

Abstract
Background
Computed tomography (CT) emphysema quantification is affected by both radiation dose (i.e. image noise) and reconstruction technique. At reduced dose, filtered back projection (FBP) results in an overestimation of the amount of emphysema due to higher noise levels, while the use of iterative reconstruction (IR) can result in an underestimation due to reduced noise. The objective of this study was to determine the influence of dose reduction and hybrid IR (HIR) or model-based IR (MIR) on CT emphysema quantification.
Methods
Twenty-two patients underwent inspiratory chest CT scan at routine radiation dose and at 45%, 60% and 75% reduced radiation dose. Acquisitions were reconstructed with FBP, HIR and MIR. Emphysema was quantified using the 15th percentile of the attenuation curve and the percentage of voxels below -950 HU. To determine whether the use of a different percentile or HU threshold is more accurate at reduced dose levels and with IR, additional measurements were performed using different percentiles and HU thresholds to determine the optimal combination.
Results
Dose reduction resulted in a significant overestimation of emphysema, while HIR and MIR resulted in an underestimation. Lower HU thresholds with FBP at reduced dose and higher HU thresholds with HIR and MIR resulted in emphysema percentages comparable to the reference. The 15th percentile quantification method showed similar results as the HU threshold method.
Conclusions
This within-patients study showed that CT emphysema quantification is significantly affected by dose reduction and IR. This can potentially be solved by adapting commonly used thresholds.
Electronic supplementary material
The online version of this article (10.1186/s41747-018-0064-3) contains supplementary material, which is available to authorized users.
Keywords: Densitometry, Emphysema, Radiation dosage, Thorax, Tomography (x-ray computed)
Key points
Dose reduction resulted in a significant CT overestimation of emphysema, while iterative reconstruction resulted in a significant underestimation
This can potentially be solved by adapting the commonly used densitometry thresholds
The maximal intraclass correlation coefficient between reduced dose and the reference standard was achieved at 75% reduced dose with hybrid iterative reconstruction
Background
Chest computed tomography (CT) offers the possibility of quantifying the amount of emphysema. The number of chest CT acquisitions is expected to increase due to the favourable results of the National Lung Screening Trial [1] and the interest in subtyping chronic obstructive pulmonary disease (COPD) patients [2]. Additional quantification of emphysema on screening CT acquisitions will therefore likely gain importance. Furthermore, this additional information may also contribute to optimisation of the benefits and cost-effectiveness of CT screening [3]. CT can be used to both identify patients with emphysema as well as to monitor progression in patients with COPD. Although emphysema is traditionally a pathology-based diagnosis [4, 5], CT densitometry of the lungs has demonstrated it to be associated with airflow obstruction, forced expiratory volume in 1 s and severity according to the Global initiative for chronic Obstructive Lung Disease (GOLD) criteria [6–8]. CT densitometry is based on either the 15th percentile of the attenuation curve or the percentage of voxels below -950 HU because those parameters show the strongest correlation with microscopic and macroscopic emphysema findings [8, 9]. Although pulmonary function tests measure limitation of airflow, they are not able to differentiate between airway obstruction and emphysematous destruction. CT, on the other hand, provides in vivo information about pathological changes and allows for differentiation between airway obstruction and emphysematous destruction [10].
The increasing number of chest CT scans has urged the importance of radiation dose reduction. However, dose reduction leads to higher noise levels, especially when images are reconstructed using conventional filtered back projection (FBP). Therefore, several iterative reconstruction (IR) techniques were developed to reduce image noise [11, 12]. Recent studies showed that the radiation dose of unenhanced chest CT can be reduced to sub-millisievert dose levels when IR is applied [13].
It is known that CT emphysema quantification is affected by both radiation dose (i.e. image noise) and reconstruction technique. At reduced dose, FBP results in an overestimation of the amount of emphysema due to higher noise levels, while the use of IR can result in an underestimation due to reduced noise [14–16].
The primary aim of the current study was to determine the effect of both dose reduction and IR on CT emphysema quantification using a within-patients study design. The secondary aim was to investigate whether adapting CT densitometry thresholds is a valid way to correct for over- or underestimation at reduced dose and with IR.
Methods
Patients
This prospective study was approved by the local Institutional Review Board (NL46146.041.13) and all study participants provided written informed consent. Patients aged ≥ 50 years scheduled for follow-up of ≥ 1 known small pulmonary nodules were eligible for inclusion. The influence of dose reduction and IR on pulmonary nodule volume and computer-aided detection of pulmonary nodules was previously investigated in the same study population [17, 18].
Image acquisition
Image acquisition was performed on a 256-slice CT system (Brilliance iCT; Philips Healthcare, Best, The Netherlands). An unenhanced chest CT was acquired during inspiration. The routine dose acquisition was performed with a tube voltage of 100 kVp (body weight < 80 kg) or 120 kV (body weight ≥ 80 kg). The tube current-time product was 60 mAs at routine dose and subsequently decreased to 33, 24 and 15 mAs to achieve 45%, 60% and 75% dose reduction, respectively. All four acquisitions were acquired consecutively in a single session. Automatic exposure control was off. Images were reconstructed at a slice thickness of 2 mm with FBP, hybrid IR (HIR; iDose level 4, Philips Healthcare, Best, The Netherlands) and model-based IR (MIR; IMR level 2, Philips Healthcare, Best, The Netherlands). Kernel filter C was used for both FBP and HIR. MIR is a more advanced reconstruction technique with different kernels; therefore, the vendor-recommended kernel filter Body Routine was used for MIR. The volume CT dose index (CTDIvol) and dose-length product (DLP) of each acquisition was recorded. The effective dose was calculated by multiplying the DLP with a conversion factor of 0.0144 (100 kVp) or 0.0145 (120 kVp) [19].
Emphysema quantification
Semi-automatic commercially available software (IntelliSpace version 8, COPD tool, Philips Healthcare, Best, The Netherlands) was used for emphysema quantification. The noise reduction option in the software was not used. The software segments airways first, followed by the lungs and finally the different lobes. No manual segmentation was needed. Subsequently, a histogram (attenuation curve) is made which displays the number of voxels with a certain density (Fig. 1). Emphysema can be quantified by using either a percentile of the attenuation curve or the percentage of voxels below a certain HU value. On the routine dose acquisition reconstructed with FBP, emphysema was defined as a HU value which describes the lowest 15% of the segmented lungs (perc15). Furthermore, the percentage of voxels with a HU value of -950 HU or lower (percentage emphysema) was calculated. To determine whether the use of a different percentile or HU threshold is more accurate at reduced dose levels and with IR, additional measurements were performed as follows (1 percentage and 10 HU increments):
reduced dose FBP: perc8 – perc35 and -960 HU – -1010 HU
HIR:perc1 – perc25 and -880 HU – -960 HU
MIR: perc1 – perc20 and -880 HU – -960 HU
Fig. 1.

Example of the semi-automatic software which was used for emphysema quantification. First, the airways, lungs and lung lobes are segmented (a). Subsequently, a histogram is made which displays the number of voxels with a certain density (b). In this example the percentage of voxels below -950 HU is displayed
Objective image quality
A region of interest was placed in the ascending aorta at the level of the tracheal bifurcation and in the subcutaneous fat dorsal of the infraspinatus muscle. The noise was defined as the standard deviation of the region of interest and the contrast-to-noise ratio (CNR) was calculated using the following formula:
Statistics
Statistical analysis was performed using SPSS version 21 (SPSS Inc., Chicago, IL, USA). The routine dose acquisition reconstructed with FBP was used as the reference standard. The Friedman test was used to compare the reconstructions at each dose level to FBP and post-hoc analyses were performed with the Wilcoxon signed rank test. A p value < 0.05 was considered significant for the Friedman test, while a Bonferroni corrected p value of 0.017 (0.05/3 reconstructions) was used for the Wilcoxon test. The intraclass correlation coefficient (ICC; two-way mixed, absolute agreement, single measures) was used to compare reduced dose and iterative reconstruction to the reference standard. For each dose level and reconstruction technique, the optimal adapted threshold for emphysema quantification was determined. The optimal adapted threshold was also compared to the reference standard using Bland–Altman plots. Results are displayed as median (interquartile range) unless specified otherwise.
Results
Twenty-two patients were included. Half of the patients (n = 11) were female. Ten patients (46%) were scanned with 100 kVp (< 80 kg) and twelve patients (54%) with 120 kVp (≥ 80 kg). The median height of the patients was 169 cm (163–176 cm) and the median weight was 83 kg (74–92 kg) resulting in a body mass index of 28.6 kg/m2 (26.0–31.4 kg/m2). The median CTDIvol was 4.1 mGy at routine dose and 2.2, 1.6 and 1.0 mGy at reduced dose levels for the 120-kVp acquisitions. For the 100-kVp acquisition, the median CTDIvol was 2.4, 1.3, 1.0 and 0.6 mGy, respectively. The median DLP was 150 (96–169), 84 (53–93), 60 (38–66) and 39 (24–42) mGy ×cm, respectively, resulting in median effective dose levels of 2.2 (1.4–2.4), 1.2 (0.8–1.3), 0.9 (0.5–1.0) and 0.6 (0.3–0.6) mSv.
Emphysema
The percentage of emphysema with FBP at routine dose was 5.1% (1.7–8.4%). FBP at reduced dose resulted in a significant overestimation of the percentage of emphysema, while HIR and MIR resulted in a significant underestimation at all dose levels compared to FBP at routine dose (Table 1, Fig. 2). The perc15 measurements resulted in decreased HU values for FBP at reduced dose, while HIR and MIR resulted in significantly increased HU values compared to FBP at routine dose (Table 1, Fig. 3). For the -950 HU threshold, HIR at 75% reduced dose resulted in the highest ICC of 0.92 (0.76–0.97), while the ICC decreased to 0.42 (0.00–0.79) with FBP at 75% reduced dose. Overall, the ICC was better with the perc15 method, resulting in a minimum ICC of 0.59 (0.00–0.88) with FBP at 75% reduced dose and a maximum ICC of 0.94 (0.81–0.98) with HIR at 75% reduced dose.
Table 1.
Percentage of emphysema using the -950 HU threshold and the perc15 method at different dose levels reconstructed with FBP, HIR and MIR
| -950 HU (%) | ICC (95% CI) | Perc15 (HU-value) | ICC (95%CI) | |
|---|---|---|---|---|
| Routine dose | ||||
| FBP | 5.1 (1.7–8.4) | NA | -923 (-936 – -895) | NA |
| HIR | 1.5 (0.1–4.5)a | 0.63 (0.00–0.88) | -914 (-927 – -881)a | 0.91 (0.00–0.98) |
| MIR | 0.9 (0.0–3.6)a | 0.50 (0.00–0.80) | -913 (-926 – -879)a | 0.88 (0.01–0.97) |
| 45% reduced dose | ||||
| FBP | 8.0 (3.3–12.4)a | 0.83 (0.00–0.96) | -932 (-944 – -898)a | 0.93 (0.39–0.98) |
| HIR | 2.5 (0.2–5.1)a | 0.79 (0.01–0.94) | -916 (-929 – -875)a | 0.89 (0.28–0.97) |
| MIR | 1.2 (0.0–3.1)a | 0.51 (0.00–0.81) | -913 (-927 – -867)a | 0.83 (0.07–0.95) |
| 60% reduced dose | ||||
| FBP | 10.2 (5.5–14.7)a | 0.63 (0.00–0.89) | -940 (-949 – -912)a | 0.77 (0.00–0.94) |
| HIR | 2.7 (0.5–6.2)a | 0.83 (0.24–0.95) | -917 (-931 – -881)a | 0.87 (0.62–0.95) |
| MIR | 1.3 (0.0–3.2)a | 0.49 (0.00–0.79) | -911 (-927 – -874)a | 0.80 (0.28–0.93) |
| 75% reduced dose | ||||
| FBP | 14.3 (9.7–19.6)a | 0.42 (0.00–0.79) | -948 (-961 – -925)a | 0.59 (0.00–0.88) |
| HIR | 3.5 (0.7–8.1)a | 0.92 (0.76–0.97) | -921 (-935 – -878)a | 0.94 (0.81–0.98) |
| MIR | 0.9 (0.0–4.2)a | 0.47 (0.00–0.78) | -914 (-927 – -869)a | 0.84 (0.16–0.95) |
Values represent the median (interquartile range). The ICC compares with the reference standard, namely FBP at routine dose
aStatistically significant difference compared to FBP at routine dose with a Bonferroni corrected p value of 0.017
FBP filtered back projection, HIR hybrid iterative reconstruction, ICC intraclass correlation coefficient, MIR model-based iterative reconstruction
Fig. 2.
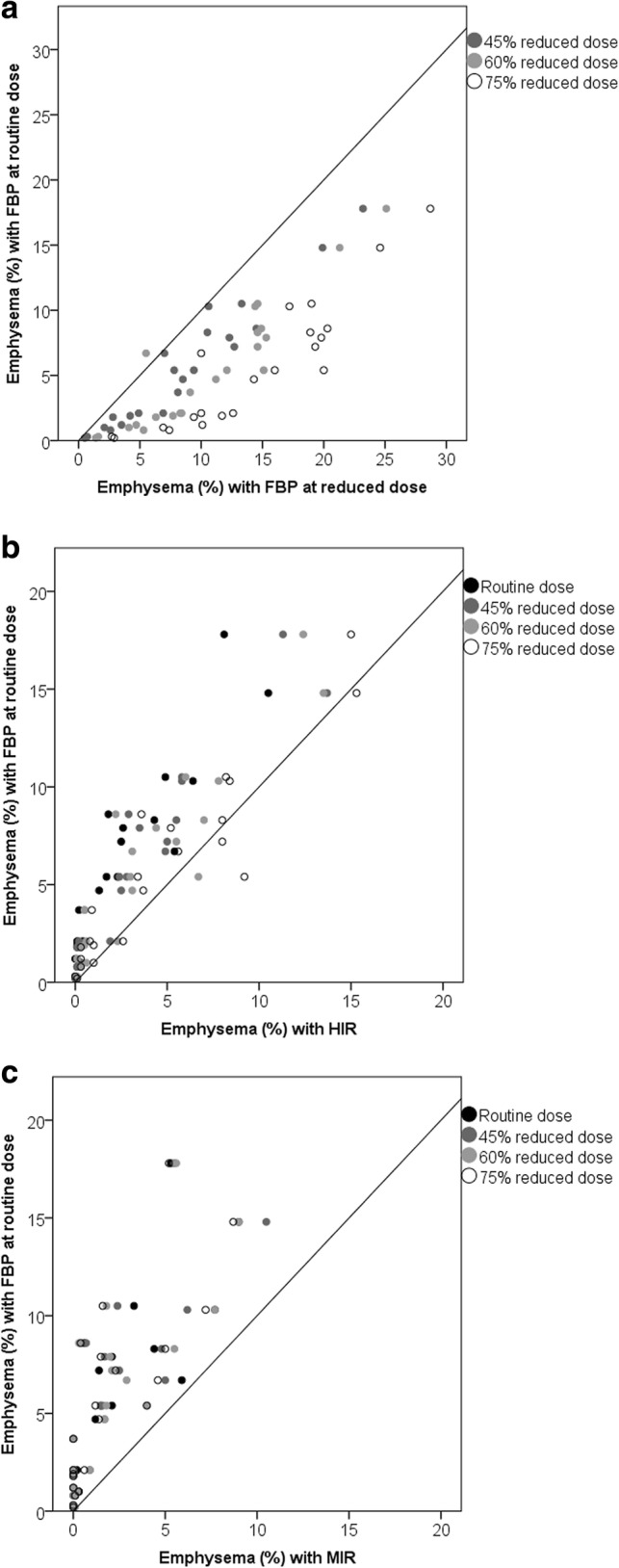
Scatterplots of the effect of radiation dose and reconstruction on the percentage emphysema. The y-axis displays the percentage emphysema with FBP at routine dose (reference), while the x-axis displays the percentage emphysema at reduced dose with FPB (a) and with HIR (b) and MIR (c). Values below the diagonal represent an overestimation of the percentage of emphysema as compared to FBP and routine dose, while values above the diagonal represent an underestimation. FBP filtered back projection, HIR hybrid iterative reconstruction, MIR model-based iterative reconstruction
Fig. 3.
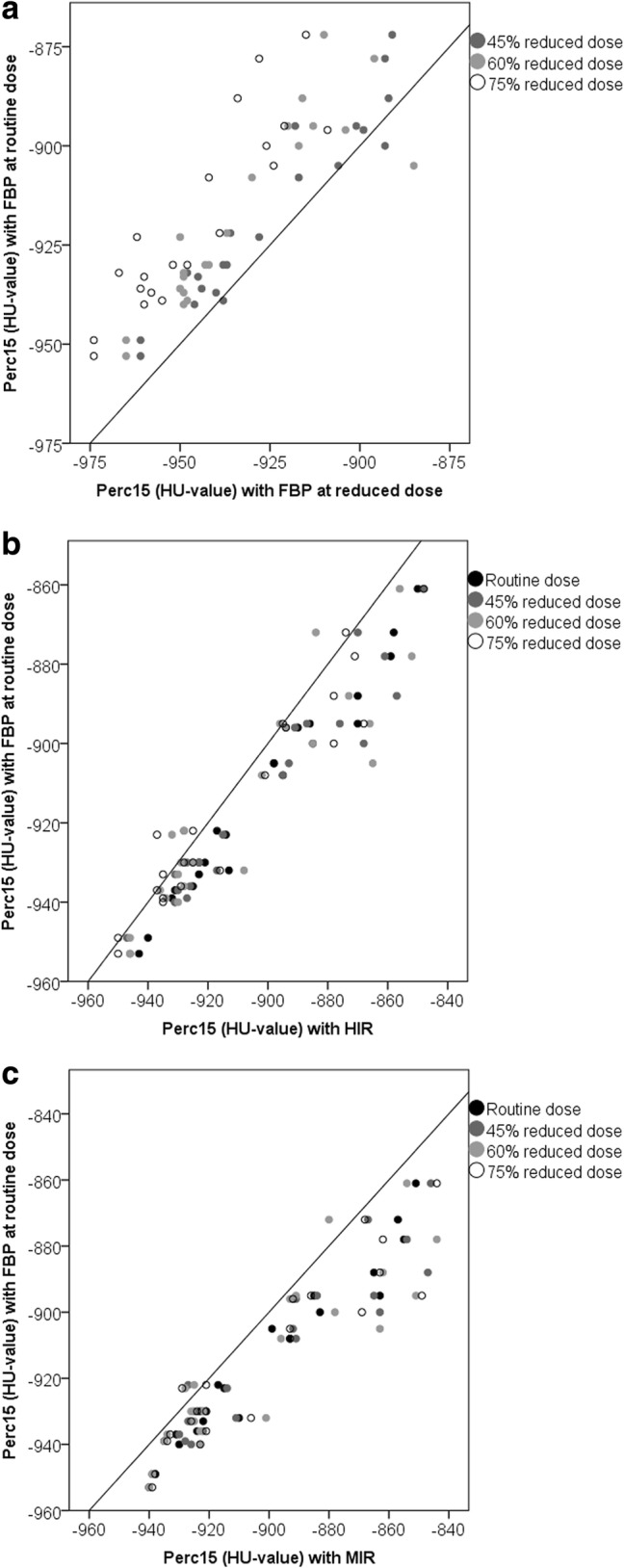
Scatterplots of the effect of radiation dose and reconstruction on the perc15. The y-axis displays the perc15 with FBP at routine dose (reference), while the x-axis displays the perc15 at reduced dose with FBP (a) and with HIR (b) and MIR (c). Values below the diagonal represent a higher HU value compared to the reference, while values above the diagonal represent a lower HU value compared to the reference. FBP filtered back projection, HIR hybrid iterative reconstruction, MIR model-based iterative reconstruction
The effect of using different HU thresholds or percentiles is shown in Fig. 4. Data for each threshold are provided in the supplemental files (Additional file 1: Table S1–S4). With FBP at reduced dose, using a lower threshold of -960 HU, -970 HU and -980 HU at 45%, 60% and 75% reduced dose, respectively, resulted in a percentage of emphysema that was not significantly different from the reference standard. For HIR, a threshold of -930 HU (routine dose) or -940 HU (reduced dose) approximated the percentage emphysema with FBP at routine dose, while this was -930 HU for MIR (all dose levels). Bland-Altman plots are provided in Additional file 2: Figure S1 of the supplemental files. The adapted threshold worked well over the whole range of patients for FBP at reduced dose, while with HIR and MIR there was a trend towards underestimation in patients with a small emphysema percentage and in patients with a higher percentage of emphysema there was an overestimation.
Fig. 4.

Effect of different thresholds (a) and percentiles (b) on emphysema quantification. For FBP at reduced dose a lower threshold is more appropriate, while with HIR and MIR a higher HU threshold should be used. With the percentile quantification method, FBP at reduced dose requires a higher percentile while with HIR and MIR a lower percentile should be used to achieve the same results as with FBP at routine dose. FBP filtered back projection, HIR hybrid iterative reconstruction, MIR model-based iterative reconstruction
FBP at reduced dose required a higher percentile of 19%, 22% and 26%, respectively, at 45%, 60% and 75% reduced dose to achieve results comparable to the reference standard. With HIR and MIR, a lower percentile was required of 8% (routine dose), 10% (45% reduced dose), 11% (60% reduced dose) or 13% (75% reduced dose) with HIR and 8% (all dose levels) with MIR. Bland–Altman plots are provided in Additional file 2: Figure S2 of the supplemental files. The adapted threshold worked well over the whole range of patients for all reconstructions.
Image quality
Noise and CNR are presented in Fig. 5 and Table 2. Noise increased with FBP at reduced dose levels, while HIR and MIR resulted in reduced noise. Noise was significantly lower with HIR at routine dose, 45% reduced dose and 60% reduced dose compared to the reference standard, while at the lowest dose level noise was comparable to FBP at routine dose. MIR resulted in a significant reduction of noise at all reduced dose levels compared to FBP at routine dose. CNR decreased with FBP at reduced dose levels. HIR and MIR resulted in comparable or improved CNR at all reduced dose levels.
Fig. 5.

Noise (a and b) and CNR (c) measured at different dose levels with FBP, HIR and MIR. Noise was measured in the aorta (a) and subcutaneous fat (b). The dotted line represents the reference (FBP at routine dose). CNR contrast-to-noise ratio, FBP filtered back projection, HIR hybrid iterative reconstruction, MIR model-based iterative reconstruction
Table 2.
Noise and CNR at different dose levels with FBP, HIR and MIR
| Noise (aorta) | Noise (fat) | CNR | |
|---|---|---|---|
| Routine dose | |||
| FBP | 37.5 (28.1–42.8) | 30.2 (25.4–52.0) | 4.8 (3.0–5.5) |
| HIR | 18.4 (15.0–22.2)a | 18.2 (14.6–23.3)a | 8.3 (6.7–10.1)a |
| MIR | 11.4 (9.5–12.5)a | 11.5 (9.8–15.2)a | 13.0 (10.7–15.9)a |
| 45% reduced dose | |||
| FBP | 46.6 (38.9–58.4)a | 39.3 (31.6–78.9)a | 3.3 (2.1–4.5)a |
| HIR | 23.2 (20.5–26.5)a | 23.5 (17.5–27.8)a | 6.7 (5.5–8.1)a |
| MIR | 12.3 (11.3–14.4)a | 13.5 (10.7–17.2)a | 11.4 (9.0–13.7)a |
| 60% reduced dose | |||
| FBP | 60.2 (47.8–81.4)a | 50.8 (42.5–94.6)a | 2.5 (1.7–3.5)a |
| HIR | 26.4 (22.9–31.8)a | 28.1 (21.4–34.7)a | 5.5 (4.4–6.8)a |
| MIR | 13.7 (12.2–16.5)a | 13.9 (12.7–17.2)a | 11.4 (8.9–12.4)a |
| 75% reduced dose | |||
| FBP | 80.0 (61.4–108.5)a | 62.8 (47.5–142.6)a | 2.3 (1.2–2.7)a |
| HIR | 32.6 (28.5–37.8) | 30.4 (24.7–39.6) | 4.7 (3.7–5.7) |
| MIR | 16.4 (14.1–19.7)a | 15.1 (13.8–19.1)a | 9.2 (7.9–11.3)a |
Values are presented as median (interquartile range)
aStatistically significant difference compared to FBP at routine dose with a Bonferroni corrected p value of 0.017
CNR contrast-to-noise ratio, FBP filtered back projection, HIR hybrid iterative reconstruction, MIR model-based iterative reconstruction
Discussion
This study shows the effect of different reconstruction techniques at four decreasing radiation dose levels. While FBP resulted in an overestimation of emphysema on CT at reduced dose, both HIR and MIR resulted in an underestimation of the amount of emphysema compared to reconstruction of the images with FBP at routine dose. Furthermore, we showed that by using different thresholds or percentages in HIR and MIR, it was possible to derive results comparable to FBP at routine dose.
There are two commonly used measures to quantify emphysema on CT based on densitometry, namely the density at the 15th percentile of the attenuation curve and the percentage of voxels below -950 HU. Previous studies indicated that those thresholds show the strongest correlation with microscopic and macroscopic emphysema findings in studies using FBP [8, 9]. The 15th percentile and the -950 HU thresholds are widely used; however, different thresholds have been applied in the literature [8, 9, 20, 21]. Several other studies have investigated the effect of dose and image reconstruction on pulmonary emphysema quantification. Schilham et al. [22] compared a clinical routine dose CT acquisition with a low dose acquisition in 25 patients. A post-processing filter was used to reduce the amount of noise in the low dose images and three different thresholds (-950, -930 and -910 HU) were used to quantify emphysema. The application of the filter resulted in a reduction of the effect of noise on the emphysema percentage. A different study by Mets et al. [23] in 75 patients who underwent a routine dose CT acquisition reconstructed with FBP and HIR reported an underestimation of the amount of emphysema with HIR when the cut-off was not adjusted. In a study by Nishio et al. [24], the application of IR at reduced dose improved the agreement in emphysema quantification with routine dose FBP. Three studies comparing a routine dose acquisition with a low-dose acquisition in the same patient all reported an overestimation with low-dose FBP while IR resulted in an underestimation [25–27]. Messerli et al. [27] reduced the radiation dose to chest x-ray equivalent dose levels of 0.14 mSv; at this dose level, HIR resulted in a similar emphysema measurement as FBP at routine dose (1.7 mSv). Similar results were found in the study by Nishio et al. [28]. Therefore, by carefully selecting the dose reduction level, emphysema overestimation can be compensated for by using IR, since the latter results in reduced emphysema with CT quantification. To our best knowledge, only the study by Choo et al. [15] investigated the effects of both HIR and MIR. No dose reduction was used and they reported that MIR resulted in a larger underestimation than HIR compared to FBP, which is comparable to the results of the current study.
The effect of reconstruction technique and radiation dose can be explained by the density histogram. IR algorithms result in a different density distribution, which subsequently affects emphysema quantification. Due to the noise reduction with IR, the extremes of the attenuation distribution are affected [23], leading to a smaller peak in the density histogram. Dose reduction, on the other hand, results in increased image noise, leading to a broadening of the density histogram [29].
In the current study, FBP at routine dose was used as the reference standard. However, ideally a pathological reference standard should be applied or a realistic phantom to determine what is closest to the truth and if thresholds should be adapted. It is important to be aware that differences in emphysema quantification can occur and to keep the radiation dose and reconstruction algorithm constant in longitudinal follow-up studies.
Although this within-patient study systematically assessed the effect of dose and reconstruction on emphysema quantification, there are several limitations. First, the patients included in this study had a low amount of emphysema. Second, the sample size was relatively low; however, due to the within-patients study design, the statistical power of the study was increased. Although we showed that adapting the commonly used thresholds can prevent underestimation of emphysema with IR, the sample size was too small to give a clear recommendation about the optimal threshold. Third, one software package and IR algorithms from only one vendor were studied and results may differ for other packages and other vendors. Fourth, only an inspiratory chest CT was acquired; therefore, air-trapping could not be studied. Fifth, the effect of slice thickness and reconstruction kernel were not investigated in the current article. Gierada et al. [30] investigated the effect of reconstruction kernel and slice thickness and reported that patients with 10–30% emphysema are most sensitive for the effect of kernel and slice thickness, while lower emphysema percentages (such as in the current study) resulted in more stable measurements.
In conclusion, as compared to FBP at routine dose, both HIR and MIR result in an underestimation of CT emphysema at routine dose and reduced dose while FBP results in an overestimation at reduced dose. This can potentially be solved by using adapted thresholds.
Additional files
Table S1. Effect of different HU thresholds on emphysema quantification. Values represent the median [interquartile range] percentage emphysema at each dose level with FBP, HIR and MIR. FBP filtered back projection, HIR hybrid iterative reconstruction; MIR model-based iterative reconstruction, NA not applicable. Table S2. Effect of different percentiles on emphysema quantification. Values represent the median [interquartile range] HU value at each dose level with FBP. FBP filtered back projection; NA not applicable. Table S3. Effect of different percentiles on emphysema quantification. Values represent the median [interquartile range] HU value at each dose level with HIR. HIR hybrid iterative reconstruction; NA not applicable. Table S4. Effect of different percentiles on emphysema quantification. Values represent the median [interquartile range] HU value at each dose level with MIR. MIR model-based iterative reconstruction. (DOCX 35 kb)
Figure S1. Bland–Altman plots for the differences in percentage emphysema when comparing the optimal adapted threshold at each dose level to FBP at routine dose using a − 950 HU threshold. The continuous line represents the mean difference to the reference standard while the dotted lines represent the upper and lower limits of agreement (95% limits of agreement). FBP filtered back projection, HIR hybrid iterative reconstruction; MIR model-based iterative reconstruction. Figure S2. Bland–Altman plots for the differences in HU value when comparing the optimal adapted threshold at each dose level with FBP at routine dose using the perc15 method. The continuous line represents the mean difference to the reference standard while the dotted lines represent the upper and lower limits of agreement (95% limits of agreement). FBP filtered back projection; HIR hybrid iterative reconstruction; MIR model-based iterative reconstruction. (PDF 578 kb)
Availability of data and materials
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Funding
The authors state that this work has not received any funding.
Acknowledgements
The authors would like to thank Ilse van Rein and Sylvia van der Werf for their help with the data collection.
Abbreviation
- CNR
Contrast-to-noise ratio
- COPD
Obstructive pulmonary disease
- CT
Computed tomography
- CTDIvol
Volume CT dose index
- DLP
Dose-length product
- FBP
Filtered back projection
- HIR
Hybrid IR
- ICC
Intraclass correlation coefficient
- IR
Iterative reconstruction
- MIR
Model-based IR
Authors’ contributions
Data collection: AH, SL. Data analysis and interpretation: AH, SL, EB. Drafting the article: AH, SL, EB. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Institutional Review Board approval was obtained. Written informed consent was obtained from all subjects (patients) in this study.
Consent for publication
All authors provided consent for publication.
Competing interests
Julien Milles is an employee of Philips Healthcare. All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral 12with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Prosch H. Implementation of lung cancer screening: promises and hurdles. Transl Lung Cancer Res. 2014;3:286–290. doi: 10.3978/j.issn.2218-6751.2014.09.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pompe Esther, Galbán Craig J., Ross Brian D., Koenderman Leo, ten Hacken Nick HT., Postma Dirkje S., van den Berge Maarten, de Jong Pim A., Lammers Jan-Willem J., Mohamed Hoesein Firdaus AA. Parametric response mapping on chest computed tomography associates with clinical and functional parameters in chronic obstructive pulmonary disease. Respiratory Medicine. 2017;123:48–55. doi: 10.1016/j.rmed.2016.11.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mets OM, Schmidt M, Buckens CF, et al. Diagnosis of chronic obstructive pulmonary disease in lung cancer screening computed tomography scans: independent contribution of emphysema, air trapping and bronchial wall thickening. Respir Res. 2013;14:59. doi: 10.1186/1465-9921-14-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Madani Afarine, Van Muylem Alain, de Maertelaer Viviane, Zanen Jacqueline, Gevenois Pierre Alain. Pulmonary Emphysema: Size Distribution of Emphysematous Spaces on Multidetector CT Images—Comparison with Macroscopic and Microscopic Morphometry. Radiology. 2008;248(3):1036–1041. doi: 10.1148/radiol.2483071434. [DOI] [PubMed] [Google Scholar]
- 5.Madani Afarine, Zanen Jacqueline, de Maertelaer Viviane, Gevenois Pierre Alain. Pulmonary Emphysema: Objective Quantification at Multi–Detector Row CT—Comparison with Macroscopic and Microscopic Morphometry. Radiology. 2006;238(3):1036–1043. doi: 10.1148/radiol.2382042196. [DOI] [PubMed] [Google Scholar]
- 6.Mohamed Hoesein FA, de Jong PA. Landmark papers in respiratory medicine: automatic quantification of emphysema and airways disease on computed tomography. Breathe (Sheff) 2016;12:79–81. doi: 10.1183/20734735.013415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mohamed Hoesein FA, de Hoop B, Zanen P, et al. CT-quantified emphysema in male heavy smokers: association with lung function decline. Thorax. 2011;66:782–787. doi: 10.1136/thx.2010.145995. [DOI] [PubMed] [Google Scholar]
- 8.Ostridge K, Wilkinson TM. Present and future utility of computed tomography scanning in the assessment and management of COPD. Eur Respir J. 2016;48:216–228. doi: 10.1183/13993003.00041-2016. [DOI] [PubMed] [Google Scholar]
- 9.Bankier Alexander A., De Maertelaer Viviane, Keyzer Caroline, Gevenois Pierre Alain. Pulmonary Emphysema: Subjective Visual Grading versus Objective Quantification with Macroscopic Morphometry and Thin-Section CT Densitometry. Radiology. 1999;211(3):851–858. doi: 10.1148/radiology.211.3.r99jn05851. [DOI] [PubMed] [Google Scholar]
- 10.Pistolesi M. Beyond airflow limitation: another look at COPD. Thorax. 2009;64:2–4. doi: 10.1136/thx.2008.106674. [DOI] [PubMed] [Google Scholar]
- 11.Willemink MJ, de Jong PA, Leiner T, et al. Iterative reconstruction techniques for computed tomography part 1: technical principles. Eur Radiol. 2013;23:1623–1631. doi: 10.1007/s00330-012-2765-y. [DOI] [PubMed] [Google Scholar]
- 12.Willemink MJ, Leiner T, de Jong PA, et al. Iterative reconstruction techniques for computed tomography part 2: initial results in dose reduction and image quality. Eur Radiol. 2013;23:1632–1642. doi: 10.1007/s00330-012-2764-z. [DOI] [PubMed] [Google Scholar]
- 13.den Harder AM, Willemink MJ, de Ruiter QM, et al. Achievable dose reduction using iterative reconstruction for chest computed tomography: a systematic review. Eur J Radiol. 2015;84:2307–2713. doi: 10.1016/j.ejrad.2015.07.011. [DOI] [PubMed] [Google Scholar]
- 14.Baumueller S, Winklehner A, Karlo C, et al. Low-dose CT of the lung: potential value of iterative reconstructions. Eur Radiol. 2012;22:2597–2606. doi: 10.1007/s00330-012-2524-0. [DOI] [PubMed] [Google Scholar]
- 15.Choo Ji Yung, Goo Jin Mo, Lee Chang Hyun, Park Chang Min, Park Sang Joon, Shim Mi-Suk. Quantitative analysis of emphysema and airway measurements according to iterative reconstruction algorithms: comparison of filtered back projection, adaptive statistical iterative reconstruction and model-based iterative reconstruction. European Radiology. 2013;24(4):799–806. doi: 10.1007/s00330-013-3078-5. [DOI] [PubMed] [Google Scholar]
- 16.Neroladaki Angeliki, Botsikas Diomidis, Boudabbous Sana, Becker Christoph D., Montet Xavier. Computed tomography of the chest with model-based iterative reconstruction using a radiation exposure similar to chest X-ray examination: preliminary observations. European Radiology. 2012;23(2):360–366. doi: 10.1007/s00330-012-2627-7. [DOI] [PubMed] [Google Scholar]
- 17.den Harder AM, Willemink MJ, van Hamersvelt RW, et al. Effect of radiation dose reduction and iterative reconstruction on computer-aided detection of pulmonary nodules: intra-individual comparison. Eur J Radiol. 2016;85:346–351. doi: 10.1016/j.ejrad.2015.12.003. [DOI] [PubMed] [Google Scholar]
- 18.den Harder AM, Willemink MJ, van Hamersvelt RW, et al. Pulmonary nodule volumetry at different low computed tomography radiation dose levels with hybrid and model-based iterative reconstruction: a within patient analysis. J Comput Assist Tomogr. 2016;40:578–583. doi: 10.1097/RCT.0000000000000408. [DOI] [PubMed] [Google Scholar]
- 19.Deak PD, Smal Y, Kalender WA. Multisection CT protocols: sex- and age-specific conversion factors used to determine effective dose from dose-length product. Radiology. 2010;257:158–166. doi: 10.1148/radiol.10100047. [DOI] [PubMed] [Google Scholar]
- 20.Hackx M, Bankier AA, Gevenois PA. Chronic obstructive pulmonary disease: CT quantification of airways disease. Radiology. 2012;265:34–48. doi: 10.1148/radiol.12111270. [DOI] [PubMed] [Google Scholar]
- 21.Madani Afarine, De Maertelaer Viviane, Zanen Jacqueline, Gevenois Pierre Alain. Pulmonary Emphysema: Radiation Dose and Section Thickness at Multidetector CT Quantification—Comparison with Macroscopic and Microscopic Morphometry. Radiology. 2007;243(1):250–257. doi: 10.1148/radiol.2431060194. [DOI] [PubMed] [Google Scholar]
- 22.Schilham A.M.R., van Ginneken B., Gietema H., Prokop M. Local noise weighted filtering for emphysema scoring of low-dose CT images. IEEE Transactions on Medical Imaging. 2006;25(4):451–463. doi: 10.1109/TMI.2006.871545. [DOI] [PubMed] [Google Scholar]
- 23.Mets OM, Willemink MJ, de Kort FP, et al. The effect of iterative reconstruction on computed tomography assessment of emphysema, air trapping and airway dimensions. Eur Radiol. 2012;22:2103–2109. doi: 10.1007/s00330-012-2489-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nishio M, Koyama H, Ohno Y, et al. Emphysema quantification using ultralow-dose CT with iterative reconstruction and filtered back projection. AJR Am J Roentgenol. 2016;206:1184–1192. doi: 10.2214/AJR.15.15684. [DOI] [PubMed] [Google Scholar]
- 25.Wang R, Sui X, Schoepf UJ, et al. Ultralow-radiation-dose chest CT: accuracy for lung densitometry and emphysema detection. AJR Am J Roentgenol. 2015;204:743–749. doi: 10.2214/AJR.14.13101. [DOI] [PubMed] [Google Scholar]
- 26.Nishio M, Matsumoto S, Ohno Y, et al. Emphysema quantification by low-dose CT: potential impact of adaptive iterative dose reduction using 3D processing. AJR Am J Roentgenol. 2012;199:595–601. doi: 10.2214/AJR.11.8174. [DOI] [PubMed] [Google Scholar]
- 27.Messerli M, Ottilinger T, Warschkow R, et al. Emphysema quantification and lung volumetry in chest X-ray equivalent ultralow dose CT - intra-individual comparison to standard dose CT. Eur J Radiol. 2017;91:1–9. doi: 10.1016/j.ejrad.2017.03.003. [DOI] [PubMed] [Google Scholar]
- 28.Nishio M, Matsumoto S, Seki S, et al. Emphysema quantification on low-dose CT using percentage of low-attenuation volume and size distribution of low-attenuation lung regions: effects of adaptive iterative dose reduction using 3D processing. Eur J Radiol. 2014;83:2268–2276. doi: 10.1016/j.ejrad.2014.09.011. [DOI] [PubMed] [Google Scholar]
- 29.Yuan R, Mayo JR, Hogg JC, et al. The effects of radiation dose and CT manufacturer on measurements of lung densitometry. Chest. 2007;132:617–623. doi: 10.1378/chest.06-2325. [DOI] [PubMed] [Google Scholar]
- 30.Gierada DS, Bierhals AJ, Choong CK, et al. Effects of CT section thickness and reconstruction kernel on emphysema quantification relationship to the magnitude of the CT emphysema index. Acad Radiol. 2010;17:146–156. doi: 10.1016/j.acra.2009.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Effect of different HU thresholds on emphysema quantification. Values represent the median [interquartile range] percentage emphysema at each dose level with FBP, HIR and MIR. FBP filtered back projection, HIR hybrid iterative reconstruction; MIR model-based iterative reconstruction, NA not applicable. Table S2. Effect of different percentiles on emphysema quantification. Values represent the median [interquartile range] HU value at each dose level with FBP. FBP filtered back projection; NA not applicable. Table S3. Effect of different percentiles on emphysema quantification. Values represent the median [interquartile range] HU value at each dose level with HIR. HIR hybrid iterative reconstruction; NA not applicable. Table S4. Effect of different percentiles on emphysema quantification. Values represent the median [interquartile range] HU value at each dose level with MIR. MIR model-based iterative reconstruction. (DOCX 35 kb)
Figure S1. Bland–Altman plots for the differences in percentage emphysema when comparing the optimal adapted threshold at each dose level to FBP at routine dose using a − 950 HU threshold. The continuous line represents the mean difference to the reference standard while the dotted lines represent the upper and lower limits of agreement (95% limits of agreement). FBP filtered back projection, HIR hybrid iterative reconstruction; MIR model-based iterative reconstruction. Figure S2. Bland–Altman plots for the differences in HU value when comparing the optimal adapted threshold at each dose level with FBP at routine dose using the perc15 method. The continuous line represents the mean difference to the reference standard while the dotted lines represent the upper and lower limits of agreement (95% limits of agreement). FBP filtered back projection; HIR hybrid iterative reconstruction; MIR model-based iterative reconstruction. (PDF 578 kb)