

Abstract
Dry eye and dry mouth Symptoms are each reported by up to 30% of persons more than 65 years of age, particularly in women. Medication side effects are the most common contributing factors. The evaluation of these Symptoms requires measures of ocular and oral dryness. Sjögren Syndrome is the prototypic disease associated with dryness of the eyes and mouth and predominantly affects women in their perimenopausal and postmenopausal years. In addition to topical treatment of the mucosal dryness, patients with Sjögren Syndrome may require treatment with systemic immunomodulatory and immunosuppressive agents to manage a variety of extraglandular manifestations.
Keywords: Sjögren Syndrome, Dry eye, Aging, Salivary hypofunction, Xerostomia
Introduction
Henrik Sjögren used the term “sicca syndrome” to describe the disease that he studied extensively during his lifetime, beginning with a comprehensive analysis of 19 patients that he completed in 1933 as an ophthalmologist in training [1, 2]. The characteristic phenotypic features included severe ocular and oral mucosal dryness afflicting most often postmenopausal women, many of whom had associated rheumatoid arthritis. Sicca syndrome and “Sjögren syndrome” became synonymous. However, we now know that most older adults with sicca syndrome (i.e. oral and ocular mucosal dryness) do not have Sjögren syndrome. As currently defined, Sjögren syndrome is a systemic rheumatic disease with autoimmune-induced inflammation of the lacrimal and salivary glands, resulting in impaired tear and saliva production. The distinction between these two entities is important, since identification of those patients with an autoimmune basis for their sicca manifestations is the first step in deciding whether therapies directed at the immune system might be beneficial and avoiding such therapies and their attendant risks in patients with non-autoimmune sicca syndrome.
This article reviews the clinical manifestations, differential diagnosis, and medical evaluation of older adults with dry eyes and mouth, as well as the approach to the diagnosis and management of Sjögren syndrome.
Epidemiology of sicca
Symptoms of dryness of the eyes, mouth, and vagina (in women) increase with age and reach up to 30% in persons more than the age of 65 years, particularly in women [3-9]. Objective evidence of diminished tear or saliva production is much less frequent [6, 7, 10], indicating the weak association between dryness symptoms and objective measures. Both dry eye and dry mouth symptoms were reported by 4.4% of an elderly population, age 65-84 years, in Salisbury, Maryland [11] and had no association with markers of systemic autoimmunity. The prevalence of Sjögren syndrome in this population was only 0.04% [12].
Dry eye
Dry eye manifests most often with ocular irritation, including burning, stinging, soreness, and a foreign body sensation. The symptoms are aggravated by exposure to low humidity, wind, or air drafts, as well as prolonged visual attention, including reading. Less frequent symptoms include blurred vision, excess tearing, and blepharospasm.
Dry eye is generally caused by diminished tear production or by excessive tear evaporation [13] (Box 1). The former is most often caused by lacrimal gland disease but can result from lacrimal gland duct obstruction or reflex hyposecretion related to corneal sensory loss. Excessive evaporation from meibomian gland dysfunction and other forms of blepharitis is more common. Other causes of dryness include incomplete lid closure during sleep, allergic conjunctivitis, and trachoma.
Box 1. Common causes of dry eye.
| Aqueous Tear Deficiency | Evaporative Tear Deficiency |
|---|---|
|
|
Abbreviations: AIDS, acquired immunodeficiency syndrome; Ig, immunoglobulin.
The assessment of dry eye requires multiple tests (Box 2). The Schirmer test measures tear production [14] and can be reliably performed by a rheumatologist in a clinic setting. A sterile rectangular strip of filter paper, rounded and notched at the proximal end, is folded over the lower eyelid at the midpoint between the middle and lateral fornix of each eye. The patient is then asked to close the eyes gently during the 5-minute duration of the test. The extent of tear wicking or wetting is recorded in millimeters. The Schirmer test can be performed with or without anesthesia to measure basal and reflex tear secretion, respectively. Without anesthesia, a Schirmer test result of less than 5 mm in at least one eye is considered abnormal. This test is imperfect in the elderly, because the degree of wetting declines with age. In 2 population-based surveys of elderly individuals (65 years or older), the prevalence of an abnormal Schirmer test ranged from 12% to 58% [4, 6].
Box 2. Tests used to assess dry eye disease.
Data from van Bijsterveld OP. Diagnostic tests in the sicca syndrome. Arch Ophthalmol 1969;82(1):10–4; and Whitcher JP, Shiboski CH, Shiboski SC, et al. A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjögren's syndrome International Registry. Am J Ophthalmol 2010;149(3):405–15.
| Test | Abnormal Value | Significance of Abnormal Test |
|---|---|---|
| Schirmer | <5 mm/5 minute in either eye | Inadequate tear production |
| Ocular surface staining | Score ≥4 (von Bijsterveld) [15] Score ≥3 (SICCA) [17] |
Damage to the ocular surface |
| Tear break up time | <10 seconds | Poor tear film stability, as seen in meibomian gland dysfunction |
| Tear osmolarity | ≥308 mOsm/L in either eye | Excessive tear evaporation, lacrimal gland disease, or ocular surface inflammation |
Abbreviation: SICCA, Sjögren's International Collaborative Clinical Alliance.
Ocular surface staining with vital dyes allows slit lamp visualization of devitalized conjunctival cells and corneal epithelial defects. It is more sensitive than the Schirmer test for detecting dry eye. Lissamine green is most commonly used to stain the conjunctiva and fluorescein the cornea. The extent of ocular surface staining is a measure of dryness-induced ocular surface damage, is one of the classification criteria for SS, and can be scored using methods described by van Bijsterveld [15] and by the Sjögren International Collaborative Clinical Alliance (SICCA) [16, 17].
The tear breakup time is used to assess the stability of the tear film [18] and is typically abnormal in meibomian gland dysfunction. Tear osmolarity measurement [19, 20] is the best for predicting dry eye severity [20].
Xerostomia and salivary hypofunction
Symptoms of dry mouth, termed xerostomia, include burning, dry lips, alteration of taste, and a sense of having an inadequate amount of saliva. There also may be difficulty speaking, swallowing, and wearing dentures. The need to sip water to swallow dry food is an important marker of reduced salivary function [21]. Halitosis, painful tongue fissures, mucosal ulcers, and pain with ingestion of spicy or acidic foods may stem from candidal overgrowth on the oral mucosa. The relation between salivation and xerostomia is complex. Dawes [22] showed that healthy patients report dry mouth symptoms when their baseline salivary flow is reduced by 50%, even if the residual salivary flow level remains within the broad range of normal.
Saliva is produced by the major (parotid, submandibular, sublingual) and myriad submucosal minor salivary glands. The parotid glands only produce saliva on gustatory or olfactory stimulation. Saliva is continually secreted by the sublingual, submandibular, and minor salivary glands. This basal secretion is crucial for maintaining oral health.
Both unstimulated and stimulated salivary flow rates are measured. Saliva that pools in the mouth without stimulation can be collected for 5 to 15 minutes, providing a measure of so-called whole saliva production in a clinic setting (Box 3). It is considered the most relevant measure of oral health. Stimulated whole salivary flow rates can be measured with the patient chewing gum, preweighed gauze, or paraffin (e.g. Parafilm™) and are not generally affected by medication use. With special research techniques, stimulated (e.g., with lemon juice on the tongue) and unstimulated saliva flow rates can be measured from the individual parotid glands or sublingual/submandibular glands.
Box 3. Measurement of unstimulated whole salivary flow rate.
From Wu AJ. Optimizing dry mouth treatment for individuals with Sjögren's syndrome. Rheum Dis Clin North Am 2008;34(4):1004; with permission.
Unstimulated whole saliva collection measures saliva production under resting or basal conditions. The patient should not have had anything to eat or drink for 90 minutes before the procedure. The use of a parasympathomimetic should be discontinued for 12 hours before the procedure, and the use of artificial saliva should be stopped 3 hours before. During the collection procedure, the patient is instructed to minimize actions that can stimulate saliva (talking, increased orofacial movement) and should not swallow. At time 0, any saliva present in the mouth is cleared by swallowing. For the subsequent 5 minutes, any saliva collected in the mouth is emptied into a preweighed tube every minute (i.e., 5 times). This collecting tube then is weighed to determine a postcollection weight. The difference between the precollection and postcollection weight is determined, and this represents the unstimulated whole saliva production for 5 minutes. To convert to a volume of saliva from the weight of saliva, an assumption is made that saliva is similar to water, with 1 g of water/saliva at 4°C equaling 1 mL of saliva/water.
Less than 0.100 mL/min is considered a reduced unstimulated salivary flow rate.
Human salivary glands undergo atrophy with age (Fig. 1). In morphometric studies, aging was associated with acinar loss and replacement with fat and connective tissue [23, 24]. Whole unstimulated saliva flow rates decline with age, which may contribute to the age-dependent increase in dental caries [25]. However, this is not true for stimulated parotid saliva flow rates [26].
Fig. 1.
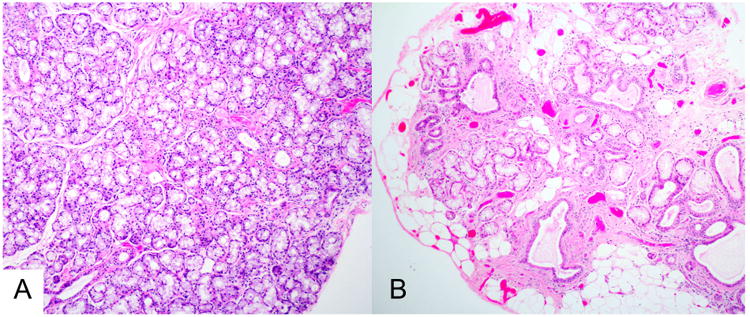
Histopathology of minor labial salivary glands. The sections are from biopsies of a 28-year-old woman (A) and a 65-year-old woman (B), shown at the same magnification. Neither had Sjögren syndrome. (A) This histopathologic section shows normal tissue, with confluent mucous acini and normal-sized intralobular ducts. (B) In contrast, this section shows extensive acinar loss, interstitial fibrosis, ductal dilatation, and fatty replacement. These changes are often seen to varying degrees in older patients (H&E stain, original magnification ×100).
There are multiple potential causes for xerostomia and salivary hypofunction (Box 4) [10]. Side effects from medications commonly used in older individuals are the most common.
Box 4. Common causes of dry mouth.
Medications, including antidepressants, anticholinergics, antispasmodics, antihypertensives, antihistamines, sedatives, and diuretics
SS
Diabetes mellitus
Head and neck irradiation
Dehydration
Parkinson disease
Vaginal dryness
Vaginal dryness, dyspareunia, and vulvar pruritus are common symptoms among postmenopausal women. These symptoms relate to menopause-related decreases in the levels of estrogen and other sex steroids but can also have other causes. In 2014, 2 international societies recommended that the range of symptoms and signs associated with menopause be termed the genitourinary syndrome of menopause [27]. These symptoms include genital dryness, burning, irritation, inadequate lubrication, dyspareunia, urinary urgency, dysuria, and recurrent urinary tract infections. Similar symptoms are also seen with infectious vaginitis, irritant or allergic vulvitis or vaginitis, vulvovaginal dermatoses, hypertonic pelvic floor muscle dysfunction, painful bladder syndrome/interstitial cystitis, vulvodynia, and pudendal neuralgia [27].
In women affected by SS, vaginal dryness can be severe and affect sexual ability and pleasure [28]. There is scant information regarding the cause of this dryness. One hypothesis is that the Skene and related glands of the vaginal introitus are affected in the same manner as exocrine glands found elsewhere [29]. There has been no histopathologic confirmation of this to date. Biopsies of vaginal mucosa from patients with SS show subepithelial inflammatory infiltrates more frequently than those from controls [30]. A negative effect of this infiltrate on the transudation of serous fluid into the vaginal vault constitutes an alternative hypothesis for vaginal dryness in women with SS.
Sjögren syndrome
Sjögren syndrome (SS) is the prototypic illness of dryness of the eyes and mouth. It is a chronic systemic autoimmune disease characterized by dry eyes and dry mouth, arising from autoimmune-induced inflammation of the lacrimal and salivary glands. This chronic inflammatory process gradually leads to glandular injury and related dysfunction over the course of years, eventually causing the cardinal symptoms of dry eyes and mouth. It primarily affects perimenopausal and postmenopausal women and can occur in a primary form or in association with another systemic autoimmune disease (termed secondary SS). The reported prevalence of primary SS in population-based studies ranges from 0.01% to 0.09% [31]. SS is present in up to 17% of patients with rheumatoid arthritis [32, 33]. Because the latter is a disease whose prevalence reaches 1.1% in the United States [34], this renders SS the second most common systemic rheumatic disease.
Key features are shown in Box 5.
Box 5.
|
Abbreviation: MALT, mucosa-associated lymphoid tissue.
SS disease onset is uncommon after the age of 65 or 70 years [35, 36]. Older patients with SS, compared with younger ones, have a lower frequency of serologic abnormalities, such as anti-SSA, anti-SSB, rheumatoid factor, and hyperglobulinemia [37]. Parotid enlargement, arthralgia, and Raynaud phenomenon are also less common, although higher frequencies of lung involvement and anemia have been noted [36]. A distinct subset of older patients with SS with anticentromere antibodies is characterized by Raynaud phenomenon, overlap features of limited systemic sclerosis, and more severe salivary and lacrimal gland dysfunction [38].
The clinical presentation of SS is varied, but is most often that of mucosal dryness (Box 6).
Box 6. Modes of presentation of Sjögren syndrome.
Symptoms or signs of dry eyes and mouth
Episodic or persistent salivary gland enlargement
Sudden increase in dental caries
An established connective tissue disease complicated by dry eyes or mouth
Extraglandular disease (eg, annular erythema, cryoglobulinemia, peripheral neuropathy, or interstitial pneumonitis)
Abnormal serologic test, such as anti-SSA and/or anti-SSB antibodies
MALT lymphoma of a salivary gland
SS is associated with a variety of systemic manifestations (Box 7). Some are direct manifestations of the disease, whereas others represent coincidental autoimmune diseases. Apart from symptoms of fatigue, joint pain, and mild cognitive impairment (often termed brain fog), the prevalence of these organ-specific manifestations is each less than 20% [39].
Box 7. Systemic manifestations of Sjögren syndrome.
| Organ Involvement | Manifestation |
|---|---|
| Constitutional | Fatigue Mild cognitive disturbance |
| Musculoskeletal | Arthritis/arthralgia Myositis (especially inclusion body myositis) |
| Cutaneous | Annular erythema Xerosis Palpable purpura |
| Pulmonary | Interstitial pneumonitis Follicular bronchiolitis |
| Vascular | Raynaud Vasculitis |
| Gastrointestinal | Atrophic gastritis Primary biliary cirrhosis |
| Endocrine | Autoimmune thyroid disease |
| Cardiac | Pericarditis |
| Renal | Interstitial nephritis with renal tubular acidosis Membranoproliferative glomerulonephritis |
| Hematologic | Leukopenia, neutropenia Thrombocytopenia Anemia Monoclonal gammopathy Cryoglobulinemia |
| Lymphoproliferative | Lymphoma |
| Neurologic | Peripheral neuropathy Ataxic ganglionopathy Myelitis (including neuromyelitis optica) |
The natural history is generally one of stability, with a slow decline in lacrimal and salivary gland function. Patients may report periods of worsening sicca or fatigue and uncommonly have the types of systemic disease flares seen in systemic lupus or rheumatoid arthritis. There is no increase in overall mortality according to a recent meta-analysis, but patients with specific extraglandular manifestations, including those with vasculitis, cryoglobulinemia, pulmonary disease, and lymphoma, have been identified as having higher mortalities [40, 41].
Diagnosis of Sjögren syndrome
The diagnosis requires evidence of autoimmune-induced inflammation targeting the salivary or lacrimal glands. In 2016, a new set of classification criteria was jointly endorsed by the American College of Rheumatology (ACR) and the European League against Rheumatism (EULAR) (Box 8) [42]. These criteria have supplanted two previous sets, those of the American-European Consensus Group (2002) and the American College of Rheumatology (2012) [43, 44]. The new criteria incorporate elements of these previous sets and eliminate some that were outdated, but maintain the requirement that the diagnosis of Sjögren's syndrome be only tenable if a patient has either anti-SSA antibodies or a “positive” minor salivary gland biopsy (focal lymphocytic sialadenitis with a focus score greater than or equal to 1).
Box 8. ACR-EULAR Classification Criteria for primary Sjögren's syndrome (SS).
The classification of primary SS applies to any individual who meets the inclusion criteria1, does not have any of the conditions listed as exclusion criteria2, and has a score ≥ 4 when the weights from the 5 criteria items below are summed:
| Item | Weight/Score |
|---|---|
| Labial salivary gland with focal lymphocytic sialadenitis and focus score of ≥ 1 foci/4 mm23 | 3 |
| Anti-Ro/SSA positive | 3 |
| Ocular Staining Score ≥ 5 (or van Bijsterveld score ≥ 4) in at least one eye4,5 | 1 |
| Schirmer's test ≤ 5 mm/5 minutes in at least one eye4 | 1 |
| Unstimulated whole saliva flow rate ≤ 0.1 ml/minute4,6 | 1 |
Inclusion criteria: these criteria are applicable to any patient with at least one symptom of ocular or oral dryness, defined as a positive response to at least 1 of the following questions: 1) Have you had daily, persistent, troublesome dry eyes for more than 3 months? 2) Do you have a recurrent sensation of sand or gravel in the eyes? 3) Do you use tear substitutes more than 3 times a day 4) Have you had a daily feeling of dry mouth for more than 3 months? 5) Do you frequently drink liquids to aid in swallowing dry food?; or in whom there is suspicion of SS from the European League Against Rheumatism SS Disease Activity Index questionnaire (at least one domain with positive item)
- History of head and neck radiation treatment
- Active Hepatitis C infection (with positive PCR)
- Acquired immunodeficiency syndrome
- Sarcoidosis
- Amyloidosis
- Graft versus host disease
- IgG4-related disease
Labial salivary gland (LSG) with focal lymphocytic sialadenitis (FLS) and focus score (FS) ≥ 1 foci/4 mm2. The histopathologic examination should be performed by a pathologist with expertise in the diagnosis of FLS, and FS count following a protocol described in Daniels TE, et al Arthritis Rheum 2011;63:2021-2030.
Patients who are normally taking anticholinergic drugs should be evaluated for objective signs of salivary hypofunction and ocular dryness after a sufficient interval off these medications for these components to be a valid measure of oral and ocular dryness
Ocular staining score described by Whitcher et al. Am J Ophthalmol 2010; 149(3):405-15. VB: van Bijsterveld score described in Van Bijsterveld OP. Arch Ophthalmol 1969;82:10-14.
UWS: unstimulated whole saliva described in Navazesh M, Kumar SK, University of Southern California School of D. Measuring salivary flow: challenges and opportunities. J Am Dent Assoc. 2008;139 Suppl:35S-40S.
From: Shiboski CH, Shiboski SC, Seror R, Criswell L, Labetoulle M, Lietman T, Rasmussen A, Scofield H, Vitali C, Bowman SJ, Mariette X. 2015 Classification Criteria for Sjögren's Syndrome: A Consensus and Data-Driven Methodology involving three International Patient Cohorts. Arthritis Rheum, 2017, 69:35-45
These criteria are only applicable to an individual with findings concerning for Sjögren's syndrome, defined as at least one symptom of ocular or oral dryness (positive response to at least one of five standardized questions), salivary gland enlargement, or a characteristic extraglandular manifestation of Sjögren's syndrome (as defined by a positive domain in the EULAR Sjögren's Syndrome Disease Activity Index) [45].
The authors use these current classification criteria as a general guide, and establish the diagnosis if a patient has an objective measure of ocular and/or oral dryness or characteristic imaging abnormalities (e.g., by ultrasonography, magnetic resonance [MR], or computed tomography [CT]), coupled with anti-SSA antibodies or a positive lip biopsy.
The authors recommend that patients suspected of having SS be evaluated as follows:
History, seeking a history of persistent symptoms of dry eyes and/or mouth. Validated screening questions are included in the ACR/EULAR Classification Criteria (see Box 8, footnote)
-
Examination, seeking signs of salivary hypofunction and of a systemic rheumatic disease
- Oral examination
- Is there enlargement of the lacrimal or major salivary glands? What is the texture of the major salivary glands? Are there discrete nodules or masses?
- Does saliva pool under the elevated tongue when observed over the course of 1 minute?
- Does the tongue have deep fissures, a hyperlobulated appearance, or absence of filiform papillae on its surface?
- The Challacombe scale, available online, can be used to identify and rate the severity of oral dryness, based on physical examination findings (http://www.challacombescale.co.uk/Challacombe-Scale-ENG.pdf, last accessed February 11, 2018) [46].
- General examination
- Look for sclerodactyly, palpable purpura, synovitis, basilar pulmonary rales
-
Laboratory testing
Screen for ANA (tested by immunofluorescence assay), anti-SSA (Ro), and anti-SSB (La), and rheumatoid factor. Anti-SSA and anti-SSB
A complete blood count, urinalysis, and chemistry profile may reveal abnormalities supportive of SS, including leukopenia and neutropenia, hyperglobulinemia, renal impairment, and proteinuria.
-
Ophthalmologic examination
Schirmer testing is an appropriate initial test. A formal ophthalmologic examination serves not only to confirm the diagnosis of dry eye but also to define the contributing causes, such as meibomian gland dysfunction and conjunctivochalasis. Guidelines for this evaluation can be found at https://sicca-online.ucsf.edu/documents/eye-exam-SOP.pdf
-
Sialometry
Documentation of salivary hypofunction is only necessary if the eye examination does not show dry eye disease (see Box 3).
-
Labial gland biopsy
A labial gland biopsy, best performed by an oral surgeon, is required for diagnosis if the patient lacks anti-SSA and/or anti-SSB antibodies. The biopsy also has value in excluding alternative diagnoses (e.g., sarcoid, amyloid, mucosa-associated lymphoid tissue lymphoma, and immunoglobulin [Ig] G4–related disease). Guidelines for its performance can be found at https://sicca-online.ucsf.edu/documents/Oral-Saliva-SOP.pdf.
-
Imaging (Fig. 2)
Salivary gland ultrasonography is favored because of its low cost and lack of ionizing radiation. The presence of multiple ovoid hypoechoic lesions, often bounded by hyperechoic bands, correlates with markers of more severe disease. These imaging abnormalities have high specificity for the diagnosis, but only moderate sensitivity [47-51].
CT imaging is not recommended because of the radiation exposure. However, the presence of multiple punctate calcifications within the parotid glands has high specificity [52].
MRI of the parotid glands may reveal heterogeneity of signal intensity on both T1-weighted and T2-weighted images, with both hypointense and hyperintense foci measuring 1 to 4 mm in diameter [53].
Fig. 2.
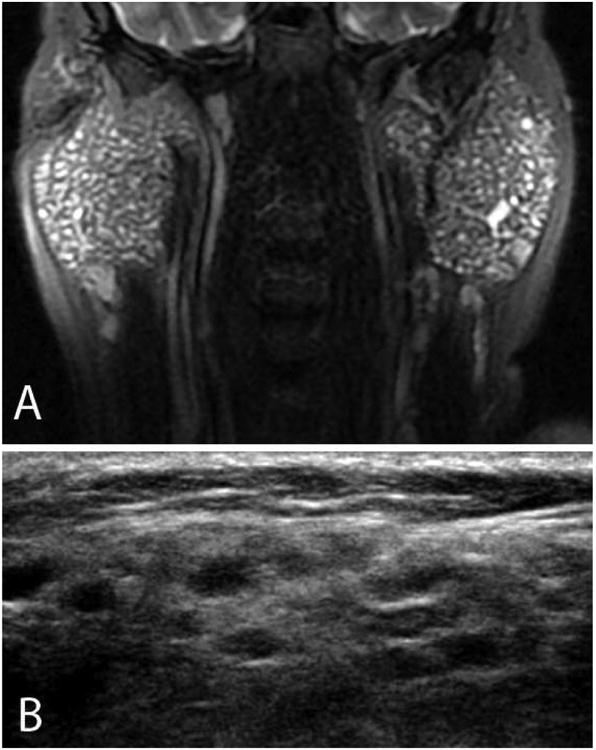
Imaging techniques in Sjögren syndrome. This patient has bilateral symmetric parotid gland enlargement, seen best on the T2 fat-suppressed MR images (A). Note the multiple T2-hyperintense foci scattered throughout both glands, a characteristic finding. With ultrasonography (B), multiple hypoechoic rounded lesions with convex borders are noted throughout the glandular parenchyma. In normal parotid gland tissue, the parenchyma has a homogeneous appearance with ultrasonography.
Be aware of common pitfalls in the diagnostic evaluation. These include:
Assessment of sicca manifestations. Certain historical features distinguish the sicca manifestations of Sjögren's syndrome from symptoms often experienced by otherwise healthy people. The symptoms of ocular and oral dryness should be a daily, persistent problem and have been present for at least 3 months. The ocular dryness should be severe enough to mandate the use of tear supplements at least 3 times per day. Positive responses to the following two questions are highly predictive of salivary hypofunction [21]: Do you sip liquids to aid in swallowing dry foods? Does your mouth feel dry when eating a meal? The ophthalmologist's assessment of a dry eye patient for SS should include a Schirmer test and conjunctival staining with Lissamine green (as opposed to simply assessing corneal staining with fluorescein), since positive results of these two tests correlate best with positive serology and positive lip biopsy [54].
Antibody testing. Antibodies to SSA and SSB are not specific. They are found in systemic lupus and inflammatory myopathies and are seen in up to 0.9% of healthy women in the US population [55]. With modern multiplex assay technology, weakly positive test results for anti-SSA and anti-SSB must also be interpreted with caution, since they have a less robust association with SS. In particular, the finding of anti-SSB antibodies alone, in the absence of anti-SSA antibodies, does not support a diagnosis of SS [56] and has thus been eliminated as a classification criterion for the disease [42]. The authors recommend the performance of a labial gland biopsy in the diagnostic evaluation of patients with weakly positive anti-SSA or anti-SSB antibodies (or anti-SSB alone), in whom SS is suspected.A commercial assay for three murine tissue specific autoantibodies, carbonic anhydrase 6, parotid specific protein, and salivary protein-1, is now available as a test for early Sjögren's syndrome. However, the ability of these antibodies to mark individuals who are destined to develop Sjögren's syndrome has not been validated [57].
Labial gland biopsy performance and interpretation. The histopathology of the minor salivary gland, termed focal lymphocytic sialadenitis, is characterized by lymphocytic aggregates that surround intralobular salivary ducts (Fig. 3) and are adjacent to normal-appearing mucus-secreting acini. The number of these lymphocytic aggregates per 4 mm2 of glandular tissue section equates to the focus score. A score greater than or equal to 1 is a criterion for the classification of SS and has been validated as the best cutoff value differentiating SS from non-SS controls [58]. Accurate assessment of the focus score requires adequate glandular tissue for analysis; ideally 3-5glands should be collected at the time of biopsy and the total surface area of the glandular surface area should be at least 4 mm2 (preferably 10-20 mm2 since the focus score can be overestimated in smaller specimens) [58]. The total glandular surface area of the tissue section should be measured with a calibrated reticule in the microscope eyepiece or with digital image software. Because chronic inflammation of the salivary gland can also arise from ductal obstruction and other forms of glandular injury, care must be taken to exclude from the focus score lymphocytic aggregates in areas of severe acinar loss, ductal dilatation, and fibrosis (Fig. 4). Assessment of the labial gland biopsy for Sjögren's syndrome may require that the slides be forwarded to a reference laboratory for interpretation and proper calculation of the focus score.
Fig. 3.
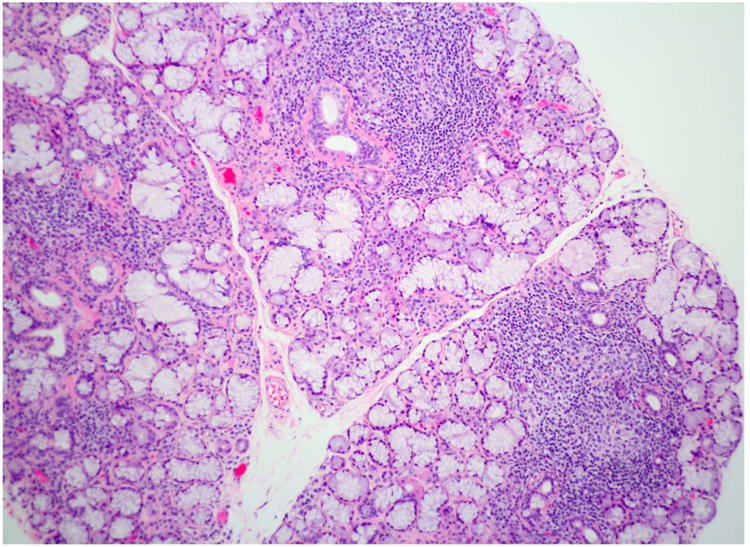
Focal lymphocytic sialadenitis. This section of a labial minor salivary gland biopsy shows the typical features of focal lymphocytic sialadenitis. Note the tightly aggregated lymphocytes surrounding ducts and adjacent to normal-appearing mucous acini. At least 3 foci are evident (H&E stain, original magnification ×100).
Fig. 4.
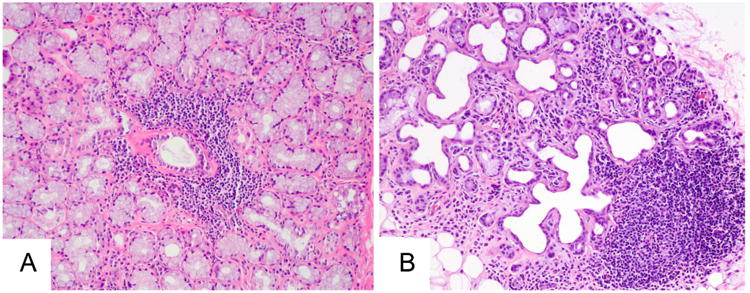
Potential misinterpretation of labial gland biopsies. (A) The lymphocytic focus is typical of that seen in focal lymphocytic sialadenitis, being centered on a duct and adjacent to normal-appearing mucus-secreting acini. (B) In contrast, the lymphocytic focus here is present within a gland lobule marked by interstitial fibrosis, ductal dilatation, and marked acinar loss. This focus should not be interpreted as representative of Sjögren syndrome (H&E stain, original magnification ×100).
The differential diagnosis of SS primarily includes alternative causes of sicca symptoms, salivary and/or lacrimal gland enlargement, and the characteristic serologic abnormalities.
Sicca complex in the elderly: age-related interstitial fibrosis, acinar atrophy, and nonspecific chronic inflammation in the labial gland biopsy may be misinterpreted as indicating SS (see Fig. 4).
Salivary and/or lacrimal gland enlargement: Particular attention should be paid to the possibility of lymphoma. IgG-4 related disease is most common in older men. It may present as unilateral submandibular gland enlargement (Küttner tumor) or parotid and lacrimal gland enlargement. Other diagnostic possibilities include amyloid infiltration, sarcoidosis, human immunodeficiency virus infection, bulimia, and hyperlipoproteinemia [59].
Serologic abnormalities: antinuclear antibodies, rheumatoid factor, and monoclonal proteins are more prevalent in the elderly population [55]. Thus, positive tests must be interpreted cautiously when they coincide with symptoms or signs of oral or ocular dryness.
Management of Sjögren syndrome
Most patients only require topical and systemic treatments directed at alleviating their ocular, oral, and vaginal dryness; preventing dental decay; and managing oral candidiasis. Patients with systemic manifestations, including those with joint pain, skin lesions, and internal organ involvement, may benefit from immunomodulatory treatments. All patients with SS require monitoring for disease complications, especially lymphoma. The British Society for Rheumatology has recently established guidelines for the management of Sjögren's syndrome [60].
Management of ocular dryness depends on its severity and the patient's response to therapy [61]. Avoidance of wind and smoke, and the use of protective eyewear, can be helpful for all patients. Artificial tears with a demulcent (e.g., methylcellulose, propylene glycol, and glycerin) are a mainstay of treatment. Patients should use preservative-free drops if drops are instilled 4 or more times a day. Use of thicker ocular gels and ointments before bed can help with dryness that occurs during sleep. Supplementation of the diet with omega-3 essential fatty acids has been shown to be of benefit. Use of topical cyclosporine and steroid solutions can be useful in a variety of dry eye conditions but should be undertaken in consultation with an ophthalmologist. Punctal plugs to preserve tears are often used in moderate to severe dry eye. Patients with more severe dry eye disease may require the use of moisture chamber spectacles, autologous serum tears, contact lenses, or scleral prostheses.
Prevention of oral dryness includes maintaining good hydration and avoiding medications that worsen dryness. Patients should be counseled to be more aware of factors that can aggravate dryness, such as low-humidity environments and mouth breathing. Frequent sips of oral solutions can be helpful, with options ranging from water to artificial saliva. Sucking on sugar-free hard candies helps stimulate saliva flow. Oral hygiene and dental care are essential in preserving dentition in persons with pathologic oral dryness.
Muscarinic agonists, such as pilocarpine and cevimeline, can substantially increase saliva and, to a lesser extent, tear flow. However, overall tolerance of these agents may be hampered by cholinergic side effects of excessive sweating, increased urinary frequency, flushing, chills, rhinitis, nausea, and diarrhea. Care must be taken when these medications are prescribed to the elderly.
Vaginal moisturizers and lubricants, including olive and vitamin E oils, are initial treatment options for vaginal dryness. Vitamin E capsules can be opened and the oil used in and around the vagina. A suppository containing hyaluronic acid, vitamin E, and vitamin A, used once daily for 14 days, then once every other day for the next 2 weeks, can be effective [62]. Obtaining these suppositories requires a compounding pharmacist. Low-dose vaginal estrogen therapy is indicated if symptoms do not improve with these nonprescription measures. The available options include a vaginal cream, insert, ring, or soft gel capsule [63].
Hydroxychloroquine is commonly used for the management of joint pain and/or fatigue. However, clinical trials with this drug have shown mixed results, with none showing major clinical improvements [64-66]. The effect of immunosuppressive therapies on the glandular manifestations has been disappointing to date. The effect of rituximab on SS dryness is still being evaluated, with potential benefit being observed in a small, double-blind, placebo-controlled trial [67] but not in two larger ones [68, 69]. Prolonged therapy may be required for benefit [70].
Summary
Dryness of the eyes and mouth is a prevalent symptom in the population, especially among the elderly, and is most often related to the side effects of medications. However, there is a broad differential diagnosis for each symptom, and careful evaluation is important to define the cause and correct treatment. SS is the prototypic disease that leads to these symptoms and primarily affects perimenopausal women. The diagnosis requires demonstration of an autoimmune disease underlying the sicca manifestations, either serologically or pathologically. Management can involve both topical and systemic therapies.
Key points.
Dryness of the eyes, mouth, and other mucosal membranes (sicca) is reported by up to 30% of persons over the age of 65, but is related to an underlying autoimmune disease in only a minority of these.
Sjögren Syndrome is the prototypic autoimmune illness that causes dry eyes and dry mouth and is an important diagnostic consideration in individuals presenting with dry eye and mouth Symptoms.
The diagnosis of Sjögren Syndrome requires the presence of anti-Sjögren Syndrome A (SSA) and/or anti-Sjögren Syndrome B (SSB) antibodies, or a minor salivary gland biopsy showing at least 1 tightly aggregated periductal lymphocytic aggregate per 4 mm2 of glandulär tissue section (focal lymphocytic sialadenitis with a focus score ≥1).
Management of Sjögren Syndrome requires attention to both the glandulär (ocular and oral dryness, glandulär enlargement) and extraglandular manifestations (e.g., arthritis, Pneumonitis, nephritis, vasculitis).
Acknowledgments
This article was supported in part by the Intramural Research Program of the NIH, NIDCR. Dr. Baer's work was supported by NIH grant ROI DE12354-15A1 and the Jerome L. Greene Foundation.
Footnotes
Disclosure: Dr A.N. Baer reports Consulting fees from Bristol-Myers Squibb, Abbvie, and Novartis.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Sjögren H. On knowledge of the keratoconjunctivitis sicca. VII. The sicca syndrome--an autoimmune disease. Acta Ophthalmol (Copenh) 1968;46(2):201–6. doi: 10.1111/j.1755-3768.1968.tb05177.x. [DOI] [PubMed] [Google Scholar]
- 2.Sjögren H. Zur Kenntnis der Keratoconjunctivitis sicca (Keratitis filiformis bei Hypofunktion der Tränendrüsen) Acta Ophthalmol (Copenh) 1933;11(Suppl 2):1–151. [Google Scholar]
- 3.Johansson AK, Johansson A, Unell L, et al. Self-reported dry mouth in Swedish population samples aged 50, 65 and 75 years. Gerodontology. 2012;29(2):e107–15. doi: 10.1111/j.1741-2358.2010.00420.x. [DOI] [PubMed] [Google Scholar]
- 4.Lin PY, Tsai SY, Cheng CY, et al. Prevalence of dry eye among an elderly Chinese population in Taiwan: the Shihpai Eye Study. Ophthalmology. 2003;110(6):1096–101. doi: 10.1016/S0161-6420(03)00262-8. [DOI] [PubMed] [Google Scholar]
- 5.Billings RJ, Proskin HM, Moss ME. Xerostomia and associated factors in a community-dwelling adult population. Community Dent Oral Epidemiol. 1996;24(5):312–6. doi: 10.1111/j.1600-0528.1996.tb00868.x. [DOI] [PubMed] [Google Scholar]
- 6.Schein OD, Munoz B, Tielsch JM, et al. Prevalence of dry eye among the elderly. Am J Ophthalmol. 1997;124(6):723–8. doi: 10.1016/s0002-9394(14)71688-5. [DOI] [PubMed] [Google Scholar]
- 7.Hay EM, Thomas E, Pal B, et al. Weak association between subjective symptoms or and objective testing for dry eyes and dry mouth: results from a population based study. Ann Rheum Dis. 1998;57(1):20–4. doi: 10.1136/ard.57.1.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Orellana MF, Lagravere MO, Boychuk DG, et al. Prevalence of xerostomia in population-based samples: a systematic review. J Public Health Dent. 2006;66(2):152–8. doi: 10.1111/j.1752-7325.2006.tb02572.x. [DOI] [PubMed] [Google Scholar]
- 9.Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334–65. doi: 10.1016/j.jtos.2017.05.003. [DOI] [PubMed] [Google Scholar]
- 10.Liu B, Dion MR, Jurasic MM, et al. Xerostomia and salivary hypofunction in vulnerable elders: prevalence and etiology. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114(1):52–60. doi: 10.1016/j.oooo.2011.11.014. [DOI] [PubMed] [Google Scholar]
- 11.Schein OD, Hochberg MC, Munoz B, et al. Dry eye and dry mouth in the elderly: a population-based assessment. Arch Intern Med. 1999;159(12):1359–63. doi: 10.1001/archinte.159.12.1359. [DOI] [PubMed] [Google Scholar]
- 12.Hochberg MC, Schein OD, Munoz B, et al. The prevalence of dry eye, dry mouth, autoimmunity and primary Sjögren's syndrome in the general population [abstract] Arthritis Rheum. 1996;39(Suppl):S66. [Google Scholar]
- 13.The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007) Ocul Surf. 2007;5(2):75–92. doi: 10.1016/s1542-0124(12)70081-2. [DOI] [PubMed] [Google Scholar]
- 14.Cho P, Yap M. Schirmer test. I. A review. Optom Vis Sci. 1993;70(2):152–6. doi: 10.1097/00006324-199302000-00011. [DOI] [PubMed] [Google Scholar]
- 15.van Bijsterveld OP. Diagnostic tests in the Sicca syndrome. Arch Ophthalmol. 1969;82(1):10–4. doi: 10.1001/archopht.1969.00990020012003. [DOI] [PubMed] [Google Scholar]
- 16.Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640–50. doi: 10.1097/00003226-200310000-00008. [DOI] [PubMed] [Google Scholar]
- 17.Whitcher JP, Shiboski CH, Shiboski SC, et al. A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjögren's Syndrome International Registry. Am J Ophthalmol. 2010;149(3):405–15. doi: 10.1016/j.ajo.2009.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sweeney DF, Millar TJ, Raju SR. Tear film stability: a review. Exp Eye Res. 2013;117:28–38. doi: 10.1016/j.exer.2013.08.010. [DOI] [PubMed] [Google Scholar]
- 19.Lemp MA, Bron AJ, Baudouin C, et al. Tear osmolarity in the diagnosis and management of dry eye disease. Am J Ophthalmol. 2011;151(5):792–798.e1. doi: 10.1016/j.ajo.2010.10.032. [DOI] [PubMed] [Google Scholar]
- 20.Potvin R, Makari S, Rapuano CJ. Tear film osmolarity and dry eye disease: a review of the literature. Clin Ophthalmol. 2015;9:2039–47. doi: 10.2147/OPTH.S95242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fox PC, Busch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc. 1987;115(4):581–4. doi: 10.1016/s0002-8177(87)54012-0. [DOI] [PubMed] [Google Scholar]
- 22.Dawes C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66 Spec No:648–53. doi: 10.1177/00220345870660S107. [DOI] [PubMed] [Google Scholar]
- 23.Scott J, Flower EA, Burns J. A quantitative study of histological changes in the human parotid gland occurring with adult age. J Oral Pathol. 1987;16(10):505–10. doi: 10.1111/j.1600-0714.1987.tb00681.x. [DOI] [PubMed] [Google Scholar]
- 24.Syrjanen S. Age-related changes in structure of labial minor salivary glands. Age Ageing. 1984;13(3):159–65. doi: 10.1093/ageing/13.3.159. [DOI] [PubMed] [Google Scholar]
- 25.Percival RS, Challacombe SJ, Marsh PD. Flow rates of resting whole and stimulated parotid saliva in relation to age and gender. J Dent Res. 1994;73(8):1416–20. doi: 10.1177/00220345940730080401. [DOI] [PubMed] [Google Scholar]
- 26.Ship JA, Pillemer SR, Baum BJ. Xerostomia and the geriatric patient. J Am Geriatr Soc. 2002;50(3):535–43. doi: 10.1046/j.1532-5415.2002.50123.x. [DOI] [PubMed] [Google Scholar]
- 27.Portman DJ, Gass ML Vulvovaginal Atrophy Terminology Consensus Conference Panel. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women's Sexual Health and the North American Menopause Society. Menopause. 2014;21(10):1063–8. doi: 10.1097/GME.0000000000000329. [DOI] [PubMed] [Google Scholar]
- 28.Maddali Bongi S, Del Rosso A, Orlandi M, et al. Gynaecological symptoms and sexual disability in women with primary Sjögren's syndrome and sicca syndrome. Clin Exp Rheumatol. 2013;31(5):683–90. [PubMed] [Google Scholar]
- 29.Bloch KJ, Buchanan WW, Wohl MJ, et al. Sjögren's Syndrome. a Clinical, Pathological, and Serological Study of Sixty-Two Cases Medicine (Baltimore) 1965;44:187–231. [PubMed] [Google Scholar]
- 30.van Nimwegen JF, van der Tuuk K, Klinkert ER, et al. Subepithelial Infiltrate of the Vagina in Primary Sjögren's Syndrome: The Cause of Vaginal Dryness? Arthritis Rheumatol. 2017;69(Suppl 10) [Google Scholar]
- 31.Qin B, Wang J, Yang Z, et al. Epidemiology of primary Sjögren's syndrome: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74(11):1983–9. doi: 10.1136/annrheumdis-2014-205375. [DOI] [PubMed] [Google Scholar]
- 32.Uhlig T, Kvien TK, Jensen JL, et al. Sicca symptoms, saliva and tear production, and disease variables in 636 patients with rheumatoid arthritis. Ann Rheum Dis. 1999;58(7):415–22. doi: 10.1136/ard.58.7.415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Carmona L, Gonzalez-Alvaro I, Balsa A, et al. Rheumatoid arthritis in Spain: occurrence of extra-articular manifestations and estimates of disease severity. Ann Rheum Dis. 2003;62(9):897–900. doi: 10.1136/ard.62.9.897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gabriel SE, Crowson CS, O'Fallon WM. The epidemiology of rheumatoid arthritis in Rochester, Minnesota, 1955-1985. Arthritis Rheum. 1999;42(3):415–20. doi: 10.1002/1529-0131(199904)42:3<415::AID-ANR4>3.0.CO;2-Z. [DOI] [PubMed] [Google Scholar]
- 35.Botsios C, Furlan A, Ostuni P, et al. Elderly onset of primary Sjögren's syndrome: clinical manifestations, serological features and oral/ocular diagnostic tests. Comparison with adult and young onset of the disease in a cohort of 336 Italian patients. Joint Bone Spine. 2011;78(2):171–4. doi: 10.1016/j.jbspin.2010.05.008. [DOI] [PubMed] [Google Scholar]
- 36.Ramos-Casals M, Solans R, Rosas J, et al. Primary Sjögren syndrome in Spain: clinical and immunologic expression in 1010 patients. Medicine (Baltimore) 2008;87(4):210–9. doi: 10.1097/MD.0b013e318181e6af. [DOI] [PubMed] [Google Scholar]
- 37.Haga HJ, Jonsson R. The influence of age on disease manifestations and serological characteristics in primary Sjögren's syndrome. Scand J Rheumatol. 1999;28(4):227–32. doi: 10.1080/03009749950155599. [DOI] [PubMed] [Google Scholar]
- 38.Baer AN, Medrano L, McAdams-DeMarco M, et al. Anti-centromere antibodies are associated with more severe exocrine glandular dysfunction in Sjögren's syndrome: Analysis of the Sjögren's International Collaborative Clinical Alliance cohort. Arthritis Care Res (Hoboken) 2016 doi: 10.1002/acr.22859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Brito-Zeron P, Ramos-Casals M EULAR-SS task force group. Advances in the understanding and treatment of systemic complications in Sjögren's syndrome. Curr Opin Rheumatol. 2014;26(5):520–7. doi: 10.1097/BOR.0000000000000096. [DOI] [PubMed] [Google Scholar]
- 40.Singh AG, Singh S, Matteson EL. Rate, risk factors and causes of mortality in patients with Sjögren's syndrome: a systematic review and meta-analysis of cohort studies. Rheumatology (Oxford) 2016;55(3):450–60. doi: 10.1093/rheumatology/kev354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Nannini C, Jebakumar AJ, Crowson CS, et al. Primary Sjögren's syndrome 1976-2005 and associated interstitial lung disease: a population-based study of incidence and mortality. BMJ Open. 2013;3(11):e003569, 2013–003569. doi: 10.1136/bmjopen-2013-003569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Shiboski CH, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren's Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017;69(1):35–45. doi: 10.1002/art.39859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Vitali C, Bombardieri S, Jonsson R, et al. Classification criteria for Sjögren's syndrome: a revised version of the European criteria proposed by the American-European Consensus Group. Ann Rheum Dis. 2002;61(6):554–8. doi: 10.1136/ard.61.6.554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Shiboski SC, Shiboski CH, Criswell L, et al. American College of Rheumatology classification criteria for Sjögren's syndrome: a data-driven, expert consensus approach in the Sjögren's International Collaborative Clinical Alliance cohort. Arthritis Care Res (Hoboken) 2012;64(4):475–87. doi: 10.1002/acr.21591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Seror R, Bowman SJ, Brito-Zeron P, et al. EULAR Sjögren's syndrome disease activity index (ESSDAI): a user guide. RMD Open. 2015;1(1):e000022. doi: 10.1136/rmdopen-2014-000022. 2014-000022. eCollection 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Osailan SM, Pramanik R, Shirlaw P, et al. Clinical assessment of oral dryness: development of a scoring system related to salivary flow and mucosal wetness. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114(5):597–603. doi: 10.1016/j.oooo.2012.05.009. [DOI] [PubMed] [Google Scholar]
- 47.Cornec D, Jousse-Joulin S, Pers JO, et al. Contribution of salivary gland ultrasonography to the diagnosis of Sjögren's syndrome: toward new diagnostic criteria? Arthritis Rheum. 2013;65(1):216–25. doi: 10.1002/art.37698. [DOI] [PubMed] [Google Scholar]
- 48.Takagi Y, Sumi M, Nakamura H, et al. Ultrasonography as an additional item in the American College of Rheumatology classification of Sjögren's syndrome. Rheumatology (Oxford) 2014;53(11):1977–83. doi: 10.1093/rheumatology/keu238. [DOI] [PubMed] [Google Scholar]
- 49.Theander E, Mandl T. Primary Sjögren's syndrome: diagnostic and prognostic value of salivary gland ultrasonography using a simplified scoring system. Arthritis Care Res (Hoboken) 2014;66(7):1102–7. doi: 10.1002/acr.22264. [DOI] [PubMed] [Google Scholar]
- 50.Baldini C, Luciano N, Tarantini G, et al. Salivary gland ultrasonography: a highly specific tool for the early diagnosis of primary Sjögren's syndrome. Arthritis Res Ther. 2015;17:146. doi: 10.1186/s13075-015-0657-7. 015-0657-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Luciano N, Baldini C, Tarantini G, et al. Ultrasonography of major salivary glands: a highly specific tool for distinguishing primary Sjögren's syndrome from undifferentiated connective tissue diseases. Rheumatology (Oxford) 2015;54(12):2198–204. doi: 10.1093/rheumatology/kev253. [DOI] [PubMed] [Google Scholar]
- 52.Sun Z, Zhang Z, Fu K, et al. Diagnostic accuracy of parotid CT for identifying Sjögren's syndrome. Eur J Radiol. 2012;81(10):2702–9. doi: 10.1016/j.ejrad.2011.12.034. [DOI] [PubMed] [Google Scholar]
- 53.Takashima S, Takeuchi N, Morimoto S, et al. MR imaging of Sjögren syndrome: correlation with sialography and pathology. J Comput Assist Tomogr. 1991;15(3):393–400. doi: 10.1097/00004728-199105000-00009. [DOI] [PubMed] [Google Scholar]
- 54.Bunya VY, Bhosai SJ, Heidenreich AM, et al. Association of Dry Eye Tests With Extraocular Signs Among 3514 Participants in the Sjögren's Syndrome International Registry. Am J Ophthalmol. 2016;172:87–93. doi: 10.1016/j.ajo.2016.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Satoh M, Chan EK, Ho LA, et al. Prevalence and sociodemographic correlates of antinuclear antibodies in the United States. Arthritis Rheum. 2012;64(7):2319–27. doi: 10.1002/art.34380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Baer AN, McAdams DeMarco M, Shiboski SC, et al. The SSB-positive/SSA-negative antibody profile is not associated with key phenotypic features of Sjögren's syndrome. Ann Rheum Dis. 2015;74(8):1557–61. doi: 10.1136/annrheumdis-2014-206683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Beckman KA, Luchs J, Milner MS, et al. The Potential Role for Early Biomarker Testing as Part of a Modern, Multidisciplinary Approach to Sjögren's Syndrome Diagnosis. Adv Ther. 2017;34(4):799–812. doi: 10.1007/s12325-017-0501-3. [DOI] [PubMed] [Google Scholar]
- 58.Daniels TE, Cox D, Shiboski CH, et al. Associations between salivary gland histopathologic diagnoses and phenotypic features of Sjögren's syndrome among 1,726 registry participants. Arthritis Rheum. 2011;63(7):2021–30. doi: 10.1002/art.30381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Cornec D, Saraux A, Jousse-Joulin S, et al. The Differential Diagnosis of Dry Eyes, Dry Mouth, and Parotidomegaly: A Comprehensive Review. Clin Rev Allergy Immunol. 2015;49(3):278–87. doi: 10.1007/s12016-014-8431-1. [DOI] [PubMed] [Google Scholar]
- 60.Price EJ, Rauz S, Tappuni AR, et al. The British Society for Rheumatology guideline for the management of adults with primary Sjögren's Syndrome. Rheumatology (Oxford) 2017;56(10):1643–7. doi: 10.1093/rheumatology/kex163. [DOI] [PubMed] [Google Scholar]
- 61.Foulks GN, Forstot SL, Donshik PC, et al. Clinical guidelines for management of dry eye associated with Sjögren disease. Ocul Surf. 2015;13(2):118–32. doi: 10.1016/j.jtos.2014.12.001. [DOI] [PubMed] [Google Scholar]
- 62.Costantino D, Guaraldi C. Effectiveness and safety of vaginal suppositories for the treatment of the vaginal atrophy in postmenopausal women: an open, non-controlled clinical trial. Eur Rev Med Pharmacol Sci. 2008;12(6):411–6. [PubMed] [Google Scholar]
- 63.Faubion SS, Sood R, Kapoor E. Genitourinary Syndrome of Menopause: Management Strategies for the Clinician. Mayo Clin Proc. 2017;92(12):1842–9. doi: 10.1016/j.mayocp.2017.08.019. [DOI] [PubMed] [Google Scholar]
- 64.Gottenberg JE, Ravaud P, Puechal X, et al. Effects of hydroxychloroquine on symptomatic improvement in primary Sjögren syndrome: the JOQUER randomized clinical trial. JAMA. 2014;312(3):249–58. doi: 10.1001/jama.2014.7682. [DOI] [PubMed] [Google Scholar]
- 65.Kruize AA, Hene RJ, Kallenberg CG, et al. Hydroxychloroquine treatment for primary Sjögren's syndrome: a two year double blind crossover trial. Ann Rheum Dis. 1993;52(5):360–4. doi: 10.1136/ard.52.5.360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Fox RI, Dixon R, Guarrasi V, et al. Treatment of primary Sjögren's syndrome with hydroxychloroquine: a retrospective, open-label study. Lupus. 1996;5(Suppl 1):S31–6. [PubMed] [Google Scholar]
- 67.Meijer JM, Meiners PM, Vissink A, et al. Effectiveness of rituximab treatment in primary Sjögren's syndrome: a randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2010;62(4):960–8. doi: 10.1002/art.27314. [DOI] [PubMed] [Google Scholar]
- 68.Devauchelle-Pensec V, Mariette X, Jousse-Joulin S, et al. Treatment of primary Sjögren syndrome with rituximab: a randomized trial. Ann Intern Med. 2014;160(4):233–42. doi: 10.7326/M13-1085. [DOI] [PubMed] [Google Scholar]
- 69.Bowman SJ, Everett CC, ODwyer JL, et al. Randomized Controlled Trial of Rituximab and Cost-Effectiveness Analysis in Treating Fatigue and Oral Dryness in Primary Sjögren's Syndrome. Arthritis Rheumatol. 2017;69(7):1440–50. doi: 10.1002/art.40093. [DOI] [PubMed] [Google Scholar]
- 70.Carubbi F, Cipriani P, Marrelli A, et al. Efficacy and safety of rituximab treatment in early primary Sjögren's syndrome: a prospective, multi-center, follow-up study. Arthritis Res Ther. 2013;15(5):R172. doi: 10.1186/ar4359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Malladi AS, Sack KE, Shiboski SC, et al. Primary Sjögren's syndrome as a systemic disease: a study of participants enrolled in an international Sjögren's syndrome registry. Arthritis Care Res (Hoboken) 2012;64(6):911–8. doi: 10.1002/acr.21610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Theander E, Henriksson G, Ljungberg O, et al. Lymphoma and other malignancies in primary Sjögren's syndrome: a cohort study on cancer incidence and lymphoma predictors. Ann Rheum Dis. 2006;65(6):796–803. doi: 10.1136/ard.2005.041186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Lin DF, Yan SM, Zhao Y, et al. Clinical and prognostic characteristics of 573 cases of primary Sjögrens syndrome. Chin Med J (Engl) 2010;123(22):3252–7. [PubMed] [Google Scholar]
- 74.Ramos-Casals M, Brito-Zeron P, Perez-De-Lis M, et al. Sjögren syndrome or Sjögren disease? The histological and immunological bias caused by the 2002 criteria. Clin Rev Allergy Immunol. 2010;38(2-3):178–85. doi: 10.1007/s12016-009-8152-z. [DOI] [PubMed] [Google Scholar]
- 75.Ekstrom Smedby K, Vajdic CM, Falster M, et al. Autoimmune disorders and risk of non-Hodgkin lymphoma subtypes: a pooled analysis within the InterLymph Consortium. Blood. 2008;111(8):4029–38. doi: 10.1182/blood-2007-10-119974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Papageorgiou A, Ziogas DC, Mavragani CP, et al. Predicting the outcome of Sjögren's syndrome-associated non-hodgkins lymphoma patients. PLoS One. 2015;10(2):e0116189. doi: 10.1371/journal.pone.0116189. [DOI] [PMC free article] [PubMed] [Google Scholar]