 6.8). Almost one-third of the sample reported no drinking occasions at all within the past 30 days (n = 55) whereas 6.6% of the sample reported consuming alcohol daily over the past month (n = 12). Eight percent reported at least one binge drinking episode in the past month.
In the final analytic sample (n = 191), there were a total of 4,186 observations with positive affect data. Across all observations, not accounting for the nesting of occasions within people, mothers reported moderate levels of positive affect (M = 2.6 on a 1 to 4 scale; SD = 0.7). The intraclass correlation (ICC) was 0.34, indicating that approximately two-thirds of the variance in positive affect occurred within subjects.
Correlations amongst key mental health and behavioral variables as well as mean levels positive affect and variability in positive affect and relevant covariates are displayed in Table 1.
Table 1.
Descriptive statistics and correlations between maternal mental health and behavioral variables, mean in positive affect, and other key variables
| M (%) | SD | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Depressive Symptoms | 7.9 | 8.3 | 1.00 | |||||||||
| 2. Anxiety | 37.1 | 9.5 | 0.80* | 1.00 | ||||||||
| 3. Drinking occasions in the past month |
3.9 | 6.8 | -0.05 | -0.10 | 1.00 | |||||||
| 4. Binge Drinking | 8.4% | -- | 0.25* | 0.18* | 0.02 | 1.00 | ||||||
| 5. Mean Positive Affect | 2.6 | 0.7 | -0.39* | -0.43 | -0.01 | -0.05 | 1.00 | |||||
| 6. Age | 40.9 | 6.2 | 0.01 | -0.08 | 0.09 | -0.17* | -0.04 | 1.00 | ||||
| 7. Ethnicity | 49.2% | -- | 0.04 | 0.06 | -0.14 | 0.09 | -0.02 | -0.38* | 1.00 | |||
| 8. Single Parent Household |
23.6% | -- | 0.16* | 0.17* | -0.04 | -0.02 | -0.16* | 0.03 | 0.04 | 1.00 | ||
| 9. Work full time | 56.4% | -- | -0.01 | -0.01 | -0.02 | -0.04 | -0.03 | -0.20* | 0.01 | 0.06 | 1.00 | |
| 10. Income | $65,000-$74.999 | -- | -0.29* | -0.21* | 0.16* | -0.07 | 0.10 | 0.21* | -0.29* | -0.40* | 0.04 | 1.00 |
| 11. Attended college | 56.5% | -- | -0.19* | -0.17* | -0.02 | -0.19* | 0.16* | -0.28* | -0.38* | -0.09 | 0.01 | 0.46* |
Note. n=191. Higher composite scores for depressive symptoms and anxiety indicate greater feelings of depressive symptoms or anxiety, respectively. Frequency of alcohol consumption refers to the number of days in the past month participants consumed alcohol. Binge drinking refers to if a participant consumed 6+ drinks in one sitting in the last past month. Binge drinking, ethnicity, household type, and employment status are dichotomous variables with engaging in binge drinking, being Hispanic, being in a single-parent household, working full time, and attending college representing the higher value.
Positive Affect Mean level and Variability Main Effects and Interaction Effects for Association with Mental Health
Results from the original models as well as results from resampling are shown in Table 2.
Table 2.
Modeling associations between mean level and variability in positive affect and mental health and behavioral outcomes.
| Adjusted Models | Adjusted Models With Resampling |
|||||
|---|---|---|---|---|---|---|
| Estimate | Standard Error |
p- value |
Estimate | Standard Error |
p- value |
|
| Depressive Symptoms (n = 178) | ||||||
| Intercept | -.01 | .07 | .99 | .37 | .14 | .01 |
| Positive Affect Mean | -.35 | .07 | <.001 | -.42 | .07 | <.001 |
| Positive Affect Variability | .10 | .08 | .20 | .06 | .08 | .41 |
| Positive Affect Mean × Variability interaction |
.20 | .09 | .02 | .17 | .09 | .05 |
|
Anxiety (n = 171) | ||||||
| Intercept | -.02 | .06 | .80 | .27 | .14 | .05 |
| Positive Affect Mean | -.40 | .08 | <.001 | -.44 | .07 | <.001 |
| Positive Affect Variability | .21 | .08 | .01 | .18 | .08 | .03 |
| Positive Affect Mean × Variability interaction |
.11 | .09 | .23 | .09 | .09 | .31 |
|
Frequency of Alcohol Consumption (n = 177) | ||||||
| Intercept | -.35 | .20 | .08 | -.19 | .14 | .19 |
| Positive Affect Mean | .06 | .08 | .4 | -.03 | .07 | .68 |
| Positive Affect Variability | .07 | .08 | .38 | .01 | .08 | .87 |
| Positive Affect Mean × Variability interaction |
.22 | .09 | .02 | .18 | .09 | .06 |
|
Binge Drinking (n=184) | ||||||
| Intercept | -1.58 | .84 | .06 | -1.56 | .59 | .01 |
| Positive Affect Mean | -.12 | .36 | .73 | -.36 | .34 | .30 |
| Positive Affect Variability | .34 | .38 | .37 | .20 | .40 | .60 |
| Positive Affect Mean × Variability interaction |
.51 | .32 | .12 | .40 | .35 | .24 |
Note. Estimates for depressive symptoms, anxiety, and frequency of alcohol consumption in the past 30 days were standardized (M=0, SD=1) and served as the outcome variable in separate linear regressions. Binge drinking in the past 30 days and was the outcome variable in a logistic regression. Models control for income quartiles, household type (single-parent vs dual-parent/multigenerational) and education (college vs no college).
Depressive symptoms.
Based on results from the original model, the mean level of positive affect main effect was significantly negatively associated with depressive symptoms (β Mean = −0.35, p <.001, 95% CI [−0.49, −0.21]); whereas variability in positive affect main effect did not significantly predict depressive symptoms. In addition, the association between variability in positive affect and depressive symptoms varied as a function of mean levels of positive affect (β Mean × Variability Interaction term = 0.20, p = .02, 95% CI [0.02, 0.38]). More specifically, the magnitude of the relationship between variability in positive affect and depressive symptoms increased (i.e., became more positive) for individuals with higher mean levels of positive affect, but for individuals with low mean levels of positive affect the association between variability in positive affect and depressive symptoms became more negative (see Figure 2).
Figure 2. Interaction between mean level and variability in positive affect predicting depressive symptoms.
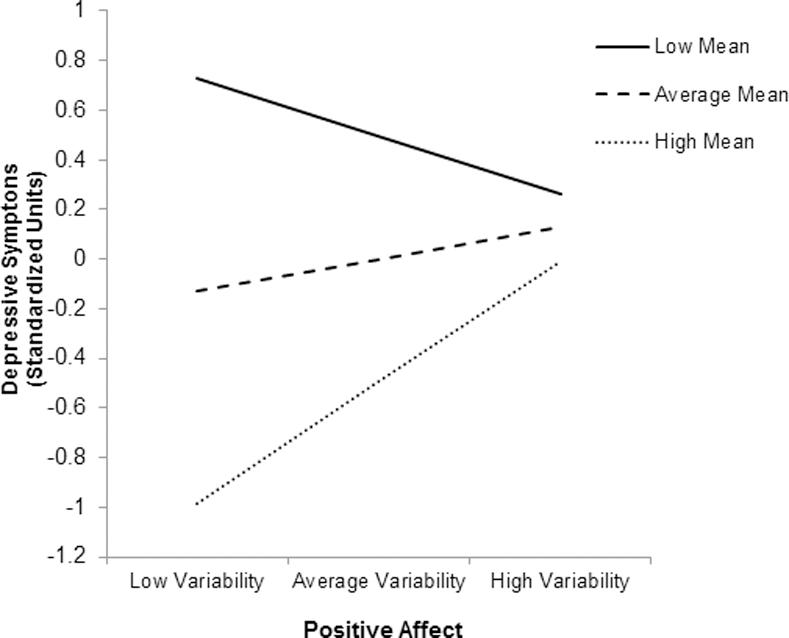
Low and high mean and variability refer to 1.5 standard deviations below and above the mean, respectively.
Because deficient positive affect is a component of depression (Shafer, 2016), secondary analyses that utilized CESD depressive symptom subscales for somatic features, interpersonal problems, and negative effect were conducted to elucidate whether the positive affect mean × variability interaction term was associated with the three non-positive affect symptom domains captured by the CESD. Reported in detail in the Electronic Supplementary File, results from the original model indicated that the association between variability in positive affect and negative affect subscale and somatization subscale varied as a function of mean level of positive affect (Negative Affect: β Mean × Variability Interaction term = 0.20, p = 0.02, 95% CI [0.02, 0.38]; Somatization Features: β Mean × Variability Interaction term = 0.22, p =0.01, 95% CI [0.02, 0.40,] respectively).
Anxiety.
Based on results from the original model, the positive affect mean level main effect was negatively associated with anxiety (β Mean = −0.40, p <.001, 95% CI [−0.56, −0.34]), whereas positive affect variability main effect was positively associated with anxiety (β Variability = 0.21, p = .01, 95% CI [0.05, 0.37]). The interaction between mean levels and variability in positive affect was not significantly associated with anxiety.
Frequency of drinking occasions.
Based on results from the original model, the main effects of mean level and variability in positive affect were not associated with frequency of drinking occasions in the past 30 days. The association between variability in positive affect and frequency of drinking occasions varied as a function of mean levels of positive affect (β mean × variability interaction = .22, p = .02, 95% CI [0.04, 0.40]). More specifically, the strength of the relationship between variability in positive affect and frequency of alcohol consumption is increased (or became more positive) for individuals with higher mean levels of variability in positive affect (see Figure 3).
Figure 3. Interaction between mean level and variability in positive affect predicting frequency of alcohol consumption in the past 30 days.
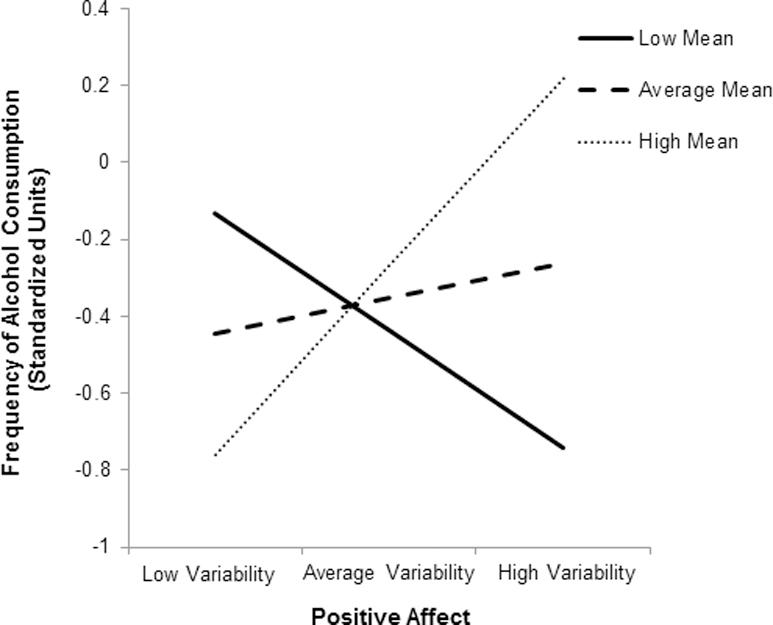
Low and high mean and variability refer to 1.5 standard deviations below and above the mean, respectively.
Binge drinking.
Based on results from the original model, neither the main effects nor interaction of mean level and variability in positive affect were significantly associated with odds of engaging in binge drinking within the past month.
Resampling.
Results from resampling were similar with coefficients in the same direction as in the original model although the size of beta coefficients did decrease and the p-values did increase slightly. Central to the main research questions of this manuscript, the interaction between mean level and variability in positive affect non-significantly predicted depressive symptoms (β mean × variability interaction = .17, p = .05, 95% CI [−0.01, 0.35]) and frequency of alcohol consumption (β mean × variability interaction = .18, p = .06, 95% CI [0.00, 0.36]).
Discussion
This study provides the first known evidence that associations between volatility in positive affect and psychological and behavioral outcomes may vary as a function of one’s mean levels in positive affect. Previous work in non-clinical populations has been equivocal regarding the role of variability in momentary ratings of positive affect on aspects of health and well-being (Gruber et al., 2013; Kashdan & Rottenberg, 2010; Kuppens et al., 2010). This study helps to further disentangle the associations between these constructs by exploring the role of mean level as a moderator Although this study sampled individuals with relatively healthy psychological and behavioral health profiles, the current study extends previous work by demonstrating that greater variability in positive affect may be adaptive for those with low means levels of positive affect but maladaptive for those with high mean levels of positive affect. The novel methodology and results from this study have broad implications for future research aiming to understand the dynamic nature of emotion and its relationship with health and well-being in both clinical and non-clinical populations. The novel methodological and analytical approach employed in this manuscript can be applied to a variety of populations as well as research in psychopathology that utilize real-time data capture methodology.
Affective volatility is considered a possible cause of non-clinical depression (Costello, Benjamin, Angold, & Silver, 1991; Eid & Diener, 1999). Results from this study indicated that, for mothers with high mean levels of positive affect, depressive symptoms were higher amongst mothers with high variability in positive compared to mothers that had low variability in positive affect. Conversely, among mothers with low mean levels of positive affect, depressive symptoms were higher amongst mothers with low variability in positive compared to mothers that had high variability in positive affect. Sensitivity analyses suggest that these associations between positive affect and depressive symptoms may be driven largely by the negative affect and interpersonal problems CESD subscales. These results suggest that the simple presence of affective variability is not maladaptive regarding depressive symptoms, rather the consequences of affective variability depend on one’s typical level of affect. Previous studies in non-clinical populations investigating associations between variability in positive affect and mental health outcomes did not explore the potential moderating role of mean levels positive affect in these associations (Eid & Diener, 1999; Gruber et al., 2013). Individuals with greater variability in positive affect coupled with high mean levels of positive affect may experience affective vacillations between extreme states of joy and temporary periods of moderate or lower positive affect. These momentary emotional declines may be maladaptive among non-clinical populations in that they signal psychological instability and an inability to cope with changes within one’s environment (Gruber, Mauss, & Tamir, 2011). Conversely, greater variability in positive affect coupled with low mean levels of positive affect responsiveness to changing contextual factors and able to experience higher than mean levels of positive affect. Therefore, despite overall low levels of positive affect, these individuals may experience the cumulative effects of brief states of joy and pleasure leading to a more adaptive psychological profile.
It is possible that these same pathways may be responsible for potential interactive effects of mean levels of and volatility in positive affect on anxiety. Although the interaction between mean level of and variability in positive affect was not significantly related to anxiety in this study, the effect size of the coefficient was smaller than that of depression and it may be that this study was not adequately powered to detect that association. Further research is necessary to replicate these finding as well as explore potential mechanisms underlying associations between mean levels of positive affect, volatility in positive affect, and mental health outcomes such as depression and anxiety.
This study was also one of the first to investigate whether associations between volatility in positive affect and alcohol consumption related-behaviors varied as a function of mean levels of positive affect. Results from this study indicated that, for mothers with high mean levels of positive affect, frequency of drinking occasions was higher amongst mothers with high variability in positive affect compared to mothers that had low variability in positive affect. Conversely, among mothers with low mean levels of positive affect, frequency of drinking occasions was higher amongst mothers with low variability in positive compared to mothers that had high variability in positive affect. Previous research among non-clinical populations has documented that affective variability is associated with greater risk for development of alcohol dependence symptoms (Simons, Carey, & Wills, 2009) as well as increased frequency of alcohol consumption (Jahng et al., 2011) and self-reported drinking to cope (Gottfredson & Hussong, 2013). Work by Mohr, Arpin, and McCabe (2015) in community-dwelling adults has also documented that greater affective variability, specifically in positive affect, is positively associated with alcohol consumption (both solitary and social). However, none of these studies have investigated the moderating role of mean levels of positive affect in associations between variability in positive affect and alcohol related behaviors. For individuals with high mean levels of and high variability in positive affect, frequent alcohol consumption may serve a way to dampen momentary changes in affect as a result of changing context (Curtin, Patrick, Lang, Cacioppo, & Birbaume, 2001; Gottfredson & Hussong, 2013). Steele and Josephs’ (1990) theory of alcohol myopia suggests that alcohol consumption limits unwanted cognitions which may be especially desirable for individuals experiencing frequent negative shifts in affective states. However, for individuals with low mean levels but high variability in positive affect, experiencing momentary increases in positive affect may represent welcomed affective states. Future research is necessary to illuminate mechanisms linking mean levels of positive affect, variability in positive affect, and frequency of alcohol consumptions.
Moreover, the majority of studies investigating affective volatility and drinking behaviors have been conducted among college students (Gottfredson & Hussong, 2013) whose frequency of drinking is much higher than adults (Substance Abuse and Mental Health Services Administration, 2013), or among samples where participants were considered moderate-to-heavy drinkers (Mohr et al., 2015). Therefore, null associations documented in this study regarding variability in positive affect and binge drinking may be the results of sampling a population with a minimal occurrence of binge drinking. Expanding the samples in which associations between mean levels of and variability in positive affect and health risk behaviors are examined will lead to a more comprehensive understanding of contexts in which affective variability is adaptive or maladaptive in specific populations.
Regarding practical implications, the findings from this study provide a nuanced perspective on the role of positive affect volatility which may ultimately benefit clinical services for working mothers. Working mothers with low mean levels and low variability as well as mothers with high mean level and high variability in positive affect represent a subset of mothers that may have inadequate resources and support (e.g., tangible, emotional, informational) available to them to cope with daily events, hassles, and stressors. The results from this study may serve as a starting point for tailoring workplace wellness programs as well as counseling and clinical services.
Although this study provides valuable insights into the dynamics of positive affect in women, it is not without limitations. First this study focused exclusively on mothers with children. Although this is an important subsample of women to focus on because mothers often serve as primary caregiver of children and as a result are role models and gate keepers for a variety of health behaviors (e.g., Bianchi, 2000; Maher et al., 2017; O’Connor et al., 2017), results from this study are not generalizable to other women or men. Furthermore, we recognize that the sample included in this study exhibited relatively low levels of poor mental health and maladaptive health behaviors (although these rates probably reflect levels among the general nonclinical population of adults). However, this research is novel with respect to the methodology and analytic approach employed in this study. This paper, in part, represents an empirical example of how to investigate differences in associations between volatility in positive affect, mental health, and alcohol consumption as a function of mean levels of positive affect. This type of approach can be applied to a variety of other populations, both clinical and non-clinical, to provide novel insights into dynamic nature of affect in everyday life as well as inform practical applications for intervention. Therefore, future research would benefit from rigorously exploring differences in associations between volatility in positive affect, mental health, and alcohol consumption as a function of mean levels of positive affect in populations that exhibit higher levels of depressive symptoms as well as alcohol consumption. Furthermore, the methods and results highlighted in this study also have implications for research in psychopathology that currently utilize real-time data capture methodologies to assess affective volatility but have not considered mean levels of affect, leading to critical insights related to how the two may interact.
Due to the primary objective of the MATCH study, mothers were assessed through EMA during the times when they were most likely to be with their child (after 3:00pm on weekdays and all day on weekend days). Therefore, the sampling protocol did not allow for assessment of positive affect during weekday mornings or afternoons. It is possible that affect during common activities that take place during weekday mornings and afternoons such as work may systematically influence either mean levels of or variability in positive affect (Amabile, Barsade, Mueller, & Staw, 2005). Additionally, to minimize participant fatigue and burden, items assessing positive affect were limited to two items. These items were selected to capture positive activated affect (e.g., happy) and positive-deactivated affect (e.g., calm), while limiting participant fatigue and burden. Although these items have been used to assess positive affect in previous research (Liao, Shonkoff, & Dunton, 2015), only including two items may limit the representativeness as well as provide less fine gradations in the positive affect construct (Ekkekakis, 2013). Future research regarding variability in positive affect would benefit from more broadly sampling affective domains within the positive affect construct. Frequency of alcohol consumption was assessed with a single-item measure. This measure was derived from the Monitoring Our Future national survey and has been used widely to assess alcohol consumption in national samples (Johnston et al., 2010). While this item accounts for the frequency of alcohol-consumption, the item does not provide information on the intensity of drinking behaviors. The intensity of drinking behaviors during drinking occasions can provide valuable information regarding hazardous patterns of alcohol consumption (e.g., Patrick, Terry-McElrath, Kloska, & Schulenberg, 2016). A more comprehensive measure that includes both the frequency and intensity of alcohol consumption would contribute to greater understanding of relations between variability in positive affect and hazardous drinking patterns.
Furthermore, results from this study do not explore different types of variability displayed in momentary ratings of positive affect. An underlying theoretical assumption of the findings from this study suggests that variability in positive affect reflects responses to changing contexts and that certain affective responses may be adaptive whereas other affective responses may be maladaptive given contextual and person-level factors. Future research is necessary to parse apart which are the most detrimental aspects of variability and whether the affective lability is context-appropriate (Gruber et al., 2013; Kashdan & Rottenberg, 2010).
Finally, this study cannot disentangle the temporal direction of the associations between mean levels of and variability in positive affect and maternal mental health or health risk behaviors. For example, health risk behaviors like frequency of alcohol consumption may influence means levels and variability in affective states (e.g., Baker, Piper, McCarthy, Majeskie, & Fiore, 2004). Future work is needed to better understand the causal links between mean levels and variability in positive affect and mental health and health risk behavior outcomes.
In conclusion, this study is one of the first to investigate the interactive association between mean levels and volatility in positive affect and mental health and health risk behaviors. Results indicate that considering of mean levels of positive affect may be important for understanding how variability in positive affect influences psychological and behavioral outcomes. This study adds to our theoretical understanding of the ways in which variability in positive affect can be adaptive for individuals with low mean levels of positive affect but maladaptive for individuals with high mean levels of positive affect.
Supplementary Material
References
- Amabile TM, Barsade SG, Mueller JS, & Staw BM (2005). Affect and creativity at work. Administrative Science Quarterly, 50(3), 367–403. [Google Scholar]
- Baker TB, Piper ME, McCarthy DE, Majeskie MR, & Fiore MC (2004). Addiction motivation reformulated: an affective processing model of negative reinforcement. Psychological Review, 111(1), 33–51. [DOI] [PubMed] [Google Scholar]
- Bianchi SM (2000). Maternal employment and time with children: Dramatic change or surprising continuity? Demography, 37(4), 401–414. [DOI] [PubMed] [Google Scholar]
- Carsey TM, & Harden JJ (2013). Monte Carlo simulation and resampling methods for social science Thousand Oaks, CA: Sage Publications. [Google Scholar]
- Carstensen LL, Pasupathi M, Mayr U, & Nesselroade JR (2000). Emotional experience in everyday life across the adult life span. Journal of Personality and Social Psychology, 79(4), 644–655. 10.1037/0022-3514.79.4.644 [DOI] [PubMed] [Google Scholar]
- Carstensen LL, Turan B, Scheibe S, Ram N, Ersner-Hershfield H, Samanez-Larkin GR, … Nesselroade JR. (2011). Emotional experience improves with age: Evidence based on over 10 years of experience sampling. Psychology and Aging, 26(1), 21–33. 10.1037/a0021285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caspersen CJ, Pereira MA, & Curran KM (2000). Changes in physical activity patterns in the United States, by sex and cross-sectional age. Medicine and Science in Sports and Exercise, 32(9), 1601–1609. [DOI] [PubMed] [Google Scholar]
- Cohn MA, Fredrickson BL, Brown SL, Mikels JA, & Conway AM (2009). Happiness unpacked: positive emotions increase life satisfaction by building resilience. Emotion, 9(3), 361–368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costello EJ, Benjamin R, Angold A, & Silver D (1991). Mood variability in adolescents: a study of depressed, nondepressed and comorbid patients. Journal of Affective Disorders, 23(4), 199–212. [DOI] [PubMed] [Google Scholar]
- Cummings EM, & Davies PT (1994). Maternal depression and child development. Journal of Child Psychology and Psychiatry, 35(1), 73–122. [DOI] [PubMed] [Google Scholar]
- Curtin JJ, Patrick CJ, Lang AR, Cacioppo JT, & Birbaume N (2001). Alcohol affects emotion through cognition. Psychological Science, 12(6), 527–531. 10.1111/1467-9280.00397 [DOI] [PubMed] [Google Scholar]
- Dunton GF, Dzubur E, Huh J, Belcher BR, Maher JP, O’Connor S, & Margolin G (2016). Daily Associations of Stress and Eating in Mother–Child Dyads. Health Education & Behavior, 1–5. 10.1177/1090198116663132 [DOI] [PubMed]
- Dunton GF, Huh J, Leventhal AM, Riggs N, Hedeker D, Spruijt-Metz D, & Pentz MA (2014). Momentary assessment of affect, physical feeling states, and physical activity in children. Health Psychology, 33(3), 255–263. 10.1037/a0032640 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunton GF, Liao Y, Dzubur E, Leventhal AM, Huh J, Gruenewald T, … Intille S. (2015). Investigating within-day and longitudinal effects of maternal stress on children’s physical activity, dietary intake, and body composition: Protocol for the MATCH study. Contemporary Clinical Trials, 43, 142–154. 10.1016/j.cct.2015.05.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eid M, & Diener E (1999). Intraindividual variability in affect: Reliability, validity, and personality correlates. Journal of Personality and Social Psychology, 76(4), 662. [Google Scholar]
- Ekkekakis P (2013). The measurement of affect, mood, and emotion: A guide for health-behavioral research Cambridge University Press. [Google Scholar]
- Elliot AJ, & Thrash TM (2002). Approach-avoidance motivation in personality: Approach and avoidance temperaments and goals. Journal of Personality and Social Psychology, 82(5), 804–818. [DOI] [PubMed] [Google Scholar]
- Fredrickson BL, & Losada MF (2005). Positive affect and the complex dynamics of human flourishing. American Psychologist, 60(7), 678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garfield JBB, Lubman DI, & Yücel M (2014). Anhedonia in substance use disorders: A systematic review of its nature, course and clinical correlates. Australian & New Zealand Journal of Psychiatry, 48(1), 36–51. 10.1177/0004867413508455 [DOI] [PubMed] [Google Scholar]
- Gottfredson NC, & Hussong AM (2013). Drinking to dampen affect variability: Findings from a college student sample. Journal of Studies on Alcohol and Drugs, 74(4), 576–583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gruber J, Johnson SL, Oveis C, & Keltner D (2008). Risk for mania and positive emotional responding: too much of a good thing? Emotion, 8(1), 23–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gruber J, Kogan A, Quoidbach J, & Mauss IB (2013). Happiness is best kept stable: Positive emotion variability is associated with poorer psychological health. Emotion, 13(1), 1–6. [DOI] [PubMed] [Google Scholar]
- Gruber J, Mauss IB, & Tamir M (2011). A Dark Side of Happiness? How, When, and Why Happiness Is Not Always Good. Perspectives on Psychological Science: A Journal of the Association for Psychological Science, 6(3), 222–233. 10.1177/1745691611406927 [DOI] [PubMed] [Google Scholar]
- Hedeker D, Mermelstein RJ, & Demirtas H (2008). An application of a Mixed-Effects Location Scale Model for analysis of Ecological Momentary Assessment (EMA) data. Biometrics, 64(2), 627–634. 10.1111/j.1541-0420.2007.00924.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hedeker D, Mermelstein RJ, & Demirtas H (2012). Modeling between-subject and within-subject variances in ecological momentary assessment data using mixed-effects location scale models. Statistics in Medicine, 31(27), 3328–3336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hedeker D, & Nordgren R (2013). MIXREGLS: a program for mixed-effects location scale analysis. Journal of Statistical Software, 52(12), 1–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Isen AM, Daubman KA, & Nowicki GP (1987). Positive affect facilitates creative problem solving. Journal of Personality and Social Psychology, 52(6), 1122–1131. [DOI] [PubMed] [Google Scholar]
- Jahng S, Solhan MB, Tomko RL, Wood PK, Piasecki TM, & Trull TJ (2011). Affect and alcohol use: An ecological momentary assessment study of outpatients with borderline personality disorder. Journal of Abnormal Psychology, 120(3), 572–584. 10.1037/a0024686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, & Schulenberg JE (2010). Monitoring the Future: National Survey Results on Drug Use, 1975–2009. Volume I: Secondary School Students (No. NIH Publication No. 10–7584). National Institute on Drug Abuse; Retrieved from http://eric.ed.gov/?id=ED514370 [Google Scholar]
- Kashdan TB, & Rottenberg J (2010). Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review, 30(7), 865–878. 10.1016/j.cpr.2010.03.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kendall-Tackett KA (2016). Depression in new mothers: Causes, consequences and treatment alternatives Taylor & Francis. Retrieved from https://books.google.com/books?hl=en&lr=&id=JjolDwAAQBAJ&oi=fnd&pg=PP1&dq=depression+in+mothers+book&ots=YnHX9lAvVs&sig=xvwuTA02hHpd7rtkp2VH9UawMCI [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, & Walters EE (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. [DOI] [PubMed] [Google Scholar]
- Kuppens P, Allen NB, & Sheeber LB (2010). Emotional inertia and psychological maladjustment. Psychological Science, 21(7), 984–991. 10.1177/0956797610372634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lawton MP, Parmelee PA, Katz IR, & Nesselroade J (1996). Affective states in normal and depressed older people. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 51(6), P309–P316. [DOI] [PubMed] [Google Scholar]
- Liao Y, Shonkoff ET, & Dunton GF (2015). The acute relationships between affect, physical feeling states, and physical activity in daily life: A review of current evidence. Frontiers in Psychology, 6 10.3389/fpsyg.2015.01975 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lyubomirsky S, King L, & Diener E (2005). The Benefits of Frequent Positive Affect: Does Happiness Lead to Success? Psychological Bulletin, 131(6), 803–855. 10.1037/0033-2909.131.6.803 [DOI] [PubMed] [Google Scholar]
- Maher JP, Ra CK, O’Connor SG, Belcher BR, Leventhal AM, Margolin G, & Dunton GF (2017). Associations between maternal mental health and well-being and physical activity and sedentary behavior in children. Journal of Developmental and Behavioral Pediatrics [DOI] [PMC free article] [PubMed]
- Mohr CD, Arpin S, & McCabe CT (2015). Daily affect variability and context-specific alcohol consumption. Drug and Alcohol Review, 34(6), 581–587. 10.1111/dar.12253 [DOI] [PubMed] [Google Scholar]
- Musick K, Meier A, & Flood S (2016). How Parents Fare: Mothers’ and Fathers’ subjective well-being in time with children. American Sociological Review, 81(5), 1069–1095. 10.1177/0003122416663917 [DOI] [Google Scholar]
- O’Connor SG, Maher JP, Belcher BR, Leventhal AM, Margolin G, Shonkoff ET, & Dunton GF (2017). Associations of maternal stress with children’s weight-related behaviors: A systematic literature review. Obesity Reviews 10.1111/obr.12522 [DOI] [PMC free article] [PubMed]
- Patrick ME, Terry-McElrath YM, Kloska DD, & Schulenberg JE (2016). High-Intensity Drinking Among Young Adults in the United States: Prevalence, Frequency, and Developmental Change. Alcoholism, Clinical and Experimental Research, 40(9), 1905–1912. 10.1111/acer.13164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Penner LA, Shiffman S, Paty JA, & Fritzsche BA (1994). Individual differences in intraperson variability in mood. Journal of Personality and Social Psychology, 66(4), 712–721. [DOI] [PubMed] [Google Scholar]
- Pizzagalli DA (2014). Depression, Stress, and Anhedonia: Toward a Synthesis and Integrated Model. Annual Review of Clinical Psychology, 10(1), 393–423. 10.1146/annurev-clinpsy-050212-185606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radloff LS (1977). The CES-D scale a self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. [Google Scholar]
- Rutherford HJV, Wallace NS, Laurent HK, & Mayes LC (2015). Emotion Regulation in Parenthood. Developmental Review, 36, 1–14. 10.1016/j.dr.2014.12.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shafer AB (2006). Meta-analysis of the factor structures of four depression questionnaires: Beck, CES-D, Hamilton, and Zung. Journal of Clinical Psychology, 62(1), 123–146. [DOI] [PubMed] [Google Scholar]
- Simons JS, Carey KB, & Wills TA (2009). Alcohol abuse and dependence symptoms: A multidimensional model of common and specific etiology. Psychology of Addictive Behaviors: Journal of the Society of Psychologists in Addictive Behaviors, 23(3), 415–427. 10.1037/a0016003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spielberger CD (1989). State-trait anxiety inventory: A comprehensive bibliography Consulting Psychologists Press. [Google Scholar]
- Stanton K, & Watson D (2014). Positive and Negative Affective Dysfunction in Psychopathology. Social and Personality Psychology Compass, 8(9), 555–567. 10.1111/spc3.12132 [DOI] [Google Scholar]
- Steele CM, & Josephs RA (1990). Alcohol myopia: Its prized and dangerous effects. American Psychologist, 45(8), 921–933. 10.1037/0003-066X.45.8.921 [DOI] [PubMed] [Google Scholar]
- Stone AA, & Shiffman S (1994). Ecological momentary assessment (EMA) in behavorial medicine. Annals of Behavioral Medicine, 16(3), 199–202. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. (2013). Results from the 2012 National Survey on Drug Use and Health: Summary of NAtional Findings (No. HHS Publication No. (SMA) 13–4795). Rockville, MD: Substance Abuse and Mental Health Services Administration. [Google Scholar]
- Watson D, Clark LA, & Tellegen A (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
There were 202 mothers enrolled in the study at baseline. Of those, 11 mothers provided no positive affect data across the EMA protocol (2 due to malfunction and 9 due to non-response). Of mothers providing EMA data on positive affect (n = 191), mothers answered an average of 78.2% (range 3.4% – 100%) of delivered EMA prompts. Additionally, due to missing demographic information (n = 7) as well as incomplete paper-and-pencil questionnaire data regarding outcomes of interest, the final analytic sample sizes for each series of models ranged from 171 (anxiety) - 184 (drinking) participants. Of participants providing valid EMA data and demographic information, mother’s age ranged from 24 to 57 years (M = 40.9 years, SD = 6.2). Approximately half of mothers identified as Hispanic or Latina (49.2%). The majority of mothers were a part of two-parent households (62.8%) while 23.6% of mothers were single-parents and 13.6% were apart of multigenerational households. Sixty percent of mothers reported attending attended college. More than half of the sample reported working full-time (56.4%). Median annual household income in the sample ranged between $65,000 and $74,999.
On average, mothers reported relatively low-to-moderate levels of depressive symptoms (M = 7.9 on a 0 to 60 scale; SD = 8.3) and anxiety (M = 37.1 on a 20 to 80 scale; SD = 9.5). Participants reported approximately 4 drinking occasions, on average, within the past month (M = 3.9 occasions; SD = 6.8). Almost one-third of the sample reported no drinking occasions at all within the past 30 days (n = 55) whereas 6.6% of the sample reported consuming alcohol daily over the past month (n = 12). Eight percent reported at least one binge drinking episode in the past month.
In the final analytic sample (n = 191), there were a total of 4,186 observations with positive affect data. Across all observations, not accounting for the nesting of occasions within people, mothers reported moderate levels of positive affect (M = 2.6 on a 1 to 4 scale; SD = 0.7). The intraclass correlation (ICC) was 0.34, indicating that approximately two-thirds of the variance in positive affect occurred within subjects.
Correlations amongst key mental health and behavioral variables as well as mean levels positive affect and variability in positive affect and relevant covariates are displayed in Table 1.
Table 1.
Descriptive statistics and correlations between maternal mental health and behavioral variables, mean in positive affect, and other key variables
| M (%) | SD | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Depressive Symptoms | 7.9 | 8.3 | 1.00 | |||||||||
| 2. Anxiety | 37.1 | 9.5 | 0.80* | 1.00 | ||||||||
| 3. Drinking occasions in the past month |
3.9 | 6.8 | -0.05 | -0.10 | 1.00 | |||||||
| 4. Binge Drinking | 8.4% | -- | 0.25* | 0.18* | 0.02 | 1.00 | ||||||
| 5. Mean Positive Affect | 2.6 | 0.7 | -0.39* | -0.43 | -0.01 | -0.05 | 1.00 | |||||
| 6. Age | 40.9 | 6.2 | 0.01 | -0.08 | 0.09 | -0.17* | -0.04 | 1.00 | ||||
| 7. Ethnicity | 49.2% | -- | 0.04 | 0.06 | -0.14 | 0.09 | -0.02 | -0.38* | 1.00 | |||
| 8. Single Parent Household |
23.6% | -- | 0.16* | 0.17* | -0.04 | -0.02 | -0.16* | 0.03 | 0.04 | 1.00 | ||
| 9. Work full time | 56.4% | -- | -0.01 | -0.01 | -0.02 | -0.04 | -0.03 | -0.20* | 0.01 | 0.06 | 1.00 | |
| 10. Income | $65,000-$74.999 | -- | -0.29* | -0.21* | 0.16* | -0.07 | 0.10 | 0.21* | -0.29* | -0.40* | 0.04 | 1.00 |
| 11. Attended college | 56.5% | -- | -0.19* | -0.17* | -0.02 | -0.19* | 0.16* | -0.28* | -0.38* | -0.09 | 0.01 | 0.46* |
Note. n=191. Higher composite scores for depressive symptoms and anxiety indicate greater feelings of depressive symptoms or anxiety, respectively. Frequency of alcohol consumption refers to the number of days in the past month participants consumed alcohol. Binge drinking refers to if a participant consumed 6+ drinks in one sitting in the last past month. Binge drinking, ethnicity, household type, and employment status are dichotomous variables with engaging in binge drinking, being Hispanic, being in a single-parent household, working full time, and attending college representing the higher value.