

Summary
Background
Emotional over‐eating (EOE) and emotional under‐eating (EUE) are common behaviours that develop in early childhood and are hypothesised to play a role in weight status. Data from a British twin cohort demonstrated that environmental, rather than genetic, factors shape individual differences in both behaviours in early childhood.
Objective
The aim of this current study was to replicate this finding in a subsample (n = 398) of 4‐year‐old twins selected for high or low risk of obesity from another population‐based cohort of British twins (the Twins Early Development Study).
Methods
Parental ratings of child EOE and EUE were analysed using genetic model fitting.
Results
Genetic influence was not significant, while shared environmental factors explained 71% (52–79%) of the variance in EOE and 77% (62–85%) in EUE. The two behaviours correlated positively (r = 0.53, 95% CI: 0.44, 0.61), and about two‐thirds of the shared environmental factors influencing EOE and EUE were the same (r C = 0.67, 95% CI: 0.51, 0.85).
Conclusions
Emotional eating in childhood is shaped by the home family environment; parents are therefore promising intervention targets.
Keywords: Childhood obesity, eating behaviour, emotional eating, twin research
Introduction
Stress and negative emotions can have differential impacts on appetite, with some individuals experiencing decreased, and some increased, desire to eat 1. These behaviours, termed emotional over‐eating (EOE) and emotional under‐eating (EUE), have been implicated in the development of childhood weight 2 and eating disorders 3. Data from the Gemini twin study (2402 families; 4804 twins) showed that both EOE 4 and EUE 5 are shaped primarily by the shared family environment, not by genes, in early childhood. This contrasts strongly with other eating behaviours found to be under substantial genetic control in early life 6, 7. Replication is an essential part of scientific progress 8, and here we aimed to verify the strong environmental component to child EOE and EUE in a sample selected for high and low obesity risk.
Methods
Data were from a subsample of the Twins Early Development Study 9, which included 214 pairs of twins from ‘obese’ and ‘lean’ families. One hundred sets of overweight or parents with obesity [maternal body mass index {BMI} > 28.5, paternal BMI > 25] and 114 healthy weight parents (both parents' BMI < 25) were identified and matched by social class, indexed using parental occupation. Families were visited at home for data collection when the twins were 4 years old 10. All anthropometrics were measured by the researchers. Parents indicated the ethnicity of their children by choosing between White and non‐White.
Parents reported on their children's emotional eating using the Child Eating Behaviour Questionnaire 11 subscales for EOE (four items, example item: ‘My child wants to eat more when irritable’) and EUE (four items, example item: ‘My child wants to eat less when sad’). BMI‐standard deviation (SD) scores were calculated for the children using British 1990 growth reference data 12, 13.
Analyses
Prior to analyses, EOE and EUE scores were regressed by gestational age, age at measurement and sex. The twin method compares the twin pair similarity of mono‐zygotic (MZ) and di‐zygotic (DZ) twin pairs to decompose variation in EOE and EUE into three latent factors – additive genetic influences (A, heritability), shared (C) and non‐shared environmental influences (E). A great difference between MZ and DZ twin similarity implies significant contribution from genetic factors, whereas similar twin correlations, regardless of zygosity, indicate a contribution of the shared environment. Here, in addition, a bivariate correlated factors model was used to derive aetiological correlations between EOE and EUE, indicating the extent to which the genetic (rA), shared environmental (rC) and unique environmental (rE) influences underlying the two behaviours are the same 14. Analyses use maximum likelihood structural equation modelling and were carried out using OpenMx 15, a statistical package in R.
Results
Data for EOE and EUE were available for 394 twins (197 pairs) when the children were 4 years old (Table 1). EOE and EUE correlated positively [r = 0.53, 95% confidence interval {CI}: 0.44, 0.61].
Table 1.
Descriptive statistics for the TEDS analysis sample
| Twin pairs | % or mean (SD) |
|---|---|
| Total | 197 pairs (394 children) |
| Zygosity | |
| MZ pairs* | 89 (45.2) |
| DZ pairs* | 108 (54.8) |
| Sex | |
| Males | 177 (44.9) |
| Females | 217 (55.1) |
| Gestational age (weeks) | 36.63 (2.61) |
| Age at measurement of EOE and EUE (years) | 4.41 (0.35) |
| Emotional over‐eating (EOE) | 1.84 (0.53) |
| Emotional under‐eating (EUE) | 2.84 (0.82) |
| Child BMI‐SDS | 0.45 (1.19) |
| Child weight status† | |
| Normal weight | 319 (81) |
| Overweight | 55 (14) |
| Obese | 16 (4) |
| Missing | 4 (1) |
| Maternal age at twin birth (years) | 34.80 (4.36) |
| Ethnicity | |
| White | 368 (93.4) |
| Non‐White | 26 (6.6) |
| Socio‐economic status‡ | |
| High | 76 (38.6%) |
| Intermediate | 78 (39.6%) |
| Low | 27 (13.7%) |
| Missing | 16 (8.1%) |
DZ, di‐zygotic; MZ, mono‐zygotic.
Weight status was derived using the International Obesity Task Force reference standards 16.
Families were grouped by the occupation of the highest earner per family: high (higher and lower managerial and professional occupations), intermediate (intermediate occupations, small employers and own account workers – self‐employed with no employees) and lower occupational classifications [lower supervisory and technical occupations, {semi‐} routine occupations, never worked and long‐term unemployed].
BMI‐SDS, body mass index‐standard deviation scores; SD, standard deviation; TEDS, Twins Early Development Study.
The full ACE model fitted the data well compared with the saturated model which estimates means and variances freely without any constraints (Δχ2 = 6.134, Δ Df = 17, p = 0.99). Heritability was not significant for either EOE (A = 0.03, 95% CI: 0.00, 0.25) or EUE (A = 0.04, 95% CI: 0.00, 0.21), but CIs were wide. Shared environmental influences were strong for both EOE (C = 0.71, 95% CI: 0.52, 0.79) and EUE (C = 0.77, 95% CI: 0.62, 0.85). The contributions from non‐shared environmental factors were moderate (EOE: E = 0.26, 95% CI: 0.19, 0.34; EUE: E = 0.19, 95% CI: 0.14, 0.25).
The aetiological correlations indicated that only shared environmental factors (rC = 0.67, 95% CI: 0.51, 0.85) were common to both behaviours because neither genetic nor non‐shared environmental correlations were significant (rE = 0.21, 95% CI: −0.00, 0.38; rA = 0.26, 95% CI: −1.00, 0.99). Figure 1 shows a path diagram illustrating the results.
Figure 1.
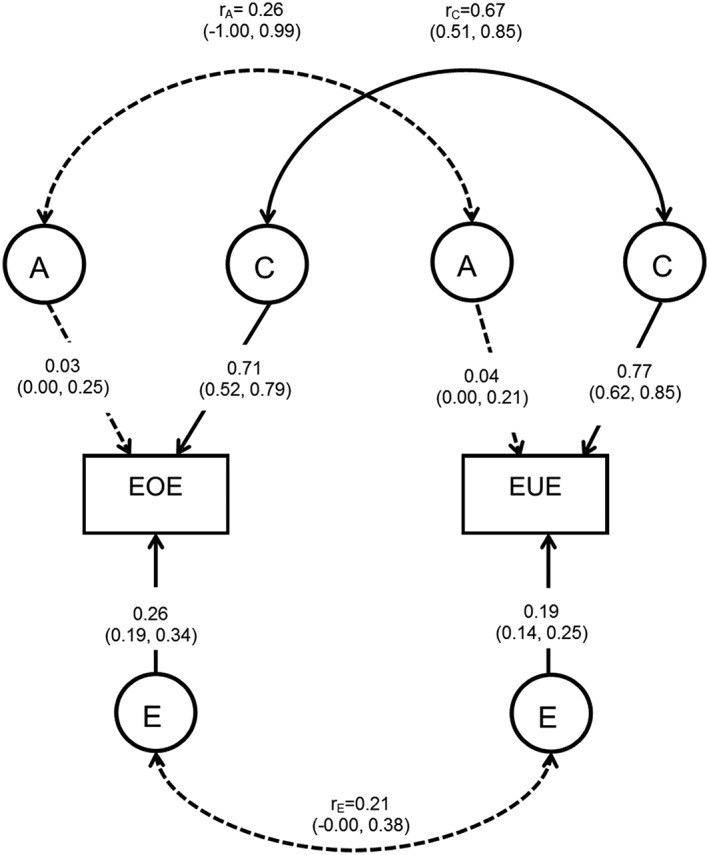
Correlated factors model of emotional over‐eating and emotional under‐eating. The rectangular boxes represent the measured phenotype [emotional over‐eating {EOE} and emotional under‐eating {EUE}] using the Child Eating Behaviour Questionnaire at 4 years of age. The circles indicate the latent factors: genetic effects (A), shared environmental effects (C) and non‐shared environmental effects (E). The straight single‐headed arrows reflect pathways with the variance explained by each latent factor [including 95% confidence intervals {CIs}]. The non‐significant A paths, with 95% CIs including 0, are represented as dotted lines. The aetiological correlations are shown on the curved double‐headed arrows. These indicate the extent of common genetic (rA), shared environmental (rC) and non‐shared environmental (rE) influences across the two phenotypes. The non‐significant aetiological correlations (rA and rE), with 95% CI crossing 0, are represented as dotted lines.
Discussion
This twin study of the aetiology of EOE and EUE in early childhood replicated previous findings from the Gemini twin cohort. As previously found 5, EOE and EUE correlated positively (r = 0.53), indicating that some children tend to both over‐eat and under‐eat in response to stress. Previous research has suggested that an individual's appetitive response to stress might be due to the nature and intensity of the stress – consistent low level stress relating to over‐eating, whereas intense stress might lead to under‐eating 17. Results supported that both behaviours are learned in childhood, with the shared environment exerting the strongest effect. Genetic contributions were minimal and non‐significant. Furthermore, EOE and EUE had some shared aetiology, in line with previous findings; approximately two thirds of the shared environmental influences on each behaviour were the same (rC = 0.67). Notably, this sample was selected to include families with varying degrees of obesity risk, increasing the heterogeneity and representativeness of the findings. The mean and SD of the BMI‐SD scores (mean = 0.45, SD = 1.19) indicated higher mean BMI than the UK population‐based reference data for children of this age and sex, as well as large weight variation in this sample. Limitations were the reduced sample size, leading to wide CIs, and the inclusion of only same‐sex DZ twin pairs, precluding testing for aetiological differences between boys and girls. Furthermore, parental weight is only one of many risk factors for child obesity and does not capture the full ‘picture’, and more research is needed to establish if the aetiology of EOE and EUE changes with developmental stage. The effect of stress on eating behaviour is complex, and a previous study has indicated a Gene–Environment interaction demonstrating that parents are more inclined to use maladaptive feeding strategies if their children are of increased genetic risk associated with emotional dysregulation 18.
In summary, this study supported that emotional eating is learned in early childhood, not inherited. Shared environmental factors, potentially parental feeding strategies such as emotional feeding 19, are key drivers of EOE and EUE regardless of a child's familial risk of obesity. These findings highlight family level factors as promising intervention targets for the prevention of emotional eating in children.
Conflict of interest statement
No conflict of interest was declared.
Author contributions
The authors' responsibilities were as follows: all authors (M. H., A. F. and C. L.) designed the research; M. H. performed the statistical analyses; and all authors wrote, read and approved the final manuscript.
Acknowledgements
We would like to thank the TEDS twins and their families for participating in the research. Data analysed came from a grant awarded to the late Professor Jane Wardle by the Biotechnology and Biological Sciences Research Council (31/D19086).
Herle M., Fildes A., and Llewellyn C. H. (2018) Emotional eating is learned not inherited in children, regardless of obesity risk, Pediatric Obesity. 13, 628–631, 10.1111/ijpo.12428.
References
- 1. Ashcroft J, Semmler C, Carnell S, van Jaarsveld CH, Wardle J. Continuity and stability of eating behaviour traits in children. Eur J Clin Nutr 2008; 62: 985–990. [DOI] [PubMed] [Google Scholar]
- 2. Parkinson KN, Drewett RF, Le Couteur AS, Adamson AJ, T GMSC . Do maternal ratings of appetite in infants predict later Child Eating Behaviour Questionnaire scores and body mass index? Appetite 2010; 54: 186–190. [DOI] [PubMed] [Google Scholar]
- 3. Kim YR, Heo SY, Kang H, Song KJ, Treasure J. Childhood risk factors in Korean women with anorexia nervosa: two sets of case‐control studies with retrospective comparisons. Int J Eat Disord 2010; 43: 589–595. [DOI] [PubMed] [Google Scholar]
- 4. Herle M, Fildes A, Rijsdijk F, Steinsbekk S, Llewellyn C. The home environment shapes emotional eating. Child Dev 2017. [DOI] [PubMed] [Google Scholar]
- 5. Herle M, Fildes A, Steinsbekk S, Rijsdijk F, Llewellyn CH. Emotional over‐ and under‐eating in early childhood are learned not inherited. Sci Rep‐Uk 2017; 7: 9092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Smith AD, Herle M, Fildes A, Cooke L, Steinsbekk S, Llewellyn CH. Food fussiness and food neophobia share a common etiology in early childhood. J Child Psychol Psychiatry 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Llewellyn CH, van Jaarsveld CH, Johnson L, Carnell S, Wardle J. Nature and nurture in infant appetite: analysis of the Gemini twin birth cohort. Am J Clin Nutr 2010; 91: 1172–1179. [DOI] [PubMed] [Google Scholar]
- 8. Munafò MR, Nosek BA, Bishop DVM, Button KS, Chambers CD, Percie du Sert N, Simonsohn U, Wagenmakers EJ, Ware JJ, Ioannidis JPA. A manifesto for reproducible science. 2017;1:0021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Trouton A, Spinath FM, Plomin R. Twins Early Development Study (TEDS): a multivariate, longitudinal genetic investigation of language, cognition and behavior problems in childhood. Twin Res 2002; 5: 444–448. [DOI] [PubMed] [Google Scholar]
- 10. Wardle J, Sanderson S, Guthrie CA, Rapoport L, Plomin R. Parental feeding style and the inter‐generational transmission of obesity risk. Obes Res 2002; 10: 453–462. [DOI] [PubMed] [Google Scholar]
- 11. Wardle J, Guthrie CA, Sanderson S, Rapoport L. Development of the Children's Eating Behaviour Questionnaire. J Child Psychol Psychiatry 2001; 42: 963–970. [DOI] [PubMed] [Google Scholar]
- 12. Freeman JV, Cole TJ, Chinn S, Jones PR, White EM, Preece MA. Cross sectional stature and weight reference curves for the UK, 1990. Arch Dis Child 1995; 73: 17–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Cole TJ. The Lms method for constructing normalized growth standards. Eur J Clin Nutr 1990; 44: 45–60. [PubMed] [Google Scholar]
- 14. Rijsdijk FV, Sham PC. Analytic approaches to twin data using structural equation models. Brief Bioinform 2002; 3: 119–133. [DOI] [PubMed] [Google Scholar]
- 15. Boker S, Neale M, Maes H, et al OpenMx: an open source extended structural equation modeling framework. Psychometrika 2011; 76: 306–317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. Brit Med J 2000; 320: 1240–1243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Macht M. How emotions affect eating: a five‐way model. Appetite 2008; 50: 1–11. [DOI] [PubMed] [Google Scholar]
- 18. Bost KK, Teran‐Garcia M, Donovan SM, Fiese BH, Team SK. Child body mass index, genotype and parenting in the prediction of restrictive feeding. Pediatr Obes 2018; 13: 239–246. [DOI] [PubMed] [Google Scholar]
- 19. Steinsbekk S, Barker ED, Llewellyn C, Fildes A, Wichstrom L. Emotional feeding and emotional eating: reciprocal processes and the influence of negative affectivity. Child Dev 2017. [DOI] [PubMed] [Google Scholar]