

Abstract
Background:
Heat loss and core-to-peripheral redistribution of body heat occur in patients undergoing neuraxial anesthesia resulted to decrease of core temperature and early reach of shivering threshold. Because shivering has deleterious metabolic and cardiovascular effects, it should ideally be prevented by pharmacologic or other means. Tizanidine is an alpha-2 agonist. We evaluated the usefulness of oral tizanidine (TI) and tramadol in preventing of shivering in patients undergoing spinal anesthesia for transurethral resection of the prostate (TURP).
Materials and Methods:
Ninety patients, scheduled for TURP with spinal anesthesia, were prospectively enrolled. Patients were randomly assigned to 1 of 3 groups. 90 min before spinal anesthesia, 30 patients received 4 mg oral TI, 30 patients received 50 mg tramadol, and 30 patients received placebo as control group. Spinal anesthesia was induced at the L3–L4 or L4–L5 interspaces with 12.5 mg bupivacaine. An investigator blinded to the drugs recorded the frequency and degree of shivering.
Results:
The overall frequency and severity of shivering were significantly lower in patients treated with TI and tramadol compared to placebo (P = 0.04) (P = 0.001). There was not much difference in the nausea and vomiting of both the drugs (P = 026) (P = 011). There was no difference in hemodynamic parameters between three groups (P = 0.08) (P = 013).
Conclusions:
Oral TI and tramadol were comparable in respect to their effect in decreasing the incidence, intensity shivering when used prophylactically in patients who underwent TURP with spinal anesthesia.
Keywords: Shivering, spinal, tizanidine, tramadol
Introduction
Postoperative shivering has been seen in 40% of cases. However, it seems that this incidence has been decreased due to maintenance of normothermia during surgery and the use of opiates.[1] The findings showed that increased body metabolism during shivering can lead to myocardial ischemia.[2] Postoperative shivering can increase intracranial and intraocular pressure and through inducing tenderness lead to postoperative pain.[3]
Shivering incidence during neuraxial block may be reduced by warming the body surface skin.[4] The drugs including Meperidine (25 mg intravenous),[5] Clonidine (75 mg intravenous solution), Ketanserin (10 mg intravenous),[6] Dexmedetomidine[7] and Magnesium sulfate (30 mg intravenous)[8] are effective for tremor after anesthesia and neuraxial block. Opioids such as meperidine have been used to treat and prevent postoperative shivering.[9,10,11,12] However, some side effects such as respiratory depression, low blood pressure, nausea, and vomiting have limited the use of opiates after surgery.[13] Tramadol is associated with lower risk of respiratory disease, drug tolerance and drug dependence for the treatment and prevention of shivering.[14,15,16] Various studies have been conducted on the effects of intravenous tramadol on treatment and prevention of postoperative shivering.[17] Alpha-2 agonists as antihypertensive drugs can improve sleep disorders, anxiety, and pain.[18]
Tizanidine (TI) is an oral alpha-2 agonist and mediates central muscle relaxant activity for the treatment of painful muscle spasms. Moreover, less cardiovascular side effects of TI compared to other medications make it an important and useful alternative in anesthetics.[19]
Patients undergoing transurethral resection of the prostate (TURP) due to other underlying disease such as cardiovascular disease and aging have many problems. Hypothermia in these patients can be associated with complications such as myocardial ischemia.[20] Therefore, the aim of this study was to evaluate the effect of oral TI, tramadol, and placebo on intra- and post-operative shivering in patients undergoing TURP with spinal anesthesia.
Materials and Methods
Study population
This randomized, double-blind clinical trial study was conducted on patients undergoing TURP in Imam Khomeini Hospital. In the current study, the number of patients according to the previous study[21] was considered 90. Moreover, this study was approved by Urmia University of Medical Sciences [Figure 1].
Figure 1.

CONSRT flowchart
Eligibility criteria
Inclusion criteria were patients 40–60 years old with the American Society of Anesthesiologists Classification I and II undergoing TURP and exclusion criteria were obesity, sensitivity to tramadol or TI, ischemic heart disease history, thyroid and cerebrovascular disease, diabetic autonomic neuropathy, contraindication for regional anesthesia, and duration of surgery more than 1.5 h. Moreover, patient taking vascular medications were excluded from the study.
The first patient received tramadol, the second patient TI and the third patient placebo. The first group received 4 mg oral TI, the second group 50 mg tramadol and other group placebo 90 min before surgery. The colleague of the operating room was unaware of the patient classification. Another person analyzed the data based on the collected forms and personal profile data. All patients before surgery were fasting for at least 8 h. Prostatectomy surgery was performed in an operating room with the same temperature and humidity.
In the operating room, pulse oximetry monitoring, noninvasive blood pressure, and electrocardiogram were used for all patients.
In the current study, all patients received injection of 12.5 mg 0.5% hyperbaric bupivacaine through spinal anesthesia in sitting position at the L3–L4 interspaces with a 25 G Quincke bevel needle. The level of spinal anesthesia was achieved to T9–T10. The temperature of fluid bladder washing in all patients was the same (36°C). The incidence of nausea, vomiting and severity of shivering during surgery and recovery were recorded. Heart rate, mean arterial pressure, respiratory rate, arterial oxygen saturation, and skin surface temperature were measured and recorded at the beginning and then every 10 min during the operation. If systolic pressure drop (more than 20% of the base) intravenous ephedrine was used as a vasopressor. In patients who develop shivering, intravenous meperidine (25 mg) should be used.
0 - No shivering
1 - Mild Fasciculations of face or neck
2 - Visible tremor involving more than one muscle group
3 - Gross muscular activity involving the entire body.[22]
Statistical analysis
Data were entered into SPSS version 16 (SPSS Inc., Chicago, Ill., USA). Fisher's exact test, ANOVA, and repeated measures was used for analysis of data. Moreover, data were expressed as mean ± standard deviation.
Results
The mean age of patients receiving tramadol (TR), TI and placebo (P) was 51.86 ± 5.70, 54.2 ± 5.65, and 55.36 ± 5.26 years old, respectively. Table 1 shows the mean age and body mass index (BMI) among three groups. As shown in Table 1, there was no significant difference among three groups in terms of age and BMI (P > 0.05).
Table 1.
The mean age and body mass index among three groups
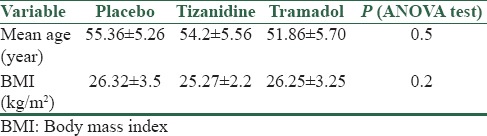
Table 2 shows the frequency of shivering in three groups during surgery and recovery.
Table 2.
Frequency of shivering in three groups
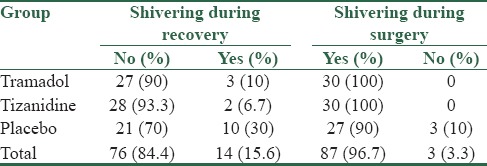
There was a significant difference among three groups in terms of shivering (P = 0.04). Moreover, no significant difference was seen between TR group with placebo and TI group with P in terms of shivering during surgery (P = 0.11). According to Fisher's exact test, significant difference was seen between TI group and P in terms of shivering during recovery (P = 0.02). Furthermore, significant difference was observed between TR group and P in terms of shivering during recovery (P = 0.05), while this difference was not significant between TR group and TI group (P = 0.5).
Table 3 shows severity of shivering in three groups.
Table 3.
Severity of shivering in three groups

According to ANOVA test, significant difference was observed among three groups in terms of severity of shivering (P = 0.001). No significant difference was observed between TR group and TI group with respect to severity of shivering (P = 0.80). However, significant difference was observed between TR group with P (P = 0.001) and TI group with P in terms of severity of shivering (P = 0.001).
Table 4 shows the frequency of nausea and vomiting in all groups during surgery and recovery.
Table 4.
Frequency of nausea and vomiting in all groups
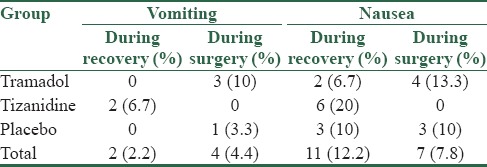
According to Fisher's exact test, there was no significant difference between TI group and P in terms of nausea during surgery (P = 0.11) and recovery (P = 0.05). No significant difference was seen between TR group and P with respect to nausea during surgery (P = 0.5) and recovery (P = 0.23). Moreover, no significant difference was seen between TR group and TI group with respect to nausea during surgery (P = 0.5) and recovery (P = 0.12).
Furthermore, there was no significant difference between TI group and P in terms of vomiting during surgery (P = 0.11) and recovery (P = 0.05). No significant difference was seen between TR group and P with respect to vomiting during surgery (P = 0.3) and recovery (P = 0.33). Moreover, no significant difference was seen between TR group and TI group with respect to vomiting during surgery (P = 0.11) and recovery (P = 0.24).
The mean arterial pressure before and during surgery (90 min) in three groups is shown in Table 5.
Table 5.
The mean arterial pressure before and during surgery in three groups
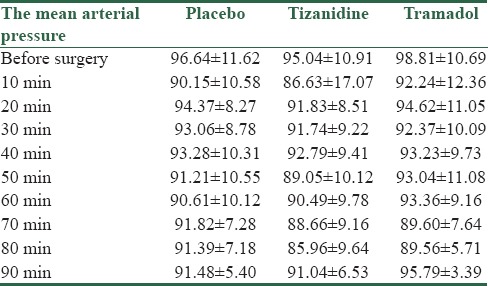
According to repeated measures, there was no significant difference between the mean arterial pressure before and during surgery in three groups (P = 0.08).
The mean heart rate before and during surgery (90 min) in three groups is shown in Table 6.
Table 6.
The mean heart rate before and during surgery in three groups
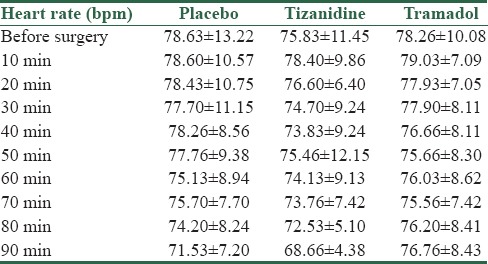
According to repeated measures, no significant difference was observed among three groups in terms of heart rate (P = 0.13). Table 7 shows the mean arterial oxygen saturation before and during surgery.
Table 7.
The mean arterial oxygen saturation before and during surgery
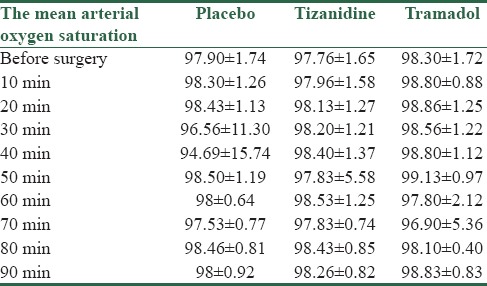
According to repeated measures, no significant difference was seen among three groups with respect to arterial oxygen saturation before and during surgery (P = 0.43). Table 8 shows the mean temperature in three groups before and during surgery.
Table 8.
The mean temperature in three groups before and during surgery
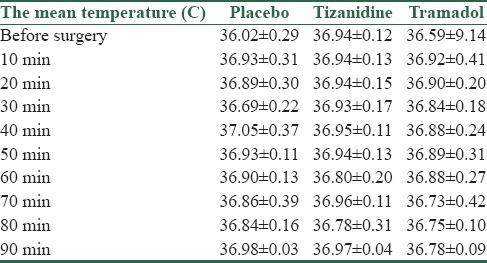
According to repeated measures, no significant difference was observed among three groups in terms of the mean temperature (P = 0.12).
Discussion
This study was conducted in operating room of Imam Khomeini Hospital during 1.5 years. Intra- and post-operative shivering is very unpleasant and annoying for patients and can lead to multiple complications. Today, the prevention and treatment of intra- and post-operative shivering is as important as the treatment of pain, and various methods and medications are used in this regard, but no method or an ideal drug has yet been identified. Tramadol is an opioid and it exerts its effect mainly through μ receptors. However, kappa and delta receptors are used less by tramadol. Moreover, it activates descending pain inhibitory pathways in the spinal cord. The mechanism of anti-shivering effect of tramadol is through serotonergic and noradrenergic receptors.
Obviously, prevention is preferable than treatment and causes the patient do not experience an unpleasant state of postoperative shivering.[11] Alpha-2 adrenergic agonists are now extensively used in anesthesia and critical care. Alpha-2-adrenergic agonists through binding to alpha-2 receptors cause vasoconstriction and decrease shivering. They also act on the thermoregulatory center (temperature control) in the hypothalamus.[15,22] The results of this study showed that oral TI and Tramadol before surgery decrease intra- and post-operative shivering in patients underwent spinal anesthesia, while there was no significant difference among three groups in terms of some parameters including nausea, vomiting, and hemodynamics. The heart rate of patients in TI group was significantly lower than other groups in recovery.
Shukla et al., in 2011 evaluated the effects of intravenous clonidine and tramadol on postoperative shivering in patients underwent spinal anesthesia. They reported that the loss of shivering was faster in clonidine group than tramadol group, although no significant difference was observed between two groups in terms of shivering.[21] Clonidine is more effective than tramadol for controlling body temperature. Moreover, clonidine has less side effects than tramadol. Furthermore, shivering is lower in TI group than other groups in our study. Tewari et al., in 2014 demonstrated the effect of 50 mg oral tramadol on decreasing shivering during TURP surgery with spinal anesthesia.[22] Moreover, they compared the effects of oral clonidine and tramadol for preventing shivering in patients underwent TURP with spinal anesthesia and found that both tramadol and clonidine were effective in reducing the severity and duration of shivering.[23]
Mittal et al., in 2014 evaluated the effects of dexmedetomidine and tramadol on hemodynamic and shivering after spinal anesthesia. They concluded that both drugs are effective on shivering rate, nausea, and vomiting. The alpha-2 agonist drug used in our study was TI, in which we did not evaluate the decrease rate of shivering incidence. However, the incidence of shivering decreased in both groups. The incidence of nausea and vomiting was lower in the TI group than other groups, but this difference was not significant.[24]
Heidari et al., in 2014 evaluated the effects of oral tramadol and placebo on the severity of postoperative shivering in patients with general anesthesia. The results showed that there was no significant difference between case and control groups in terms of shivering which was not consistent with our study. The type of surgery and sex difference of the patients can justify this inconsistency.[25] It seems that the use of alpha-2 agonists to prevent and reduce shivering in patients underwent spinal anesthesia is reasonable and appropriate. These drugs can have a sedative effect on the patients during surgery which lead to reduce anxiety. In our study, we could evaluate and compare other parameters such as sedation and postoperative analgesia.
Conclusions
The use of methadone or alpha-2 agonists in patients with contraindications for meperidine is important. According to the results of the current study further studies are needed to confirm the effects of methadone and TI on shivering treatment, especially the dose and long-term side effects of medications. Moreover, it is proposed that injectable drugs including dexmedetomidine and methadone are used and compared for controlling and treating shivering.
Financial support and sponsorship
Urmia University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We are very grateful from all the people and friends who helped us in this study.
References
- 1.Lienhart A, Fiez N, Deriaz H. Postoperative shivering: Analysis of main associated factors. Ann Fr Anesth Reanim. 1992;11:488–95. doi: 10.1016/s0750-7658(05)80753-1. [DOI] [PubMed] [Google Scholar]
- 2.Frank SM, Fleisher LA, Breslow MJ, Higgins MS, Olson KF, Kelly S, et al. Perioperative maintenance of Normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA. 1997;277:1127–34. [PubMed] [Google Scholar]
- 3.Eberhart LH, Döderlein F, Eisenhardt G, Kranke P, Sessler DI, Torossian A, et al. Independent risk factors for postoperative shivering. Anesth Analg. 2005;101:1849–57. doi: 10.1213/01.ANE.0000184128.41795.FE. [DOI] [PubMed] [Google Scholar]
- 4.Sharkey A, Lipton JM, Murphy MT, Giesecke AH. Inhibition of postanesthetic shivering with radiant heat. Anesthesiology. 1987;66:249–52. doi: 10.1097/00000542-198702000-00029. [DOI] [PubMed] [Google Scholar]
- 5.Brownridge P. Shivering related to epidural blockade with bupivacaine in labour, and the influence of epidural pethidine. Anaesth Intensive Care. 1986;14:412–7. doi: 10.1177/0310057X8601400414. [DOI] [PubMed] [Google Scholar]
- 6.Joris J, Banache M, Bonnet F, Sessler DI, Lamy M. Clonidine and ketanserin both are effective treatment for postanesthetic shivering. Anesthesiology. 1993;79:532–9. doi: 10.1097/00000542-199309000-00017. [DOI] [PubMed] [Google Scholar]
- 7.Doufas AG, Lin CM, Suleman MI, Liem EB, Lenhardt R, Morioka N, et al. Dexmedetomidine and meperidine additively reduce the shivering threshold in humans. Stroke. 2003;34:1218–23. doi: 10.1161/01.STR.0000068787.76670.A4. [DOI] [PubMed] [Google Scholar]
- 8.Kizilirmak S, Karakaş SE, Akça O, Ozkan T, Yavru A, Pembeci K, et al. Magnesium sulphatestops postanesthetic shivering. Proc N Y Acad Sci. 1997;813:799–806. doi: 10.1111/j.1749-6632.1997.tb51784.x. [DOI] [PubMed] [Google Scholar]
- 9.Shrestha AB. Comparative study on effectiveness of doxapram and pethidine for postanaesthetic shivering. JNMA J Nepal Med Assoc. 2009;48:116–20. [PubMed] [Google Scholar]
- 10.Alfonsi P. Postanaesthetic shivering. Epidemiology, pathophysiology and approaches to prevention and management. Minerva Anestesiol. 2003;69:438–42. [PubMed] [Google Scholar]
- 11.Mahmood MA, Zweifler RM. Progress in shivering control. J Neurol Sci. 2007;261:47–54. doi: 10.1016/j.jns.2007.04.038. [DOI] [PubMed] [Google Scholar]
- 12.Roy JD, Girard M, Drolet P. Intrathecal meperidine decreases shivering during cesarean delivery under spinal anesthesia. Anesth Analg. 2004;98:230–4. doi: 10.1213/01.ANE.0000093251.42341.74. [DOI] [PubMed] [Google Scholar]
- 13.Techanivate A, Dusitkasem S, Anuwattanavit C. Dexmedetomidine compare with fentanyl for postoperative analgesia in outpatient gynecologic laparoscopy: A randomized controlled trial. J Med Assoc Thai. 2012;95:383–90. [PubMed] [Google Scholar]
- 14.le Roux PJ, Coetzee JF. Tramadol today. Curr Opin Anaesthesiol. 2000;13:457–61. doi: 10.1097/00001503-200008000-00010. [DOI] [PubMed] [Google Scholar]
- 15.Mathews S, Al Mulla A, Varghese PK, Radim K, Mumtaz S. Postanaesthetic shivering – A new look at tramadol. Anaesthesia. 2002;57:394–8. doi: 10.1046/j.1365-2044.2002.2457_3.x. [DOI] [PubMed] [Google Scholar]
- 16.Trekova NA, Buniatian AA, Zolicheva NI. Tramadol hydrochloride in the treatment of postoperative shivering. Anesteziol Reanimatol. 2004;(5):86–9. [PubMed] [Google Scholar]
- 17.Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43:879–923. doi: 10.2165/00003088-200443130-00004. [DOI] [PubMed] [Google Scholar]
- 18.Miller E, Fleisher LA, Wiener-Kronish Y. Millers Anesthesia. 7th ed. Philadelphia: Churchill Livingstone; 2010. p. 1869. [Google Scholar]
- 19.Miettinen TJ, Kanto JH, Salonen MA, Scheinin M. The sedative and sympatholytic effects of oral tizanidine in healthy volunteers. Anesth Analg. 1996;82:817–20. doi: 10.1097/00000539-199604000-00024. [DOI] [PubMed] [Google Scholar]
- 20.Movassaghi G, Palideh H. Comparison between antishiverig effects of meperidine and methadon. RJMS. 2002;9:107–11. [Google Scholar]
- 21.Shukla U, Malhotra K, Prabhakar T. A comparative study of the effect of clonidine and tramadol on post-spinal anaesthesia shivering. Indian J Anaesth. 2011;55:242–6. doi: 10.4103/0019-5049.82666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tewari A, Dhawan I, Mahendru V, Katyal S, Singh A, Garg S, et al. Use of oral tramadol to prevent perianesthetic shivering in patients undergoing transurethral resection of prostate under subarachnoid blockade. Saudi J Anaesth. 2014;8:11–6. doi: 10.4103/1658-354X.125898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tewari A, Dhawan I, Mahendru V, Katyal S, Singh A, Narula N, et al. A comparative study evaluating the prophylactic efficacy of oral clonidine and tramadol for perioperative shivering in geriatric patients undergoing transurethral resection of prostate. J Anaesthesiol Clin Pharmacol. 2014;30:340–4. doi: 10.4103/0970-9185.137264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mittal G, Gupta K, Katyal S, Kaushal S. Randomised double-blind comparative study of dexmedetomidine and tramadol for post-spinal anaesthesia shivering. Indian J Anaesth. 2014;58:257–62. doi: 10.4103/0019-5049.135031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Heidari SM, Rahimi M, Soltani H, Hashemi SJ, Shabahang S. Premedication with oral tramadol reduces severity of postoperative shivering after general anesthesia. Adv Biomed Res. 2014;3:64. doi: 10.4103/2277-9175.125845. [DOI] [PMC free article] [PubMed] [Google Scholar]