

Abstract
Coccidioidal meningitis typically presents with symptoms that may include headache, altered mental status including personality changes, fever, nausea, vomiting, gait abnormalities, and focal neurological deficits. This is a case of coccidioidal meningitis that initially presented as 4 consecutive crescendo cerebrovascular transient ischemic attacks with focal neurological deficits that resolved within minutes. Imaging showed a left basilar coccidioma. Follow-up at 4 months showed treatment response to conservative therapy of fluconazole 1000 mg with a dexamethasone taper. Crescendo cerebrovascular transient ischemic attacks are a unique initial presentation of coccidioidal meningitis.
Keywords: coccidioidomycosis, coccidioidal meningitis, crescendo transient ischemic attack
Introduction
Coccidioides is found as 2 species, immitis and posadasii, that are clinically indistinguishable. Coccidioidomycosis is most commonly an asymptomatic infection. When symptomatic, it is commonly a pneumonia often mistaken for community-acquired pneumonia.1 However, in the few the disease can disseminate anywhere in the body. Meningitis is the most feared form of disseminated coccidioidomycosis. The most common presenting symptom is headache. Other symptoms include altered mental status, with or without fever, personality changes, nausea, vomiting, meningismus, gait abnormalities, and focal neurological deficits.2 Presented here is a case of coccidioidal meningitis that initially presented as multiple consecutive crescendo cerebrovascular transient ischemic attacks (TIAs).
Case
A 64-year-old Hispanic male with diagnosis of pulmonary coccidioidomycosis 2 years prior at another institution and placed on therapy with 400 mg fluconazole daily for 1½ years. Initial serum coccidioidal immunodiffusion of IgM (immunoglobulin) and IgG were weakly reactive with complement fixation titers of 1:4. Symptoms resolved, and his physician decreased fluconazole to 200 mg daily for 4 months. He did well for 1 month until he developed left-sided headaches. After 2 weeks, he had 2 episodes of left arm and leg weakness without ability to walk and lower right facial palsy over a period of 10 minutes.
In the emergency department, while having his vitals taken, the patient had another episode of lower right facial palsy and left-sided weakness that resolved in 5 minutes. Computed tomography scan of brain without contrast as well as computed tomography angiogram of head and neck were completed and were unremarkable. Three hours later, the patient had another episode of right facial droop and left-sided weakness, followed by new-onset slurring of speech, resolving in 5 minutes. Magnetic resonance imaging of the brain showed no infarcts or intracranial hemorrhage, but it did show increased peripontine enhancement with several nodular enhancements in the basilar area suspicious for coccidioma (Figure 1). Lumbar puncture demonstrated opening pressure of 140 mm H2O, white blood cells 240 (34% lymphocytes, 39% monocytes, 18% neutrophils, 4% eosinophils, and 5% basophils), elevated protein 127 mg/dL (normal = 14-45 mg/dL), glucose 38 mg/dL (normal = 40-75 mg/dL), and coccidioidal compliment fixation titer of 1:4 diagnostic of coccidioidal meningitis. Serum coccidioidal immunodiffusion IgM and IgG were reactive with a compliment fixation titer of 1:16 (Table 1). He had a total of 4 cerebrovascular TIAs that were increasing in intensity and symptomology. He was placed on fluconazole 1000 mg daily1 and a dexamethasone 20 mg daily for 7 days then tapered by 4 mg every 4 days.3 He was discharged to be followed in clinic.
Figure 1.
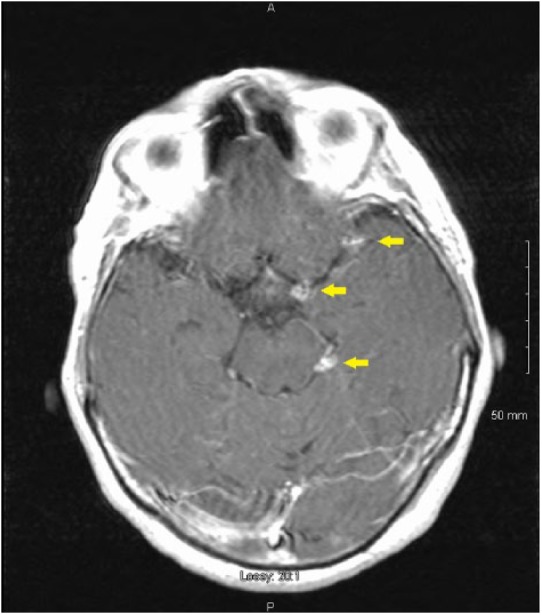
T1-weighted magnetic resonance image with gadopentetate dimeglumine contrast showing several nodular enhancements in the left peripontine area suspicious for coccidioma (arrows) in patient with multiple consecutive crescendo cerebrovascular transient ischemic attacks.
Table 1.
Laboratory Results Summary. Serum serology at 2-month postdischarge were from a hospital visit for skin and soft tissue infection of left ankle unrelated to coccidioidomycosis.
| Laboratory Test | 2 Years Prior | Presenting Studies | 2-Month Hospital Visit | 4-Month Follow-up | Normal Range |
|---|---|---|---|---|---|
| CSF WBC | 240 cells/cm2 | 50 cells/cm2 | <5 cells/cm2 | ||
| CSF protein | 127 mg/dL | 66 mg/dL | 15-45 mg/dL | ||
| CSF glucose | 38 mg/dL | 43 mg/dL | 40-75 mg/dL | ||
| CSF CF | 1:4 | <1:1 | <1:1 | ||
| Serum IgM | Weakly reactive | Very weakly reactive | Not reactive | Not reactive | Not reactive |
| Serum IgG | Weakly reactive | Reactive | Reactive | Reactive | Not reactive |
| Serum CF | 1:4 | 1:16 | 1:4 | 1:8 | <1:1 |
Abbreviations: CSF, cerebrospinal fluid; WBC, white blood cell; CF, compliment immunofixation titer; IgM/IgG, immunoglobulin immunodiffusion serology.
He had been and continues to be compliant with fluconazole therapy. At 2-month hospital visit for skin and soft tissue infection of left ankle unrelated to coccidioidomycosis, serum coccidioidal fixation titers were improved to 1:4. At 4-month follow-up, the patient had been asymptomatic. Lumbar puncture in office demonstrated white blood cell count of 50 (81% lymphocytes, 16% monocytes, 1% neutrophils, 1% eosinophils, and 1% basophils), protein 66 mg/dL (normal = 15-45 mg/dL), glucose 43 (normal = 40-75 mg/dL), and coccidioidal fixation titer of less than 1:1. However, serum coccidioidal fixation titers were 1:8 (Table 1).
Discussion
To our knowledge, this is the first reported case of multiple consecutive cerebrovascular TIAs that were increasing in intensity and symptomology with each attack as the presenting manifestation of coccidioidal meningitis.4 Presenting characteristics are recurrent episodes of sudden discrete neurological symptoms that completely resolve within 24 hours that repeat with increasing duration, frequency, and severity indicative of critical narrowing of the involved artery.5 This patient had 3 coccidiomas in the basilar meninges (Figure 1). Four episodes of transient neurological deficits were documented. The coccidioidal meningitis with associated transient vasculitis was treated conservatively with fluconazole 1000 mg1 and a dexamethasone taper.3 Cerebrospinal fluid studies at 4 months showed treatment response. However, repeat serum serology at 2 and 4 months demonstrated persistent coccidioidomycosis (Table 1). Whenever logistically feasible, follow-up sooner than 4 months for CSF studies is ideal. There were no early indications of risk to dissemination at time of pulmonary coccidioidomycosis diagnosis. Physicians in areas endemic for coccidioidomycosis should be aware that cerebrovascular TIAs can be the initial presentation of coccidioidal meningitis.
Footnotes
Authors’ Note: This case report was presented as a poster at the 61st Annual Meeting of the Coccidioidomycosis Study Group in collaboration with the 7th International Coccidioidomycosis Symposium at Stanford University, California, on August 2017, as well as at the American Federation for Medical Research Western Medical Research Conference in Carmel, California, on January 2018. Views expressed in this article are our own and not the official position of the institutions listed.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval: Ethical approval to report this case was obtained from the Kern Medical Center Institutional Review Board (Study #17048).
Informed Consent: Informed consent for patient information to be published in this article was not obtained because patient or legal representative was not available in time for publication. The information in the investigator’s written request for “Waiver of Consent” coupled with the written research proposal disclosing the data use plan were reviewed by Kern Medical Center Institutional Review Board to determine that under the conditions of study approval, there should be minimal or less risk for exposure of patient identity. Kern Medical Center Institutional Review Board approved the request for the Waiver of Consent as part of its ethics approval of the study.
ORCID iD: Carlos D’Assumpcao  https://orcid.org/0000-0001-9967-9612
https://orcid.org/0000-0001-9967-9612
References
- 1. Galgiani JN, Ampel NM, Blair JE, et al. 2016 Infectious Diseases Society of America (IDSA) clinical practice guideline for the treatment of coccidioidomycosis. Clin Infect Dis. 2016;63:e112-e146. [DOI] [PubMed] [Google Scholar]
- 2. Johnson RH, Einstein HE. Coccidioidal meningitis. Clin Infect Dis. 2006;42:103-107. [DOI] [PubMed] [Google Scholar]
- 3. Thompson GR, 3rd, Blair JE, Wang S, et al. Adjunctive corticosteroid therapy in the treatment of coccidioidal meningitis. Clin Infect Dis. 2017;65:338-341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Williams PL, Johnson R, Pappagianis D, et al. Vasculitic and encephalitic complications associated with Coccidioides immitis infection of the central nervous system in humans: report of 10 cases and review. Clin Infect Dis. 1992;14:673-682. [DOI] [PubMed] [Google Scholar]
- 5. Spengos K, Panas M, Tsivgoulis G, Vemmos K, Sfagos K, Vassilopoulos D. Crescendo transient ischemic attacks due to middle cerebral artery stenosis. Cerebrovasc Dis. 2004;17:266-268. [DOI] [PubMed] [Google Scholar]