

Overview
Introduction
Among many treatments for shoulder stiffness, which is a common debilitating condition, arthroscopic capsular release is an effective surgical method for patients who have not responded to conservative treatment, as it provides visual control of the capsular release with a lower risk of potential traumatic damage than manipulation under anesthesia.
Step 1: Position the Patient
Place the patient either in the lateral decubitus position or in the beach-chair position, depending on one’s preference.
Step 2: Portal Placement
Create a standard posterior viewing portal, an anterior portal, and a lateral portal for approaching the glenohumeral joint and the subacromial space.
Step 3: Remove Rotator Interval Tissue
Begin the capsular release with the rotator interval and middle glenohumeral ligament using a 3.0-mm 90° electrocautery device through the anterior portal.
Step 4: Release the Anterior Capsule
Begin the anterior capsular release below the long head of the biceps tendon origin and preserve the glenoid labrum.
Step 5: Release the Inferior Capsule
As the electrocautery device may not reach the inferior portion of the inferior glenohumeral ligament, switch the working portal to the posterior portal for an easier approach to the inferior portion.
Step 6: Release the Coracohumeral Ligament and the Subscapularis
Begin this procedure with the camera in the lateral portal viewing the anterior portion of the subdeltoid space.
Step 7: Postoperative Rehabilitation
The goal for the patient is to achieve an immediate range of motion by performing active-assisted and passive range-of-motion exercises including pendulum circumduction or the pulley exercise.
Results
In our recently reported series of seventy-five patients who had a rotator cuff tear with simultaneous shoulder stiffness, treatment with an anterior and inferior capsular release showed favorable results.
What to Watch For
Introduction
Among many treatments for shoulder stiffness, which is a common debilitating condition, arthroscopic capsular release is an effective surgical method for patients who have not responded to conservative treatment1-3, as it provides visual control of the capsular release with a lower risk of potential traumatic damage than manipulation under anesthesia4,5. In addition, the accompanying shoulder pathology can be examined and treated with a simultaneous capsular release. Even though capsular release has shown favorable results, there have been many controversies regarding the extent of the release. The release of the rotator interval tissue is known to increase the range of flexion and external rotation6. Besides the rotator interval, release of the subscapularis tendon7, inferior capsule8, or global capsule9 can improve elevation and internal rotation, as well as external rotation. A posterior capsular release to improve internal rotation is controversial, with some authors advocating it10,11 and others stating it will not improve outcome compared with anterior release alone5,12,13.
In the present report, we demonstrate a simple way to release the anterior and inferior capsule, including the removal of rotator interval tissue, without incurring the morbidity of a posterior capsular release. The whole procedure is represented in seven steps.
Step 1: Position the Patient
Place the patient either in the lateral decubitus position or in the beach-chair position, depending on one’s preference.
Place the patient under anesthesia before the final positioning. With the patient in the lateral decubitus position, the position of the arm is from 60° to 70° of abduction and 15° to 20° of forward flexion.
Step 2: Portal Placement
Create a standard posterior viewing portal, an anterior portal, and a lateral portal for approaching the glenohumeral joint and the subacromial space.
Posterior Portal
Create a standard posterior viewing portal. The posterior portal is the first portal made during the arthroscopy that allows adequate visualization of the entire glenohumeral joint.
Make a small vertical incision 2 to 3 cm inferior and 1 to 2 cm medial to the posterolateral corner of the acromion14 (Fig. 1-A). For correct access to the glenohumeral joint, aim the direction of the trocar toward the coracoid process (Fig. 1-B). After the introduction of the trocar through the capsule, a popping sensation can be felt as the joint is entered. In a patient with severe stiffness, it is somewhat difficult for the trocar to enter the glenohumeral joint. Feeling the trocar tip placed between the humeral head and glenoid allows the correct placement of the portal within the glenohumeral joint. After proper placement of the trocar, diagnostic arthroscopy can be performed.
Figs. 1-A and 1-B Location of the portals and placement of the camera and electrocautery device.
Fig. 1-A.
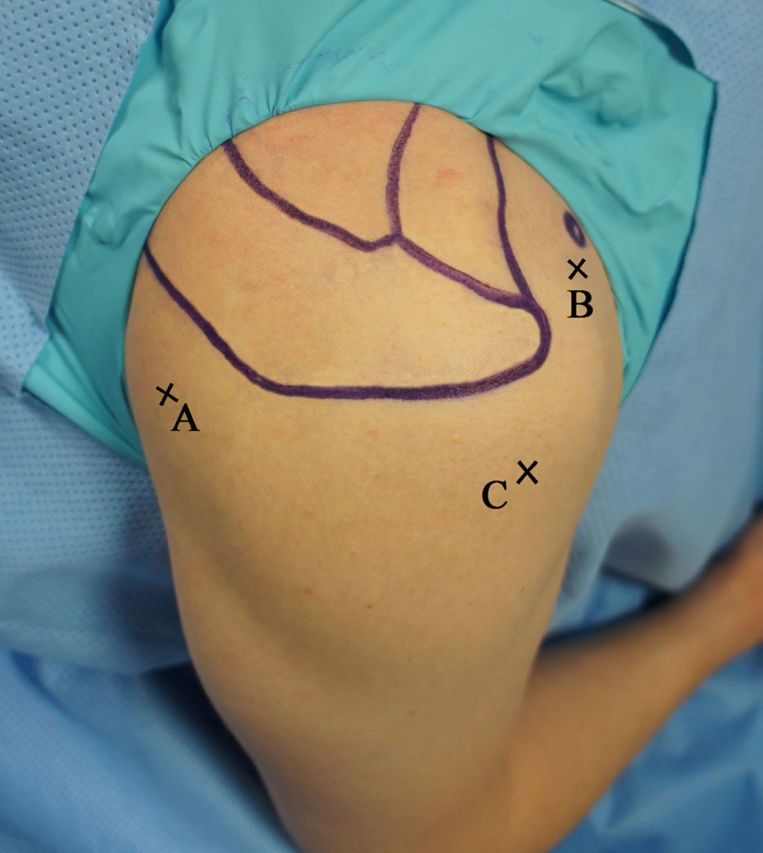
Portal locations are marked on the right shoulder. A = the posterior portal, B = the anterior portal, and C = the lateral portal.
Fig. 1-B.

The camera is placed in the posterior portal and the electrocautery device is in the anterior portal.
Anterior Portal
An anterior portal can be created by either an outside-in or an inside-out technique.
Perform the outside-in technique under the visualization of the arthroscope from the posterior portal. Introduce an 18-gauge spinal needle 1 to 2 cm inferomedial to the anterolateral corner of the acromion just lateral to the tip of the coracoid process (Figs. 1-A and 1-B). Take care to avoid damaging the brachial plexus and the axillary vessels that are located inferomedially15. Placing the anterior portal too inferiorly may damage the musculocutaneous nerve and cephalic vein.
Perform the inside-out technique by advancing the arthroscope toward the rotator interval just below the biceps tendon across the glenoid. Holding the cannula firmly, withdraw the arthroscope and insert a switching stick through the posterior portal. As advancement of the stick leads to skin tenting, make a small stab incision at the tip of the stick, which enables the stick to pass through the skin incision. Insert a cannula over the stick and gently advance it until the capsule is penetrated.
Lateral Portal
A lateral portal is commonly used to approach the subacromial space. Usually, it is used as a working portal for addressing the acromioclavicular joint pathology including resection of the distal end of the clavicle and acromioplasty. However, in the case of shoulder stiffness, it is used as a viewing portal for the visualization of the coracoid process and the superoanterior portion of the subscapularis.
Make the skin incision 2 cm lateral to the anterolateral edge of the acromion. Prior insertion of the spinal needle is helpful for the appropriate placement of the portal. Placing the portal too inferiorly may damage the axillary nerve, as it lies approximately 3 cm distal to the anterolateral margin of the acromion (Fig. 1-A).
Step 3: Remove Rotator Interval Tissue
Begin the capsular release with the rotator interval and the middle glenohumeral ligament using a 3.0-mm 90° electrocautery device (ArthroCare, Sunnyvale, California) through the anterior portal (Video 1).
When removing the interval tissue, begin the process superiorly with resection of the superior glenohumeral ligament and coracohumeral ligament. Continue the removal of tissue until the vertically oriented fibers of the coracoacromial ligament and conjoined tendon are visualized.
Video 1.
Removal of the rotator interval tissue including the coracohumeral ligament and superior glenohumeral ligament (SGHL) in the right shoulder with the patient in the left lateral decubitus position. The camera is in the posterior portal, and the operating instrument is in the anterior portal.
Step 4: Release the Anterior Capsule
Begin the anterior capsular release below the long head of the biceps tendon origin and preserve the glenoid labrum.
We recommend that the middle glenohumeral ligament be resected or divided without damaging the subscapularis tendon.
Carefully dissect the hypertrophied capsule without injuring the subscapularis (Video 2).
To avoid damage to the subscapularis, the tip of the electrocautery device should face the articular side during the process.
Continue the capsular release down to the 7 o’clock (right) or 5 o’clock (left) position, involving both the anterior and posterior bands of the inferior glenohumeral ligament.
Video 2.
Release of the anterior capsule including the middle glenohumeral ligament (MGHL) and anterior band of the inferior glenohumeral ligament (IGHL) in the right shoulder with the patient in the left lateral decubitus position. The camera is in the posterior portal, and the operating instrument is in the anterior portal.
Step 5: Release the Inferior Capsule
As the electrocautery device may not reach the inferior portion of the inferior glenohumeral ligament, switch the working portal to the posterior portal for an easier approach to the inferior portion.
After switching the portal, use the anterior portal as a viewing portal and the posterior portal as a working portal. From the posterior portal, the approach to the posterior portion of the inferior capsule is much easier (Fig. 2 and Video 3).
Starting from the previously released anterior capsule, extend the process to the 7 o’clock (right shoulder) and 5 o’clock (left shoulder) position of the inferior capsule. The release should be extended over the posterior band of the inferior glenohumeral ligament.
To avoid axillary nerve damage, perform the capsular release just off the glenoid rim without violating the glenoid labrum. According to Yoo et al.16, the closest distance between the axillary nerve and the glenoid, ranging from 10 to 25 mm, was with the arm in the neutral position, and the greatest distance was with the arm in abduction-neutral position. Therefore, we believe that axillary nerve damage can be prevented if the electrocautery tip stays within 10 mm of the glenoid rim. Also, the electrical conduction of the electrocautery discharge through the local tissues will stimulate the axillary nerve when it is in proximity so that damage can be prevented prior to direct injury.
Fig. 2.

The viewing and working portals are reversed compared with those shown in Figure 1-B. That is, the camera is placed in the anterior portal and the electrocautery device is placed in the posterior portal.
Video 3.
Release of the inferior portion of the inferior glenohumeral ligament (IGHL) in the right shoulder with the patient in the left lateral decubitus position. The camera is placed in the anterior portal, and the operating instrument is in the posterior portal.
Step 6: Release the Coracohumeral Ligament and the Subscapularis
Begin this procedure with the camera in the lateral portal viewing the anterior portion of the subdeltoid space.
Use the anterior portal as a working portal. Using the electrocautery device, find the base of the coracoid process. The part of the coracohumeral ligament that originates from the coracoid process and extends to the rotator interval is mostly removed during the process of rotator interval tissue removal. However, the coracohumeral ligament also extends over to the superior part of the subscapularis muscle and covers a broad area of the anterior surface of the subscapularis.
For the complete release of the coracohumeral ligament, thoroughly examine and debride the anterior and superior portion of the subscapularis (Video 4).
Video 4.
Release of the remnant coracohumeral ligament from the coracoid process and the anterior adhesion of the subscapularis (SSC) tendon in the right shoulder with the patient in the left lateral decubitus position. The camera is placed in the lateral portal, and the operating instrument is in the anterior portal.
Step 7: Postoperative Rehabilitation
The goal for the patient is to achieve an immediate range of motion by performing active-assisted and passive range-of-motion exercises, including pendulum circumduction or the pulley exercise.
Active-assisted and passive range-of-motion exercises can be started on the first postoperative day. If a simultaneous rotator cuff repair or reconstruction is performed, only gentle passive range-of-motion exercise is recommended, with the application of an abduction brace. For such patients, we also recommend that pulley exercises be started four weeks after the surgery.
The patient is instructed in a home-based exercise program and is encouraged to perform the exercises at least three times daily. Starting on the first day after the operation, pendulum circumduction, including gentle passive range-of-motion exercise, is done within a painless range. Pulley exercises are prescribed to increase flexion after one week. When the passive shoulder range of motion is restored to 90% of the normal range, isometric exercises in all planes are recommended. The patient is taught to perform exercises using a TheraBand (Hygenic, Akron, Ohio), strengthening exercises for the muscles stabilizing the scapula, and advanced muscle strengthening exercises using dumbbells. We recommend that the patient continue to perform all of these exercises regularly until the last visit at twelve months. No limit is imposed on the use of the shoulder within a tolerable extent.
Results
In our recently reported series of seventy-five patients who had a rotator cuff tear with simultaneous shoulder stiffness, treatment with an anterior and inferior capsular release showed favorable results13. The twenty-two male and fifty-three female patients had an average age of 56.4 years. The patients were randomized into two groups: one group had an anterior and inferior capsular release, and the other group had a capsular release that was extended to the posterior capsule. The patients were evaluated with the American Shoulder and Elbow Surgeons scoring system, the Simple Shoulder Test, and a visual analog scale for pain, and the shoulder range of motion was assessed, before surgery; at three, six, and twelve months after surgery; and at the latest follow-up. The functional scores and range of motion at an average of 18.4 months postoperatively showed significant improvement compared with the preoperative findings. However, no significant difference was found between the groups with regard to range of motion, pain, and functional scores with or without posterior capsular release. There were no complications from the surgical procedures. No shoulder developed recurrent stiffness or required repeat surgery.
What to Watch For
Indications
Contraindications
Pitfalls & Challenges
During the process of capsular release, be careful not to damage the subscapularis tendon and long head of the biceps tendon.
When removing the rotator interval tissue, be aware of the musculocutaneous nerve and try not to go too far medially beyond the coracoid process.
Axillary nerve injury is a devastating complication during the process of capsular release. When capsular release is done from the 5 o’clock to the 7 o’clock position (right side), or from the 7 o’clock to the 5 o’clock position (left side), the release should be done just off the glenoid rim without violating the glenoid labrum in order to avoid axillary nerve damage.
Clinical Comments
The release of the capsule should be continued until the muscle fibers are exposed.
If manipulation under anesthesia is needed prior to the arthroscopic procedure, avoid forceful manipulation of the joint. Forceful manipulation can lead to dislocation or fractures of the humeral head or neck or the glenoid, especially during external rotation.
We could not find any significant differences in the overall outcome between the anteroinferior capsular release and the extended posterior capsular release at each time point after capsular release. We cautiously state that there was no apparent benefit in terms of range of motion and functional scores with the additional posterior capsular release in the patients with shoulder stiffness.
Footnotes
Based on an original article: Am J Sports Med. 2014 May;42(5):1143-9.
Disclosure: None of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support of any aspect of this work. None of the authors, or their institution(s), have had any financial relationship, in the thirty-six months prior to submission of this work, with any entity in the biomedical arena that could be perceived to influence or have the potential to influence what is written in this work. Also, no author has had any other relationships, or has engaged in any other activities, that could be perceived to influence or have the potential to influence what is written in this work. The complete Disclosures of Potential Conflicts of Interest submitted by authors are always provided with the online version of the article.
References
- 1.Holloway GB, Schenk T, Williams GR, Ramsey ML, Iannotti JP. Arthroscopic capsular release for the treatment of refractory postoperative or post-fracture shoulder stiffness. J Bone Joint Surg Am. 2001. November;83(11):1682-7. [DOI] [PubMed] [Google Scholar]
- 2.Pollock RG, Duralde XA, Flatow EL, Bigliani LU. The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop Relat Res. 1994. July;304:30-6. [PubMed] [Google Scholar]
- 3.Segmüller HE, Taylor DE, Hogan CS, Saies AD, Hayes MG. Arthroscopic treatment of adhesive capsulitis. J Shoulder Elbow Surg. 1995. Nov-Dec;4(6):403-8. [DOI] [PubMed] [Google Scholar]
- 4.Harryman DT, 2nd, Matsen FA, 3rd, Sidles JA. Arthroscopic management of refractory shoulder stiffness. Arthroscopy. 1997. April;13(2):133-47. [DOI] [PubMed] [Google Scholar]
- 5.Snow M, Boutros I, Funk L. Posterior arthroscopic capsular release in frozen shoulder. Arthroscopy. 2009. January;25(1):19-23. Epub 2008 Oct 10. [DOI] [PubMed] [Google Scholar]
- 6.Harryman DT, 2nd, Sidles JA, Harris SL, Matsen FA., 3rd The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am. 1992. January;74(1):53-66. Epub 1992 Jan 1. [PubMed] [Google Scholar]
- 7.Pearsall AW, 4th, Holovacs TF, Speer KP. The intra-articular component of the subscapularis tendon: anatomic and histological correlation in reference to surgical release in patients with frozen-shoulder syndrome. Arthroscopy. 2000. April;16(3):236-42. Epub 2000 Apr 6. [DOI] [PubMed] [Google Scholar]
- 8.Massoud SN, Pearse EO, Levy O, Copeland SA. Operative management of the frozen shoulder in patients with diabetes. J Shoulder Elbow Surg. 2002. Nov-Dec;11(6):609-13. Epub 2002 Dec 7. [DOI] [PubMed] [Google Scholar]
- 9.Jerosch J. 360 degrees arthroscopic capsular release in patients with adhesive capsulitis of the glenohumeral joint—indication, surgical technique, results. Knee Surg Sports Traumatol Arthrosc. 2001. May;9(3):178-86. Epub 2001 Jun 26. [DOI] [PubMed] [Google Scholar]
- 10.Nicholson GP. Arthroscopic capsular release for stiff shoulders: effect of etiology on outcomes. Arthroscopy. 2003. January;19(1):40-9. Epub 2003 Jan 11. [DOI] [PubMed] [Google Scholar]
- 11.Ide J, Takagi K. Early and long-term results of arthroscopic treatment for shoulder stiffness. J Shoulder Elbow Surg. 2004. Mar-Apr;13(2):174-9. Epub 2004 Mar 5. [DOI] [PubMed] [Google Scholar]
- 12.Chen J, Chen S, Li Y, Hua Y, Li H. Is the extended release of the inferior glenohumeral ligament necessary for frozen shoulder? Arthroscopy. 2010. April;26(4):529-35. Epub 2010 Apr 7. [DOI] [PubMed] [Google Scholar]
- 13.Kim YS, Lee HJ, Park IJ. Clinical outcomes do not support arthroscopic posterior capsular release in addition to anterior release for shoulder stiffness: a randomized controlled study. Am J Sports Med. 2014. May;42(5):1143-9. Epub 2014 Feb 28. [DOI] [PubMed] [Google Scholar]
- 14.Andrews JR, Carson WG, Jr, Ortega K. Arthroscopy of the shoulder: technique and normal anatomy. Am J Sports Med. 1984. Jan-Feb;12(1):1-7. [DOI] [PubMed] [Google Scholar]
- 15.Paxton ES, Backus J, Keener J, Brophy RH. Shoulder arthroscopy: basic principles of positioning, anesthesia, and portal anatomy. J Am Acad Orthop Surg. 2013. June;21(6):332-42. [DOI] [PubMed] [Google Scholar]
- 16.Yoo JC, Kim JH, Ahn JH, Lee SH. Arthroscopic perspective of the axillary nerve in relation to the glenoid and arm position: a cadaveric study. Arthroscopy. 2007. December;23(12):1271-7. [DOI] [PubMed] [Google Scholar]
- 17.Neviaser AS, Neviaser RJ. Adhesive capsulitis of the shoulder. J Am Acad Orthop Surg. 2011. September;19(9):536-42. [DOI] [PubMed] [Google Scholar]
- 18.Levine WN, Kashyap CP, Bak SF, Ahmad CS, Blaine TA, Bigliani LU. Nonoperative management of idiopathic adhesive capsulitis. J Shoulder Elbow Surg. 2007. Sep-Oct;16(5):569-73. Epub 2007 May 24. [DOI] [PubMed] [Google Scholar]