

Abstract
Purpose
Traditional heart-rate monitoring through the use of electrocardiograms or chest-worn heart rate sensors can be challenging in certain sports or in field settings. New technologies, such as photoplethysmography (PPG), have enabled heart-rate monitoring at alternate sites. However, to date, the accuracy and validity of various PPG sensors has not been examined in detail. The purpose of the present investigation was to determine the validity of an arm-worn PPG sensor during yoga sequences.
Methods
Fifteen college-aged men and women participated in a ~45 min power vinyasa yoga class. During the class, participants wore Polar ® H7 chest straps and RCX3 receivers (criterion) and Polar ® OH1 arm bands on their upper right arm (practical). Mean differences were compared via a paired t -test, heart rate during yoga using a time*device repeated measures ANOVA, and agreement assessed with Bland-Altman analysis.
Results
Mean heart rates during yoga were not different (mean difference=0.76, 95% CI: –0.54 to 2.06; p =0.229). Yoga created a main effect of time on heart rate ( p <0.0001), but there was no difference between devices ( p =0.86) or interaction ( p =0.90). Mean bias±95% limits of agreement was 0.76±1.30 bpm, with a typical error of 2.42±1.49 bpm and a coefficient of variation of 1.8±1.5%.
Conclusions
Results of the present investigation revealed that the Polar ® OH1 is a valid measure of heart rate during moderate-vigorous exercise. Future validation studies should consider other exercise modes and participant characteristics.
Key words: Yoga, Agreement, Validation, Photoplethysmography
Introduction
Heart-rate monitoring is widely used by athletes and the general public to quantify heart rate during training and provide real-time feedback 2 9 . Traditional heart-rate monitors include a chest-worn strap that transmits data to a wrist-worn receiver unit 2 9 . A limitation of the chest strap, however, is discomfort and possible skin irritation, especially in female users. In recent years, leaps in technology have enabled miniaturization and increased capability in heart-rate monitoring, including the potential to assess heart rate at sites besides the chest. This is due to the use of photoplethysmography (PPG) sensors. PPG is a non-invasive technique using LED lights as “probes” to emit light into the skin to interpolate heart rate based on changes in blood flow 11 .
To date, nearly all PPG sensors are wrist-worn. This may influence the quality of the PPG signal due to bones and other tissue in the area of the measurement site. For example, bioengineers have reported that the most significant challenge to wrist PPG is movement artifacts associated with tissue-induced noise and sensor movement 11 13 16 . Recent work has examined two of the more popular wrist-worn PPG units, the Apple Watch and the FitBit Charge HR. In one study, these devices were compared to ECG and found to be reasonably accurate (mean difference –1.3 and –9.3 bpm, respectively) but with large limits of agreement (LoA) 15 . Specifically, the LoA for the Apple Watch (–9.9 to 7.3 bpm) and the FitBit (–26 to 7.4 bpm) were rather wide during a 58-min protocol involving various activities (sitting, standing, treadmill and cycling exercise). Another study examined the Apple Watch during maximal exercise testing compared to a Polar T31 chest strap, and found regardless of wrist (left or right), that the mean difference was small (–1 bpm); however, LoA was still rather wide (–10 to 14 for the left and –4 to 6 for the right) 1 .
Recently (October 2017 in the USA), Polar ® released a stand-alone optical heart rate sensor (Polar ® OH1) that is worn on the forearm or upper arm. A comparable unit (Scosche Rhythm+) is a forearm monitor, which was recently evaluated during aerobic exercise (treadmill, cycling, and elliptical) at light, moderate, and vigorous intensities 4 . These authors reported that, compared to ECG, the Scosche had reasonable agreement at rest and during treadmill and cycling exercise, but not on the elliptical 4 . Because the OH1 and Scosche devices can be worn on forearm (and upper arm for the OH1), it is possible that these devices may avoid some of the movement artifacts and noise associated with wrist-worn PPGs. However, the OH1 has not yet been validated during exercise against an established criterion.
Yoga has also recently gained much attention and interest in the scientific community. Despite being around for several millennia, it was not until recently that yoga was considered as a possible form of exercise 14 . Yoga is characterized by poses and movements of varying difficulty, joined together in sequences 8 . There is a broad range of types of yoga, with “power” yoga, vinyasa yoga, and Bikram yoga being among the more popular 14 . In particular, yoga may appeal to individuals with limited mobility or joint injuries that preclude participation in other types of activity. Some research on the energetic and metabolic costs of yoga exist, with a recent review concluding most forms of yoga fall within the “light-to-moderate” physical activity category based upon metabolic equivalent (MET) costs 8 . Bikram yoga, typically done in hot and humid environments, elicits heart rates ~80% of age-predicted maximum 10 , but the cardiovascular demands of other forms of yoga, such as power vinyasa, deserve more attention.
Therefore, the purpose of the present study was to test the validity of the Polar ® OH1 PPG arm band when compared to a criterion measure (Polar ® H7 chest strap) during yoga sequences.
Methods
The present analysis is part of a larger study that examined heart rate and hydration responses to a power vinyasa yoga class. Results for that study are presently in review.
Participants
Fifteen men (n=3; mean age & BMI=26.75 years; 25.2±1.2 kg·m -2 ) and women (n=12; mean age & BMI=22.8±3.3 years; 22.6±3.7 kg·m -2 ) participated in ~45 min of yoga in a university human performance lab. The class was led by a 500-h certified yoga instructor. All participants were educated on risks and benefits, and provided informed consent before participation. The study was approved by the institutional Human Subjects Review board, and conformed to the guidelines required by the journal 5 and set forth under the Declaration of Helsinki.
Devices
The Polar ® OH1 ( Fig. 1 ) is a new optical heart rate sensor from Polar ® (Polar Electro Inc., Bethpage, NY, USA). In contrast to other PPG sensors typically worn on the wrist, the OH1 is worn on an armband on the lower or upper arm. For the present study, the device was worn on the upper right arm, distal to the biceps brachii. The sensor can transmit live data via Bluetooth ® to compatible Polar ® products or to compatible mobile devices where data can be observed via one of Polar’s applications (i. e., Polar ® Beat or Polar ® Flow). Alternately, the device can function as a standalone recorder, saving the data for later download. The OH1 records at 1- s intervals using 6 LED sensors.
Fig. 1.

Polar ® OH1 optical arm-band heart rate sensor. US quarter-dollar shown for scale.
The Polar ® H7 is a traditional electrode heart rate strap, which transmitted to a Polar ® RCX3 wrist receiver. The RCX3 recorded the H7’s heart rate data at 5-s intervals. The H7 has been found to be valid when compared to ECG, with a correlation of r=0.996 and a mean absolute percentage difference of 1.1% 4 . Other validation studies have utilized similar products 1 .
Procedures
Participants were instructed to arrive hydrated and at least 3 h after their last exercise bout. Upon arrival, they were weighed nude on a digital scale (Bluetooth Smart Scale Model #0375, Greater Goods Brand, St. Louis, MO, USA) behind a curtain. After this, they were fitted with the aforementioned heart rate monitors and were shown how to start the heart rate recordings before beginning the yoga class. Upon completion of the class, participants stopped the recordings, turned in the monitors, and reweighed themselves.
Statistical analysis
All heart rate data were uploaded via computer using Polar ® software (Polar Electro Inc., Bethpage, NY, USA). Raw data were downloaded for each participant as a Microsoft Excel © file. Data were checked for integrity and then averaged at 30-s intervals for analysis. To examine if differences existed between devices over time during the yoga class, data were imported to SPSS v. 24 (IBM Corp., Chicago, IL, USA) and analyzed with a 2-way (time*device) repeated-measures ANOVA. Mean heart rate data from the entire session were also examined using a paired samples t -test, and a Pearson correlation was also performed. Statistical significance was set as p<0.05.
Validity analysis was conducted using a freely available spreadsheet 6 . This spreadsheet provides Bland-Altman agreement data (bias and LoA), typical error of the estimate (TEE), and coefficient of variation (CV). According to a recent publication examining wrist-worn PPG sensors, the following criteria should be met for validation purposes: a correlation between devices of r≥0.90, and a mean bias of less than 3 bpm 7 .
Results
Mean±SD heart rates averaged over the entire yoga sequences were 131±15 bpm (H7) versus 130±14 bpm (OH1). A paired t -test revealed these means were not different (mean difference = –0.76 bpm, 95% CI: –2.06 to 0.54; t 14 =–1.26, p =0.229). The Pearson correlation between the means was r =0.987 ( p <0.0001).
The influence of the yoga class on heart rate, separated by device, is shown in Fig. 2 . The repeated-measures ANOVA revealed a main effect of time on heart rate ( F =139.85, p <0.0001), but no effect of device ( F =0.03, p =0.865) or device*time interaction ( F =0.81, p =0.90). Heart rate was lower during the first 6 and last 4 min of the class, compared to the middle 35 min ( p <0.045 for all comparisons).
Fig. 2.
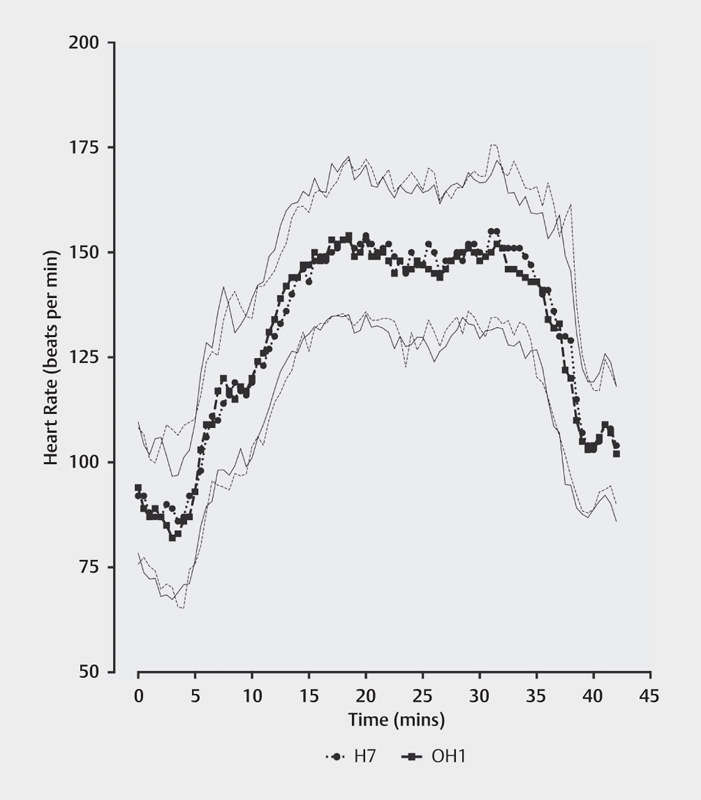
Heart rate during yoga exercise by device. Data are means±standard deviation. The dashed line with circles represents the Polar ® H7 (criterion) with the thin dotted lines representing the associated SD. The solid line with squares represents the Polar ® OH1, with the thin solid lines representing the associated SD.
Validity analysis revealed a small mean bias of –0.76 bpm (95% CI: –2.06 to 0.53 bpm). TEE was calculated as 2.42 bpm (95% CI: 1.76 to 3.91 bpm), while the CV was 1.8% (95% CI: 1.3 to 2.9%). Bland-Altman 95% LoAs were –3.83 to 5.35 bpm and are shown in Fig. 3 .
Fig. 3.
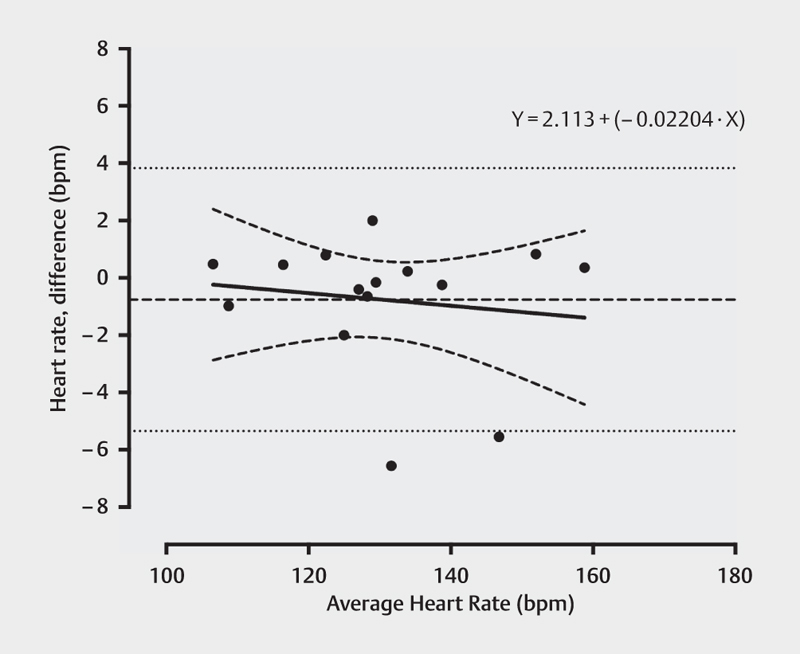
Bland-Altman plot with bias (bold dashed line) and 95% limits of agreement (dotted lines) comparing H7 and OH1. Solid line represents line of identity while bold dashed curves represent 95% confidence bands for the line of identity.
Discussion
The purpose of the present study was to compare a practical heart rate monitor using arm-based PPG to a criterion chest-strap unit. Results showed a high level of agreement between the units, therefore suggesting that the OH1 is a valid method of measuring heart rate during moderate-vigorous exercise (yoga).
Compared to wrist-worn sensors, our reported mean bias and LoAs are considerably smaller. For example, Wallen and colleagues reported a mean bias of –1.3 bpm (–9.9 to 7.3) for the Apple Watch and –9.3 bpm (–26 to 7.4) for the FitBit Charge HR, while Stahl et al. reported a mean absolute percentage error of 6.2% for the FitBit 12 15 . Jo and colleagues also reported similar mean bias and LoAs for the FitBit unit 7 . Our smaller LoAs are likely due to yoga being a largely static as opposed to dynamic mode of exercise (i. e., running, walking, cycling). However, it should be noted that when examining the Bland-Altman plot, two participants had their mean heart rates clearly underestimated (–6 and –7 bpm), and one participant had theirs overestimated (+2 bpm) ( Fig. 3 ). Regarding the two who had their heart rates underestimated, a closer analysis of the data revealed that one participant had their heart rate systematically underestimated for the first ~12 min before the two devices reached agreement; whereas for the second participant, during the middle ~20 min there were several large discrepancies between devices. We can only speculate that this was caused by device malfunction (improper set-up, low battery, loss of signal, etc.).
To our knowledge, only one other arm-based heart-rate monitor has been assessed for validity. Gillinov and colleagues examined the Scosche Rhythm+ during 3 modes of aerobic exercise (treadmill, cycle ergometer, and elliptical) 4 . The Scosche unit appeared to significantly underestimate HR compared to ECG when all conditions were compared in their analysis 4 . The LoAs were –31 to 38 bpm. This discrepancy is intriguing but is likely due to differences between the devices (i. e., number of LED lights), their algorithms, and mode/intensity of exercise 13 16 .
The foremost practical application of the current study is that an arm-worn heart rate sensor is valid, and this increases the potential of heart rate monitoring for athletes, coaches, and the general public. Arm-based heart rate monitoring, compared to chest-based monitoring, does offer a few advantages. For one, participants found the OH1 more comfortable and less irritating than the H7. Second, due to some of the yoga poses, the H7 would lose contact with the skin (i. e., it would “bow” out and away from the skin) or the watch was too far from the sensor, thereby reporting heart rate values of zero. The OH1 may particularly hold appeal for women, who would not have to go to a changing room to secure a chest strap under their clothing or worry about skin irritation from the heart-rate strap during exercise.
The intensity and associated heart rate responses to yoga have been poorly examined, but it is worth noting that our participants spent a significantly greater portion of the class time at intensities corresponding to moderate (60–75% HR MAX ) and vigorous (76–90% HR MAX ) compared to light-intensity exercise (16, 17, and 7 min, respectively, with the remaining 5 min at > 90% HRmax). Thus, we were able to elicit various levels of intensity, which strengthens the results and applications of the present study.
The primary limitation of the present study is that the study (and therefore, the comparison) is limited in scope (only one exercise mode was assessed). Yoga is a fairly static form of exercise; thus, dynamic exercise needs to be examined in the future. Inter- and intra-device reliability should also be assessed using both arms. Future studies should consider other exercise modes and individuals of various levels of adiposity to determine the validity of the OH1. It would also be worth conducting future studies comparing the OH1 with a wrist-based unit and collecting perceptual data from the participants on which one they find more comfortable. Another study could compare comfort and acceptance of wrist/arm/chest-based heart-rate monitoring between men and women.
A secondary limitation is the small homogenous sample size; thus, our results should be considered preliminary until larger studies with more robust and heterogeneous samples are completed. A tertiary limitation is the technology itself. Despite increased accuracy of PPG sensors in recent years 1 12 13 15 , much work and validation remains to be conducted, because results are not always in agreement 3 4 . Differences in agreement between studies are likely due to different criterion devices, exercise modalities, and study participants.
Conclusions
Results of the present study indicate that the OH1 is valid during yoga sequences at moderate and vigorous intensities, exhibiting excellent agreement with a traditional chest-worn heart-rate strap. Future studies should seek to determine the influence of other exercise modes and participant characteristics on OH1 validity.
Footnotes
Conflict of interest The authors declare that they have no conflict of interest.
References
- 1.Abt G, Bray J, Benson A C.The validity and inter-device variability of the Apple Watch for measuring maximal heart rate J Sports Sci 2017. 10.1080/02640414.2017.13972821–6. [DOI] [PubMed] [Google Scholar]
- 2.Achten J, Jeukendrup A E. Heart rate monitoring: applications and limitations. Sports Med. 2003;33:517–538. doi: 10.2165/00007256-200333070-00004. [DOI] [PubMed] [Google Scholar]
- 3.Boudreaux B D, Hebert E P, Hollander D B, Williams B M, Cormier C L, Naquin M R, Gillan W W, Gusew E E, Kraemer R R. Validity of wearable activity monitors during cycling and resistance exercise. Med Sci Sports Exerc. 2018;50:624–633. doi: 10.1249/MSS.0000000000001471. [DOI] [PubMed] [Google Scholar]
- 4.Gillinov S, Etiwy M, Wang R, Blackburn G, Phelan D, Gillinov A M, Houghtaling P, Javadikasgari H, Desai M Y. Variable accuracy of wearable heart rate nonitors during aerobic exercise. Med Sci Sports Exerc. 2017;49:1697–1703. doi: 10.1249/MSS.0000000000001284. [DOI] [PubMed] [Google Scholar]
- 5.Harriss D J, Macsween A, Atkinson G. Standards for ethics in sport and exercise science research: 2018 update. Int J Sports Med. 2017;38:1126–1131. doi: 10.1055/s-0043-124001. [DOI] [PubMed] [Google Scholar]
- 6.Hopkins W G. Spreadsheets for analysis of validity and reliability. Sportscience. 2015;19:36–42. [Google Scholar]
- 7.Jo E, Lewis K, Directo D, Kim M J, Dolezal B A. Validation of biofeedback wearables for photoplethysmographic heart rate tracking. J Sports Sci Med. 2016;15:540–547. [PMC free article] [PubMed] [Google Scholar]
- 8.Larson-Meyer D E. A systematic review of the energy cost and metabolic intensity of yoga. Med Sci Sports Exerc. 2016;48:1558–1569. doi: 10.1249/MSS.0000000000000922. [DOI] [PubMed] [Google Scholar]
- 9.Laukkanen R M, Virtanen P K.Heart rate monitors: state of the art J Sports Sci 199816SupplS3–S7. [DOI] [PubMed] [Google Scholar]
- 10.Pate J L, Buono M J. The physiological responses to Bikram yoga in novice and experienced practitioners. Altern Ther Health Med. 2014;20:12–18. [PubMed] [Google Scholar]
- 11.Spierer D K, Rosen Z, Litman L L, Fujii K. Validation of photoplethysmography as a method to detect heart rate during rest and exercise. J Med Eng Technol. 2015;39:264–271. doi: 10.3109/03091902.2015.1047536. [DOI] [PubMed] [Google Scholar]
- 12.Stahl S E, An H S, Dinkel D M, Noble J M, Lee J M. How accurate are the wrist-based heart rate monitors during walking and running activities? Are they accurate enough? BMJ Open Sport Exerc Med. 2016;2:e000106. doi: 10.1136/bmjsem-2015-000106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Temko A. Accurate heart rate nonitoring during physical exercises using PPG. IEEE Trans Biomed Eng. 2017;64:2016–2024. doi: 10.1109/TBME.2017.2676243. [DOI] [PubMed] [Google Scholar]
- 14.Thompson W R. Worldwide survey of fitness trends for 2018: The CREP Edition. ACMS Health Fit J. 2017;21:10–19. [Google Scholar]
- 15.Wallen M P, Gomersall S R, Keating S E, Wisloff U, Coombes J S. Accuracy of heart rate watches: implications for weight management. PLoS One. 2016;11:e0154420. doi: 10.1371/journal.pone.0154420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhang Z. Heart rate monitoring from wrist-type photoplethysmographic (PPG) signals during intensive physical exercise. In, 2014 IEEE Global Conference on Signal and Information Processing (GlobalSIP); 2014; 698–702