

Abstract
We present a 26-year-old male patient who presented with complete bowel obstruction and peritonitis. His abdominal X-rays showed grossly distended large bowels with air–fluid levels. A differential diagnosis of sigmoid volvulus was entertained and the patient was taken for an exploratory laparotomy. Intraoperatively, we found a sigmoid volvulus and a concurrent transverse colon volvulus. A subtotal colectomy and colostomy was performed. The histopathology results showed mucosal and submucosal congestion, chronic inflammation, and no malignancy or dysplasia. Synchronous volvulus of the sigmoid and transverse colon is an extremely rare. Management includes endoscopic derotation and decompression followed by semi-elective surgery in non-complicated cases. When endoscopic decompression has failed or there is suspicion of necrosis or perforation, surgery is mandatory.
INTRODUCTION
Volvulus is rotation or twisting of the intestine around their vascular pedicle. The occurrence of concurrent sigmoid and transverse colon volvulus is extremely rare. There is paucity of information in the literature regarding synchronous sigmoid and transverse colon volvulus.
CASE PRESENTATION
We present a 26-year-old male patient who presented at our accident and emergency department with complete bowel obstruction of 3 days’ duration. He presented with grossly distended abdomen, abdominal pains, vomiting and passing no flatus. The patient had no background history of chronic illnesses nor previous operations. On examination he was tachypnoic (24 bpm), his temperature was 38.5, heart rate was 68 and was peritonitic with a tense distended abdomen. Digital rectal examination revealed an empty rectum. His blood results revealed a potassium of 2.8 but the rest of his electrolytes and full blood count were normal. The erect chest and abdominal X-rays showed no air under the diaphragm and grossly distended large bowels with air–fluid levels (Fig. 1). A differential diagnosis of sigmoid volvulus was entertained after reviewing the X-rays. In view of peritonitis endoscopy was omitted and the patient was taken for an exploratory laparotomy after resuscitation. Intraoperative findings were a sigmoid volvulus and to our surprise a concurrent transverse colon volvulus with a non-distended cecum and collapsed small bowels. The sigmoid and transverse colon were redundant and their mesocolon had narrow parietal attachments. The involved segments were grossly distended and slightly dusky but pinked up after derotation (Figs 2 and 3). A subtotal colectomy and colostomy was performed and the surgical specimen sent for histopathology. The patient was discharged on the fifth day post operation and his recovery was uneventful. The histopathology results showed mucosal and submucosal congestion, chronic inflammation, compatible with volvulus and no malignancy or dysplasia was found. At 6 weeks’ follow-up clinic the patient was informed about the results.
Figure 1:
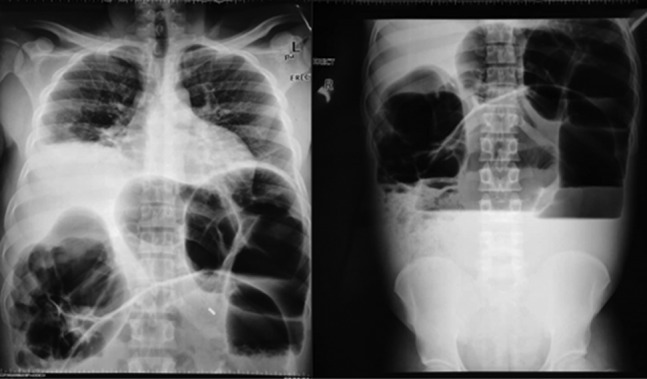
Erect chest and abdominal X-rays showing dilated colon and air–fluid levels.
Figure 2:
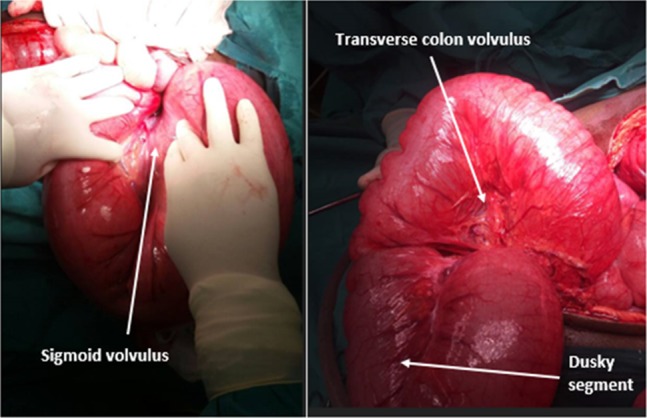
Sigmoid volvulus and transverse colon volvulus.
Figure 3:
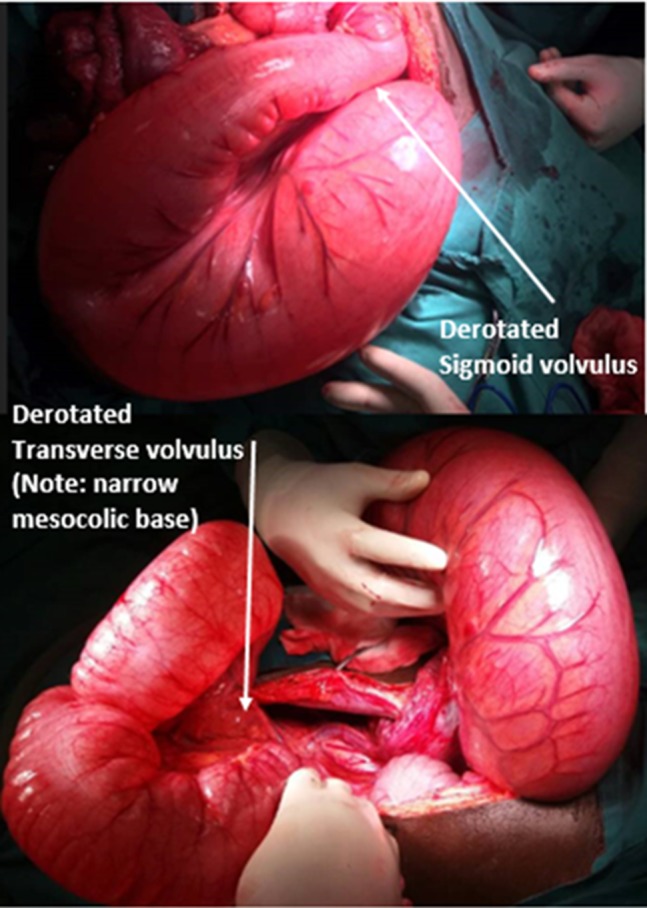
Post-derotation of the sigmoid and transverse volvulus.
DISCUSSION
Synchronous sigmoid and transverse colon volvulus is an extremely rare occurrence [1–4]. Most of the reported cases are elderly patients over the age of 60. Our patient was 26-year-old. Colonic volvulus accounts for 1–7% of cases of large bowel obstruction in Western Europe and USA. This is variable in different regions. Tropical and subtropical areas experience higher rates. The sigmoid colon is involved in 65–80% of the cases reported, followed by right colon in 15–30% of cases while transverse colon and splenic flexure volvulus are rare [4]. Parish et al. [5] described a case of coexistent volvulus of the transverse, sigmoid and right colon. To the author’s knowledge there is a single pediatric case with metachronous sigmoid and transverse colon volvulus that was reported in 2000. This was a case of cerebral palsy who initially presented with transverse colon volvulus and resection and colocolic anastomosis was performed following which he developed a sigmoid volvulus. This was also treated with resection and primary anastomosis [6].
Risk factors of colonic volvulus in adults include acquired redundant sigmoid colon or any segment of the colon, use of psychotropic drugs as seen in patient with mental retardation and neuropsychiatric disorders, narrow base of mesocolic parietal attachment in a redundant colon and chronic institutionalization. Anomalous fixation of the colon is considered the main factor in volvulus development in pediatric population. A clinical condition involving elongation and dilation of the colon known as dolichocolon is also considered a risk factor for volvulus. This condition is most commonly seen in elderly people [6, 7]. Our patient had redundant colon with narrow sigmoid and transverse mesoscopic parietal attachments.
Radiographic findings are diagnostic in 75% of cases in sigmoid volvulus. The following may be seen on plain abdominal films: a vertical dense white line representing apposed inner walls of sigmoid colon pointing toward pelvis, closed loop obstruction, absence of gas in rectum, inverted ‘U’ shape with absent haustra, northern exposure sign (dilated, twisted sigmoid colon projects above transverse colon on supine radiograph), apex above T10 vertebra and under left hemidiaphragm and directed toward right shoulder. Water-soluble contrast enema imaging shows ‘Beaking’ at the point of torsion at rectosigmoid junction and mucosal folds imaging often show corkscrew pattern at the point of torsion. One may also see shouldering caused by localized wall thickening at the site of twist particularly in chronic or recurrent volvulus. Contrast enhanced computer tomography may show ‘Beaking’ caused by progressive tapering of afferent and efferent limbs leading into the twist. The whirl sign may also be present caused by tightly twisted mesentery and bowel near base of volvulus [8, 9].
In the absence of clinical and radiological signs of necrosis or perforation, the initial management of volvulus involves colonoscopic derotation and decompression followed by semi-elective resection and anastomosis after optimizing the patient. This approach increases the chances of having a single stage definitive procedure. However, if there is evidence of necrosis or perforation clinically or radiologically, surgery is mandatory. If endoscopic derotation and decompression fails, the patient should be taken for an operation [10]. Resection of involved segments is mandatory followed by ostomy or primary anastomosis depending on the bowel status and patient stability. A detorsion without resection of the colon is associated with high recurrence rates. In the presence of megacolon, a limited colonic resection leads to recurrence in as high as 82% of the times. The concomitant presence of megacolon and megarectum are reported to be significant predictors of recurrence [10].
CONCLUSION
Synchronous volvulus of the sigmoid and transverse colon is an extremely rare clinical entity. Management includes endoscopic derotation and decompression followed by semi-elective surgery in non-complicated cases. When endoscopic decompression has failed or there is suspicion of necrosis or perforation, surgery is mandatory. Lone derotation is discouraged as it is associated with very high recurrence rates.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
GUARANTOR
Mpapho Joseph Motsumi.
REFERENCES
- 1. Alireza H, Reza ES, Hamed P, Hamidreza J. Synchronic volvulus of sigmoid and transverse colon: a rare case of large bowel obstruction. Ann Colorectal Res 2014;2:e16520. [Google Scholar]
- 2. Lianos G, Ignatiadou E, Lianou E, Anastasiadi Z, Fatouros M. Simultaneous volvulus of the transverse and sigmoid colon: case report. G Chir 2012;33:324–6. [PubMed] [Google Scholar]
- 3. Wisler JR, Stawicki SPA. Interesting clinical image: colonic ¨double twist¨. OPUS 12 Scientist 2009;3:58–9. [Google Scholar]
- 4. Katsanos K, Ignatiadou E, Markouizos G, Doukas M, Siafakas M, Fatouros M, et al. Non-toxic megacolon due to transverse and sigmoid colon volvulus in a patient with ulcerative colitis. J Crohns Colitis 2009;3:38–41. [DOI] [PubMed] [Google Scholar]
- 5. Parrish RA, Crook JA, Moretz WH. Coexistent volvulus of the transverse, sigmoid and right colon. Am Surg 1964;030:313–6. [PubMed] [Google Scholar]
- 6. Samuel M, Boddy SA, Capps S. Volvulus of the transverse and sigmoid colon. Pediatr Surg Int 2000;16:522–4. [DOI] [PubMed] [Google Scholar]
- 7. Islam S, Hosein D, Harnarayan P, Naraynsingh V. Synchronic volvulus of splenic flexure and caecum: a very rare cause of large bowel obstruction. BMJ Case Rep 2016;2016:bcr2015213029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Lin MP, Chen YL, Tzeng WS. Diagnosis of sigmoid volvulus using the coffee bean, northern exposure sign, whirl sign and transition point. BMJ Case Rep 2011;2011:4334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Levsky JM, Den EI, DuBrow RA. CT findings of sigmoid volvulus. AJR Am J Roentgenol 2010;194:136–43. [DOI] [PubMed] [Google Scholar]
- 10. Chung YF, Eu KW, Nyam DC. Minimizing recurrence after sigmoid volvulus. Br J Surg 1999;86:231–3. [DOI] [PubMed] [Google Scholar]