

Abstract
Background:
Aphasia is a neurogenic communication disorder with significant deficits in various domains of language and communication. One such type of aphasia, which impacts the quality of life significantly is Broca's aphasia, where the individual is aware of the communication difficulty.
Objective:
To compare the Quality of Communication Life (QoCL) between individuals with Broca's aphasia and normal individuals.
Methods:
The first phase of the study translated and validated QCL scale in Tamil. The second phase involved administration of the Tamil QCL scale on 12 individuals with Broca's aphasia and 12 age matched normal adults. The marked responses were analysed on a visual analogue scale independently.
Statistical Analysis:
Three domains of QoCL were compared between the two groups using Mann–Whitney U-test.
Results:
The QoCL scores across three domains were observed to be lower in individuals with Broca's aphasia, when compared to normal adults. Individuals with Broca's aphasia expressed greater challenges in socialization/activities domain of QoCL than confidence/self-concept and roles and responsibilities domains.
Conclusions:
Information obtained on self-reported QCL scale in familiar or native language will facilitate in planning client-oriented management of aphasia.
Keywords: Broca's aphasia, quality of communication life, Tamil
INTRODUCTION
Communication is a dynamic process in which people attempt to share their internal states with other people through the use of symbols. In human communication, symbol is an expression that stands for or represents something.[1] The ability to communicate is of fundamental importance to psychosocial adjustment in the society.[2] However, society has overlooked the importance of communication due to predominant focus in other aspects such as body, health and functioning.[3] Communication difficulty may result in social isolation, challenges with interpersonal relationships, mental and emotional changes, difficulty or inability to return to work and corresponding lack of independence.[4] Since communication is an essential aspect of human existence, losing the ability to execute it effectively affects the quality of life (QoL), as in individuals with communication disorders.[5] QoL is broadly defined as an individual's subjective feeling of well-being as it relates to emotional state, physical functioning, psychosocial attitudes or a combination therein.[6] One such disorder where the communication difficulty has a significant impact on QoL is in individuals with neurogenic disorder such as aphasia.[3] However, the extent to which this impact is felt across various domains such as socialization, physical abilities, emotional health and communication remains unclear.[7] Moreover, exactly how QoL is influenced by linguistic impairments per se is far from obvious.[8] QoL measures that are used in individuals with aphasia effectively reflect the needs of these individuals.[9]
Individuals with Broca's aphasia are usually aware of their difficulty in communication, thereby expressing frustration when they fail to communicate and this in turn impairs their QoCL.[10,11] Current trends in assessment of aphasia also involve estimation of QoCL. Studies on QoCL in individuals with aphasia have been explored in the western population. The results obtained from these studies may not be generalized to the Indian population because of sociocultural and linguistic differences. There is a dearth of available QoCL measures in individuals with aphasia in India, thus it becomes necessary to carry out a study in these individuals to ascertain the QoCL. There is a steady rise in the prevalence of aphasia from several thousands to a few millions in India.[12,13] Perception of the QoCL is highly individual specific, be it individuals with Broca's aphasia or normal individuals. However, a few commonalities may be identified amongst the groups. The domain specific information obtained through comparison between the aphasic and normal individual groups would help the clinician to design effective intervention programs in management of aphasia. With this background, the current study aimed at comparing Quality of Communication Life (QoCL) in individuals with Broca's aphasia and normal individuals using Quality of Communication Life Scale (QCL).
METHODS
Participants
The study included 24 adults (20 males and 4 females) categorized under clinical group comprising of individuals with Broca's aphasia (n = 12) and nonclinical group comprising of normal individuals (n = 12). The age of these individuals ranged from 28 to 57 years (M = 43.08; standard deviation [SD] =6.30). Participants in the clinical group were identified from various hospitals in Chennai. These participants were native speakers of Tamil.
Clinical group (individuals with Broca's aphasia)
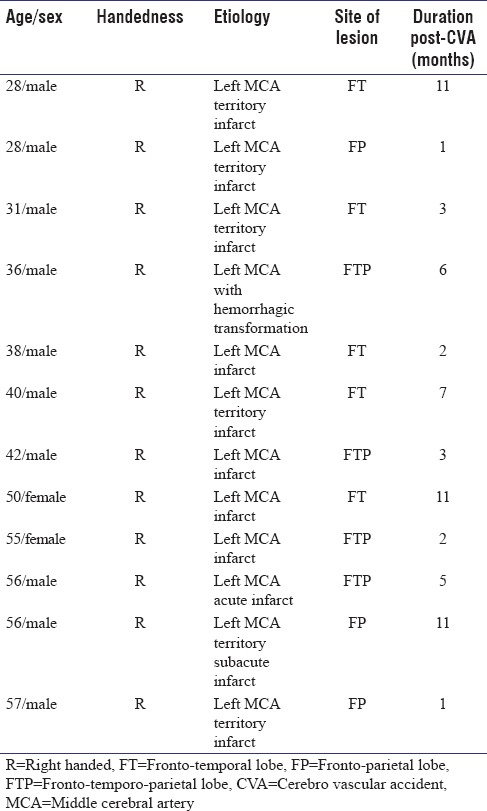
These individuals had a minimum of 8 years of formal education and were able to read Tamil. Individuals with other associated neurogenic, cognitive or sensory issues were not included in the study. All the participants had a single episode of a cerebro vascular accident (CVA) with left middle cerebral artery territory infarct and a post onset period of 1 year. Details about handedness, etiology and site of lesion are represented in Table 1. Diagnosis of type of aphasia was confirmed using Western Aphasia Battery.[14] These individuals had one of the upper extremities (right or left) sufficiently intact to point, gesture or write, able to read (silent/loud) simple sentences in Tamil.
Table 1.
Demographic data, etiology, site of lesion and duration postcerebro vascular accident (months) of the individuals with Broca’s aphasia
Nonclinical group (normal adults)
Participants in nonclinical group, i.e., normal individuals were matched for age, gender, marital status and employment level with the clinical group. Individuals with obvious sensory, motor, cognitive and neurogenic concerns were not included in the study.
Procedure
Quality of Communication Life (QoCL) was estimated using translated Tamil version of American Speech Language Hearing Association's Quality of Communication Life Scale (QCL).[15] This questionnaire consists of 18 statements under three domains (Socialization/activities, Confidence/self-concept and Roles and responsibilities). First 17 statements focus on Quality of Communication Life (QoCL) and the 18th statement relates to overall QoL.
The current study was carried out in two phases,
Phase I: Translation and validation of QCL
Phase II: Administration of QCL.
Phase I: Translation and validation of QCL
QCL was translated to Tamil by a linguist, with permission from American Speech-Language-Hearing Association (ASHA). Further, two qualified speech language pathologists (SLPs) were involved in the face validity of QCL. The statements were modified according to the suggestions provided by the SLPs. Reverse translation was carried out by a different linguist who is also a native speaker of Tamil to ensure the accuracy of the translated scale.
Phase II: Administration of QCL
Informed consent was obtained from the participant/caregiver prior to the study. Quality of Communication Life (QCL) scale was administered only when the participants' were stable to respond. Information such as age, marital status, education, duration post CVA, site of lesion, motor impairment, ambulatory status, surgical details, intake of medications, speech therapy, other therapies, living arrangement and employment status were also obtained.
Administration of the scale was carried out in a relatively quiet room at the participant's home or hospital. Prior to administration of the scale, participants were instructed to read the statement in practice item. They were also oriented about marking the best suitable response based on the perception on the vertical visual analogue scale. Participants were instructed to skip statement(s) if not applicable to them. Each participant took about 15–20 min to complete the entire scale. Assistance was provided by the investigator when there was difficulty in reading or marking on the scale.
Scoring
Each statement in the QCL has a vertically placed visual analogue scale, consisting of five equally spaced referents. These were corresponding to a numerical value, where 1 indicates a lowest score and 5 indicates a highest score. Higher scores indicate better QoCL. A simple line drawing representing the extreme attributes of each statement was presented at either extremity of the visual analogue scale. When the response was marked in between any two corresponding referents it was rounded up to the next higher referent. Only the statements which were answered by the participants were scored in a scoring sheet. The QoCL scores for each participant were calculated as follows:

Similarly, the scores for each item within QoCL domains were added for obtaining domain specific scores. Scores were computed by the investigator and subjected to statistical analysis.
Data analysis
The scores of Quality of Communication Life (QoCL) were analyzed and compared between the clinical (individuals with Broca's aphasia) and nonclinical (normal individuals) groups. Mean and SD were calculated for the scored responses. Mann–Whitney U-test was used to determine the differences in QoCL scores between the two groups.
RESULTS
Figure 1 and Table 2 indicate lower QoCL scores in individuals with Broca's aphasia (clinical group) in all the three domains, viz., socialisation/activities, confidence/self-concept, roles and responsibilities, when compared to normal individuals (non-clinical group). Further, it was observed that among the three domains, Socialization/activities domain had a greater mean difference (2.08), followed by roles and responsibilities domain (1.79); and confidence and self-concept domain, which has the least difference (1.06). The result of Mann–Whitney U-test revealed that the QoCL of all the three domains is significantly different between the groups at P < 0.05 level.
Figure 1.
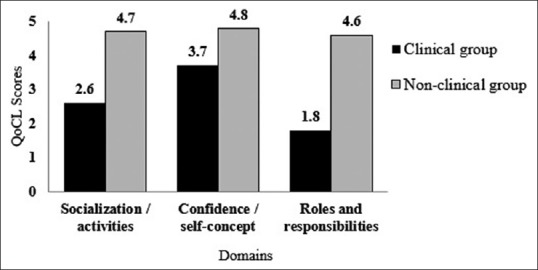
Quality of communication life domain scores of clinical group (individuals with Broca's aphasia) and non clinical group (normal individuals)
Table 2.
Mean, standard deviation, mean difference and P value of the three domains of Quality of Communication Life Scale in clinical and nonclinical group

Socialization/activities
Seven statements in this domain measured the impact of difficulty in communication on activities pertaining to socialization at various environments (e.g., communication in work environment, home, etc.). It is evident from the Table 2 that, the mean QoCL score was higher in normal individuals (4.72) than in individuals with Broca's aphasia (2.64) indicating the fact that normal individuals perceived their QoCL in socialization/activities domain to be significantly better than individuals with aphasia. The results of Mann–Whitney U-test also highlighted significant difference in the QoCL scores (P < 0.05) between the groups.
Confidence/self-concept
Six statements such as confidence in communicating, voicing opinion, etc., in this domain measured respondents' perception of confidence/self-concept. The mean QoCL score (4.79) in normal individuals and mean score (3.73) in individuals with Broca's aphasia was significantly different (P < 0.05) which emphasized the notion that normal individuals perceived their QoCL to be significantly higher compared to the individuals with aphasia.
Roles and responsibilities
Four statements relating to family roles and household responsibilities in this domain measured individual roles and responsibilities. The mean QoCL scores of normal individuals (4.64) was higher than individuals with aphasia (2.85). Mann–Whitney U-test revealed significant difference (P < 0.05) in the QoCL scores between the groups.
DISCUSSION
Rehabilitation of individuals with aphasia is focussing predominantly on social participation, health and wellness.[16,17] In addition to the medical model, clinical and research advances in speech language pathology focus on systemic model of understanding disability.[18] With this background, the current study aimed at comparing Quality of Communication Life (QoCL) in individuals with Broca's aphasia. Considering language and cultural difference, QoCL was translated and adapted to Tamil with permission from American Speech and Hearing Association. Eighteen statements on Tamil version of QoCL was scored on a visual analog scale by 12 individuals with Broca's Aphasia and 12 normal individuals. Comparison of the results indicated that overall scores and domain specific scores in individuals with Broca's aphasia was lower than the scores obtained by normal individuals. Further, individuals with aphasia had lowest score in socialization/activities domain when compared to other domains. It may be inferred that these individuals restricted themselves from involving in social activities due to impairments related to motor and communication skills. Fotiadou et al.[19] reported similar findings that, stroke and aphasia affect a person's ability to maintain healthy social relationships negatively, both within family and also with friends and the wider network. Few other researchers such as Hilari and Northcott;[20] and Parr[21] observed that social activities such as social companionship and informational support is affected in chronic aphasia which inturn impacts the QoL. Research also reports that individuals with aphasia communicated with fewer friends and had smaller social networks[22] impacting the social interactions and life experience.[23] Decrease in the participation in activities related to domestic life was also observed, as in interpersonal interactions and relationships, education and employment, community, civic and social life. Interpersonal interactions and relationships tend to change after the onset of aphasia with shifts in contacts from friends to professionals, shifts in roles as partner, family member, parent, friend and citizen. Participation in different aspects of life is affected in individuals with aphasia.[23] Wallace[24] reported that individuals with stroke and aphasia have participation restrictions related to communication.
Lower scores in confidence/self-concept domain could be due to the difficulty in communication in individuals with aphasia which indirectly decreases the confidence levels. Babbitt and Cherney[25] reported that communication confidence is a construct that has not been explored in the aphasia literature. With respect to the domain roles and responsibilities, the results revealed that individuals in nonclinical group perceived their QoCL to be significantly higher compared to the clinical group. The reason for this could be due to the perceived difficulty in individual's role in the family, staying in touch with family and friends, making their own decisions and household responsibilities such as cooking, shopping, home repairs. The results are in accordance with the study conducted by Bose et al.[2] who confirmed that normal individuals tend to exhibit higher QoCL score in roles and responsibilities domain compared to the individuals with aphasia. Such information along with routine assessment and intervention protocols followed by professionals will augment better planning of intervention for individuals with aphasia.[26]
CONCLUSIONS
This study validates the need for considering self-reported information related to the impact of communication difficulty in individuals with aphasia. Such information regarding the extent of impact of communication difficulty on the QoCL is best expressed in native and familiar language. Thus, a multilingual and multicultural country like India requires language specific self-reported scales for facilitating appropriate client-specific intervention plans. This information can also be used to gauge the prognosis and progress of communication intervention programmes.
Financial support and sponsorship
This study was self-funded.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.McDaniel ER, Samovar LA, Porter RE. Intercultural Communication: A Reader. Boston: Lyn Uhl; 2011. [Google Scholar]
- 2.Bose A, McHugh T, Schollenberger H, Buchanan L. Measuring quality of life in aphasia: Results from two scales. Aphasiology. 2009;23:797–808. [Google Scholar]
- 3.Cruice M, Worrall L, Hickson L, Murison R. Finding a focus for quality of life with aphasia: Social and emotional health and psychological well-being. Aphasiology. 2003;17:333–53. [Google Scholar]
- 4.Ross KB, Wertz RT. Quality of life with and without aphasia. Aphasiology. 2003;17:355–64. [Google Scholar]
- 5.Kelly RJ, Atcherson SR. Quality of life for individuals with hearing impairment who have not consulted for services and their significant others: Same- and different-sex couples. J Commun Disord. 2011;44:336–44. doi: 10.1016/j.jcomdis.2011.01.004. [DOI] [PubMed] [Google Scholar]
- 6.Aaronson NK. Quality of life: What is it? How should it be measured. Oncology (Williston Park) 1988;2:69–76, 64. [PubMed] [Google Scholar]
- 7.Worrall LE, Holland AL. Editorial: Quality of life in aphasia. Aphasiology. 2003;17:329–32. [Google Scholar]
- 8.Engell RJ, Hutter BO, Willmes K, Huber W. Quality of life in aphasia: Validation of a pictorial self-rating procedure. Aphasiology. 2003;17:383–96. [Google Scholar]
- 9.Aprile I, Piazzini DB, Bertolini C, Caliandro P, Pazzaglia C, Tonali P, et al. Predictive variables on disability and quality of life in stroke outpatients undergoing rehabilitation. Neurol Sci. 2006;27:40–6. doi: 10.1007/s10072-006-0563-5. [DOI] [PubMed] [Google Scholar]
- 10.Ross KB, Wertz RT. Relationship between language-based disability and quality of life in chronically aphasic adults. Aphasiology. 2002;16:791–800. [Google Scholar]
- 11.Murdoch BE. Acquired Speech and Language Disorders: A Neuroanatomical and Functional Neurological Approach. Singapore: Chapman and Hall; 2010. [Google Scholar]
- 12.Mitra IH, Krishnan G. Adaptation and validation of stroke-aphasia quality of life (SAQOL-39) scale to Hindi. Ann Indian Acad Neurol. 2015;18:29–32. doi: 10.4103/0972-2327.144276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Raju R, Krishnan G. Adaptation and validation of stroke-aphasia quality of life (SAQOL-39) scale to Malayalam. Ann Indian Acad Neurol. 2015;18:441–4. doi: 10.4103/0972-2327.160068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kertesz A. Western Aphasia Battery. New York: Grune and Stratton; 1982. [Google Scholar]
- 15.Paul DR, Frattali CM, Holland AL, Thompson CK, Caperton CJ, Slater SC. Quality of Communication Life Scale. Rockville, MD: American Speech-Language Hearing Association; 2004. [Google Scholar]
- 16.Spaccavento S, Craca A, Del Prete M, Falcone R, Colucci A, Di Palma A, et al. Quality of life measurement and outcome in aphasia. Neuropsychiatr Dis Treat. 2014;10:27–37. doi: 10.2147/NDT.S52357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Worrall L, Hickson L. Communication Disability in Aging: From Prevention to Intervention. USA: Delmar Publishers; 2003. [Google Scholar]
- 18.World Health Organization. Towards a Common Language for Functioning, Disability, and Health: The International Classification of Functioning, Disability and Health. 2002. [Last accessed on 2017 Nov 20]. Available from: http://www3.who.int/icf/intros/ICF-Eng-Intro.pdf .
- 19.Fotiadou D, Northcott S, Chatzidaki A, Hilari K. Aphasia blog talk: How does stroke and aphasia affect a person's social relationships? Aphasiology. 2014;28:1281–300. [Google Scholar]
- 20.Hilari K, Northcott S. Social support in people with chronic aphasia. Aphasiology. 2006;20:17–36. [Google Scholar]
- 21.Parr S. Living with severe aphasia: Tracking social exclusion. Aphasiology. 2007;21:98–123. [Google Scholar]
- 22.Davidson B, Howe T, Worrall L, Hickson L, Togher L. Social participation for older people with aphasia: The impact of communication disability on friendships. Top Stroke Rehabil. 2008;15:325–40. doi: 10.1310/tsr1504-325. [DOI] [PubMed] [Google Scholar]
- 23.Dalemans RJ, De Witte LP, Van den Heuvel D, Wade DT. A description of social participation in working-age people with aphasia: A review of literature. Aphasiology. 2008;22:1071–91. [Google Scholar]
- 24.Wallace GL. Profile of life participation after stroke and aphasia. Top Stroke Rehabil. 2010;17:432–50. doi: 10.1310/tsr1706-432. [DOI] [PubMed] [Google Scholar]
- 25.Babbitt EM, Cherney LR. Communication confidence in persons with aphasia. Top Stroke Rehabil. 2010;17:214–23. doi: 10.1310/tsr1703-214. [DOI] [PubMed] [Google Scholar]
- 26.Morrow-Odom KL, Moser DC, Neils-Strunjas J. Current practices in the assessment of quality of life in individuals with aphasia. Clin Arch Commun Disord. 2017;2:185–95. [Google Scholar]