

Abstract
Femoral neck stress fractures (FNSFs) account for 3% of all sport-related stress fractures. The commonest causative sports are marathon and long-distance running.
The main types of FNSF are compression-sided, tension-sided and displaced. The most common reported symptom is exercise-related groin pain. Radiographs form the first line of investigation, with MRI the second-line investigation.
The management of FNSFs is guided by the location and displacement of the fracture. Delay in diagnosis is common and increases the likelihood of fracture displacement. Sporting outcomes are considerably worse for displaced fractures. Education programmes and treatment protocols can reduce the rates of displaced FNSFs.
This article aims to provide a current concepts review on the topic of FNSFs in sport, assess the current evidence on the epidemiology and pathophysiology of these injuries, detail the current recommendations for their imaging and management, and review the recorded sporting outcomes for FNSFs in the existing literature.
From this study, we conclude that although FNSFs are a rare injury, they should be considered in all athletes presenting with exercise-related hip pain, because delay in diagnosis and subsequent fracture displacement can significantly impair future return to sport. However, when detected early, FNSFs show promising results in terms of return-to-sport rates and times.
Key words: hip, pain, exercise, athlete, stress, fracture
Introduction
Femoral neck stress fractures (FNSFs) comprise around 3% of all stress fractures seen in the athlete 29 . Although rare, they have the potential to be one of the most serious injuries in sport, because left untreated, with subsequent fracture propagation and displacement, they can result in avascular necrosis (AVN) of the femoral head, necessitating a total hip replacement in a young athletic individual 37 . Around 50% of all athletes who suffer these injuries fail to return to previous sporting levels, with rates as high as 60% in those who suffer a displaced fracture 30 .
The initial reports of these injuries were published by German military surgeons in 1905 9 and 1936 4 . Between then and 1990, there had been a limited number of case series of these injuries, mainly from military personnel 12 22 24 60 . However, since the early 1990s, there have been increasing reports of this injury occurring in sporting individuals 30 39 46 49 , prompting the need for non-military medical staff to be more aware of FNSFs.
The importance of this condition is that if detected early and the injury is undisplaced, management and outcome have much higher success rates compared to FNSFs that remain undetected and displace 37 39 44 45 . Early detection and management of undisplaced FNSFs have been associated with return rates as high as 100% to previous functional capacity, with rates as low as 0% for both the development of femoral head AVN and the need for delayed surgical intervention 45 49 . In contrast, displaced FNSFs have been associated with military discharge rates as high as 100% 44 , with rates of post-treatment AVN and need for further intervention as high as 42% respectively 60 . Unsurprisingly, an increased awareness of such injuries among medical staff, along with educational programmes and established treatment protocols, has been shown to improve early detection of FNSFs, reducing rates of displaced fractures and improving outcomes of such injuries 44 45 52 .
This article aims to provide a current concepts review on the topic of FNSFs in sport, assess the current evidence on the epidemiology and pathophysiology of these injuries, detail the current recommendations for their imaging and management, and review the recorded sporting outcomes for FNSFs in the existing literature.
Methodology and Objectives
Methodology
The search methodology for the review comprised a systematic literature search in October 2016 of the following databases: Medline (PubMED), Cochrane Collaboration Database, EMBASE, SPORTDiscus, CINAHAL, Google Scholar, Physiotherapy Evidence Database (PEDro), Scopus and Web of Science. The key words used were ‘femoral’, ‘neck’, ‘stress’, ‘fracture’, ‘athlete’, ‘sports’ to locate all articles published in the English language in peer-reviewed journals that provided information on the epidemiology, pathophysiology, assessment, management and return to sport following treatment for FNSFs. There was no limit regarding the year of publication. All article categories including case reports, expert opinions, literature reviews, instructional courses, biomechanical reports, and technical notes were reviewed to determine if they provided relevant information
Objectives
The main objectives of the review article were to:
provide concise information on the epidemiology and risk factors for FNSFs;
detail the current concepts on the pathophysiology of these injuries;
define the standard clinical presentation and examination findings for FNSFs;
determine the evidence-based recommendations for radiological imaging of these injuries;
determine the evidence-based recommendations for management of these injuries;
review the evidence regarding return to sport for FNSFs;
establish the benefit of injury prevention programmes for this injury type.
Epidemiology and Risk Factors
Epidemiology
The only study to provide an accurate incidence of sport-related FNSFs is that by Hulko & Ovara 29 , who noted 9 FNSFs from a cohort of 368 stress fractures, recorded over a 14-year study period. The incidence of FNSFs will, however, vary based on the intensity and level of sport played, as well as the nature of the sport 53 .
As a cohort, FNSFs comprise around 3% of all stress fractures in athletes 29 . Regarding stress fractures of the femur, FNSFs represent the highest proportion of these, comprising 50% of such injuries 40 .
The reported mean age within FNSF cohorts varies from 16 to 56 years. Higher incidences of FNSFs are seen among female athletes 29 . Hulko & Ovara 29 noted that FNSFs comprised 4.1% of all stress fractures in their female athletes but only 1.8% of all stress fractures in their male athletes. Within athletic cohorts, the most commonly reported causative sports are marathon running, long-distance running, basketball, gymnastics and ballet dancing 8 30 37 39 .
Risk factors
Recent data from a case-control study of 47 military trainees who sustained FNSFs showed that the main risk factors for this injury were female gender and poor baseline physical fitness 35 . Body mass index was not observed as a risk factor 35 .
Key factors postulated for the increased risk seen in the female gender are the effects of abnormal physiology secondary to the components of the female athlete triad, namely disordered eating, amenorrhoea and decreased bone mineral density 26 27 35 43 .
Previous data by Pouilles et al. 47 also confirmed that decreased femoral bone mineral density (BMD) is associated with an increased risk of sustaining an FNSF. Pouilles et al. 47 found that the femoral BMD of military recruits who sustained FNSFs was around 10% less than a matched control cohort.
Further factors found to pre-dispose individuals to develop FNSFs include a sudden increase in training intensity, coxa vara, coxa profunda and acetabular retroversion, as seen in pincer-type femoral acetabular impingement (FAI) 14 25 39 . However, an established link between FNSF and FAI has yet to be confirmed 25 34 59 .
Classification, Pathophysiology and Biomechanics
Classification ( Fig. 1 )
Fig. 1.
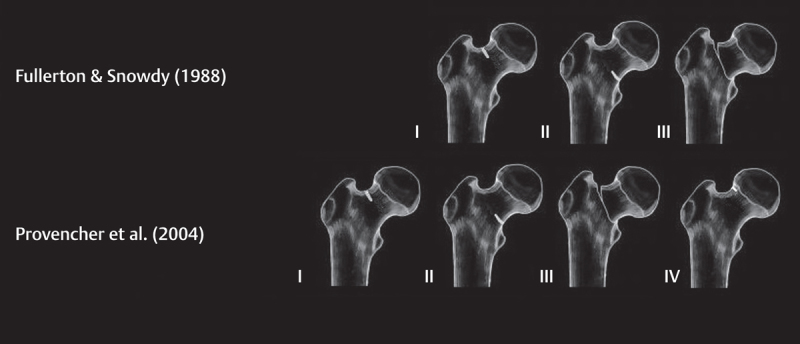
The classification systems for femoral neck stress fractures.
Since the 1960s, there have been multiple attempts to classify FNSFs 12 17 22 .
The mostly commonly used classification at present is that of Fullerton & Snowdy 24 , who categorized FNSFs into 3 groups, using both plain radiographs and bone scans. Type I fractures occurred on the tension-side of the femoral neck, type II fractures on the compression-side and type III fractures were displaced 24 .
This classification was further developed by Shin & Gillingham 53 . Based on MRI findings of FNSFs, they subdivided compression injuries into those without a fracture line, those with a fracture line less than 50% of the femoral neck width, and those with a fracture line greater than or equal to 50% of femoral neck width 53 .
Further additions to the Fullerton & Snowdy 24 classification include those by Provencher et al. 48 , who reported a fourth category, namely an atypical superiorly based incomplete tension-type fracture, which is routinely absent on plain radiographs though present on MRI 48 .
More recently, Arendt & Griffth 2 presented a MRI-based classification system that has been validated to predict the outcome of FNSF 2 49 . Divided into 4 grades, Grade 1 shows signal change on STIR sequencing exclusively; Grade 2 shows change on STIR and T2; Grade 3 shows change on STIR, T1, and T2 but with no fracture line present; and Grade 4 shows change on STIR, T1, and T2 but with a fracture line present 2 .
Pathophysiology and biomechanics
FNSFs develop in response to repetitive sub-maximal mechanical loads applied across the femoral neck, when the absorption of bone exceeds metabolic repair during the remodelling process 8 19 31 53 . The vast majority of FNSFs in athletes are fatigue fractures induced by repetitive loading of normal bone with abnormal forces 8 19 31 53 . However, FNSFs that develop along with female athlete triad are, in effect, partial insufficiency fractures, because they develop in abnormal bone 8 19 31 53 .
Forces up to 3 to 5 times body weight can be transferred along the femoral neck during activities such as jogging 19 53 . The vast majority of these are compressive-type forces, which occur at the inferior aspect of the neck 19 53 . Significant tensile forces can develop at the superior aspect of the femoral neck due to bending forces across the neck: however, these are normally counterbalanced through the stabilising forces of gluteus medius and minimus 19 53 .
Compression FNSFs develop from the compression forces at the inferior aspect of the femoral neck. When the forces applied exceed the elastic properties of bone and outpace the healing response of bone, microfractures develop and propagate at 45 degrees to the application of forces 19 53 . This creates an oblique fracture line across the femoral neck, which can remain stable until it exceeds around 50% of the femoral neck width 19 53 . The fracture line created with a compression fracture is more oblique than that of a tension fracture, and is thus more stable and less likely to displace 50 .
Tension FNSFs arise from the tension forces at the superior aspect of the femoral neck 19 53 . While normally counterbalanced by the forces of the gluteus medius and minimus, when these muscles fatigue, high tension forces develop across the superior femoral neck on load bearing 19 53 . This results in microfracture formation and propagation with subsequent fracturing of the superior aspect of the femoral neck 19 53 . Such a fracture line propagates at 90 degrees to the broken cortex, creating a transverse fracture, which is more unstable than that of the compression fracture, with a higher likelihood of displacement 19 53 . Note that altered hip geometry such as coxa vara can decrease the efficiency of the gluteal muscles, promoting early fatigue of these muscles and development of tension-sided FNSFs 14 .
Clinical Presentation, Examination and Investigations
Clinical presentation
The common presenting complaint with FNSFs is that of a gradual onset hip or groin pain that is poorly localized, aggravated by activity and weight-bearing, and ceases with rest 19 39 53 . The pain is most often sited at the anterior groin region (reported in 87% of patients in one study) 24 39 ; however this can be located at the thigh or gluteal region and can radiate to the knee 19 39 51 53 . Patients often note a recent increase in intensity or duration of exercise, such as preparation for a marathon or a sports event 19 39 53 .
Typically, the pain is initially noted late in activity and then increases in intensity with prolonged participation in exercise, often limiting or prohibiting further activity 19 24 39 53 . This is regularly associated with an antalgic gait 19 24 39 53 . Eventually the pain is noted at rest and at night 19 24 53 .
These symptoms can be followed by an episode of the hip giving way or ‘cracking’ or ‘popping’ during exercise as the fracture completes and displaces 26 27 . Occasionally, little pain is experienced until the patient suffers a complete fracture 19 53 .
As soon as the diagnosis of FNSF is suspected, the patient should cease weight-bearing on the affected hip and a screening radiograph should be performed urgently 8 19 53 .
Examination
Physical examination can often be non-specific, though the most consistent findings are pain at the extremes of hip range of motion (present in 79% of FNSF patients in one study) 24 39 , especially with internal rotation 19 39 53 . Tenderness on palpation over the anterior aspect of the hip and the inguinal area is also a common finding (present in 62% of FNSF patients in one study) 19 24 39 53 . The pain can be aggravated if the patient performs a straight-leg raise or if the examiner logrolls the thigh 19 53 . Heel strike testing is of limited value in diagnosing FNSF (present in 6% of FNSF patients in one study) 19 24 53 .
A complete examination should include assessment of the lower lumbar and sacral spine, the lower extremities, and the contralateral hip so that alternative causes for the symptoms are not missed 1 19 42 53 .
Investigations
Radiographs
Plain radiographs form the first-line imaging investigation for FNSFs 56 . An anteroposterior view of the pelvis (including the proximal third of the femur) and a direct lateral view of the proximal femora should be acquired 10 19 53 56 in all athletes who present with exercise-related hip or groin pain that is exacerbated by weight-bearing.
When present, the key radiographic changes are periosteal and endosteal callous formation, a sclerotic linear region traversing the primary trabeculae of the femoral neck and a radiolucent fracture line ( Fig. 2 ) 10 56 . Such changes, however, are often subtle; assessment of the radiographs with magnification is regularly required, along with comparison against the adjacent side.
Fig. 2.
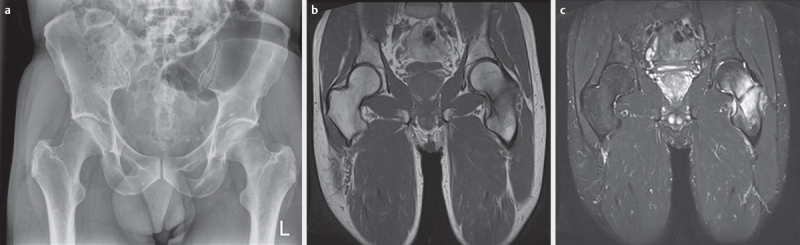
A complete compression femoral neck stress fracture: a radiograph; b t1 sequence mri; c stir sequence MRI.
However, as many as 2 thirds of FNSF patients show no changes on radiographs on presentation 10 53 56 . Typically, around 6 to 8 weeks is required before stress-related changes are visible on radiographs; however, around half of all FNSF patients will never have radiographic evidence of osseous change 10 53 56 . With negative radiographs, and history and examination findings in keeping with a suspected femoral neck stress fracture, further imaging is required 10 56 .
Magnetic resonance imaging
Magnetic resonance imaging (MRI) has now become the gold-standard second-line imaging investigation for FNSFs 10 53 54 56 . A scan should be ordered for all athletes with a suspected FNSF and whose X-rays are negative 10 53 54 56 . An MRI has been shown to have 100% sensitivity, specificity and accuracy when investigating for FNSFs, offering an unrivalled ability to specify differential diagnoses if present 54 .
The standard features of FNSFs found on MRI scanning include: a diffuse, ill-defined, rounded hypo-intense area on T1-weighted images with an equivalent hyper-intense signal on both fat-suppressed T2-weighted images and short-tau inversion-recovery (STIR) sequencing ( Fig. 2 ) 10 53 56 . With worsening severity of the stress injury, these signals are found to span an increasing width of the femoral neck 10 53 56 . When present, a fracture line is seen as a linear area of hypo-intense signal, extending at right angles from the affected cortex, and visible on all sequences of the MR scan 10 53 56 . These findings on MRI images are usually present several weeks before the appearance of radiographic changes 10 53 56 .
Specific benefits of MRI scanning for FNSF investigation include the fact that it is minimally invasive, involves no exposure to ionizing radiation, is cost-effective, and can provide accurate diagnostic information about the surrounding anatomy 10 32 53 56 .
Bone scan
Isotopic bone scanning has now been largely superseded by MRI scanning for the assessment of FNSFs 10 19 53 56 . Previously, it was the gold-standard second-line investigation for evaluating FNSFs, with sensitivity rates ranging from 93% to 100% and specificity rates ranging from 76% to 95% in assessing stress fractures 10 19 53 56 . However, with false positive rates as high as 32% in assessing patients with suspected FNSFs, as well as a requirement for radiation exposure, bone scans are inferior to MRI for FNSF imaging 54 .
Blood profile
In addition to imaging investigations, all patients should undergo routine comprehensive blood testing including a full blood count, erythrocyte sedimentation rate, C-reactive protein levels, renal and liver profile, serum calcium and albumin, with an additional hormone profile for females 19 26 43 53 .
General assessment
In addition to imaging and blood investigations, a comprehensive assessment of each individual should be performed, recording dietary habits, training profiles, gait biomechanics, baseline fitness levels, suitability of training equipment, and use of associated medications, in order to diagnose and adjust pre-disposing factors for this condition 8 .
Management and Complications
Management
The management of FNSFs is decided upon by the location, extent (complete or >50% femoral neck width; incomplete or <50% femoral neck width) and displacement of the fracture ( Table 1 ) 24 52 53 .
Table 1 The management of femoral neck stress fractures by fracture type.
| Fracture Type | Incomplete (<50% Femoral Neck Width) | Complete (>50% Femoral Neck Width) |
|---|---|---|
| Compression | Conservative – unless significant pain or unable to straight-leg raise | Surgical Fixation (Cannulated Hip Screws or Dynamic Hip Screw) |
| Tension | Surgical Fixation (Dynamic Hip Screw) | Surgical Fixation (Dynamic Hip Screw) |
| Displaced | – | Immediate Reduction and Surgical Fixation (Dynamic Hip Screw±Derotation Screw) |
| Atypical Tension | Conservative | Surgical fixation (Dynamic Hip Screw) |
The preferred surgical techniques for each fracture type have been provided in parentheses in the relevant boxes
FNSFs which can be managed conservatively include incomplete compression and incomplete atypical tension fractures ( Fig. 3 ) 24 52 53 . Those which require surgery include complete compression fractures, complete tension fractures and displaced fractures ( Fig. 3 ) 24 52 53 . There remains debate regarding incomplete tension fractures, with some advocating conservative treatment 3 24 45 , whereas the majority advocate surgical management to avoid potential displacement and the significant complications that can arise 52 53 .
Fig. 3.

A complete compression fracture treated with cannulated hip screws: a pre-operative; b post-operative. a complete tension fracture treated with a dynamic hip screw: c pre-operative; d post-operative. a displaced fracture treated with a dynamic hip screw and de-rotation screw: e pre-operative; f post-operative.
When a diagnosis of a completed FNSF is made, initial bed rest in mandatory prior to surgical intervention, because even with non-weight-bearing, the ipsilateral muscle activation required to stabilise the pelvis can result in fracture displacement 3 24 45 .
Surgical management
Timing of surgery
It is becoming increasing clear that delayed surgery for displaced FNSFs results in higher rates of post-operative AVN and failure of fixation 23 30 37 . In a series of 42 displaced FNSFs, Lee et al. 37 noted that in FNSFs which developed AVN (n=10), the mean delay until surgery was 5.9 days, whereas in those that did not develop AVN (n=32), the mean delay was 1.9 days. Johansson et al. 30 noted an AVN rate of 30% in a cohort of 10 displaced FNSF in athletes who had delayed treatment by a mean of 14 weeks. In contrast, Evans et al. 23 noted a 0% AVN rate in a cohort of 6 displaced FNSFs operated on within 12 h.
Choice of implant
There is limited evidence to guide the choice of implant in FNSFs 37 . The study by Lee et al. 37 noted that in 22 cases of displaced FNSFs, those treated by closed reduction and multiple cannulated screws (MCS) had an AVN rate and subsequent revision rate of 18% (4/22); yet those treated by closed reduction and dynamic hip screw (DHS) also had an AVN rate and subsequent revision rate of 18% (3/17) 37 .
Compression FNSFs display a more oblique fracture pattern which, biomechanically, is more stable, and thus can be safely fixed with MCS 24 50 . Tension-type FNSFs, however, are more vertical in nature and prove to be more unstable following fixation; a DHS is recommended for these fracture types because it provides more robust fixation 21 24 50 . With displaced FNSFs, a DHS with a de-rotation screw is recommended, because it provides the stablest construct and reduces the risk of rotating the femoral head during screw insertion, thus limiting damage to the femoral head blood supply 21 24 37 50 .
Reduction alignment
The evidence from Lee et al. 37 has shown that there is a high failure rate with displaced FNSFs that are fixed in varus alignment, compared to those that are fixed in valgus or neutral alignment. In their series, 71% (5/7) of the cases with post-operative varus alignment developed AVN compared to 14% (5/35) of the cases with post-operative valgus or neutral alignment 37 .
Rehabilitation
Post-operatively, the patient should remain non- to toe-touch weight-bearing with crutches for 6 weeks, followed by partial weight-bearing with crutches for a further 6 weeks 20 24 26 51 . After this, weight-bearing is permitted as tolerated 20 24 26 51
Upper limb conditioning can commence immediately post-operatively 15 . Hydrotherapy can then begin 2 weeks post-surgery, wearing an inflatable jacket for support 51 . Lower-limb athletic activity should be commenced only when there is clear evidence of fracture union, both radiologically and clinically 31 . Activity is normally commenced in a graduated manner, around 12 weeks post-surgery, with input from the physiotherapists, specifically focussing on strengthening and range-of-motion exercises around the hip 20 24 49 51 . Patient should begin with a gentle running programme, which should be increased in intensity over 6 to 8 weeks, ensuring the patient remains pain-free throughout 20 24 49 51 . Return to full sport can normally be achieved between 3 and 6 months post-surgery, though this can require up to a year if not longer 20 24 31 46 .
In all cases, dedicated regular follow-up is required with sequential radiographs to assess that the fracture unites and that the fixation does not lose reduction and displace 20 24 31 46 . If this is occurs, non-weight-bearing should be resumed immediately and revision surgery considered if required 24 31 46 . Clinical and radiographic follow-up should be maintained for a minimum of 2 years to ensure delayed post-treatment AVN does not ensue 24 31 46 .
Conservative management
Rehabilitation
If conservative management is chosen, then the patient should be limited weight-bearing with crutches until they are completely free of pain 5 24 45 49 . This normally takes between 6 to 8 weeks but can be up to 14 weeks 5 24 45 49 . During this time, weight-bearing through the injured side can be gradually increased from non-weight-bearing to toe-touch weight bearing to partial weight-bearing, as pain allows 5 24 45 49 .
Rehabilitation should be similar to that described for post-operative care 24 31 45 49 . Lower-limb athletic activity should be commenced only when there is clear evidence of fracture union, both radiologically and clinically 31 49 . The patient should be pain-free with full activity before returning to full level sport 24 31 45 49 . This can normally be resumed around 12 weeks post-injury, but can take up to 28 weeks 24 31 45 49 .
In all cases, dedicated regular follow-up with serial radiographs is required to assess that FNSFs do not propagate and displace 24 31 45 49 . As a guide, radiographs should be performed weekly for the first 4 weeks, every 2 weeks for the next 4 weeks and then every 4 weeks for the next 8 weeks 24 31 45 49 . If fracture propagation or displacement occurs, non-weight-bearing should be resumed immediately and surgical fixation performed 24 31 45 49 .
Note if patients treated conservatively for incomplete compression fractures complain of significant pain or are unable to straight-leg raise, then they should be considered for surgical fixation 52 .
Complications
The incidence of complications following FNSFs largely depends on the nature of the fracture, particularly whether the fracture is displaced or undisplaced 19 53 .
Multiple series of undisplaced conservatively managed FNSFs with prolonged follow-up reported no significant complications beyond refracture 24 30 45 49 . As an exception, however, Blickenstaff & Morris 12 reported that half of their undisplaced tension fractures healed in varus malunion and advised early surgical intervention for this injury type.
Displaced FNSFs, however, with their required surgical management, often develop significant complications 19 53 . These commonly include AVN (24–42%) 30 37 44 60 , non-union (16–44%) 12 44 60 , delayed union (8–50%) 23 37 44 60 , malunion (5–33%) 12 44 , failure of fixation (14%) 37 , revisional surgery (21–50%) 30 37 44 60 and long-term OA (68%) 44 . Such complications can, however, be limited by rapid intervention; surgery within 12 h post-injury has been shown to offer an AVN rate of 0% and a revisonal surgery rate of 0% 23 .
Return to Sport and Injury Prevention
Return to sport
The return-to-sport data in the current literature for athletes with FNSFs is limited, with only 2 studies and one systematic review providing comprehensive information on return to sport for these injuries ( Table 2 ) 30 49 . The remaining literature is restricted to case reports and case series ( Table 3 ) 5 6 7 11 13 15 16 18 20 26 27 28 32 33 36 38 41 43 46 51 55 57 58 59 61 62 63 .
Table 2 Study data and systematic review data on return to sport following femoral neck stress fractures.
| Study | n | Return-to-Sport Rates | Sub-Cohorts | Return-to-Sport Times | Sub-Cohorts |
|---|---|---|---|---|---|
| Johansson et al. (1990) | 23 | 12/23 (52%) | Blickenstaff & Morris Type 1: 6/9 (69%) | – | – |
| Blickenstaff & Morris Type 2: 2/4 (50%) | |||||
| Blickenstaff & Morris Type 3: 4/10 (40%) | |||||
| Ramey et al. (2016) | 27 | 27/27 (100%) | Arendt Grade 1: 5/5 (100%) | 14.1 weeks | Arendt Grade 1: 7.4 weeks |
| Arendt Grade 2: 5/5 (100%) | Arendt Grade 2: 13.8 weeks | ||||
| Arendt Grade 3: 8/8 (100%) | Arendt Grade 3: 14.7 weeks | ||||
| Arendt Grade 4: 9/9 (100%) | Arendt Grade 4: 17.5 weeks | ||||
| Neubauer et al. (2016) | 48 | 28/42 (67%) | Low-Performance Runner 23/32 (72%) | – | – |
| High-Performance Runner 5/16 (31%) | |||||
| Displaced Fractures 6/18 (33%) | |||||
| Non-Displaced Fractures 22/30 (73%) |
Table 3 Case report data on return to sport following femoral neck stress fractures.
| Author | n | Sport | Gender | Age (yr) | Fracture Type | Treatment | Return Time | Return Rate | Return Rate to Same Level |
|---|---|---|---|---|---|---|---|---|---|
| Diwanji et al. (2007) | 2 | Jogging (1) Walking (1) | 2F | 32 (29–35) | Displaced | Surgery: 2 (Blade Plate with VSTO) | n/a | 2/2 (100%) | 2/2 (100%) |
| Hajek & Noble (1982) | 2 | Distance Running (2) | 1M:1F | 32 | Incomplete Compression | Conservative: 2 | 14 weeks | 2/2 (100%) | 2/2 (100%) |
| Lombardo & Benson (1982) | 2 | Marathon Running (1) | 1F | 40 | Displaced | Surgery: 1 (DHS) | 11 months | 1/1 (100%) | 1/1 (100%) |
| Distance Running (1) | 1F | 24 | Incomplete Compression | Conservative: 1 | 18 months | 1/1 (100%) | 1/1 (100%) | ||
| Polacek & Smabrekke (2010) | 2 | Distance Running (2) | 1M: 1F | 38.5 (38–39) | Displaced | Surgery: 2 (DHS 1, MCS 1) | n/a | 2/2(100%) | n/a |
| St Pierre et al. (1995) | 2 | Distance Running (1) | 1M | 15 | Displaced | Surgery: 1 (DHS) | 12 months | 1/1 (100%) | 1/1 (100%) |
| Distance Running (1) | 1M | 16 | Incomplete Compression | Conservative: 1 | n/a | 0/1 (0%) | 0/1 (0%) | ||
| Avrahami & Pajaczkowski (2012) | 1 | Cross-Country Skiing/MTB (1) | 1F | 41 | Incomplete Compression | Conservative: 1 | 3 months | 1/1 (100%) | 1/1 (100%) |
| Baer & Shakespeare (1984) | 1 | Marathon Running (1) | 1M | 36 | Complete Tension | Surgery: 1 (DHS) | n/a | n/a | n/a |
| Bailie & Lamrecht (2001) | 1 | Distance Running (1) | 1M | 15 | Incomplete Compression | Conservative: 1 | n/a | 1/1(100%) | 1/1 (100%) |
| Berg (1991) | 1 | Distance Running (1) | 1M | 22 | Incomplete Compression | Conservative: 1 | 3 months | 1/1 (100%) | 1/1 (100%) |
| Breugem et al. (2009) | 1 | Distance Running (1) | 1F | 30 | Complete Tension | Surgery: 1 (DHS) | 12 months | 1/1 (100%) | 1/1 (100%) |
| Cichy et al. (2012) | 1 | Marathon Running (1) | 1M | 23 | Displaced | Surgery: 1 (DHS) | n/a | 1/1 (100%) | n/a |
| Clough(2002) | 1 | Marathon Running (1) | 1M | 55 | Displaced | Surgery: 1 (DHS) | n/a | n/a | n/a |
| Ejnisman et al. (2013) | 1 | Jogging (1) | 1F | 56 | Displaced | Surgery: 1 (MCS) | 6 months | 1/1 (100%) | 1/1 (100%) |
| Goolsky et al. (2012) | 1 | Distance Running (1) | 1F | 15 | Displaced | Surgery: 1 (MCS) | n/a | n/a | n/a |
| Haddad et al. (1997) | 1 | Distance Running (1) | 1F | 15 | Displaced | Surgery: 1 (DHS requiring revision to MCS) | n/a | n/a | n/a |
| Kerr & Johns (1995) | 1 | Marathon Running (1) | 1M | 32 | Displaced | Surgery: 1 (DHS) | 8 months | 1/1 (100%) | n/a |
| Krause & Newcomer (2008) | 1 | Marathon Running (1) | 1M | 37 | Incomplete Compression | Conservative: 1 | n/a | n/a | n/a |
| Kupke et al. (1993) | 1 | Distance Running (1) | 1F | 27 | Incomplete Compression | Conservative: 1 | n/a | 1/1 (100%) | n/a |
| O’Brien et al. (2011) | 1 | Distance Running (1) | 1F | 31 | Complete Compression | Surgery: 1 (MCS) | n/a | n/a | n/a |
| Okamoto et al. (2010) | 1 | Distance Running (1) | 1F | 17 | Displaced | Surgery: 1 (MCS) | n/a | 1/1 (100%) | 1/1 (100%) |
| Scott et al. (1999) | 1 | Marathon Running (1) | 1M | 50 | Displaced | Surgery: 1 (MCS) | 12 weeks | 1/1 (100%) | n/a |
| Skinner & Cook (1982) | 1 | Distance Running (1) | 1F | 31 | Displaced | Surgery: 1 (MCS) | n/a | n/a | n/a |
| Sterling et al. (1993) | 1 | Marathon Running (1) | 1F | 42 | Incomplete Tension | Surgery: 1 (MCS) | 3 months | 1/1 (100%) | 1/1 (100%) |
| Taylor-Haas et al. (2011) | 1 | Marathon Running (1) | 1M | 34 | Incomplete Compression | Conservative: 1 | n/a | 0/1 (0%) | 0/1 (0%) |
| Voss et al. (1997) | 1 | Marathon Running (1) | 1F | 30 | Incomplete Tension | Surgery: 1 | n/a | 1/1 (100%) | n/a |
| Wen et al. (2003) | 1 | Distance Running (1) | 1M | 44 | Incomplete Compression | Conservative: 1 | 3 months | 1/1 (100%) | 1/1 (100%) |
| Zacharias & Marsh (1980) | 1 | Distance Running (1) | 1M | 17 | Incomplete Compression | Conservative: 1 | n/a | 1/1 (100%) | n/a |
Treatment Method in Brackets. DHS – Dynamic Hip Screw. MCS – Multiple Cannulated Hip Screws. ABP – Angled Blade Plate. VSTO – Valgus Sub-Trochanteric Osteotomy
Until recently, the only comprehensive study to assess the sporting outcome in athletes with FNSFs was that by Johansson et al. 30 . They reported a series of 7 elite and 16 recreational Swedish athletes with FNSFs sustained from a variety of sports 30 . 16 underwent surgical fixation with 7 treated conservatively 30 .
From the whole cohort, 12 (52%) returned to same level of sporting activity post-treatment; however all elite athletes had to end their career secondary to their injury 30 . Those with displaced fractures had significantly worse return rates to sport (40%) than those with non-displaced fractures (62%).
More recently, Ramey et al. 49 published a study assessing the ‘return to running time’ for 27 conservatively managed compression FNSFs in 24 runners (3 recurrent fractures in a single patient). Grading the FNSFs by the Arendt scale 2 , the mean time to return to running was 14.1 weeks; increased severity per the Arendt scale was associated with an increased return to running time 49 .
In 2016, Neubauer et al. 39 published a systematic review recording all reported cases of running athletes who sustained an FNSF. From a cohort of 48 athletes, 28 were noted to return to running 39 . Fracture displacement (p=0.014) and high performance running status (p=0.012) were found to negatively influence the return to running ( Table 2 ) 39 .
From the cohort of case reports, a total of 32 athletes were recorded (17 female:15 male) ( Table 3 ) 5 6 7 11 13 15 16 18 20 26 27 28 32 33 36 38 41 43 46 51 55 57 58 59 61 62 63 . The causative sports were long-distance running in 18 cases, marathon running in 10, jogging in 2, walking in one and skiing in one 5 6 7 11 13 15 16 18 20 26 27 28 32 33 36 38 41 43 46 51 55 57 58 59 61 62 63 . There were 12 conservatively managed compression fractures, 15 surgically managed displaced fractures and 5 surgically managed undisplaced fractures 5 6 7 11 13 15 16 18 20 26 27 28 32 33 36 38 41 43 46 51 55 57 58 59 61 62 63 . For the conservatively managed compression FNSFs, the combined return rate was 9/11; the return times ranged from 3 to 18 months 5 7 11 28 33 36 38 57 59 62 63 . For the surgically managed displaced FNSFs, the combined return rate was 11/11; the return times ranged from 3 to 12 months 15 16 18 20 26 27 32 38 43 46 51 55 57 . For the surgically managed nondisplaced fractures, the combined return rate was 3/3; the return times ranged from 3 months to 12 months 6 13 41 58 61 .
Injury prevention
Treatment protocols introduced by the Finnish and US military, which advocated prompt imaging of all symptomatic servicemen, along with educational programmes for the healthcare providers, have been found to reduce rates of displaced FNSFs by over 50% 35 44 45 53 . Similar guidance should be provided for healthcare professionals managing athletic populations 35 44 45 53 .
Regarding exercise training modifications to avoid FNSFs, current recommendations advise that athletes should limit training volume increases to 10%, and that, for beginners, total training volume should not exceed 160 km over a 12 week period 39 .
Conclusion ( Table 4 )
Table 4 Summary table.
| Key Findings | |
|---|---|
| Epidemiology |
|
| Pathophysiology |
|
| Biomechanics |
|
| Presentation |
|
| Examination |
|
| Investigation |
|
| Management |
|
| Sport Outcome |
|
| Injury Prevention |
|
FNW – Femoral Neck Width
From this review article, it has been established that FNSFs comprise 3% of all sport-related stress fractures. The main causative sports are long-distance and marathon running. Female gender and poor baseline physical fitness are the key risk factors for these injuries. Compression FNSFs develop secondary to exercise-related fatigue loading of the femoral neck; tensions FNSFs develop both through this and through fatigue of the hip abductor muscles. The commonest presenting symptom is exercise-related anterior groin pain; the commonest exam finding is pain at the extremes of hip range of motion. Radiographs form the first line of imaging: MRI scans are now the gold-standard second-line imaging investigation. The management of FNSFs remains guided by the location and displacement of the fracture: conservative management is reserved for incomplete compression FNSFs; surgical management is required for complete compression FNSFs and tension FNSFs. Displaced FNSFs should be treated by urgent reduction and surgical fixation. Sporting outcomes are favourable for incomplete compression fractures, with return rates as high as 100%: however they are considerably worse for displaced fractures, with return rates as low as 33%. Education programmes and treatment algorithms can reduce the incidence of displaced FNSFs in the athlete.
Footnotes
Conflict of Interest The authors declare that they have no conflict of interest.
References
- 1.Adkins S B, 3 rd, Figler R A. Hip pain in athletes. Am Fam Physician. 2000;61:2109–2118. [PubMed] [Google Scholar]
- 2.Arendt E A, Griffiths H J. The use of MR imaging in the assessment and clinical management of stress reactions of bone in high-performance athletes. Clin Sports Med. 1997;16:291–306. doi: 10.1016/s0278-5919(05)70023-5. [DOI] [PubMed] [Google Scholar]
- 3.Aro H, Dahlstrom S. Conservative management of distraction-type stress fractures of the femoral neck. J Bone Joint Surg Br. 1986;68:65–67. doi: 10.1302/0301-620X.68B1.3941143. [DOI] [PubMed] [Google Scholar]
- 4.Asal D. Uberlastungsschaden am Knochensystem bei Soldaten. Arch für Klinische Chirurgie. 1936;186:511–522. [Google Scholar]
- 5.Avrahami D, Pajaczkowski J A. Femoral neck stress fracture in a female athlete: a case report. J Chiropr Med. 2012;11:273–279. doi: 10.1016/j.jcm.2012.05.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Baer S, Shakespeare D. Stress fracture of the femoral neck in a marathon runner. Br J Sports Med. 1984;18:42–43. doi: 10.1136/bjsm.18.1.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bailie D S, Lamprecht D E. Bilateral femoral neck stress fractures in an adolescent male runner. A case report. Am J Sports Med. 2001;29:811–813. doi: 10.1177/03635465010290062301. [DOI] [PubMed] [Google Scholar]
- 8.Behrens S B, Deren M E, Matson A, Fadale P D, Monchik K O. Stress fractures of the pelvis and legs in athletes: a review. Sports Health. 2013;5:165–174. doi: 10.1177/1941738112467423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Belcher A. Ueber den Einfluss des Parademarches auf dieEntstehung der Fussgeschwulst. Med Klin. 1905;1:305–306. [Google Scholar]
- 10.Bencardino J T, Palmer W E.Imaging of hip disorders in athletes Radiol Clin North Am 200240267–287.vi–vii [DOI] [PubMed] [Google Scholar]
- 11.Berg E E. Femoral neck stress fracture. Orthop Nurs. 1991;10:53–55. [PubMed] [Google Scholar]
- 12.Blickenstaff L D, Morris J M. Fatigue fracture of the femoral neck. J Bone Joint Surg Am. 1966;48:1031–1047. [PubMed] [Google Scholar]
- 13.Breugem S J, Hulscher J B, Steller P. Stress fracture of the femoral neck in a young female athlete. Eur J Trauma Emerg Surg. 2009;35:192. doi: 10.1007/s00068-008-8034-8. [DOI] [PubMed] [Google Scholar]
- 14.Carpintero P, Leon F, Zafra M, Serrano-Trenas J A, Roman M. Stress fractures of the femoral neck and coxa vara. Arch Orthop Trauma Surg. 2003;123:273–277. doi: 10.1007/s00402-003-0514-z. [DOI] [PubMed] [Google Scholar]
- 15.Cichy B, Roche S J, Wozniak A. Atypical femoral neck stress fracture in a marathon runner: a case report and literature review. Ir J Med Sci. 2012;181:427–429. doi: 10.1007/s11845-010-0599-7. [DOI] [PubMed] [Google Scholar]
- 16.Clough T M. Femoral neck stress fracture: the importance of clinical suspicion and early review. Br J Sports Med. 2002;36:308–309. doi: 10.1136/bjsm.36.4.308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Devas M B. Stress fractures of the femoral neck. J Bone Joint Surg Br. 1965;47:728–738. [PubMed] [Google Scholar]
- 18.Diwanji S R, Kong I K, Cho S G, Seon J K, Yoon T R. Displaced stress fracture of the femoral neck treated by valgus subtrochanteric osteotomy: 2 case studies. Am J Sports Med. 2007;35:1567–1570. doi: 10.1177/0363546507299241. [DOI] [PubMed] [Google Scholar]
- 19.Egol K A, Koval K J, Kummer F, Frankel V H.Stress fractures of the femoral neck Clin Orthop Relat Res 1998. doi:http://www.ncbi.nlm.nih.gov/pubmed/955353672–78. [PubMed] [Google Scholar]
- 20.Ejnisman L, Wajnsztejn A, Queiroz R D, Ejnisman B. Unusual presentation of a femoral stress fracture. BMJ Case Rep. 2013 doi: 10.1136/bcr-2012-007828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Enocson A, Lapidus L J. The vertical hip fracture – a treatment challenge. A cohort study with an up to 9 year follow-up of 137 consecutive hips treated with sliding hip screw and antirotation screw. BMC Musculoskelet Disord. 2012;13:171. doi: 10.1186/1471-2474-13-171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ernst J. Stress fracture of the neck of the femur. J Trauma. 1964;4:71–83. doi: 10.1097/00005373-196401000-00005. [DOI] [PubMed] [Google Scholar]
- 23.Evans J T, Guyver P M, Kassam A M, Hubble M J. Displaced femoral neck stress fractures in Royal Marine recruits – management and results of operative treatment. J R Nav Med Serv. 2012;98:3–5. [PubMed] [Google Scholar]
- 24.Fullerton L R, Jr., Snowdy H A. Femoral neck stress fractures. Am J Sports Med. 1988;16:365–377. doi: 10.1177/036354658801600411. [DOI] [PubMed] [Google Scholar]
- 25.Goldin M, Anderson C N, Fredericson M, Safran M R, Stevens K J. Femoral neck atress fractures and imaging features of femoroacetabular impingement. PM R. 2015;7:584–592. doi: 10.1016/j.pmrj.2014.12.008. [DOI] [PubMed] [Google Scholar]
- 26.Goolsby M A, Barrack M T, Nattiv A. A displaced femoral neck stress fracture in an amenorrheic adolescent female runner. Sports Health. 2012;4:352–356. doi: 10.1177/1941738111429929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Haddad F S, Bann S, Hill R A, Jones D H. Displaced stress fracture of the femoral neck in an active amenorrhoeic adolescent. Br J Sports Med. 1997;31:70–72. doi: 10.1136/bjsm.31.1.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hajek M R, Noble H B. Stress fractures of the femoral neck in joggers: case reports and review of the literature. Am J Sports Med. 1982;10:112–116. doi: 10.1177/036354658201000210. [DOI] [PubMed] [Google Scholar]
- 29.Hulkko A, Orava S. Stress fractures in athletes. Int J Sports Med. 1987;8:221–226. doi: 10.1055/s-2008-1025659. [DOI] [PubMed] [Google Scholar]
- 30.Johansson C, Ekenman I, Tornkvist H, Eriksson E. Stress fractures of the femoral neck in athletes. The consequence of a delay in diagnosis. Am J Sports Med. 1990;18:524–528. doi: 10.1177/036354659001800514. [DOI] [PubMed] [Google Scholar]
- 31.Kaeding C C, Yu J R, Wright R, Amendola A, Spindler K P. Management and return to play of stress fractures. Clin J Sport Med. 2005;15:442–447. doi: 10.1097/01.jsm.0000188207.62608.35. [DOI] [PubMed] [Google Scholar]
- 32.Kerr P S, Johnson D P. Displaced femoral neck stress fracture in a marathon runner. Injury. 1995;26:491–493. doi: 10.1016/0020-1383(95)00063-f. [DOI] [PubMed] [Google Scholar]
- 33.Krause D A, Newcomer K L. Femoral neck stress fracture in a male runner. J Orthop Sports Phys Ther. 2008;38:517. doi: 10.2519/jospt.2008.0408. [DOI] [PubMed] [Google Scholar]
- 34.Kuhn K M, Riccio A I, Saldua N S, Cassidy J. Acetabular retroversion in military recruits with femoral neck stress fractures. Clin Orthop Relat Res. 2010;468:846–851. doi: 10.1007/s11999-009-0969-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kupferer K R, Bush D M, Cornell J E, Lawrence V A, Alexander J L, Ramos R G, Curtis D. Femoral neck stress fracture in Air Force basic trainees. Mil Med. 2014;179:56–61. doi: 10.7205/MILMED-D-13-00154. [DOI] [PubMed] [Google Scholar]
- 36.Kupke M J, Kahler D M, Lorenzoni M H, Edlich R F. Stress fracture of the femoral neck in a long distance runner: biomechanical aspects. J Emerg Med. 1993;11:587–591. doi: 10.1016/0736-4679(93)90314-w. [DOI] [PubMed] [Google Scholar]
- 37.Lee C H, Huang G S, Chao K H, Jean J L, Wu S S. Surgical treatment of displaced stress fractures of the femoral neck in military recruits: a report of 42 cases. Arch Orthop Trauma Surg. 2003;123:527–533. doi: 10.1007/s00402-003-0579-8. [DOI] [PubMed] [Google Scholar]
- 38.Lombardo S J, Benson D W. Stress fractures of the femur in runners. Am J Sports Med. 1982;10:219–227. doi: 10.1177/036354658201000406. [DOI] [PubMed] [Google Scholar]
- 39.Neubauer T, Brand J, Lidder S, Krawany M.Stress fractures of the femoral neck in runners: a review. Res Sports Med 2016. doi:10.1080/15438627.2016.11914891–15. [DOI] [PubMed] [Google Scholar]
- 40.Niva M H, Kiuru M J, Haataja R, Pihlajamaki H K. Fatigue injuries of the femur. J Bone Joint Surg Br. 2005;87:1385–1390. doi: 10.1302/0301-620X.87B10.16666. [DOI] [PubMed] [Google Scholar]
- 41.O’Brien J, Taunton J, Larsen J, Forster B B. 31-year-old female runner with 5-week history of hip pain. Br J Sports Med. 2011;45:136–139. doi: 10.1136/bjsm.2009.069559. [DOI] [PubMed] [Google Scholar]
- 42.O’Kane J W. Anterior hip pain. Am Fam Physician. 1999;60:1687–1696. [PubMed] [Google Scholar]
- 43.Okamoto S, Arai Y, Hara K, Tsuzihara T, Kubo T. A displaced stress fracture of the femoral neck in an adolescent female distance runner with female athlete triad: a case report. Sports Med Arthrosc Rehabil Ther Technol. 2010;2:6. doi: 10.1186/1758-2555-2-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Pihlajamaki H K, Ruohola J P, Kiuru M J, Visuri T I. Displaced femoral neck fatigue fractures in military recruits. J Bone Joint Surg Am. 2006;88:1989–1997. doi: 10.2106/JBJS.E.00505. [DOI] [PubMed] [Google Scholar]
- 45.Pihlajamaki H K, Ruohola J P, Weckstrom M, Kiuru M J, Visuri T I. Long-term outcome of undisplaced fatigue fractures of the femoral neck in young male adults. J Bone Joint Surg Br. 2006;88:1574–1579. doi: 10.1302/0301-620X.88B12.17996. [DOI] [PubMed] [Google Scholar]
- 46.Polacek M, Smabrekke A. Displaced stress fracture of the femoral neck in young active adults. BMJ Case Rep 2010; 2010: [DOI] [PMC free article] [PubMed]
- 47.Pouilles J M, Bernard J, Tremollieres F, Louvet J P, Ribot C. Femoral bone density in young male adults with stress fractures. Bone. 1989;10:105–108. doi: 10.1016/8756-3282(89)90006-9. [DOI] [PubMed] [Google Scholar]
- 48.Provencher M T, Baldwin A J, Gorman J D, Gould M T, Shin A Y. Atypical tensile-sided femoral neck stress fractures: the value of magnetic resonance imaging. Am J Sports Med. 2004;32:1528–1534. doi: 10.1177/0363546503262195. [DOI] [PubMed] [Google Scholar]
- 49.Ramey L N, McInnis K C, Palmer W E. Femoral neck stress fracture: can MRI grade help predict return-to-running time? Am J Sports Med. 2016 doi: 10.1177/0363546516648319. [DOI] [PubMed] [Google Scholar]
- 50.Rockwood CA G D, Jr, Bucholz R W, Heckman J D.eds.Rockwood and Green’s Fractures in Adults Philadelphia: Lippincott-Raven; 1996 [Google Scholar]
- 51.Scott M P, Finnoff J T, Davis B A. Femoral neck stress fracture presenting as gluteal pain in a marathon runner: case report. Arch Phys Med Rehabil. 1999;80:236–238. doi: 10.1016/s0003-9993(99)90127-2. [DOI] [PubMed] [Google Scholar]
- 52.Scott S J, Feltwell D N, Knapik J J, Barkley C B, Hauret K G, Bullock S H, Evans R K. A multiple intervention strategy for reducing femoral neck stress injuries and other serious overuse injuries in U.S. Army Basic Combat Training. Mil Med. 2012;177:1081–1089. doi: 10.7205/milmed-d-12-00085. [DOI] [PubMed] [Google Scholar]
- 53.Shin A Y, Gillingham B L. Fatigue fractures of the femoral neck in athletes. J Am Acad Orthop Surg. 1997;5:293–302. doi: 10.5435/00124635-199711000-00001. [DOI] [PubMed] [Google Scholar]
- 54.Shin A Y, Morin W D, Gorman J D, Jones S B, Lapinsky A S. The superiority of magnetic resonance imaging in differentiating the cause of hip pain in endurance athletes. Am J Sports Med. 1996;24:168–176. doi: 10.1177/036354659602400209. [DOI] [PubMed] [Google Scholar]
- 55.Skinner H B, Cook S D. Fatigue failure stress of the femoral neck. A case report. Am J Sports Med. 1982;10:245–247. doi: 10.1177/036354658201000411. [DOI] [PubMed] [Google Scholar]
- 56.Spitz D J, Newberg A H. Imaging of stress fractures in the athlete. Radiol Clin North Am. 2002;40:313–331. doi: 10.1016/s0033-8389(02)00010-6. [DOI] [PubMed] [Google Scholar]
- 57.St Pierre P, Staheli L T, Smith J B, Green N E. Femoral neck stress fractures in children and adolescents. J Pediatr Orthop. 1995;15:470–473. doi: 10.1097/01241398-199507000-00012. [DOI] [PubMed] [Google Scholar]
- 58.Sterling J C, Webb R F, Jr., Meyers M C, Calvo R D. False negative bone scan in a female runner. Med Sci Sports Exerc. 1993;25:179–185. [PubMed] [Google Scholar]
- 59.Taylor-Haas J A, Paterno M V, Shaffer M D. Femoral neck stress fracture and femoroacetabular impingement. J Orthop Sports Phys Ther. 2011;41:905. doi: 10.2519/jospt.2011.0423. [DOI] [PubMed] [Google Scholar]
- 60.Visuri T, Vara A, Meurman K O. Displaced stress fractures of the femoral neck in young male adults: a report of twelve operative cases. J Trauma. 1988;28:1562–1569. doi: 10.1097/00005373-198811000-00007. [DOI] [PubMed] [Google Scholar]
- 61.Voss L, DaSilva M, Trafton P G. Bilateral femoral neck stress fractures in an amenorrheic athlete. Am J Orthop (Belle Mead NJ) 1997;26:789–792. [PubMed] [Google Scholar]
- 62.Wen D Y, Propeck T, Singh A. Femoral neck stress injury with negative bone scan. J Am Board Fam Pract. 2003;16:170–174. doi: 10.3122/jabfm.16.2.170. [DOI] [PubMed] [Google Scholar]
- 63.Zacharias C K, Marsh H O. Jogging! a non-traumatic exercise? J Kans Med Soc. 1980;81:563–565. [PubMed] [Google Scholar]