

Abstract
Background
Halitosis is a common medico social symptom among children.
Aim
To determine the clinical, epidemiological patterns, aetiology and psycho-social issues of halitosis among children in a tertiary hospital in Nigeria.
Methodology
This was a prospective hospital based study of children with complaints of halitosis. The study was carried out in Ear, Nose & throat Department, Ekiti State University Teaching Hospital, Ado Ekiti over a period of two years, (October 2015 to September 2017). Consent was obtained from the parents/guardian. Data was obtained by using pretested interviewer assisted questionnaire.
All the data obtained were collated and analyzed by using SPSS version 16.0.
Ethical clearance was obtained from the ethical committee of the institution.
Results
The prevalence of halitosis in this study was 6.8% and there were 58.5% males and 41.5% females with a male to female ratio of 1.5:1. Their age ranged from 1 year – 18 years with a mean of 9.48 ± 5.84 SD years.
Sources of referral for the otorhinolaryngology, head and neck care were mainly from general practitioners (52.3%) and from pediatricians (24.6%).
Halitosis was noticed by family members in 50.8% and from family friends in 23.1%.
Nasal and throat diseases in 49.2% and 29.2% respectively were the commonest otorhinolaryngology, head and neck disorders that were responsible for halitosis. The major causes were rhinosinusitis in 24.6%, impacted nasal foreign body in 23.1% and adenotonsillar hypertrophy in 18.5%.
Associated disabilities in children and family with halitosis include social withdrawal in 35.4%, low social interaction in 32.3% and depression in 29.2%.
Acute halitosis (<3/12) accounted for 50.8% while chronic halitosis (>3/12) accounted for 49.2%. In all, fifty four (83.1%) of the patients were successfully treated.
Conclusion
Bad breath is a common ear, nose and throat symptom in children it is commonly due to nasal and pharyngeal diseases which are amenable to treatment.
Keywords: Halitosis in children, Rhinitis, Tonsillitis, Impacted foreign bodies
Introduction
Halitosis is an unpleasant universal medico social problem that arises from offensive breath from sufferer to the people in their vicinity1,2. Halitosis greatly affects social communication, health condition, frequent psychological alterations with social and personal isolation 3-5.
This can be classified into three groups6,7. When the halitosis is a real problem that can be easily diagnosed either by organoleptic or by physico-chemical means, it is known as genuine halitosis. If halitosis does not exist, but the patient believes that he has, it is called pseudo-halitosis. While halitophobia occurs after a successful treatment for either genuine halitosis or pseudo-halitosis and the patient still believes that he has halitosis.
Epidemiological studies have shown that halitosis is a universal medico-social problem; affecting 50-65% of the adult population worldwide8,9. It is a common complaint of up to one-third of the general population10. Researchers in Japan found that 15% of adults had halitosis and was more common in the city of Tokyo11 while in China; more than 25% of a study population had halitosis 12. In a Kuwaiti population nearly 25% of the population also had halitosis 13 while in the United States, 43% of people over 60 years had bad breath problems14.
Halitosis mostly arises from a variety of organs in the aero digestive system like the nose, sinuses, tonsils, gastrointestinal tract, lungs, and the oral cavity15. It is estimated that about 10% of cases of halitosis are due to disorders in the ear, nose and throat region16. Tonsilloliths and acute tonsillitis are thought to be a common cause17,18.
Nasal and sinuses infections cause postnasal drip from mucus glands of the nasal and paranasal sinuses19. In chronic sinusitis, 50%–70% of the patients may complain of halitosis20. Impacted foreign bodies in the nasal cavity and congenital sinonasal disorder like cleft palate with secondary bacterial infection may also be the origin of halitosis21. Laryngeal diseases are uncommon causes of halitosis.
Systemic diseases that may cause halitosis include; renal impairment and uncontrolled diabetes mellitus26.
There is paucity of literature on the subject halitosis among ear, nose, throat, head and neck surgical patients in Nigeria. Thu this study is aimed at determining the clinical, epidemiological patterns, disability and aetiology of halitosis among children seen in a tertiary hospital in Nigeria.
Materials and Methods
This is a prospective hospital based study of children with clinical complaints of halitosis. This study was carried out at the Ear, Nose and Throat Department of Ekiti State University Teaching Hospital, Ado Ekiti, Nigeria.
The study was carried out over a period of two years (October 2015 to September 2017). Consent was obtained from the parents/guardians. A total number of 65 patients who gave consent were enrolled into the study.
Data were obtained by using a pretested interviewer assisted questionnaire. General and detailed history about type, frequency, time of day, precipitating, aggravating, relieving factors and extent of halitosis was obtained. History on previous therapies by physicians the resultant psychological stress were documented.
Prior to clinical evaluation, patients were instructed not to eat onion, or perform oral hygiene for at least 4 hours before arrival at the clinic. They were also to refrain from chewing gum, use of candy or mouthwash.
The examination findings of the ear, nose, and throat were documented. Based on the findings, appropriate investigations such as radiology and microbiology were requested and findings were documented.
An organoleptic evaluation was carried out with the distance of operator to patient to detect oral malodor (bad breathe): thus grade 1 is at 10 cm, grade 2 is at 30 cm while grade 3 is at 100cm (Seemann 2001). `
All the data obtained were collated and analyzed by using SPSS version 16.0. The obtained information were expressed by descriptive method and illustrated by using frequency tables, bar chart and pie charts.
Ethical clearance was sought for this study from the ethical committee of the institution.
Results
During the study period a total of 962 patients were seen in the ear, nose and throat department, out of which a total of 65 children had complaints of halitosis giving halitosis prevalence in children of 6.8%. All the paediatric age groups were involved with peak age at preschool age group (1-5 years) as shown in Fig. 1. There were 38 (58.5%) males and 27 (41.5%) females with male/female ratio of 1.5:1. Majority 42 (64.6%) of the patients were urban dwellers while minority 23 (35.4%) were rural dwellers. Assessment of the educational level of their parents showed that, 24 (36.9%) of them were graduates while 19 (29.2%) were secondary school leavers. Parents’ occupations showed that; 29 (44.6%) were civil servants, 11 (16.9%) health workers and 3 (4.6%) were farmers. The sociodemographic features of children with halitosis are shown in Table 1.
Fig. 1. Age group of the children with halitosis.
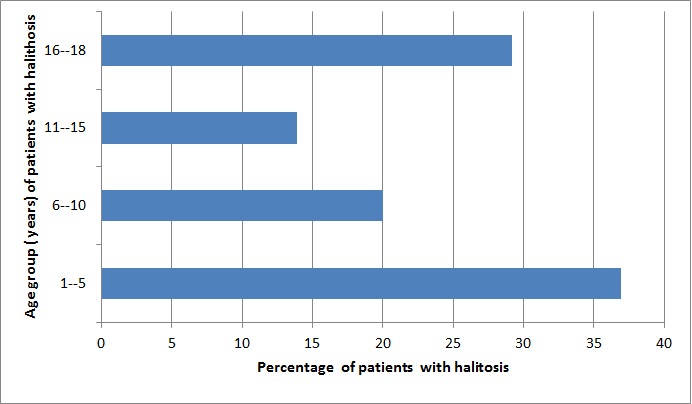
Table 1. Sociodemographic features of the patients.
| Sociodemographic features | Number | Percentage (%) |
| Gender | 58.5 | |
| Male | 38 | 41.5 |
| Female | 27 | |
| Domicile | 64.6 | |
| Urban | 42 | 35.4 |
| Rural | 23 | |
| Religion | 90.8 | |
| Christianity | 59 | 9.2 |
| Islamic | 6 | |
| Parent Education level | 12.3 | |
| None | 8 | 21.5 |
| Primary | 14 | 29.2 |
| Secondary | 19 | 36.9 |
| Tertiary | 24 | |
| Parent Occupation | 16.9 | |
| Health workers | 11 | 10.8 |
| Artisans | 7 | 44.6 |
| Civil servant | 29 | 4.6 |
| Farming | 3 | 13.9 |
| Trading | 9 | 9.2 |
| Others | 6 | 58.5 |
Findings on sources of awareness on halitosis among the studied patients revealed that 33 (50.8%) were by family members and 15 (23.1%) by family friends. Fig. 2 illustrates sources of awareness of halitosis among patients.
Fig. 2. Sources of awareness of halitosis among patients.

Sources of referral for otorhinolaryngology, head and neck review and management were 34 (52.3%) from general practitioners and 16 (24.6%) from paediatricians. Other modes of referrals included parents and dentists; 8 (12.3%) and 4 (6.2%) respectively. This is shown in Fig. 3.
Fig. 3. Sources of referral of halitosis patients.

Nasal diseases 32 (49.2%) were the commonest causes of halitosis. Throat and psychogenic disorders were responsible for 19 (29.2%) and 7 (10.8%) respectively. This is shown in Fig. 4.
Fig. 4. Identifiable sites of diseases causing halitosis among the patients.

The aetiology of halitosis is as summarized in Table 2.
Table 2. Identifiable diseases among children with halitosis.
| Aetiology | Number | Percentage (%) |
| Rhinosinusitis | 16 | 24.6 |
| Nasal foreign body impaction | 15 | 23.1 |
| Tonsillitis | 10 | 15.4 |
| Adenotonsillar hypertrophy | 12 | 18.5 |
| Orodental disorders | 2 | 3.1 |
| Gastrooesophageal reflux disorder | 3 | 4.6 |
| Psychogenic | 7 | 10.8 |
Fig. 5 shows the psycho social issues noted.
Fig. 5. Identifiable psycho-social problems among children with halitosis.

Acute halitosis (<3/12) was seen 33 (50.8%) while chronic halitosis (>3/12) was seen in 32 (49.2%) of the patients. 54 (83.1%) of the patients were satisfied with otorhinolaryngological treatment while 11 (16.9%) were unsatisfied.
Discussion
The prevalence of halitosis in this study was 6.8%. Studies from developed countries have reported a higher prevalence27,28. The low prevalence in this study was due to low level awareness of the significance of halitosis and management in developing countries.
This study revealed male preponderance over female. Reports from other study revealed similar finding29. While a previous study revealed equal sex proportion 30. More than half of halitosis patients were urban dwellers this may be due to easier accessibility to the patients. Geographical location barriers to access surgical services are a major challenge facing health care systems31.
Prevalence of halitosis is more common in the preschool age group (1-5years) in this study. This finding was contrary to findings in other studies that showed peak prevalence among the elderly32. In this study, there was a gradual decrease in prevalence of halitosis with age and final peak at 16-18 years.
General, few patients were self-conscious of bad breath. Majority of the sufferers have no idea of the halitosis unless from the conscious indication by other people or conscious by presumptions from the attitude of others. In this study less than half of the patients were self-aware of their halitosis. Majority of the studied patients were aware of bad breath indications by friends and family members.
Rhinosinusitis and nasal foreign body impaction constituted about half of the aetiology of nasal and sinuses diseases. Unlateral nasal discharge is pointer to impacted nasal foreign body. Tonsillitis and adenotonsillar hypertrophy were the commonest throat disorders that was responsible for halitosis in this study. Other studies have reported that tonsillitis is the commonest cause of halitosis 33-35. However, it is important to differentiate bad taste from bad breath. Oro-dental pathology is the least cause in this study. This finding is contrary to other study 36. This may be due to fact that these were mainly patients referred to the otorhinolaryngology clinic.
Social withdrawal, low social interaction and depression were the commonest psycho social effects associated with halitosis in this study. Halitosis inhibits the sufferer leading to social withdrawal; irritability and anxiety were commoner among the older children. They are afraid of attending socio-gathering (sociophobia) because of bad breathe emanating from them.
Patients with acute halitosis (when <3 months) were more than those with chronic halitosis (when >3 months). Parent of children with acute halitosis tend to look for early medical intervention. After diagnosis, treatment offered to the patients range from surgical, medical or referral to others specialist for multidisciplinary approach. Otorhinolaryngology treatment outcome was satisfactory in the majority the children and unsatisfactory to the minority of the patients in this study. This is comparable to treatment outcome in other reports37. Contrasted outcome was recorded in other study38.
Limitations of this study include lack of instruments for assessment of exhaled air and inability to assess quality of life issues with validated questionnaires.
Conclusions
Bad breath is a common ear, nose and throat symptom in children it is commonly due to nasal and pharyngeal diseases which are amenable to treatment.
References
- 1.Eldarrat A, Alkhabuli J, Malik A. The Prevalence of Self-Reported Halitosis and Oral Hygiene Practices among Libyan Students and Office Workers. . Libyan Journal of Medicine. 2008;3(4):170–176. doi: 10.4176/080527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Elias MS, Ferriani MDGC. Historical and social aspects of halitosis. Revista latino-americana de enfermagem. 2006;14(5):821–823. doi: 10.1590/s0104-11692006000500026. [DOI] [PubMed] [Google Scholar]
- 3.CE Kazor, Mitchell PM, Lee AM, Stokes LN, Loesche WJ, Dewhirst FE, Paster BJ. Diversity of Bacterial Populations on the Tongue Dorsa of Patients with Halitosis and Healthy Patients. . Journal of clinical microbiology. 2003;41(2):558–563. doi: 10.1128/JCM.41.2.558-563.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chomyszyn-Gajewska M. Contemporary views on etiology and pathogenesis of halitosis. Przegl Lek. 2011;69:1293–1296. [PubMed] [Google Scholar]
- 5.Seemann R, Conceicao MD, Filippi A, Greenman J, Lenton P, Nachnani S. Halitosis management by the general dental practitioner - results of an international consensus workshop. J Breath Res. 2014;8 doi: 10.1088/1752-7155/8/1/017101. [DOI] [PubMed] [Google Scholar]
- 6.ADA Council. Oral malodor. J Am Dent Assoc. 2003;134(2):209–214. doi: 10.14219/jada.archive.2003.0135. [DOI] [PubMed] [Google Scholar]
- 7.Nalçaci R, Dülgergil T, Oba AA, Gelgör IE. Prevalence of breath malodour in 11-year-old children living in Middle Anatolia, Turkey. Community Dent Health. 2008;25:173–177. [PubMed] [Google Scholar]
- 8.Armstrong BL, Sensat ML, Stoltenberg JL. Halitosis: a review of current literature. . American Dental Hygienists Association. 2010;84(2):65–67. [PubMed] [Google Scholar]
- 9.O'Dowd LK, Durham J, McCracken GI, Preshaw PM. Patients' experiences of the impact of periodontal disease. J Clin Periodontol. 2010;37:334–339. doi: 10.1111/j.1600-051X.2010.01545.x. [DOI] [PubMed] [Google Scholar]
- 10.Nalini Saini, Puneet Ajwani, Kulmeet Kaur, Amandeep Kumar. Oral Malodor: A Common Oral Problem. . J Bioengineer & Biomedical Sci . 2011;2(1) [Google Scholar]
- 11.Saito H, Kawaguchi Y. Halitosis prevention campaign: a report of oral health promotion activities in Japan. Int Dent J. . 2002;52(Suppl 3):197–200. doi: 10.1002/j.1875-595x.2002.tb00924.x. [DOI] [PubMed] [Google Scholar]
- 12.Liu XN, Shinada K, Chen XC. Oral malodour-related parameters in the Chinese general population. J Clin Periodontol. 2006;33(1):27–31. doi: 10.1111/j.1600-051X.2005.00862.x. [DOI] [PubMed] [Google Scholar]
- 13.Al-Ansari JM, Boodai H, Al-Sumait N. Factors associated with the self-reported halitosis in Kuwaiti patients. J Dent. 2006;34(7):444–449. doi: 10.1016/j.jdent.2005.10.002. [DOI] [PubMed] [Google Scholar]
- 14.Bornstein MM, Kislig K, Hoti BB. Prevalence of halitosis in the population of the city of Bern, Switzerland: a study comparing self-reported and clinical data. Eur J Oral Sci. 2009;117(3):261–267. doi: 10.1111/j.1600-0722.2009.00630.x. [DOI] [PubMed] [Google Scholar]
- 15.Umeizudike KA, Oyetola OE, Ayanbadejo PO, Alade GO, Ameh PO. Prevalence of self-reported halitosis and associated factors among dental patients attending a tertiary hospital in Nigeria. Sahel Med J. 2017;19:150–154. [Google Scholar]
- 16.van den Broek AM, Feenstra L, de Baat C. A review of the current literature on aetiology and measurement methods of halitosis. J Dent. 2007;35(8):627–635. doi: 10.1016/j.jdent.2007.04.009. [DOI] [PubMed] [Google Scholar]
- 17.Ansai T, Takehara T. Tonsilloliths as a halitosis-inducing factor. Br Dent J. 2005;198(5):263–264. doi: 10.1038/sj.bdj.4812116. [DOI] [PubMed] [Google Scholar]
- 18.Mulwafu W, Fagan JJ, Isaacs S. Adult tonsillectomy—are long waiting lists putting patients at risk. S Afr J Surg. 2006;44(2):66–68. [PubMed] [Google Scholar]
- 19.Amir E, Shimonov R, Rosenberg M. Halitosis in children. . J Pediatr. 1999;134(4):338–343. doi: 10.1016/s0022-3476(99)70460-9. [DOI] [PubMed] [Google Scholar]
- 20.Lanza DC. Diagnosis of chronic rhinosinusitis. Ann Otol Rhinol Laryngol. 2004;193(Suppl 1):10–14. doi: 10.1177/00034894041130s504. [DOI] [PubMed] [Google Scholar]
- 21.Monteiro-Amado F, Chinellato LE, de Rezende ML. Evaluation of oral and nasal halitosis parameters in patients with repaired cleft lip and/or palate. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(6):682–687. doi: 10.1016/j.tripleo.2005.03.019. [DOI] [PubMed] [Google Scholar]
- 22.Hughesa FJ, McNabb R. Oral malodour - a review. . Archives of oral biology . 2008;53(Suppl.1):s1–s7. doi: 10.1016/S0003-9969(08)70002-5. [DOI] [PubMed] [Google Scholar]
- 23.Porter SR, Scully C. Oral malodour (halitosis). . BMJ. 2006;333(7569):632–635. doi: 10.1136/bmj.38954.631968.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yokoyama S, Ohnuki M, Shinada K, Ueno M, Wright FA, Kawaguchi Y. Oral malodor and related factors in Japanese senior high school students. . Journal of School Health. 2010;80(7):346–352. doi: 10.1111/j.1746-1561.2010.00512.x. [DOI] [PubMed] [Google Scholar]
- 25.Bornstein MM, Kislig K, Hoti BB, Seemann R, Lussi A. Prevalence of halitosis in the population of the city of Bern, Switzerland: a study comparing self-reported and clinical data. European Journal of Oral Sciences. 2009;117(3):261–267. doi: 10.1111/j.1600-0722.2009.00630.x. [DOI] [PubMed] [Google Scholar]
- 26.Takehara S, Yanagishita M, PodymaInoue KA, Ueno M, Shinada K, Kawaguchi Y. Relationship between Oral Malodor and Glycosylated Salivary Proteins. J Med Dent Sci. 2010;57:25–33. [PubMed] [Google Scholar]
- 27.Lee SS, Zhang W, Li Y. Halitosis update: A review of causes, diagnoses, and treatments. . J Calif Dent Assoc. 2007;35:258–260. [PubMed] [Google Scholar]
- 28.Frexinos J, Denis P, Allemand H, Allouche S, Los F, Bonnelye G. Descriptive study of digestive functional symptoms in the French general population. Gastroenterol Clin Biol. 1998;22:785–791. [PubMed] [Google Scholar]
- 29.Talebian A, Tazhibi M, Semyari H, Iranpoor R, Talebian H, Oreizy SM, Khansari M. Clinical evaluation of 222 Iranian patients with halitosis. . J Breath Res. 2008;2 doi: 10.1088/1752-7155/2/1/017015. [DOI] [PubMed] [Google Scholar]
- 30.Akpata O, Omoregie OF, Ibhawoh LO. The role of dentists as a stop-gap in the initial management of patients with delusional halitosis. West Afr J Med. 2013;32:291–296. [PubMed] [Google Scholar]
- 31.Adegbiji WA, Aremu SK, Lasisi AO. Patients Barrier to Ear, Nose and Throat Surgical Care in Nigeria. American Scientific Research Journal for Engineering, Technology, and Sciences (ASRJETS) . 2017;32(1):96–104. [Google Scholar]
- 32.Arowojulo MO, Dosumu EB. Halitosis (Fetor oris) in patients seen at the periodontology clinic of the University College Hospital, Ibadan - a subjective evaluation. Niger Postgrad Med J. 2004;11(3):221–224. [PubMed] [Google Scholar]
- 33.Ansai T, Takehara T. Tonsilloliths as a halitosis-inducing factor. Br Dent J. 2005;198(5):263–264. doi: 10.1038/sj.bdj.4812116. [DOI] [PubMed] [Google Scholar]
- 34.Mulwafu W, Fagan JJ, Isaacs S. Adult tonsillectomy—are long waiting lists putting patients at risk. S Afr J Surg. 2006;44(2):66–68. [PubMed] [Google Scholar]
- 35.Tsuneishi M, Yamamoto T, Kokegucji S. Composition of the bacterial flora in tonsilloliths. Microbes Infect. 2006;8(9/10):2384–2389. doi: 10.1016/j.micinf.2006.04.023. [DOI] [PubMed] [Google Scholar]
- 36.Aylıkcı BU, Çolak H. Halitosis: From diagnosis to management. J Nat Sci Biol Med. 2013 Jan-Jun;4(1):14–23. doi: 10.4103/0976-9668.107255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Filippi A, Müller N. Real and psychological halitosis--findings, diagnoses and outcomes of a halitosis clinic. Schweiz Monatsschr Zahnmed. 2006;116(2):129–135. [PubMed] [Google Scholar]
- 38.Akaji EA, Folaranmi N, Ashiwaju O. Halitosis: A review of the literature on its prevalence, impact and control. Oral Health Prev Dent. 2014;12:297–304. doi: 10.3290/j.ohpd.a33135. [DOI] [PubMed] [Google Scholar]