

Abstract
Background:
Prostaglandin E1 (P) or methylcobalamin (M) treatment has been suggested as a therapeutic approach for diabetic peripheral neuropathy (DPN) in many clinical trial reports. However, the combined effects of 2 drugs still remain dubious.
Objective:
The aim of this report was to evaluate the efficacy of M plus P (M + P) for the treatment of DPN compared with that of P monotherapy, in order to provide a reference resource for rational drug use.
Methods:
Randomized controlled trials (RCTs) of M + P for DPN published up to September 2017 were searched. Risk ratio (RR), mean difference (MD), and 95% confidence interval (CI) were calculated and heterogeneity was assessed with the I2 test. Subgroup and sensitivity analyses were also performed. The outcomes measured were as follows: the clinical efficacy, median motor nerve conduction velocities (MNCV), median sensory nerve conduction velocity (SNCV), peroneal MNCV, peroneal SNCV, and adverse effects.
Results:
Sixteen RCTs with 1136 participants were included. Clinical efficacy of M + P combination therapy was significantly better than P monotherapy (fifteen trials; RR 1.25, 95% CI 1.18–1.32, P < .00001, I2 = 27%). Compared with P monotherapy, the pooled effects of M + P combination therapy on nerve conduction velocity were (MD 6.29, 95% CI 4.63–7.94, P < .00001, I2 = 90%) for median MNCV, (MD 5.68, 95% CI 3.53–7.83, P < .00001, I2 = 94%) for median SNCV, (MD 5.36, 95% CI 3.86–6.87, P < .00001, I2 = 92%) for peroneal MNCV, (MD 4.62, 95% CI 3.48–5.75, P < .00001, I2 = 86%) for peroneal SNCV. There were no serious adverse events associated with drug intervention.
Conclusions:
M + P combination therapy was superior to P monotherapy for improvement of neuropathic symptoms and NCVs in DPN patients. Moreover, no serious adverse events occur in combination therapy.
Keywords: diabetic peripheral neuropathy, efficacy, meta-analysis, methylcobalamin, nerve conduction velocity, prostaglandin E1
1. Introduction
As one of the most common complications of diabetes mellitus (DM), diabetic peripheral neuropathy (DPN) carries complicated pathogenesis which mainly lies on microcirculatory disturbance caused by impaired endothelial function,[1] while the endothelial dysfunction can be aggravated by elevated advanced glycation end products resulted from long-term hyperglycemia.[2] Therefore, peripheral neuropathy occurred at 5 to 10 years after the onset of type 2 diabetes, the atherosclerosis of major vessels, especially in the lower extremity arteries, also appeared in diabetic patients.[1] Which is to say, a vicious circle of “ischemia-inflammation” is set up, then, the onset and progression of DPN are accelerated.[3,4] Current therapeutic options for the treatment of DPN include good glycaemic control, nerve nurturing, oxidative-stress suppressing, microcirculation improving and others.[5] As there is no effective single therapy currently existing for DPN, combination therapy with multiple drugs is generally performed. Clinically, prostaglandin E1 (P) is mainly used to relax vessels, decrease hematic viscosity, inhibit platelet aggregation and improve microcirculation.[6] Methylcobalamin (M), a kind of endogenous coenzyme, promotes axon regeneration and myelinogenesis by increasing nucleic acid, protein and phosphatidylcholine synthesis.[7,8] M also can speed up nerve conduction velocities (NCVs) through accelerating delayed nerve impulse conduction.[7,9] By far, clinical performances of the 2 medications in the treatment of DPN have been demonstrated by various studies.[7,10,11]
Deng H et al suggested that treatment with M plus P (M + P) for patients with DPN was safe and could gain better outcomes in neuropathic symptoms and NCVs compared with M alone by meta-analysis.[12] Furthermore, compared with P monotherapy, the efficacy and safety of M + P combination therapy have also been explored by numerous studies in mainland China.[13–15] In order to understand the effects of M + P for DPN comprehensively, the present meta-analysis identified the efficacy and safety of M + P in DPN more precisely by retrieving data published in the randomized controlled trials (RCTs).
2. Methods
2.1. Search strategy
We retrieved the electronic databases of PubMed, Embase, Web of Science, Cochrane Library, Chinese BioMedical Database, Chinese National Knowledge Infrastructure Database and Wanfang Database (last search date September 2017) without language restrictions. The key terms used in this search were (diabetic peripheral neuropathy or diabetic neuropathy or diabetic neuropathies or DPN) and (M or mecobalamin or vitamin B12) and (P or alprostadil).
2.2. Study selection criteria
All the following inclusion criteria must be met for this study at the same time:
-
(1)
study design was RCT.
-
(2)
Patients had DM and distal symmetrical sensorimotor polyneuropathy of the limbs, the diagnostic criteria included standardized DM criteria of World Health Organization,[16] clinical assessments and nerve conduction.[12]
-
(3)
Patients were treated with combination therapy (M + P) versus monotherapy (P).
-
(4)
Data on symptoms and (or) NCVs could be extracted,
-
(5)
treatment duration was ≥14 days, and a full-text publication was available.
The exclusion criteria included:
-
(1)
sensorimotor polyneuropathy caused by other factors.
-
(2)
Trials with some deficiencies in data or study design.
-
(3)
Patients with DPN received oral administration of M and (or) P.
2.3. Data extraction
All potentially relevant data including patient baseline characteristics, trial durations, daily doses of M and P along with outcomes were extracted independently by the investigators from the collected studies. The primary outcomes of interest were clinical efficacy, median motor nerve conduction velocity (MNCV), median sensory nerve conduction velocity (SNCV), peroneal MNCV, and peroneal SNCV. Clinical efficacy was divided into 3 categories including markedly effective (disappearance of subjective symptoms, recovered tendon reflex, and NCV increased by at least 5 m/s), effective (alleviated subjective symptoms, improved tendon reflex, and NCV increased by at least 3 m/s) and ineffective (no improvement in symptoms, tendon reflex and NCV).[17] Moreover, secondary outcomes included adverse events.
2.4. Quality assessment
The established Jadad scale was used to assess the methodological quality of included studies by the authors.[18] Four to 7 points implied high-quality trials, and 0 to 3 points implied poor or low-quality trials.[16,19] The disputes during quality assessment were solved by consensus.
2.5. Ethical approval
All the data in present meta-analysis were extracted from the previous published studies, no ethical approval or patient consent was required.
2.6. Statistical analysis
Dichotomous data (efficacy) were expressed as risk ratio (RR) and 95% confidence intervals (95% CIs), and the weighted mean difference (MD) and 95% CIs were estimated for continuous data (NCVs). The statistical heterogeneity between trials was assessed by the Q-statistic and I2-test.[20] A significant Q-statistic (P ≤.10) indicated heterogeneity across studies. The random-effect (RE) model was used to pool the data when heterogeneity was confirmed (P ≤.10 or I2 ≥50% suggested significant heterogeneity among studies),[21] otherwise, the fixed-effect (FE) model was employed. Funnel plot was used to detect the possibility of publication bias. Sensitivity analysis was performed by excluding 1 trial at a time, starting from the trial with lower-quality, to further study the effect of a single trial on pooled data. Subgroup analyses were also conducted based on the treatment duration (≥28 days or <28 days). All tests were 2-sided and a value of P < .05 was regarded as statistically significant. Statistical analysis was performed using Revman Manager 5.3 software (Cochrane Collaboration, Oxford, UK).
3. Results
3.1. Description of the studies
The process of the study selection and literature search was displayed in Figure 1. The 205 potentially relevant articles were identified from the initial searches, but only 16 trials[12–14,22–34] satisfying the inclusion and exclusion criteria were selected for this meta-analysis. The key characteristics of the 16 RCTs and Jadad scores were presented in Table 1. The 576 DPN patients were included in the M + P combination therapy group and 560 DPN patients were included in the P monotherapy group. The daily doses of M were 0.1 mg or 0.5 mg or 1.0 mg, daily doses of P were 10 μg or 20 μg or 100 μg, respectively. The routes of drug administration included intravenous bolus injection or intravenous drip infusion; furthermore, intramuscular injection was also used for M administration. The treatment durations varied from 14 to 28 days in most studies except 1 trial[22] for 30 days and the other trial[25] for 56 days. Only 2 studies[14,25] with 4 points were of high quality and the remaining 14 trials with 3 or lower points were all of low quality. Five studies[24,25,27–29] reported the DM duration. Seven trials[12,14,22,25,27,30,33] did not differentiate the type of diabetes.
Figure 1.
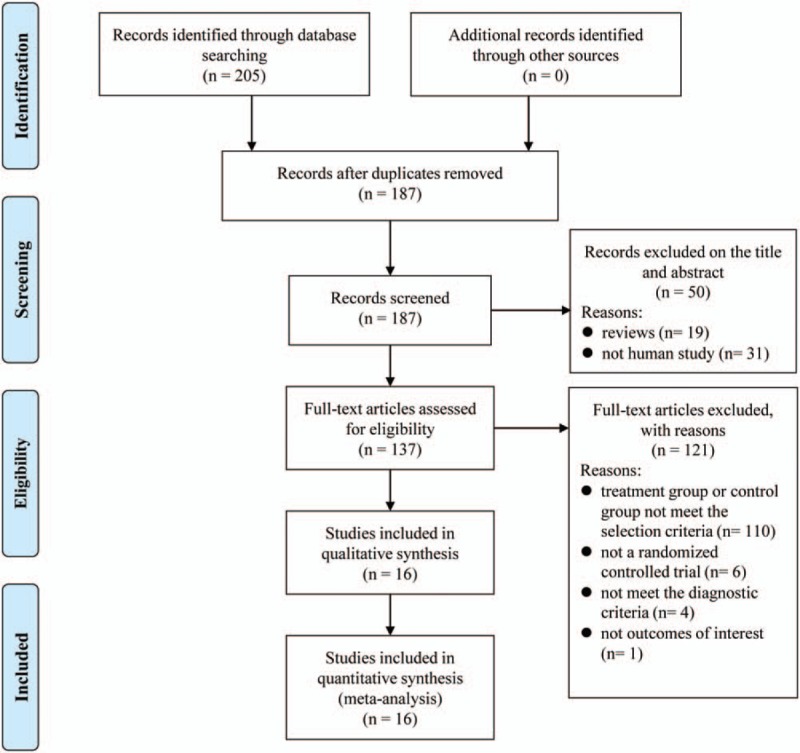
Map of the literature search and selection process.
Table 1.
Characteristics of the studies included in the meta-analysis.

3.2. Efficacy
Fifteen trials[12,13,22–34] involving 1052 patients measured the efficacy (534 patients received M + P combination therapy and 518 patients received P monotherapy). As shown in Figure 2, the FE model was used because insignificant heterogeneity between studies for the 2 groups was observed (P = .16, I2 = 27%). Compared with P monotherapy, M + P combination therapy for DPN significantly enhanced the efficacy (RR 1.25, 95% CI 1.18–1.32, P < .00001). The subgroup with ≥28 days of study duration showed moderate heterogeneity in efficacy outcome (I2 = 51%, P = .05). Figure 3 showed the funnel shape was not perfectly symmetrical, indicating a potential publication bias.
Figure 2.

Comparison of M + P combination therapy and P monotherapy in the efficacy for diabetic peripheral neuropathy, the former showed a better effect. P = prostaglandin E1, M = methylcobalamin.
Figure 3.

Funnel plot was not perfectly symmetrical, indicating the presence of between-study heterogeneity and a potential publication bias.
3.3. Median MNCV
Nine trials[12–14,22,25,27,28,32,34] involving 646 patients measured the median MNCV. Heterogeneity was significant for the analysis (P < .00001, I2 = 90%), the RE model was used. Compared with P monotherapy, median MNCV showed significant improvement in the M + P combination therapy group (MD 6.29, 95% CI 4.63–7.94, P < .00001) (Fig. 4A). On sensitivity analyses, after excluding the study reported by Li HJ,[25] the I2 value ranged from 90% to 71% and the overall effect ranged from 7.42 to 10.38. The subgroup with < 28 days of study duration showed moderate heterogeneity in median MNCV outcome (I2 = 57%, P = .07).
Figure 4.

M + P combination therapy improved the median MNCV (A) and median SNCV (B) significantly for treatment of diabetic peripheral neuropathy compared with P monotherapy. P = prostaglandin E1, M = methylcobalamin, MNCV = motor nerve conduction velocity, SNCV = sensory nerve conduction velocity.
3.4. Median SNCV
Nine trials[12–14,22,25,27,28,32,34] involving 646 patients measured the median SNCV. As shown in Figure 4B, the RE model was used because significant heterogeneity between studies for the 2 groups was observed (P < .00001, I2 = 94%). Compared with P monotherapy, M + P combination therapy increased median SNCV significantly (MD 5.68, 95% CI 3.53–7.83, P < .00001). On sensitivity analyses, we found the I2 value ranged from 89% to 95%, which indicated the result, was robust.
3.5. Peroneal MNCV
Eleven trials[12–14,22,24,25,27–29,32,34] involving 773 patients measured the peroneal MNCV. As shown in Figure 5A, the RE model was used because significant heterogeneity between studies for the two groups was observed (P < .00001, I2 = 92%). Compared with P monotherapy, M + P combination therapy accelerated peroneal MNCV significantly (MD 5.36, 95% CI 3.86–6.87, P < .00001). The sensitivity analyses showed that the I2 value ranged from 88% to 93% and the overall effect ranged from 6.07 to 7.60, which indicated the result was robust.
Figure 5.

Compared with P monotherapy, M + P combination therapy increased the peroneal MNCV (A) and peroneal SNCV (B) significantly for treatment of diabetic peripheral neuropathy. P = prostaglandin E1, M = methylcobalamin, MNCV = motor nerve conduction velocity, SNCV = sensory nerve conduction velocity.
3.6. Peroneal SNCV
Eleven trials[12–14,22,24,25,27–29,32,34] involving 773 patients measured the peroneal SNCV. As shown in Figure 5B, the RE model was used because significant heterogeneity between studies for the 2 groups was observed (P < .00001, I2 = 86%). Compared with P monotherapy, M + P combination therapy improved peroneal SNCV significantly (MD 4.62, 95% CI 3.48–5.75, P < .00001). On sensitivity analyses, we found the I2 value ranged from 80% to 88%, which indicated the result, was robust.
3.7. Safety
Eight studies[12,14,24–26,28,29,31] reported the adverse events, there were no serious treatment-related side effects during the treatment period in both M + P combination therapy group and P monotherapy group. Only some mild adverse effects including facial blushing (4 cases),[12,14,25] local skin redness (3 cases),[29] pain at the injection site (9 cases),[24,28] gastrointestinal discomfort (1 case),[25] dizziness (4 cases),[14,25,29] abdominal distention (3 cases),[12] limb burning (3 cases),[31] anepithymia (2 cases),[12] headache (2 cases)[25,28] and transient orthostatic hypotension (1 case)[26] in M + P combination therapy group, and facial blushing (2 cases),[14,29] pain at the injection site (12 cases),[24,25,28,29] abdominal distention (1 case),[12] limb burning (1 case),[31] anepithymia (2 cases),[12] headache (1 case),[28] transient orthostatic hypotension (1 case),[26] and dizziness (2 cases)[14,25] in P monotherapy group were reported. Because most studies did not report these side effects in detail, we were unable to analyze the rates of adverse events.
4. Discussion
With the raised prevalence of diabetes, the occurrence of DPN increases significantly and has become a leading cause of diabetes-related disability. Sensory neuropathy is a principal form of DPN, whose pathological changes include demyelination of nerve fibers, axonal degeneration, cell hyperplasia, and then fading-away of myelinated fibers.[3] Currently, DPN is believed to be closely related to various factors, including genetic predisposition, glucose toxicity, abnormal aldose reductase activity, oxidative stress.[5,35] Besides that, factors such as diabetic microangiopathy-induced hypoxic-ischemic neuronal death and altered hemodynamics, as well as disorder of intrinsic clotting, also play a vital role in the occurrence of DPN.[1,36] Therefore, regulating blood glucose homeostasis, improving the microcirculation of peripheral nerve endings, and suppressing oxidative stress are cures of DPN, moreover, significant treatment options for diabetic complications.
P, an efficient biological activator, induces vasodilation of blood vessels through activating intracelluar adenylate cyclase, enhances erythrocyte deformability, improves microcirculation disturbance, protects against ischemia-hypoxia injury in peripheral nerve tissue, and finally ameliorates the symptoms of peripheral nervous system involvement in the form of sensory impairment and diminished tendon jerks suggesting the presence of neuropathy.[37] In addition, P can reactivate Na(+)-K(+)-ATPase at the surfaces of nerve cells, improve neuronal metabolism and inhibit oxidation of the plasma membrane of a cell,[10,37] all of which contribute to the improvements of DPN. It has been demonstrated that P significantly improve the clinical symptoms of DPN and increase the conduction velocity of sensory and motor fibres in human median, peroneal nerves.[10,11,38]
M, a vitamin B12 analog, is involved in methyl transfer reactions in vivo by methylation. M is distributed to organelles in axons of nerve cells easily after being absorbed into the body, promotes nucleic acid and protein synthesis, and axon regeneration.[39,40] It also can stimulate phosphatidylcholine synthesis to increase myelinogenesis, and then speed up the motor and sensory NCVs.[41,42] Additionally, M accelerates NCVs directly by improving blocked nerve impulse conduction and decreased neurotransmitter levels.[43] Many studies suggested that M monotherapy or polytherapy with other drugs is an effective and safe therapy for patients with DPN.[25,44–46]
Our findings showed that, after P monotherapy and M + P combination therapy, DPN patients all had improvement in clinical symptoms and NCVs, while patients who received the later therapy showed significant higher-level improvement. Moreover, the results also indicated that synergistic potential existed in the course of combination therapy without severe adverse events. We executed subgroup and sensitivity analyses in order to minimize the influence of a particular study or an inferior study design. Results of subgroup analyses according to the study duration suggested that the efficacy and 4 NCVs benefits were seen in 2 subgroups (Table 2).
Table 2.
Subgroup analyses for efficacy and NCVs according to the treatment duration by meta-analysis.

Our analysis also has several limitations that must be taken into consideration when interpreting the results. First, the sample size of 3 trials was small.[29,32,33] Second, a reporting bias existed in our meta-analysis, due to only the data from published trials were included and the unpublished statistically nonsignificant results were excluded, but it would be very difficult to gain access to data from the unpublished studies. Third, because this study was a study-level meta-analysis, individual patient data were not included in the analysis, thus, we could not adjust for patient-level confounders. In addition, the small-study effect, insufficient number of trials, and significant statistical heterogeneity may result in the asymmetry of funnel plot, which indicated the likelihood of publication bias.
In summary, this meta-analysis suggests that DPN patients with M + P combination therapy have significant higher-level improvement in clinical symptoms and NCVs compared with P monotherapy. Moreover, the results also indicate that no serious adverse events occur during M + P combination therapy. But, due to poor methodological quality of the studies included, strong and definitive recommendations cannot be made for patients with DPN and further large-scale, well-designed RCTs are urgently needed.
Author contributions
Investigation: De-Qi Jiang, Shi-Hua Zhao, Ming-Xing Li.
Methodology: Shi-Hua Zhao, Li-Lin Jiang, Yong Wang.
Writing – original draft: De-Qi Jiang.
Writing – review & editing: Yan Wang.
Footnotes
Abbreviations: CI = confidence interval, DM = diabetes mellitus, DPN = diabetic peripheral neuropathy, FE = fixed-effect, M = methylcobalamin, MNCV = motor nerve conduction velocity, P = prostaglandin E1, RCTs = randomized controlled trials, RR = risk ratio, SNCV = sensory nerve conduction velocity.
This study was supported by grants from the Doctoral Scientific Research Foundation of Yulin Normal University of China (No. G2016006).
The authors have no conflicts of interest to disclose.
References
- [1].Flynn MD, Tooke JE. Diabetic neuropathy and the microcirculation. Diabet Med 1995;12:298–301. [DOI] [PubMed] [Google Scholar]
- [2].Kilo S, Berghoff M, Hilz M, et al. Neural and endothelial control of the microcirculation in diabetic peripheral neuropathy. Neurology 2000;54:1246–52. [DOI] [PubMed] [Google Scholar]
- [3].Dyck PJ, Giannini C. Pathologic alterations in the diabetic neuropathies of humans: a review. J Neuropathol Exp Neurol 1996;55:1181–93. [DOI] [PubMed] [Google Scholar]
- [4].Wang Y, Schmeichel AM, Iida H, et al. Enhanced inflammatory response via activation of NF-kappaB in acute experimental diabetic neuropathy subjected to ischemia-reperfusion injury. J Neurol Sci 2006;247:47–52. [DOI] [PubMed] [Google Scholar]
- [5].Tesfaye S, Stevens LK, Stephenson JM, et al. Prevalence of diabetic peripheral neuropathy and its relation to glycaemic control and potential risk factors: the EURODIAB IDDM complications Study. Diabetologia 1996;39:1377–84. [DOI] [PubMed] [Google Scholar]
- [6].Wilkens JH, Wilkens H, Elger B, et al. Cardiac and microcirculatory effects of different doses of prostaglandin E1 in man. Eur J Clin Pharmacol 1987;33:133–7. [DOI] [PubMed] [Google Scholar]
- [7].Kuwabara S, Nakazawa R, Azuma N, et al. Intravenous methylcobalamin treatment for uremic and diabetic neuropathy in chronic hemodialysis patients. Intern Med 1999;38:472–5. [DOI] [PubMed] [Google Scholar]
- [8].Jiang DQ, Li MX, Wang Y, et al. Effects of prostaglandin E1 plus methylcobalamin alone and in combination with lipoic acid on nerve conduction velocity in patients with diabetic peripheral neuropathy: A meta-analysis. Neurosci Lett 2015;594:23–9. [DOI] [PubMed] [Google Scholar]
- [9].Sun Y, Lai MS, Lu CJ. Effectiveness of vitamin B12 on diabetic neuropathy: systematic review of clinical controlled trials. Acta Neurol Taiwan 2005;14:48–54. [PubMed] [Google Scholar]
- [10].Akahori H, Takamura T, Hayakawa T, et al. Prostaglandin E1 in lipid microspheres ameliorates diabetic peripheral neuropathy: clinical usefulness of Semmes-Weinstein monofilaments for evaluating diabetic sensory abnormality. Diabetes Res Clin Pract 2004;64:153–9. [DOI] [PubMed] [Google Scholar]
- [11].Wu JD, Tao S, Jin X, et al. PGE1 improves diabetic peripheral neuropathy in patients with type 2 diabetes. Prostaglandins Other Lipid Mediat 2016;126:24–8. [DOI] [PubMed] [Google Scholar]
- [12].Deng H, Yin J, Zhang J, et al. Meta-analysis of methylcobalamin alone and in combination with prostaglandin E1 in the treatment of diabetic peripheral neuropathy. Endocrine 2014;46:445–54. [DOI] [PubMed] [Google Scholar]
- [13].An XQ, Sun JF, Jiang JR. Efficacy and safety of mecobalamine combined with alprostadil in treatment of diabetic peripheral neuropathy. J Clin Med Pract 2016;20:50–2. [Google Scholar]
- [14].Chen RL, Sun ZL. Analysis on mecobalamin combined with alprostadil in the treatment of elderly type 2 diabetic peripheral neuropathy. China Mod Doct 2014;52:132–4. [Google Scholar]
- [15].Pan LY, Liu R. Clinical effects observation of prostaglandin E1 and mecobalamine in the treatment of patients with diabetic peripheral neuropathy. J Commun Med 2015;13:41–2. [Google Scholar]
- [16].Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 1998;15:539–53. [DOI] [PubMed] [Google Scholar]
- [17].Xu Q, Pan J, Yu J, et al. Meta-analysis of methylcobalamin alone and in combination with lipoic acid in patients with diabetic peripheral neuropathy. Diabetes Res Clin Pract 2013;101:99–105. [DOI] [PubMed] [Google Scholar]
- [18].Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary. Control Clin Trials 1996;17:1–2. [DOI] [PubMed] [Google Scholar]
- [19].Moher D, Pham B, Jones A, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses. Lancet 1998;352:609–13. [DOI] [PubMed] [Google Scholar]
- [20].Cochran WG. The combination of estimates from different experiments. Biometrics 1954;10:101–29. [Google Scholar]
- [21].Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539–58. [DOI] [PubMed] [Google Scholar]
- [22].Dai HB. Clinical observation of mecobalamin combined with alprostadil in the treatment of diabetic peripheral neuropathy. Guide China Med 2011;9:216–7. [Google Scholar]
- [23].Feng LH, Feng YS, Li CX, et al. Combined therapeutic effects of mecobalamine and prostaglandin E1 on treating patients with peripheral neuropathy. Henan J Pract Nerv Dis 1999;2:25–6. [Google Scholar]
- [24].Fu QL, Rao GF. Effects and safety of methylcobalamin combined with alprostadil in the treatment of type 2 diabetes mellitus patients with peripheral neuropathy. Chin J Clin Pharmacol 2012;28:490–2. [Google Scholar]
- [25].Li HJ. Clinical study of prostaglandin E1 plus mecobalamine combination therapy for patients with diabetic neuropathy. Lab Med Clin 2014;11:485–6. [Google Scholar]
- [26].Li YH, Sun HB, Wang Q. Clinical efficacy of alprostadil combined with methylcobalamin in the treatment of diabetic patients with peripheral neuropathy. Guide China Med 2013;11:185–6. [Google Scholar]
- [27].Liu XL. Clinical observation of prostaglandin E1 combined with mecobalamine in the treatment of patients with diabetic neuropathy. Diabet New World 2015;35:41–3. [Google Scholar]
- [28].Liu Y, Zhou L, Xie XM. Clinical study of prostaglandin E1 combined with mecobalamine in the treatment of diabetic neuropathy. Baotou Med 2012;36:65–6. [Google Scholar]
- [29].Niu XH, Si QQ, Song Q. Combined therapeutic effects of mecobalamine and prostaglandin E1 for patients with diabetic peripheral neuropathy. J Clin Intern Med 2009;26:707–8. [Google Scholar]
- [30].Peng WD. Clinical analysis of alprostadil combined with methycobalamin treatment for 48 cases of diabetic neuropathy. China Prac Med 2013;8:156–7. [Google Scholar]
- [31].Wang ZH, Chen HY, Guo RQ. Combined therapeutic effect of alprostadil and mecobalamin on 128 patients with diabetic peripheral neuropathy. Chin J Pract Med 2009;36:2–3. [Google Scholar]
- [32].Yi LJ, Yue YH. Clinical efficacy of comprehensive treatment for patients with diabetic peripheral neuropathy. J Clin Exp Med 2005;4:25–7. [Google Scholar]
- [33].Yu JT, Xu CC. Efficacy analysis of alprostadil combined with mecobalamine in the treatment of diabetic peripheral neuropathy. Chin Foreign Med Res 2014;12:27–8. [Google Scholar]
- [34].Zhu XP, Zhu ZG. Clinical observation of combined therapeutic effect of prostaglandin E1 and mecobalamin on diabetic peripheral neuropathy. Bull Hunan Med Univ 2001;26:343–4. [PubMed] [Google Scholar]
- [35].Boulton AJ, Gries FA, Jervell JA. Guidelines for the diagnosis and outpatient management of diabetic peripheral neuropathy. Diabet Med 1998;15:508–14. [DOI] [PubMed] [Google Scholar]
- [36].Brooks B, Delaney-Robinson C, Molyneaux L, et al. Endothelial and neural regulation of skin microvascular blood flow in patients with diabetic peripheral neuropathy: effect of treatment with the isoform-specific protein kinase C beta inhibitor, ruboxistaurin. J Diabetes Complications 2008;22:88–95. [DOI] [PubMed] [Google Scholar]
- [37].Toyota T, Hirata Y, Ikeda Y, et al. Lipo-PGE1, a new lipid-encapsulated preparation of prostaglandin E1: placebo-and prostaglandin E1-controlled multicenter trials in patients with diabetic neuropathy and leg ulcers. Prostaglandins 1993;46:453–68. [DOI] [PubMed] [Google Scholar]
- [38].Hong L, Zhang J, Shen J. Clinical efficacy of different doses of lipo-prostaglandin E1 in the treatment of painful diabetic peripheral neuropathy. J Diabetes Complications 2015;29:1283–6. [DOI] [PubMed] [Google Scholar]
- [39].Okada K, Tanaka H, Temporin K, et al. Methylcobalamin increases Erk1/2 and Akt activities through the methylation cycle and promotes nerve regeneration in a rat sciatic nerve injury model. Exp Neurol 2010;222:191–203. [DOI] [PubMed] [Google Scholar]
- [40].Watanabe T, Kaji R, Oka N, et al. Ultra-high dose methylcobalamin promotes nerve regeneration in experimental acrylamide neuropathy. J Neurol Sci 1994;122:140–3. [DOI] [PubMed] [Google Scholar]
- [41].Jian-bo L, Cheng-ya W, Jia-wei C, et al. The preventive efficacy of methylcobalamin on rat peripheral neuropathy influenced by diabetes via neural IGF-1 levels. Nutr Neurosci 2010;13:79–86. [DOI] [PubMed] [Google Scholar]
- [42].Kikuchi M, Kashii S, Honda Y, et al. Protective effects of methylcobalamin, a vitamin B12 analog, against glutamate-induced neurotoxicity in retinal cell culture. Invest Ophthalmol Vis Sci 1997;38:848–54. [PubMed] [Google Scholar]
- [43].Yagihashi S, Tokui A, Kashiwamura H, et al. In vivo effect of methylcobalamin on the peripheral nerve structure in streptozotocin diabetic rats. Horm Metab Res 1982;14:10–3. [DOI] [PubMed] [Google Scholar]
- [44].Yaqub BA, Siddique A, Sulimani R. Effects of methylcobalamin on diabetic neuropathy. Clin Neurol Neurosurg 1992;94:105–11. [DOI] [PubMed] [Google Scholar]
- [45].Li S, Chen X, Li Q, et al. Effects of acetyl-L-carnitine and methylcobalamin for diabetic peripheral neuropathy: A multicenter, randomized, double-blind, controlled trial. J Diabetes Investig 2016;7:777–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Han Y, Wang M, Shen J, et al. Differential efficacy of methylcobalamin and alpha-lipoic acid treatment on symptoms of diabetic peripheral neuropathy. Minerva Endocrinol 2018;43:11–8. [DOI] [PubMed] [Google Scholar]