

Abstract
Background
The use of mobile phone information technology (IT) in the health sector has received much attention especially during the 2014-2015 Ebola virus disease (EVD) outbreak. mHealth can be attributed to a major improvement in EVD control, but there lacks an overview of what kinds of tools were available and used based on the functionalities they offer.
Objective
We aimed to conduct a systematic review of mHealth tools in the context of the recent EVD outbreak to identify the most promising approaches and guide further mHealth developments for infectious disease control.
Methods
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, we searched for all reports on mHealth tools developed in the context of the 2014-2015 EVD outbreak published between January 1, 2014 and December 31, 2015 on Google Scholar, MEDLINE, CAB Abstracts (Global Health), POPLINE, and Web of Science in any language using the search strategy: (“outbreak” OR “epidemic”) AND (“mobile phone” OR “smartphone” OR “smart phone” OR “mobile phone” OR “tablet” OR “mHealth”) AND (“Ebola” OR ”EVD” OR “VHF” OR “Ebola virus disease” OR “viral hemorrhagic fever”) AND (“2014” OR “2015”). The relevant publications were selected by 2 independent reviewers who applied a standardized data extraction form on the tools’ functionalities.
Results
We identified 1220 publications through the search strategy, of which 6.31% (77/1220) were original publications reporting on 58 specific mHealth tools in the context of the EVD outbreak. Of these, 62% (34/55) offered functionalities for surveillance, 22% (10/45) for case management, 18% (7/38) for contact tracing, and 6% (3/51) for laboratory data management. Only 3 tools, namely Community Care, Sense Ebola Followup, and Surveillance and Outbreak Response Management and Analysis System supported all four of these functionalities.
Conclusions
Among the 58 identified tools related to EVD management in 2014 and 2015, only 3 appeared to contain all 4 key functionalities relevant for the response to EVD outbreaks and may be most promising for further development.
Keywords: case management, contact tracing, Ebola virus disease, eHealth, mHealth, systematic review, West Africa
Introduction
Background
The 2014-2015 Ebola virus disease (EVD) outbreak caused almost 11,000 deaths and tragically demonstrated the need for effective surveillance and outbreak management [1]. In the absence of established vaccines and specific pharmaceutical treatment, the main measure of containment for epidemics caused by emerging pathogens like Ebola virus is a rapid and efficient interruption of human-to-human transmission. Even for diseases for which vaccines or specific treatments are available, the epidemiological, nonpharmaceutical control measures are indispensable [2]. A particular challenge for EVD control is contact tracing, which assures that all persons who had contact with an EVD case are identified and monitored for the potential appearance of symptoms for 21 days after exposure to a patient with EVD [3].
Containment Strategy
Dhillon et al (2014) stated that for an epidemic such as Ebola virus to be controlled, complementary interventions are required, namely (1) community engagement; (2) identification of contacts; (3) contact monitoring for symptoms; (4) rapid lab confirmation of cases; (5) isolation and treatment of new cases; and (6) safe and dignified burials. Each activity is fundamentally complex, yet all need to be harmonized to stop transmission and control the outbreak [4]. Because of the dynamically changing nature of epidemics, it is important to have real-time data for action, strategy, and coordination of multiple efforts or interventions to ensure efficient execution of tasks and protocols and also a management platform that aligns, coordinates, and monitors all these measures and information resulting from them.
Integrated Disease and Surveillance Response
In 1998, the World Health Organization (WHO) African Regional Office established the resolution of the 48th assembly endorsing Integrated Disease Surveillance and Response (IDSR) for all member countries to adopt as the core strategy to strengthen national disease surveillance systems. The objective of the IDSR is to strengthen district-level surveillance and response for epidemic-prone diseases, integrating laboratory support for reference laboratories, reducing the duplication of reporting, and sharing resources among disease control programs, which in turn translates surveillance and laboratory data into timely public health actions [5]. The major setback with the IDSR since 1998 is that in practice, it remains majorly a paper-based system, collecting information from the periphery and transporting it in an aggregated manner, which results in considerable delay to the national level without implementing the notion of bidirectional information flow and even less that of integrated response [6].
mHealth Technology
The use of mobile phone information technology (IT) in the health sector (mobile health, mHealth) has received much attention, especially during the EVD outbreak and could in principle help implement the basic fundamentals of IDSR [7]. mHealth promises to overcome many of the communication and management hurdles and delays commonly experienced in countries with limited infrastructure in communication and transportation [8]. A study conducted in 2009 by WHO confirmed that majority of the WHO member states offer health call centers and toll-free emergency services using mobile communications, but these programs rarely used mHealth in surveillance, raising public awareness, and decision support systems [9]. These require enhanced capabilities and infrastructure to implement and therefore may not be a health priority in affiliate states with financial constraints. Evaluation is important to determine cost-effectiveness and involves educating the community about the benefits of mHealth, which leads to government policy. Despite the need for evaluation, the survey found that results-based evaluation of mHealth implementations is not routinely conducted, and only 12% of member states reported evaluating mHealth services [9].
Study Objective
The main objective of this study was to generate an overview of mHealth tools that were developed from 2014 to 2015 to identify tools with the most promising portfolio of functionalities, which might build the basis for further mHealth developments for infectious disease surveillance and control.
Methods
Identification Criteria
We conducted a systematic search for all articles published in any language indexed in Google Scholar, MEDLINE, CAB Abstracts (Global Health), POPLINE, and Web of Science with publication dates from January 1, 2014 to December 31, 2015 using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [10].
Systematic Search and Selection
We used the following search strategy: (“Outbreak” OR “Epidemic”) AND (“mobile phone” OR “smartphone” OR “smart phone” OR “mobile phone” OR “tablet” OR “mHealth”) AND (“Ebola” OR ”EVD” OR “VHF” OR “Ebola Virus Disease” OR “viral hemorrhagic fever”) AND (“2014” OR “2015”).
The publications that were original, addressed mHealth in the context of the EVD outbreak, and reported on specific mHealth tools were independently selected by 2 coauthors (DTA and CCA). In case of discrepancy in assessment, both authors revised the findings and agreed on a joint assessment.
The first step was to screen titles and abstracts and discard any publication that was not original such as editorials, summaries, videos, and commentaries. The second step was to select those publications that, based on title or abstract, covered or dealt with an actual mHealth tool that runs on mobile phones and tablets and dealt with the management of EVD or other hemorrhagic fever outbreaks. The third step was to select those publications that, based on the full article, reported on or described ≥1 specific mHealth tool within the context defined above.
Categorization and Extraction
Each publication finally selected for review was categorized as one of the following: book chapter, scientific peer-reviewed journal article, or nonpeer-reviewed Web article. To extract the content of these publications, we used a standardized extraction form assessing key functionalities, technical characteristics, and epidemiological capabilities of the respective mHealth tools.
Key Functionalities
The key functionalities included (1) surveillance capability (ability of the tool to cover surveillance tasks); (2) contact tracing (capacity of the tool to conduct contact interviews, take temperature, follow-up contacts for a certain number of days, and display results); (3) case management (ability of the tool to handle case management issues such as alert response for immediate suspect case evacuation, disinfection, and isolation as well as provide feedback for contact tracing and follow-up) [8]; and (4) laboratory data management (ability to integrate and update laboratory findings, an essential component of case verification).
Technical Characteristics
The technical characteristics included the following:
Offline capabilities: the ability of the tool to still function if there is no internet or data network and to send automatically stored data to the server once it connects again to a network.
Type of system: whether the tool was developed on an open or closed source platform.
Server characteristics: the ability of the tool to function as a cloud network or client side network, installation criteria regarding automatic updates, and user-friendly installation process.
Integrated data analytics: the capacity of the tool to analyze and generate reports for immediate action automatically.
Data migration: the capability of the tool to import and export data and its elements from 1 platform to the other.
Data security system: the security of the data system with respect to disaster recovery, data protection, and backups.
Bidirectional information flow: the data flow from the lowest level of data entry to the highest level of decision making and analysis with a standardized feedback mechanism back to the lowest level.
Epidemiological Characteristics
The epidemiological characteristics included the following:
Outbreak management unspecified, referring to tools that state the offering of functionalities but do not specify which ones and how.
Rumor management capability to capture rumors from the community via a hotline and real-time situational awareness to track the detection of diseases and spread.
National response management functionality to coordinate response measures at national level.
Regional response management functionality to coordinate response measures at regional or state level.
District response management functionality to coordinate response measures at the district level.
Performance of a systematic evaluation to evaluate the usefulness of the tool.
Piloted or deployed for use in the field via tool implementation in the field with real patients, at least for piloting.
Design based on IDSR concepts and strategy used for health surveillance in Africa.
Design based on preexisting data models such as Centers for Disease Control and Prevention viral hemorrhagic fever case investigation form integration or Epi Info Viral Hemorrhagic Fever App [11].
Health facility notification, referring to health facilities using the tool to notify cases digitally.
Data Analysis
Data variable responses were categorized into yes (function available), no (function not available), or unknown (publication does not clearly reveal whether the tool offers the respective function or not). For computation of percentages, we used the sum of yes and no answers for each of the respective outcomes as the denominator.
Results
Identified Publications
We identified 1220 publications from the automatic search in Google Scholar. PubMed found 8 publications that were duplicates of those in Google Scholar, 4 of which were relevant to the topic. We did not find any publications in CAB Abstracts (Global Health), POPLINE, or and Web of Science using the same search string across the search engines. After manual selection, we identified 79.10% (965/1220) original publications of which 15.0% (145/965) addressed mHealth and EVD outbreak response. Among these 145 publications, 53.1% (77/145) reported on 58 specific mHealth tools. Figure 1 shows the flowchart of the number of publications initially retrieved and the proportion selected for extraction following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses approach.
Figure 1.
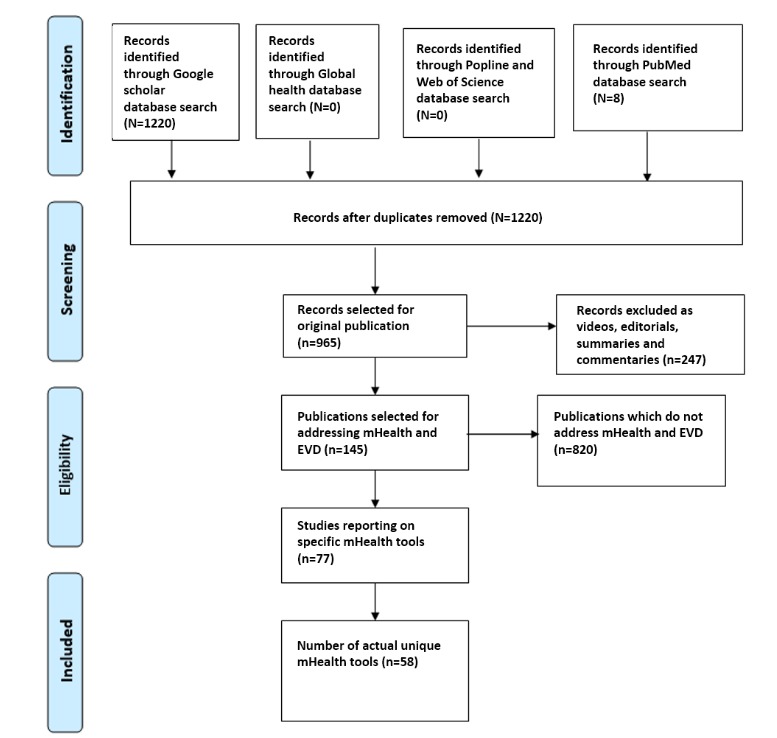
Preferred Reporting Items for Systematic Reviews and Meta-Analyses approach for the selection of publications on mHealth tools for the 2014-2015 Ebola virus disease outbreak. EVD: Ebola virus disease.
Key Functionalities
With respect to the 4 key functionalities, 62% (34/55) out of the 55 tools offered functionalities for surveillance, 22% (10/45) for case management, 18% (7/38) for contact tracing, and 6% (3/51) for laboratory data management. Only 3 tools, namely Community Care (CommCare) [12], Sense Ebola Followup [13], and Surveillance and Outbreak Response Management and Analysis System (SORMAS) [14] supported all 4 of these functionalities (3/58, 5%). The detailed profile of key functionalities is displayed in Table 1.
Table 1.
Key functionalities for 58 mHealth Ebola virus disease tools, 2014-2015.
| Key functionalities | Yes, n | No, n | Unknown, n | Yesa, % |
| Surveillance capability | 34 | 21 | 3 | 62 |
| Contact tracing | 7 | 31 | 1 | 18 |
| Case management | 10 | 35 | 13 | 22 |
| Laboratory data management | 3 | 48 | 7 | 6 |
aThe sum of yes and no answers for each of the respective functionalities was used as the denominator.
Technical Characteristics
Table 2 displays the technical characteristics of the 58 identified tools. For 3% (2/58) of the tools, namely CommCare and Sense Ebola Followup, the publications indicated that they displayed all 7 technical characteristics.
Table 2.
Technical characteristics for 58 mHealth Ebola virus disease tools, 2014-2015.
| Technical characteristics | Yes, n | No, n | Unknown, n | Yesa, % |
| Offline capabilities | 9 | 24 | 25 | 27 |
| Type of system (open source) | 36 | 21 | 1 | 63 |
| Server characteristics | 43 | 15 | 0 | 74 |
| Integrated data analytics | 22 | 11 | 25 | 67 |
| Data migration | 40 | 18 | 0 | 69 |
| Data security system | 33 | 6 | 19 | 85 |
| Bidirectional information flow | 7 | 40 | 11 | 15 |
aThe sum of yes and no answers for each of the respective characteristics was used as the denominator.
Epidemiological Characteristics
Table 3 contains the results of the epidemiological characteristics. All 10 epidemiological characteristics were present for 2% (1/58) of the tools, namely SORMAS.
Table 3.
Epidemiological characteristics for 58 mHealth Ebola virus disease tools, 2014-2015.
| Epidemiological characteristics | Yes, n | No, n | Unknown, n | Yesa, % |
| Outbreak management unspecified | 5 | 50 | 3 | 9 |
| Rumor management | 7 | 31 | 20 | 18 |
| National response management | 6 | 43 | 9 | 12 |
| Regional response management | 8 | 42 | 8 | 16 |
| District response management | 8 | 42 | 8 | 16 |
| Systematic evaluation | 24 | 16 | 18 | 60 |
| Piloted or deployed | 26 | 16 | 16 | 62 |
| Design based on Integrated Disease and Surveillance Response concepts and strategy used for health surveillance in Africa | 3 | 52 | 3 | 5 |
| Design based on preexisting data models such as Center for Disease Control and Prevention viral hemorrhagic fever case investigation form integrated or Epi Info Viral Hemorrhagic Fever Application | 2 | 53 | 3 | 4 |
| Health facility notification | 27 | 23 | 8 | 54 |
aThe sum of yes and no answers for each of the respective outcomes was used as the denominator.
None of the 58 tools covered all 4 key functionalities, all 7 technical characteristics, and all 10 epidemiological characteristics. SORMAS covered 20 functionalities and characteristics, the highest within 1 tool, 1 of its missing characteristics being open source. Table 4 shows a breakdown of the 58 identified mHealth tools according to the key functionalities for EVD outbreak management.
Table 4.
Characteristics of the 58 mHealth tools showing the key functionalities for Ebola virus disease outbreak management.
| Name of mHealth tool | Surveillance | Contact tracing | Case management | Laboratory data management |
| BioCaster Portal | Yes | Unknown | Yes | No |
| Bio-Sense 2.0 | Yes | Unknown | Yes | No |
| BSVE | Yes | Unknown | Unknown | No |
| CDRs Simulator | Unknown | Unknown | Unknown | Unknown |
| Cell phone messaging technology | No | No | No | No |
| CKAN | No | No | No | No |
| CliniPAK | Unknown | Unknown | Unknown | Unknown |
| Collaborative Overarching Multi-feed Biosurveillance System (COMBS) | Yes | Unknown | Yes | No |
| CommCare Contact Tracing | Yes | Yes | Yes | Yes |
| Data De-Identification Toolkit | Yes | Unknown | Unknown | No |
| DHIS 2 | Yes | No | No | No |
| Doctor App | No | No | No | No |
| Early Warning systems (EWS) | Yes | No | No | No |
| Sense Ebola Followup | Yes | Yes | Yes | Yes |
| Ebola Spatial Care Path (POCT) | Unknown | Unknown | Unknown | Unknown |
| Ebola Tracks | Yes | Yes | No |
|
| EbolaAlert | Yes | Unknown | No | No |
| EIDSS | Yes | Unknown | Unknown | No |
| EpiRobot | No | No | No | No |
| Esoko SMS app/WhatsApp | No | No | No | No |
| ESSENCE-FL | Yes | Unknown | Unknown | No |
| No | No | No | No | |
| Flu Caster | Yes | No | No | No |
| Google Analytics | No | No | No | No |
| GPHIN | Yes | No | No | No |
| GSMS | No | No | No | Unknown |
| Hadoop | No | No | No | No |
| Health 2.0 | No | No | No | No |
| Healthmap | Yes | No | No | No |
| HIT | No | No | No | No |
| iPhone app | No | No | No | No |
| LEEDS | Yes | Unknown | Unknown | No |
| mHealth real-time infectious disease interface (contact tracing app) | Yes | Yes | No | Unknown |
| NNDSS | Yes | Unknown | Yes | No |
| Open Data Kit | Yes | Yes | No | No |
| OpenESSENCE | Yes | Unknown | Unknown | No |
| OpenMRS | Yes | Unknown | Unknown | No |
| OpenStreetMap (maapJack) | No | No | No | No |
| PHIN-MS | Yes | Unknown | Unknown | No |
| Polly | No | No | No | No |
| POP (Practice-Oriented Project) on Crowdmap | No | No | No | No |
| QGIS | No | No | Yes | No |
| R | Yes | Unknown | Unknown | No |
| RapidSMS | No | No | No | No |
| Response Call Center app | Yes | No | No | Unknown |
| SAGES | Yes | Unknown | Unknown | No |
| Screening expert system (SES) | Yes | No | No | No |
| Sentinel surveillance system (SSS) | Yes | Unknown | Yes | No |
| SMARTech | Yes | Unknown | No | No |
| Smartphone-based contact tracing system | Yes | Yes | No | No |
| SORMAS | Yes | Yes | Yes | Yes |
| SoundCloud | No | No | No | No |
| SWAP (surveillance window app) | Yes | Unknown | Unknown | No |
| Telefónica | No | No | No | No |
| Telemedicine | Yes | No | Yes | No |
| The Minnesota African Task Force Against Ebola (MATFAE) | No | No | No | No |
| No | No | No | No | |
| WBDS | Yes | Unknown | Unknown | No |
Discussion
Principal Findings
It is surprising that as many as 58 mHealth tools identified in our search addressed management of EVD (hemorrhagic fever) during the 2014-2015 outbreak. The vast difference in functionality indicates that during the wake of the tragic outbreak and the urgency to stop the outbreak, many initiatives were started, which aimed and claimed to provide support for EVD outbreak response. However, only a few appear to have contained sufficient medical and public health expertise to actually address the procedural and technical needs. It is, therefore, needful to carefully assess the respective specifications and functionalities via a quality control system before deciding on one tool or another for deployment in such a situation. Only 3 tools have the overall capability for the key functionalities of surveillance and outbreak management (surveillance capability, contact tracing, and case management) and contain embedded functional requirements for data reporting and analytics through an integrated implementation of the surveillance guidelines and standards regarding functionality. Some tools, such as District Health Information System 2, had the advantage of being widespread in West Africa as a health management information system [15], yet it was not designed to manage interventions as needed for infection control and outbreak response by itself. Such a tool should feed information into every task related to a particular officer and improve each task assigned to the officer [16]. Ideally, it can be used as a real-time rumor management system, contact-tracing management system, case management system, and a surveillance system. The tool should include disease control management functionalities [17].
The tools CommCare, Sense Ebola Followup, and SORMAS supported all tasks and functions involving surveillance, contact tracing, and case management. CommCare and Sense Ebola Followup were used during the EVD outbreak. SORMAS was piloted in the field during the EVD outbreak after the epidemic in Nigeria and is therefore based on a practical EVD outbreak scenario. Additionally, it contains a function for rumor management, which was particularly important during the 2014-2015 Ebola outbreak [18]. Sense Ebola Followup was deployed during the EVD outbreak in Nigeria [19]. Since outbreaks only occur sporadically, and the information processed during an outbreak is comparable to that handled for surveillance purposes, it appears necessary to aim for a system that can function as a monitoring tool as well as an outbreak management tool [20]. Another factor that is likely to affect the acceptability of an mHealth tool is the independence from a specific provider. Tools based on open source platforms are more sustainable in this aspect and can potentially build a dynamic broader programming community for further developments and improvements. CommCare and Sense Ebola Followup were developed on an open source platform [21]. SORMAS was originally programmed in platforms proprietary to Systems Applications and Products [22] but has now been developed on an open source platform (SORMAS-open) [23].
CommCare Ebola Contact Tracking
The cloud server open source Android app for contact tracking developed in 2014 was based on the CommCare development platform, which was designed to support Community Health Extension Workers acting in Guinea, and it has been promoted by the United Nations Population Fund, other United Nations agencies, and the actors involved in the fight against Ebola in Guinea [21]. CommCare technology was chosen to support the implementation of the Government Response Plan against EVD in order to obtain timely and reliable information as well as facilitate contact tracing. The Earth Institute at Columbia University (USA), United Nations Population Fund, and the Monitoring Cell of the National Coordination Against the Ebola Virus have promoted the idea. It requires a CommCare account and the Open Data Kit for Android to be deployed on an Android phone or tablet [24].
Sense Ebola Followup App
The contact-tracing follow-up electronic health (eHealth) Sense app was developed in 2014 during the EVD outbreak in Nigeria. It is a mobile phone app for real-time data capture. The major technologies used were 2 Android-based apps, the Open Data Kit and Formhub [24]. Supporting technologies were dashboard technology and ArcGIS mapping. The contact listing form, contact follow-up form, laboratory investigation request, and case investigation forms were created using extensible markup language and the eHealth Sense Ebola Android app [19] developed for 21-day follow-up. It has an automatic alert system for temperature readings ≥38°C for contacts that were under follow-up.
Surveillance and Outbreak Response Management and Analysis System
SORMAS is an open source Android and Web app, which was developed for case management, contact tracing, and surveillance with an equipped laboratory module for management of laboratory samples and tests [25]. SORMAS enables surveillance officers and epidemiologists to detect diseases based on real-time health facility data. Automatic notification validates rumors and notifications, and SORMAS enables decision makers to respond immediately to incoming information and to take adequate measures via the public health officers. Information about cases and contacts are made readily available for action, data quality assurance is performed for decontamination, and isolation tasks can be conducted.
Limitations
Only a fraction of the identified publications was found in conventional scientific literature databases, such as Medline and PubMed, all of which were duplicates, but 99% of the publications were found in Google Scholar. This may indicate a major limitation of our approach. The methodology of systematic reviews, being well established in evidence-based medicine, may be of limited value for health informatics because it may not be as common practice in the IT field to publish developments and findings in scientific journals, even less so in peer-reviewed ones. The urgency by which tools were developed in response to the EVD outbreak may even have accentuated this effect. Search criteria imputed to PubMed displayed only 8 results compared with 965 results in Google Scholar. An explanation might be that mHealth initiatives born out of urgent public health needs may not be accompanied by a systematic process of planning and evaluation and are thus not likely to be transferred into sustainable continuous implementation and even less likely to be published in scientific publications once the urgency of the need has diminished.
While it would have been valuable to conduct this review beyond the application of EVD and hemorrhagic fevers and beyond 2015, removing these selection criteria from the search strategy would have resulted in an unmanageably large output with an extremely low positive predictive value. Hence, we covered mHealth tools developed between 2014 and 2015. Taking into consideration the fact that we stopped data collection on December 31, 2015 on a topic that became relevant shortly before that, the delay in publication may have led to some tools not being captured in our analysis. There was a limited appearance of publications in established databases such as Medline, although Google Scholar will generate a very comprehensive, but also unspecified, output of search strategies that are not defined in a highly-targeted way, especially if the period is increased beyond 2015.
Conclusion
Among a large number of reported tools developed in the context of the EVD outbreak response, it appears that only 3 of these tools contain the 3 key functionalities of outbreak management for EVD (surveillance capability, contact tracing, and case management) supported by tools developed from January 2014 to December 2015. These 3 tools, namely CommCare, Sense Ebola Followup, and SORMAS may serve as an orientation and reference for further developments of mHealth tools for infectious disease surveillance and outbreak management.
Acknowledgments
The authors wish to thank Salla E Toikkanen, Prof Adebola Olayinka, Bernard Silenou Chawo, and Gabriele Poggensee.
Abbreviations
- CommCare
Community Care open source mobile platform
- EVD
Ebola virus disease
- IDSR
Integrated Disease Surveillance and Response
- IT
information technology
- SORMAS
Surveillance and Outbreak Response Management and Analysis System
- WHO
World Health Organization
Footnotes
Authors' Contributions: DTA and CCA searched, selected, and extracted data based on criteria; DTA and GK conceptualized the study design and analyzed and interpreted the results of the data; GK initiated the study approach and supervised all steps of the study; PMN contributed to the manuscript confirming events and outcomes of software applications. All authors read and approved the final manuscript.
Conflicts of Interest: None declared.
References
- 1.World Health Organization. 2016. Situation Report 2016 Ebola Virus Disease in West Africa http://apps.who.int/iris/bitstream/10665/206536/1/ebolasitrep_19May2016_eng.pdf?ua=1 .
- 2.Center for Disease Control and Prevention. [2018-03-29]. Treatment https://www.cdc.gov/vhf/ebola/treatment/
- 3.Center for Disease Control and Prevention. [2018-03-29]. Implementation and management of contact tracing for Ebola virus disease https://www.cdc.gov/vhf/ebola/pdf/contact-tracing-guidelines.pdf .
- 4.Dhillon RS, Srikrishna D, Sachs J. Controlling Ebola: next steps. Lancet. 2014 Oct 18;384(9952):1409–11. doi: 10.1016/S0140-6736(14)61696-2.S0140-6736(14)61696-2 [DOI] [PubMed] [Google Scholar]
- 5.Brinkel J, Krämer A, Krumkamp R, May J, Fobil J. Mobile Phone-Based mHealth Approaches for Public Health Surveillance in Sub-Saharan Africa: A Systematic Review. IJERPH. 2014 Nov 12;11(11):11559–11582. doi: 10.3390/ijerph111111559. http://www.mdpi.com/1660-4601/11/11/11559/htm . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Isere Elvis E, Fatiregun Akinola A, Ajayi Ikeoluwapo O. An overview of disease surveillance and notification system in Nigeria and the roles of clinicians in disease outbreak prevention and control. Niger Med J. 2015;56(3):161–8. doi: 10.4103/0300-1652.160347. http://www.nigeriamedj.com/article.asp?issn=0300-1652;year=2015;volume=56;issue=3;spage=161;epage=168;aulast=Isere .NMJ-56-161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nasi GCM, Cucciniello Maria, Guerrazzi Claudia. The role of mobile technologies in health care processes: the case of cancer supportive care. J Med Internet Res. 2015 Feb 12;17(2):e26. doi: 10.2196/jmir.3757. http://www.jmir.org/2015/2/e26/ v17i2e26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fähnrich C, Denecke K, Adeoye O O, Benzler J, Claus H, Kirchner G, Mall S, Richter R, Schapranow M P, Schwarz N, Tom-Aba D, Uflacker M, Poggensee G, Krause G. Surveillance and Outbreak Response Management System (SORMAS) to support the control of the Ebola virus disease outbreak in West Africa. Euro Surveill. 2015 Mar 26;20(12) doi: 10.2807/1560-7917.es2015.20.12.21071. http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=21071 . [DOI] [PubMed] [Google Scholar]
- 9.World Health Organization. New horizons for health through mobile technologies: second global survey on eHealth http://www.who.int/goe/publications/goe_mhealth_web.pdf .
- 10.PRISMA. 2018. PRISMA Flow Diagram http://www.prisma-statement.org/PRISMAStatement/FlowDiagram .
- 11.Centers for Disease Control and Prevention. Epi Info viral hemorrhagic fever application https://archive.codeplex.com/?p=epiinfovhf .
- 12.Dimagi. [2018-03-29]. Commcare for Ebola Response https://www.dimagi.com/sectors/ebola-response/
- 13.Tom-Aba Daniel, Olaleye Adeniyi, Olayinka Adebola Tolulope, Nguku Patrick, Waziri Ndadilnasiya, Adewuyi Peter, Adeoye Olawunmi, Oladele Saliu, Adeseye Aderonke, Oguntimehin Olukayode, Shuaib Faisal. Innovative Technological Approach to Ebola Virus Disease Outbreak Response in Nigeria Using the Open Data Kit and Form Hub Technology. PLoS One. 2015;10(6):e0131000. doi: 10.1371/journal.pone.0131000. http://dx.plos.org/10.1371/journal.pone.0131000 .PONE-D-14-53622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Adeoye O, Tom-Aba D, Ameh C, Ojo O, Ilori E, Gidado S, Waziri E, Nguku P, Mall S, Denecke K, Lamshoeft M, Schwarz N, Krause G, Poggensee G. Implementing Surveillance and Outbreak Response Management and Analysis System (SORMAS) for Public Health in West Africa- Lessons Learnt and Future Direction. Int J Trop Dis Health. 2017 Jan 10;22(2):1–17. doi: 10.9734/IJTDH/2017/31584. http://www.sciencedomain.org/abstract/18127 . [DOI] [Google Scholar]
- 15.Open Health News. 2018. [2018-03-29]. District Health Information System: DHIS2 https://www.dhis2.org/
- 16.World Health Organization. 2014. Oct 20, [2018-03-29]. Nigeria is now free of Ebola virus transmission http://www.who.int/mediacentre/news/ebola/20-october-2014/en/
- 17.Tambo E, Ugwu Emmanuel Chidiebere, Ngogang Jeane Yonkeu. Need of surveillance response systems to combat Ebola outbreaks and other emerging infectious diseases in African countries. Infect Dis Poverty. 2014;3:29. doi: 10.1186/2049-9957-3-29. https://idpjournal.biomedcentral.com/articles/10.1186/2049-9957-3-29 .2049-9957-3-29 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Perscheid C, Benzler J, Hermann C, Janke M, Moyer D, Laedtke T, Adeoye O, Denecke K, Kirchner G, Beermann S, Schwarz N, Tom-Aba D, Krause G. Ebola Outbreak Containment: Real-Time Task and Resource Coordination With SORMAS. Front. ICT. 2018 Apr 10;5:2018–03. doi: 10.3389/fict.2018.00007. https://www.frontiersin.org/articles/10.3389/fict.2018.00007/abstract . [DOI] [Google Scholar]
- 19.EHealth Africa. 2018. [2018-03-29]. EHealth Sense Ebola app http://ehealthafrica.github.io/case-studies/sense-followup.html .
- 20.SORMAS. [2018-03-30]. Open Source version of SORMAS https://sormasorg.helmholtz-hzi.de/Github_SORMAS.html .
- 21.Dimagi. [2018-03-29]. Introducing CommCare https://www.dimagi.com/
- 22.Fähnrich C, Denecke K, Adeoye O O, Benzler J, Claus H, Kirchner G, Mall S, Richter R, Schapranow M P, Schwarz N, Tom-Aba D, Uflacker M, Poggensee G, Krause G. Surveillance and Outbreak Response Management System (SORMAS) to support the control of the Ebola virus disease outbreak in West Africa. Euro Surveill. 2015 Mar 26;20(12) doi: 10.2807/1560-7917.es2015.20.12.21071. http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=21071 . [DOI] [PubMed] [Google Scholar]
- 23.SORMAS. SORMAS-Project https://github.com/hzi-braunschweig/SORMAS-Project .
- 24.Open Data Kit. 2018. [2018-03-29]. Introducing Formhub, Free Hosted Data Service for ODK Collect https://opendatakit.org/2011/12/introducing-formhub-free-hosted-data-service-for-odk-collect/
- 25.SORMAS. [2018-03-29]. Surveillance Outbreak Response Management & Analysis System (SORMAS): Digital Solutions for mHealth & eHealth Surveillance https://sormasorg.helmholtz-hzi.de/