

Abstract
Achieving an adequate exposure in laryngoscopy is an extremely tedious task for the operating surgeon, especially for the anterior commissure lesions. Various maneuvers have been described to overcome this difficulty, but failed in providing an adequate exposure leading to a poor outcome. To create a device that can deliver uniform pressure over the laryngeal cartilage and succeed in providing an adequate exposure of the glottic lesion. A total of 44 patients were included in the study, divided into two groups containing 22 patients each. The distance at the level of anterior commissure from the superior border of the distal end of the laryngoscope was noted and compared. Group A subjected to digital cricoid pressure showed a mean distance of 9.09 of exposure with variance of 1.22 and Group B subjected to cricoid pressure with the cricoid catapult showed a mean distance of 11.76 with variance of 1.59. The groups were statistically analyzed using Anova Test and the test was found to be very significant (p < 0.0001). The catapult is made of a hanger defining its economics, which has a vital role in difficult intubations especially in anterior placed larynx, short neck and obese patients, also succeeds in providing an adequate exposure of the glottic lesion, (especially the anterior commissure) by delivering uniform pressure over the laryngeal cartilage, leading to a superior operative outcome.
Keywords: Catapult, Cricoid pressure, Anterior commissure, Intubation
Introduction
Laryngoscopy is an essential entity of ENT examination for visualizing any laryngeal pathology. It includes indirect laryngoscopy, direct laryngoscopy and micro-laryngoscopy. These laryngeal examinations are performed with the aid of laryngoscopes and endoscopes that are available. The most significant and common problem faced by the surgeons for examining the larynx, is the inadequate exposure of anterior portion of the glottis in the surgical field.
To overcome this difficulty in clinical practice, it is vital to select a laryngoscope of appropriate size and shape. The technique of application is also very crucial that includes proper patient positioning, placement of the laryngoscope along the path of least resistance and the most vital being correct application of force in manipulating the laryngeal framework. The laryngeal anterior commissure is a specific anatomic area of the glottis which often remains unnoticed despite of all the above mentioned measures exercised.
The anterior commissure is the midline anterior meeting point of the true vocal cords. It comprises of the anterior cord, the anterior junction of the two vocal cords, the thyroid cartilage and the Broyle’s ligament and a fibrous structure connecting the vocal ligaments to the cartilage. There is no perichondrium at that point, so the fibers extend directly from the vocal ligament into the cartilage [1]. Moreover, cancers of the larynx constitute about 25% of all head and neck malignancies [2]. Of these, the malignancies involving the anterior commissure are considered to have higher rate of recurrence after laser microsurgery for early glottic carcinoma. The treatment failures is attributed to either under-estimation of the disease due to the limited visualization of the anterior glottic lesion by video laryngoscopy or direct laryngoscopy, or under treatment due to inadequate exposure of the lesion [3]. Thus, one of the most challenging part posed to a surgeon in examining a glottic lesion is visualizing the anterior commissure adequately.
To overcome this difficulty of visualizing the anterior commissure lesion, the most commonly employed manoeuver is to apply adequate cricoid pressure after giving an optimal position. The cricoid pressure is applied by means of digital pressure or by applying silk tapes wrapped around the neck but these methods pose their own mechanical limitations. Here, in this article we describe a novel method of delivering this cricoid pressure with the help of a “wire hanger” which gives uniform pressure around the thyroid cartilage and provides an adequate exposure of the anterior commissure even in the absence of a skilled assistant.
Material and Method
This study is a prospective, single centred study of 44 patients subjected to micro-laryngoscopy hospitalized in the ENT department during the period of 15 November 2016 to 15 May 2017. Informed consent was taken from all the patients included in the study. Patients below the age of 10 years, patients with midline neck swellings, laryngeal cartilage fracture, burns and patients with stridulous breathing were excluded. These patients were divided into two groups each containing 22 patients, Group A subjected to digital cricoid pressure and Group B subjected to cricoid pressure with the cricoid catapult. All patients were subjected to Micro-Laryngoscopy with Kleinsasser laryngoscope under General Anesthesia. The distance at the level of anterior commissure from the superior border of the distal end of the laryngoscope was noted using a Photoshop CS6 application. The number of pixel was calculated in 1 cm of the scale using the measuring tool from the photoshop CS6 (‘P’ pixels per cm) and compared between the groups.
Making of Cricoid Catapult
A malleable steel wire hanger is used (Fig. 1).
Fig. 1.
Use of a malleable steel Hanger
The two limbs of the wire hanger are bent close to each other at both the lateral ends with the hook in the center (Fig. 2).
Fig. 2.

Bending of the hanger
The bent limbs of the wire hanger are cut at the distance of 5 cm from the center on both the ends (Fig. 3).
Fig. 3.
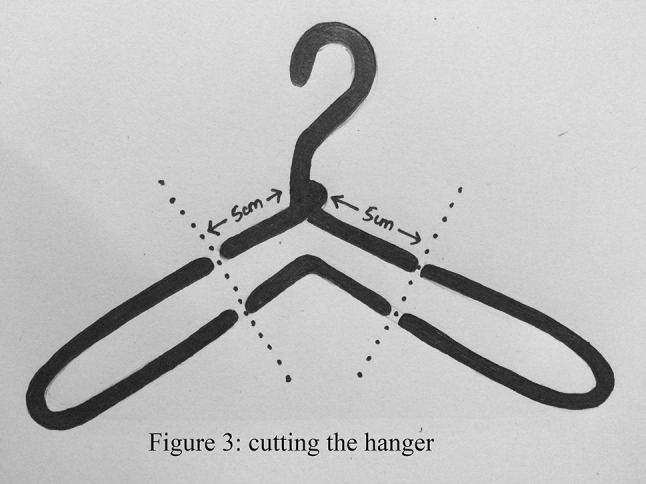
Cutting the limbs of the hanger
This cut wire hanger has two limbs one with the hook and the other the bent limb. The limbs are strapped together with the help of an elastic tape to make it soft, rigid with smooth edges and fixed in the position, resembling a catapult. (Fig. 4a, b).
Fig. 4.
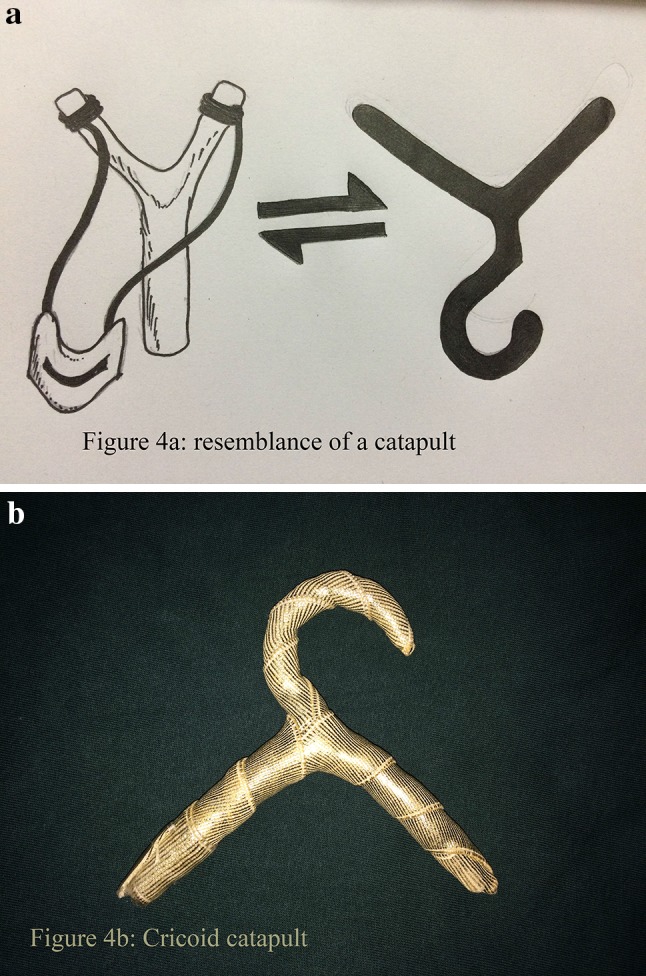
a Resemblance of the Catapult. b Cricoid catapult
Optimal positioning i.e. the sniffing position is essential prior doing a laryngeal examination [4]. The anesthetists use the catapult to view the glottis especially in difficult airway cases for easy and rapid intubation (Fig. 5). The laryngoscope of adequate size and type is inserted and after the glottis comes into view, the scope is fixed in place with the aid of chest piece in cases of micro-laryngoscopy. Once the assembly is in place, the cricoid catapult is placed at the mid-level of the thyroid cartilage lamina. The assistant gives pressure over the cartilage till the anterior commissure is visualized adequately. Once the position is confirmed by the operating surgeon who is seated at the head end, the assistant holds the catapult and maintains the same position with the required amount of force. (Figure 6) The distance at the level of anterior commissure from the superior border of the distal end of the laryngoscope was noted (Fig. 7a, b) using the photoshop CS6 application.
Fig. 5.

Use of catapult for intubation by the anesthetist
Fig. 6.

Cricoid pressure delivered with the catapult by the OT assistant
Fig. 7.

Exposure at the level of anterior commissure with a digital cricoid pressure. b Cricoid catapult
The hanger was specially used as the angulation formed between the two limbs at the center corresponds to the angulation of the thyroid lamina and the hook helps in holding the cricoid catapult in place. Moreover, the limbs of the malleable hanger could be bent in the particular angulation as per the angulation of the patient’s thyroid lamina vis-a-vis adult male (90 degree) and adult female (120 degree).
Advantages of cricoid catapult:
Gives adequate and complete exposure of the anterior commissure.
As the catapult is held by the assistant, both the hands of the surgeon are free for instrumentation.
Uniform pressure over the cartilage is maintained.
The cricoid catapult applied as and when demanded by the surgeon unlike the elastic tape that is strapped around the neck throughout the surgery.
Holding the cricoid catapult in place doesn’t require any skilled assistance.
It can be manipulated as per the patients cartilage framework.
In cases of difficult intubation in an anterior placed larynx, short neck, obese patients and in rapid sequence intubation this can be of help to the anesthetists.
Inexpensive, simple and effective.
Results
A total of 44 patients were included in the study with 26 male patients (59%) and 18 female patients (40%) (Table 1). These patients were divided into two groups each containing 22 patients, Group A containing 13 male and 9 female patients subjected to digital cricoid pressure and Group B containing 13 male and 9 female subjected to cricoid pressure with the cricoid catapult. The distance at the level of anterior commissure from the superior border of the distal end of the laryngoscope was noted in millimeter and compared between the groups. Group A showed a mean a distance of 9.09 with variance of 1.22 and Group B showed a mean distance of 11.76 with variance of 1.59 (Table 2). The groups were statistically analyzed using Anova Test and the test was found to be very significant (p < 0.0001).
Table 1.
Gender distribution
| No of patients | Percentage (%) | |
|---|---|---|
| Male | 26 | 59 |
| Female | 18 | 40 |
Table 2.
Mean distance at the level of anterior commissure among the groups
| Groups | Mean distance | Variance |
|---|---|---|
| Group A | 9.09 | 1.22 |
| Group B | 11.76 | 1.59 |
Discussion
Alfred Kirstein was the first to perform direct laryngoscopy and to describe direct visualization of the vocal cords. [5] Since the inception of laryngoscopy, the anterior commissure lesions have always posed a grave challenge in clinical practice, due to its anatomical location which hinders with its complete visualization. The inadequate exposure for the intended laryngoscopy and the repeated ill-judged attempts at laryngoscopy can lead to laryngeal injury, imperfect surgery, or may even lead to the abandonment of the procedure which may be infuriating and disappointing at times. In clinical practice to overcome these difficulties not only an appropriate selection of laryngoscope is crucial but, also a proper application technique which includes a proper head and neck positioning and adjunct it with perfect cricoid pressure for the better exposure.
Generally, the Jackson-Boyce position provides satisfactory glottic exposure to the surgeon who is seated on the head end of the patient. Extreme extension of the head on the neck and anterior flexion of the neck on the chest reduces the distance between the lips and larynx, resulting in maximum flaccidity of the soft tissues in the neck and better exposure of the glottis. In difficult patients, this may help in the visualization of the anterior glottis. However, with the patient in this position manipulation of the instruments becomes a tough task while performing microscopic surgery [6]. A variety of laryngoscopes are available of different sizes and shape. Laryngoscope selection is of utmost importance, but performing a successful surgery invariably depends on the nature of the procedure, the presenting problem, the ease of access, the anatomic site for close examination and the method of anesthesia. Though, the general rule is to use the larger caliber laryngoscope that can be placed with no or minimal trauma for better exposure and operative manipulation. Many surgeons believe that for adequate exposure of the vocal cords and anterior commissure the non-hinged micro-laryngoscopes of the Hollinger or Dedo variety with an upward flair at the distal tip were simple to use. These Anterior commissure laryngoscopes however, hampered the binocular vision when connected to the microscope. The other major disadvantage of these anterior commissure laryngoscopes were that the surgical laser beam when directed, used to escape close to the posterior lip of the tube due to the overhang that posed a great risk, as the beam may pass outside the tube to injure the patient’s lip, teeth, or gums [7].
Finally, many surgeons preferred the straight blade laryngoscopes over the curved blade laryngoscopes and among the various shapes of the glotto-scopes many preferred the one with a triangular distal tip which mimics the shape of glottis that provided a better anatomical orientation [8]. Despite all these measures if the extension of the anterior commissure couldn’t be achieved, the surgeon may consider for a constant cricoid pressure.
In 1774, Monro was the first who described Cricoid pressure (CP), he had used it on drowning victims to prevent gastric distention [9]. Later, this procedure was popularized by Sellick to prevent regurgitation of gastric contents during anesthesia induction. In his original description Sellick stated that “the manoeuver consists of temporary occlusion of the upper end of the esophagus by backward pressure of cricoid cartilage against bodies of cervical vertebrae” this manoeuver then became an integral part of rapid sequence induction [10]. Sellick also described that the depression of the thyroid cartilage posteriorly augmented the exposure of anterior larynx. This principle to manipulate larynx by firm pressure on the neck with fingers or hand for better visualization is frequently used by anesthesiologists to assist intubation [11]. The same principle of manual pressure was applied by the examiner or an assistant for the better visualization of the anterior commissure. Although cricoid pressure is a learnable skill, the potential risks in its application are laryngeal and cricoid cartilage fracture, potential injury to the cervical spine, esophageal rupture and catastrophic airway obstruction have been reported [12–14].
To deliver the cricoid pressure, the surgeon himself or the assistant may begin to apply the three finger digital pressure on the thyroid cartilage visualizing the larynx through the proximal end of the suspended laryngoscope. Alternatively, surgeon may consider using silk tape externally to exert constant cricoid pressure. The tape is strapped from the undersurface of the operating table on one side, over the cricoid and secured on the contralateral undersurface of the operating table in such a manner as to mimic digital pressure [8]. To further improve visualization, the larynx may need to be manipulated to one side, while internal counter pressure is maintained with the laryngoscope. Many a times, even a strong counter pressure may not reveal the anterior commissure. Moreover, the surgical field is more compromised due to the apparent increase in size of the endotracheal tube as it is displaced forward to bend across. Instead with the use of cricoid catapult overcomes the cumbersome act of tying the silk tape around the operation table and succeeds in delivering uniform pressure around the cartilage as and when required unlike the silk tape that is strapped around the neck throughout the surgery. Holding a cricoid catapult is although a learnable skill it can be delivered by any assistant, this gives the surgeon the privilege for instrumentation with both the hands unlike the cricoid pressure applied by the surgeon. Moreover, being a malleable tool it can be molded as per the patient’s cartilage framework and the pressure may be applied as per the surgeon’s demand which alleviates the complications of post-operative neck pain or any contusion or strap mark of the tape.
Limitation
Making the cricoid catapult requires requisite expertise. The anatomical and morpholoical differences among the patients were not considered in this study. The amount of pressure applied over the cartilage needs to be optimum. Improper application of cricoid pressure may cause trauma to the cartilage. Although, we didn’t encounter any trauma to the cartilage and none of the patient suffered any contusion or pain in the neck region post operatively.
Conclusion
Cricoid catapult is a convenient device that provides consistent and reproducible cricoid pressure. The skill required to use the instrument can be easily learnt. It abates the difficulty in visualizing the anterior commissure especially in circumstances where the availability of skilled assistance is limited, thus leading to a superior operative outcome and better quality of life.
Acknowledgement
I acknowledge the support of our head of the departments of ENT and Head & Neck Surgery and Anesthesia. I also acknowledge the support of nursing and technical staff who were involved in the process of surgery, postoperative care and other works. I also acknowledge all the patients who gave us consent and supported us for this. I acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. I am also grateful to the authors/editors/publishers of all those articles and journals from where the literature for this article has been reviewed and discussed. There were no special support sources/or grants used. There were no conflicts of interest.
Compliance with Ethical Standards
Conflict of interest
There is no conflict of interest.
References
- 1.Joshi VM, Wadhwa V, Mukherji SK. Imaging in laryngeal cancers–Bизyaлизaция paкa гopтaни [DOI] [PMC free article] [PubMed]
- 2.Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA: A Cancer J Clin. 2005;55(2):74–108. doi: 10.3322/canjclin.55.2.74. [DOI] [PubMed] [Google Scholar]
- 3.Rucci L, Gammarota L, Gallo O. Carcinoma of the anterior commissure of the larynx: II. Proposal of a new staging system. Ann Otol Rhinol Laryngol. 1996;105(5):391–396. doi: 10.1177/000348949610500512. [DOI] [PubMed] [Google Scholar]
- 4.El-Orbany M, Woehlck H, Salem MR. Head and neck position for direct laryngoscopy. Anesth Analg. 2011;113(1):103–109. doi: 10.1213/ANE.0b013e31821c7e9c. [DOI] [PubMed] [Google Scholar]
- 5.Reinhard M, Eberhardt E (1995) Alfred Kirstein (1863–1922) Pionier der direkten Laryngoskopie. AINS-Anästhesiologie· Intensivmedizin· Notfallmedizin· Schmerztherapie 30(04): 240–246 [DOI] [PubMed]
- 6.Zeitels SM, Vaughan CW, Domanowski GF. Endoscopic management of early supraglottic cancer. Ann Otol Rhinol Laryngol. 1990;99(12):951–956. doi: 10.1177/000348949009901204. [DOI] [PubMed] [Google Scholar]
- 7.Woodrow JH. Improved suspension laryngoscope for use with operative microscope. Trans Am Acad Ophthalmol Otolaryngol. 1971;75(2):412. [PubMed] [Google Scholar]
- 8.Sataloff RT, Chowdhury F, Portnoy JE, Hawkshaw MJ, Joglekar S (2013) Surgical techniques in otolaryngology-head and neck surgery: laryngeal surgery. JP Medical Ltd
- 9.Cullen W, Cathcart W. A letter to lord cathcart… concerning the recovery of persons drowned and seemingly dead. C. Elliot; 1784
- 10.Sellick BA. Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia. Lancet. 1961;278(7199):404–406. doi: 10.1016/S0140-6736(61)92485-0. [DOI] [PubMed] [Google Scholar]
- 11.Benjamin B, Lindholm CE. Systematic direct laryngoscopy: the Lindholm laryngoscopes. Ann Otol Rhinol Laryngol. 2003;112(9):787–797. doi: 10.1177/000348940311200908. [DOI] [PubMed] [Google Scholar]
- 12.Ralph SJ, Wareham CA. Rupture of the oesophagus during cricoid pressure. Anaesthesia. 1991;46(1):40–41. doi: 10.1111/j.1365-2044.1991.tb09314.x. [DOI] [PubMed] [Google Scholar]
- 13.Vanner RG, Pryle BJ. Regurgitation and oesophageal rupture with cricoid pressure: a cActaver study. Anaesthesia. 1992;47(9):732–735. doi: 10.1111/j.1365-2044.1992.tb03248.x. [DOI] [PubMed] [Google Scholar]
- 14.Gabbott DA. The effect of single-handed cricoid pressure on neck movement after applying manual in-line stabilisation. Anaesthesia. 1997;52(6):586–588. doi: 10.1111/j.1365-2044.1997.138-az0131.x. [DOI] [PubMed] [Google Scholar]