

Abstract
Background
Following up on previous work demonstrating the involvement of the transcription factor forkhead box M1 (FOXM1) in the biology and outcome of a high-risk subset of newly diagnosed multiple myeloma (nMM), this study evaluated whether FOXM1 gene expression may be further upregulated upon tumor recurrence in patients with relapsed multiple myeloma (rMM). Also assessed was the hypothesis that increased levels of FOXM1 diminish the sensitivity of myeloma cells to commonly used myeloma drugs, such as the proteasome inhibitor bortezomib (Bz) and the DNA intercalator doxorubicin (Dox).
Methods
FOXM1 message was evaluated in 88 paired myeloma samples from patients with nMM and rMM, using gene expression microarrays as measurement tool. Sources of differential gene expression were identified and outlier analyses were performed using statistical methods. Two independent human myeloma cell lines (HMCLs) containing normal levels of FOXM1 (FOXM1N) or elevated levels of lentivirus-encoded FOXM1 (FOXM1Hi) were employed to determine FOXM1-dependent changes in cell proliferation, survival, efflux-pump activity, and drug sensitivity. Levels of retinoblastoma (Rb) protein were determined with the assistance of Western blotting.
Results
Upregulation of FOXM1 occurred in 61 of 88 (69%) patients with rMM, including 4 patients that exhibited > 20-fold elevated expression peaks. Increased FOXM1 levels in FOXM1Hi myeloma cells caused partial resistance to Bz (1.9–5.6 fold) and Dox (1.5–2.9 fold) in vitro, using FOXM1N myeloma as control. Reduced sensitivity of FOXM1Hi cells to Bz was confirmed in vivo using myeloma-in-mouse xenografts. FOXM1-dependent regulation of total and phosphorylated Rb agreed with a working model of myeloma suggesting that FOXM1 governs both chromosomal instability (CIN) and E2F-dependent proliferation, using a mechanism that involves interaction with NIMA related kinase 2 (NEK2) and cyclin dependent kinase 6 (CDK6), respectively.
Conclusions
These findings enhanced our understanding of the emerging FOXM1 genetic network in myeloma and provided preclinical support for the therapeutic targeting of the FOXM1-NEK2 and CDK4/6-Rb-E2F pathways using small-drug CDK and NEK2 inhibitors. Clinical research is warranted to assess whether this approach may overcome drug resistance in FOXM1Hi myeloma and, thereby, improve the outcome of patients in which the transcription factor is expressed at high levels.
Electronic supplementary material
The online version of this article (10.1186/s12885-018-5015-0) contains supplementary material, which is available to authorized users.
Keywords: Plasma-cell neoplasm, Targeted cancer therapy, Small-drug inhibitor, Cellular senescence
Background
With an estimated 30 thousand cases annually, newly diagnosed multiple myeloma (nMM) is the second most common blood cancer in the United States [1]. MM is a neoplasm of immunoglobulin-producing plasma cells that reside in the bone marrow. Quintessential disease manifestations include serum M-spikes (paraproteins), lytic bone lesions, hypercalcemia and renal insufficiency [2]. Owing to both newly developed myeloma drugs and the continuous refinement of therapeutic regimens that combine high-dose chemotherapy (HDT) with autologous hematopoietic stem cell transplantation (ASCT), the outcome for patients with nMM has significantly improved in recent years [3] – making it possible, at long last, to cure a tangible number of patients [4]. However, in the great majority of cases, following a period of successful therapy, myeloma relapses as a drug-refractory aggressive disease that leaves few, if any, therapeutic options. The unmet medical need of relapsed multiple myeloma (rMM) warrants dedicated research to enhance our understanding of the underlying pathways and identify new molecular targets for the design and testing of novel treatment approaches.
Although potent myeloma treatments, particularly proteasome inhibitors (PIs) and immunomodulatory drugs (IMiDs), have given the means to durable responses and prolonged survival of patients with myeloma, the inevitable relapse with drug-resistant disease is all too common. The root cause of acquired drug resistance in rMM is poorly elucidated, yet increasing evidence points to the involvement of a complex population dynamic of neoplastic myeloma growth [5] characterized by competition of co-existing tumor cell clones that eventually give rise to a dominant treatment-refractory clone able to thrive under conditions of strong drug-induced selective pressure. Genetic and genomic studies have shown that the evolutionary process sketched out above is driven by point mutations in drug response and other genes [6], copy number alterations that can abrogate tumor suppressor pathways [7] and changes in the epigenome that can reshape phenotypic and functional features of myeloma cells by virtue of affecting gene expression [8]. Another driver of the intricate pathophysiology of rMM is the bone marrow microenvironment, which provides tumor-promoting interactions with resident bone cells and the innate and adaptive immune system [9]. Increased cancer stemness may also be involved [10], the annoying elusiveness of bona fide myeloma stem cells notwithstanding.
Heartened by recent findings on the key role of the transcription factor, forkhead box M1 (FOXM1), in the genetic network of myeloma [11], we here continue with previous studies on the impact of FOXM1 in nMM [12] and rMM [13] and show that acquisition of drug resistance may be an important mechanism by which FOXM1 facilitates disease progression and relapse. Upregulation of FOXM1 rendered human myeloma cell lines (HMCLs) in continuous in vitro culture partially resistant to the PI, bortezomib (Bz), and the DNA intercalator, doxorubicin (Dox). In agreement with that was the in vivo result that enforced expression of FOXM1 in a HMCL designated CAG reduced the sensitivity of myeloma-in-mouse xenografts to Bz. We also provide evidence that FOXM1, presumably by virtue of its interaction with the retinoblastoma (Rb) cell cycle progression and tumor suppressor protein, promotes β-galactosidase (β-gal+) activity in myeloma – the classic Rb-regulated phenotype of cellular senescence that is mechanistically linked to relapsed cancer by means of acquired drug resistance, cancer dormancy and cancer stemness [14]. The result of this study adds strength to the contention that the therapeutic targeting of FOXM1 may benefit patients with myeloma in which the transcription factor is strongly expressed.
Methods
FOXM1 expression in myeloma and treatment of patients with myeloma
Levels of FOXM1 mRNA in myeloma cells were determined using Affymetrix U133Plus 2.0 microarrays (Santa Clara, CA) as previously described [15, 16]. Statistical analysis of microarray data relied on GCOS1.1 software (Affymetrix, Santa Clara, CA). Patients at UAMS were treated using the Total Therapy 2 regimen, the backbone of which is high-dose melphalan therapy (HDT) and autologous stem cell transplantation (ASCT). Half of the patients received thalidomide both during intensive therapy and as maintenance therapy. The therapeutic approach to relapsing disease was not uniform and depended mainly on the time to relapse, the pace of relapse (slow versus aggressive), the presence or absence of organ dysfunction, and the patient’s overall health status, physical and mental fitness and treatment preference.
Human myeloma cell lines (HMCLs), myeloma drugs, and other agents
Four IgA-producing HMCLs, designated CAG, XG1, H929 and ARP1, were included in this study. The identity of the cell lines was validated as previously described [12], using chromosomal translocation status and gene expression spikes as main parameters. Cells were propagated in vitro at 37 °C and 5% CO2 using RPMI1640 cell culture medium (Gibco) supplemented with 10% heat-inactivated fetal bovine serum (Atlanta Biologicals) and antibiotics (100 units/mL penicillin and 100 μg/mL streptomycin, Sigma). In some experiments, CAG and XG1 cells over-expressing FOXM1 (FOXM1Hi) were compared to cells containing normal amounts of FOXM1 (FOXM1N) [12]. In other experiments, H929 and ARP1 cells in which FOXM1 expression had been knocked down using shRNA (FOXM1Lo) were compared to parental FOXM1N cells [12]. Chemicals including myeloma drugs were purchased from Sigma (doxorubicin [Dox], thiostreptone [TS]), Millennium Pharmaceuticals (bortezomib [Bz]), or Invitrogen (propidium iodide, RNase A).
In vitro assays using HMCLs
For cell cycle analysis, cells were fixed in ice-cold ethanol (1 h, 4 °C), washed in PBS, re-suspended in propidium iodide (PI) solution (40 μg/ml, 3 h, 4 °C) supplemented with 50 μl RNase A (10 μg/ml), and evaluated by flow cytometry using a FACScan (Becton Dickinson, San Jose, CA). For determination of clonogenicity, 104 myeloma cells were seeded in soft-agar plates (0.5 ml RPMI1640 supplemented with 0.33% agar and 10% FBS) and grown for 2 weeks at 37 °C and 5% CO2 – in some cases exposed, during week 2, to myeloma drugs. Myeloma clones, defined as tight aggregates of ≥40 tumor cells, were enumerated on digital images of soft-agar plates analyzed with the help of Image J. For measurement of proliferation and viability, cells were counted using a hemocytometer and evaluated for exclusion of trypan blue (0.4% dye in PBS, pH 7.3), respectively. For determination of apoptosis, the flow-cytometric Annexin V APC assay (eBioscience, San Diego, CA) was used according to the manufacturer’s instructions. For determination of drug-efflux capacity, the flow-cytometric eFluxx-ID™ multidrug resistance assay was employed. MCF7 human breast cancer cells were included as benchmark. For determination of senescence-associated β-galactosidase (β-gal) activity, a kit from Cell Signaling Technology (Cat# 9860) was used. Briefly, cells were fixed (15 min), washed (PBS) and incubated in β-gal staining solution overnight at 37 °C.
Western blotting
Protein levels were determined by Western analysis using antibodies to FOXM1, Rb and pRb obtained from Santa Cruz Biotechnology (FOXM1, sc-500) or Cell Signaling Technology (Rb, 9309; pRb, 8515). Cells were lysed with assistance of the Mammalian Cell Extraction kit (K269–500) from Biovision, Milpitas, CA. 10-μg samples of protein were fractionated on 4–12% SDS-PAGE gels, followed by transfer to nitrocellulose membranes blocked with 5% non-fat dry milk in Tris-buffered saline containing 0.05% Tween-20. Incubation with primary antibodies occurred overnight at 4 °C. Proteins were visualized using HRP-conjugated secondary antibody and SuperSignal West Pico (Pierce, Rockford, IL). Membranes were subsequently stripped and re-probed for β-actin (Santa Cruz Biotechnology, sc-47778), which served as loading control.
HMCL xenografting in NSG mice
To compare the drug response in CAG myeloma cells expressing normal and elevated FOXM1 levels, respectively, 2 × 106 FOXM1N and FOXM1Hi cells were injected subcutaneously (SC) into the right or left flank of NSG mice (Jackson Laboratory, Bar Harbor, Maine). Viability of FOXM1N and FOXM1Hi cells was comparable (≥90%). Seven days later, one group of mice was treated with bortezomib (1 mg/kg) administered intraperitoneally (IP) twice weekly. Another group of mice, designated untreated control, was injected with drug vehicle, normal saline (0.9% sodium chloride). In all cases, tumor growth was measured using a pair of calipers. Mice were sacrificed for humane reasons using CO2 asphyxiation when tumors reached 20 mm in diameter. All studies were approved under protocol 1301010 of the Institutional Animal Care and Use Committee of the University of Iowa.
Statistical analysis
Two-tailed Student’s t-test was used to compare two experimental groups, employing parametric or non-parametric methods in case data were normally distributed or not, respectively. One-way analysis of variance (ANOVA) was used to evaluate more than two groups. To compare drug responses in mice, linear regression and AUC (area under curve) determination were used. For all analyses, the GraphPad Prism 7 software package (La Jolla, CA) was employed and p ≤ 0.05 was considered significant.
Results
FOXM1 message is elevated in most but not all relapsed myelomas
Using the University of Arkansas for Medical Science (UAMS) Total Therapy 2 (TT2) dataset (GSE2658) as discovery tool, we recently reported that upregulation of FOXM1 was a common feature of patients with rMM [13]. Here we confirm this finding with the help of an updated TT2 dataset that includes 127 patients with rMM and a related TT3 dataset that includes 30 patients with rMM – both available at GSE31161 (Fig. 1a). The increase in median FOXM1 mRNA levels in these datasets, 2.7-fold in case of TT2 (76/28) and 2.3-fold in case of TT3 (330/143), was very similar to the one observed in the original TT2 dataset (2.89-fold; 79.5/27.5). Furthermore, in all 3 datasets, mean FOXM1 expression at relapse was significantly elevated (p = 10− 3) compared to baseline. Next, we went back to the TT2 / GSE2658 dataset, presented in dot plot format in Fig. 1b, to visualize the two expression values, ND vs R, for each patient. Upregulation of FOXM1 mRNA at relapse was seen in more than two thirds of patients (61 of 88, 69%; indicated by dots above the diagonal line), whereas gene message was down in 20 (23%) patients (dots below the line) and unchanged in 7 (8%) patients (dots on the line). The magnitude of the elevation at relapse (~ 2.6-fold; 226/87.8) was similar to the decline (~ 2.3-fold; 151/64.6) using mean expression levels for comparison. These results indicated that the overall increase of FOXM1 message at relapse was caused by the preponderance of myelomas with elevated gene expression (69%), not by the circumstance that the magnitude of elevation exceeded that of reduction.
Fig. 1.

FOXM1 message levels in paired samples of new and relapsed myeloma. a FOXM1 message is elevated in relapsed myeloma in UAMS datasets. Shown are box plots of FOXM1 mRNA levels from Total Therapy 2 (TT2) and Total Therapy 3 (TT3) datasets. For each dataset, FOXM1 expression at baseline in newly diagnosed disease (ND) is compared to relapsed disease (R). Median FOXM1 expression is indicated by a black horizontal line within the box. The 25th and 75th percentiles are indicated by lower and upper horizontal lines, respectively. Number of patients and median FOXM1 expression are given at the bottom. Statistical comparisons relied on the Mann-Whitney test. b Dot plot of paired ND and R myelomas (n = 88) from the TT2 / GSE2658 dataset. Dots above (n = 61) and below (n = 20) the black horizontal line indicate up- and down-regulation of FOXM1 at relapse, respectively. Dots on that line (n = 7) represent patients with no change. Four R myelomas featuring a more than 20-fold elevation of gene message and five R myelomas exhibiting a more than 6-fold drop in gene expression are denoted by red and blue ellipse, respectively. These cases are also singled out in panels D and F, respectively. c Source of elevated FOXM1 at relapse. Shown is the breakdown of 61 myelomas with heightened levels of FOXM1 at relapse in two groups distinguished by lower (left) and higher (right) baseline expression. d Outliers with peak expression levels at relapse. Four myelomas exhibiting increases by more than 20-fold are indicated by black ellipse. e Source of decreased FOXM1 at relapse. Shown is the breakdown of 20 myelomas with reduced FOXM1 expression at relapse in two groups distinguished by lower (left) and higher (right) baseline expression values. f Outliers with steep drops in gene expression at relapse. Five myelomas exhibiting decreases by more than 6-fold are indicated by black ellipse
Outlier analysis of FOXM1 expression in rMM
To analyze the 61 myelomas that harbored elevated FOXM1 at relapse in greater depth, we partitioned these cases in two arbitrary groups defined by median baseline expression levels of 19 microarray units (n = 46) and 85 units (n = 15), respectively, in newly diagnosed (ND) disease (Fig. 1c, black boxes with whiskers). The increase at relapse in the low expresser group was somewhat higher (4.7-fold, 89.5/19) than in the high expresser group (4.1-fold, 346/85). The difference was due, in no small measure, to four myelomas in the low expresser group that exhibited > 20-fold elevated expression peaks at relapse. This is indicated by a black ellipse in Fig. 1d. The analysis of tumors featuring reduced FOXM1 expression at relapse is depicted in Fig. 1e. Partitioning of the dataset (n = 20) in two groups with median baseline expression of 27.5 units (n = 12) and 343 units (n = 8) at the time of diagnosis (ND) demonstrated that the decrease in the high expresser group was more pronounced (6.2-fold, 343/55) than in the low expresser group (1.2-fold, 27.5/23; Fig. 1e). The difference could be attributed in large part to a subset of myelomas in the high expresser group (n = 5) that exhibited > 6-fold drops in gene expression at relapse (Fig. 1f, black ellipse). These findings led us to conclude that the pattern of FOXM1 expression in rMM is heterogeneous, with outliers in both directions contributing disproportionally to the relapse-dependent shift in gene expression. To confirm the findings presented in Fig. 1 with an independent method not relying on Affymetrix arrays, we used RT-PCR to analyze sequential ND and R CD138+ bone marrow tumor samples from 8 patients with myeloma undergoing HDT/ASCT therapy. Although the number of clinically confirmed relapses was low (n = 3), the increase in FOXM1 expression was impressive, up to 35-fold (Additional file 1: Figure S1).
FOXM1 promotes proliferation and drug efflux activity of myeloma cells
To assess the biological outcomes of elevated FOXM1 in MM, we relied on two HMCLs, XG1 and CAG, as experimental model system. The cells were manipulated to contain either elevated levels of FOXM1 (FOXM1Hi) or normal levels of gene message and protein (FOXM1N) due to transfection with a human FOXM1 (isoform C) expressing lentivirus or a non-coding “empty” lentivirus (used as control), respectively [12] (Fig. 2a). Flow cytometric determination of cell proliferation showed that upregulation of FOXM1 promotes cell cycle progression (Fig. 2b). FOXM1Hi CAG and XG1 cells exhibited 14 and 13% higher growth rates, respectively, compared to FOXM1N cells (compare columns labeled “Co”). Treatment of cells with the FOXM1-inhibiting thiazole antibiotic, thiostrepton (TS) [17], slowed the growth of both FOXM1Hi and FOXM1N cells. However, the low Hi-to-N ratio indicated that FOXM1Hi cells were more sensitive to TS than FOXM1N cells (columns labeled “TS”). Figure 2c depicts an example of the magnitude of TS-dependent growth inhibition of FOXM1Hi cells under conditions of higher drug concentration compared to panel B. The decrease in proliferation amounted to 72% (4.72/16.9) in case of CAG cells (left panel) and 76% (6.40/26.1) in case of XG1 cells (right panel). The results presented above were in line with genetic evidence gleaned from transcriptomic studies using microarrays, indicating that FOXM1 promotes myeloma proliferation. Thus, FOXM1 expression is positively correlated (Pearson’s r = 0.712, p < 10− 4) with myeloma cell proliferation in 244 Bz-treated patients available at GSE9782 [18], using the global gene expression-based proliferation index (GPI) of myeloma devised by Bergsagel et al. [19] as proxy of actual tumor cell proliferation (Fig. 2d). Similarly, we recently reported [13] that FOXM1 message levels in nMM and rMM paralleled the GPI of developed by Hose and his associates [20]. Next, we used eFluxx-ID Gold MDR analysis to demonstrate that upregulation of FOXM1 results in enhanced ABC-transporter efflux-pump activity in myeloma (Fig. 2d). This finding suggested that FOXM1-dependent promotion of cell cycle progression in myeloma may facilitate drug resistance by means of enhanced outflow of myeloma drugs.
Fig. 2.
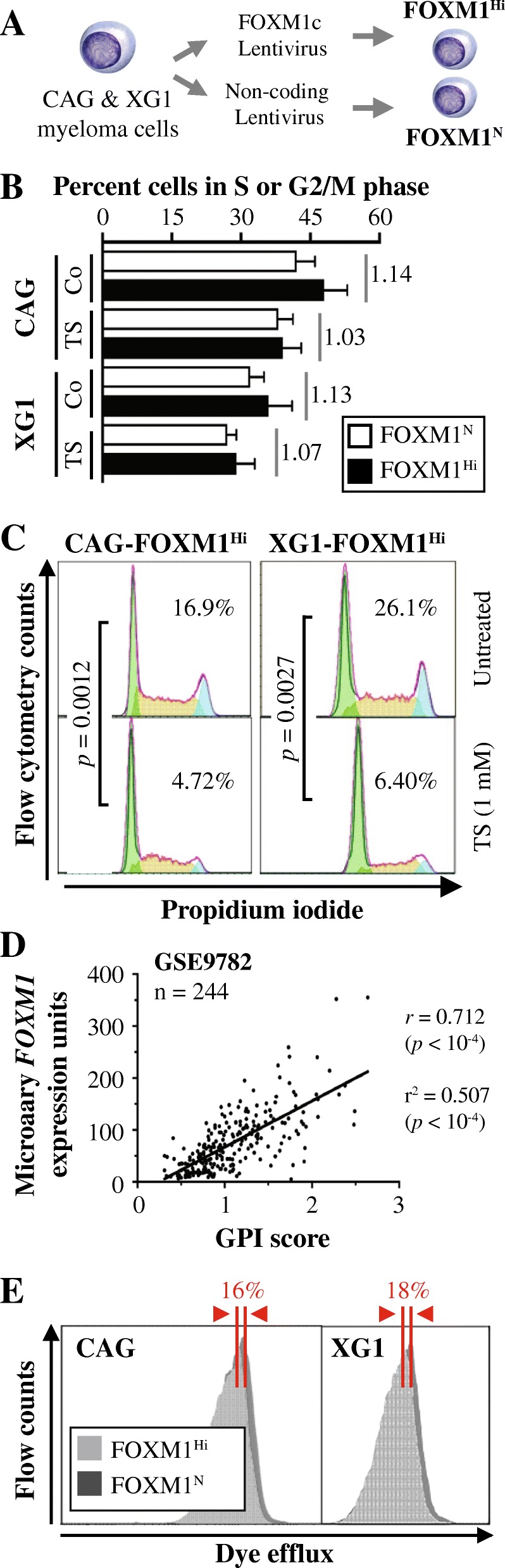
Constitutive overexpression of FOXM1 promotes growth and survival of myeloma cells in vitro. a Scheme of study design. FOXM1Hi and FOXM1N myeloma cells were generated using lentiviral gene transduction. Two HMCLs, designated CAG and XG1, were used. FOXM1 message levels in FOXM1Hi cells, relative to normal levels in FOXM1N cells, were significantly elevated in both CAG cells (~ 15 fold) and XG1 cells (~ 6-fold). FOXM1 protein levels were only moderately increased: ~ 50% and ~ 30% in CAG and XG1 cells, respectively. See Figure 4a in reference [12] for details. b Bar diagrams depicting percent FOXM1Hi and FOXM1N XG1 and CAG cells in S or G2/M phase of the active cell cycle. Cells were treated with thiostrepton (TS) or left untreated for use as control (Co). The result is consistent with the analysis of cell proliferation in Figure 4b of reference [12], showing that after 1 week in cell culture, the number of viable, actively proliferating FOXM1Hi cells was significantly higher than that of FOXM1N cells. c Cell cycle fractions determined by flow cytometry. Treatment of cells using thiostrepton (TS) resulted in a significant drop in cell proliferation, using two-way ANOVA for comparison. d Scatter plot demonstrating positive correlation of FOXM1 expression and myeloma proliferation in 244 Bz-treated patients from the Mayo Clinic. Tumor cell proliferation was scored with the assistance of a gene expression-based proliferation index (GPI) developed by Bergsagel et al. [20]. e Flow cytometric dye efflux histograms of CAG cells (left) and XG1 cells (right), demonstrating heightened ABC transporter drug pump activity in FOXM1Hi cells relative to FOXM1N cells. Percent differences in mean fluorescence intensity (MFI) were 16% in case of CAG and 18% in case of XG1
Enforced expression of FOXM1 lessens sensitivity to myeloma drugs in vitro
Because recurrent cancers including rMM may acquire therapy resistance due to alterations in biological pathways in which FOXM1 is involved [21], we wondered whether upregulation of FOXM1 may decrease the sensitivity of myeloma cells to widely used myeloma drugs, such as bortezomib (Bz) and doxorubicin (Dox). We found that enforced expression of FOXM1 renders myeloma partially resistant to both drugs, as evidenced by half-maximal inhibitory concentrations (IC50) that, in case of Bz, were 5.6-fold (CAG) and 1.9-fold (XG1) higher in FOXM1Hi than FOXM1N cells (Fig. 3a, left). In case of Dox, they were 2.9-fold (CAG) and 1.5-fold (XG1) higher (Fig. 3a, right). Flow cytometric measurements of annexin V, a marker of apoptosis, were in agreement with these results as FOXM1Hi cells invariably exhibited less drug-induced death than FOXM1N cells did. For example, there was a 2.7-fold difference in CAG cells treated with Bz (23% vs. 63%) and a 1.5-fold difference in XG1 cells treated with Dox (49% vs. 72%, Fig. 3b). Determination of myeloma growth in soft agar demonstrated the clonogenic advantage of FOXM1Hi cells. One example, depicted in Fig. 3c, shows that FOXM1Hi CAG cells treated with 2 nM Bz or left untreated produced ~ 50% (right panels) or ~ 25% more colonies (left panels), respectively, than FOXM1N controls. XG1 cells demonstrated greater differences based on Hi-to-N ratios (Fig. 3d), suggesting that FOXM1 protects the clonogenic growth of these cells under conditions of selective drug pressure even more effectively than that of CAG cells. These findings were of interest in light of published reports that suppression of FOXM1 may sensitize human cancer to killing by genotoxic drugs [22].
Fig. 3.
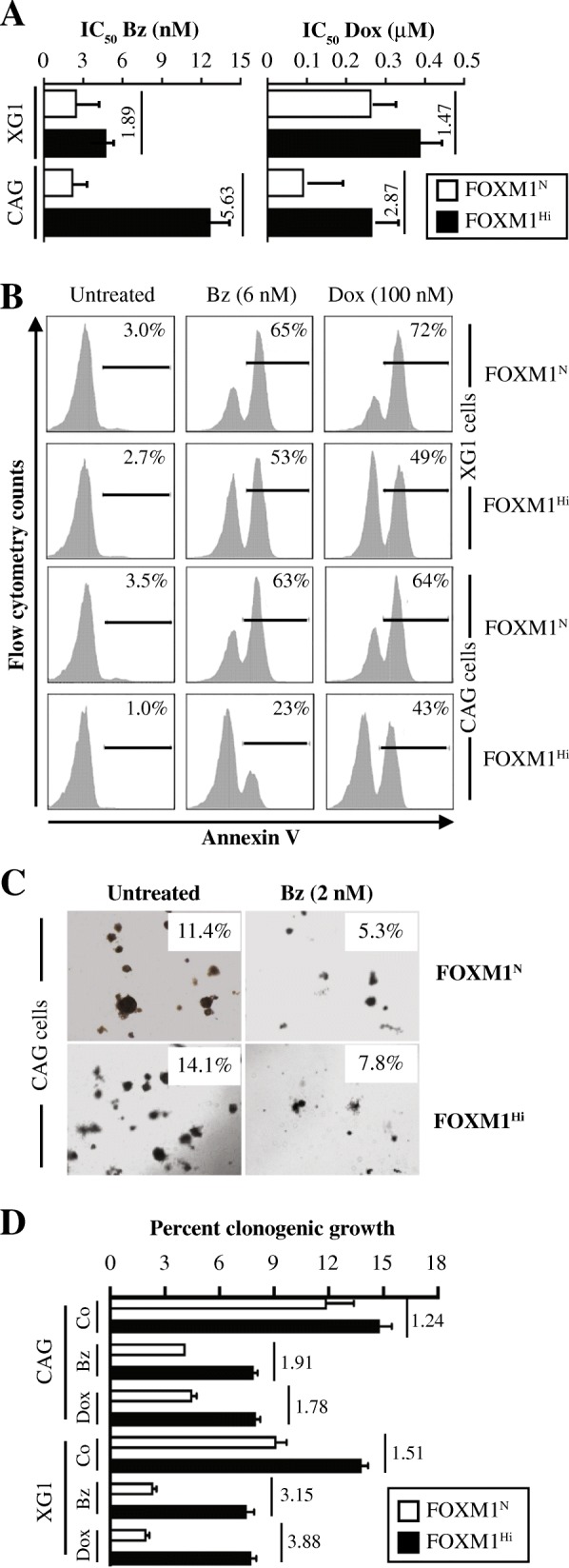
Upregulation of FOXM1 promotes drug resistance of myeloma in vitro. a Bar diagram depicting the half maximal inhibitory concentrations (IC50) of bortezomib (Bz) and doxorubicine (Dox) in XG1 and CAG myeloma cells expressing elevated (FOXM1Hi) or normal (FOXM1N) levels of the transcription factor. Cells were grown for 1 week in bulk suspension culture in presence of a log2 dose range of either drug. IC50 was determined using non-linear regression analysis of dose response curves (GraphPad Prism 7 software). Hi-to-N ratios of IC50 (indicated by vertical short lines and numbers) reflect the magnitude by which overexpression of FOXM1 reduced drug-induced cell killing. b Representative flow histograms comparing levels of drug-induced apoptosis in paired FOXM1Hi/FOXM1N samples of XG1 (upper half) and CAG (lower half) cells treated with 6 nM Bz (center column) or 0.1 μM Dox (right column). Cells left untreated were used as control (left column). APC (allophycocyanin)-conjugated antibody to annexin V was used to determine the fraction of cells undergoing apoptosis (indicated as percentages above black horizontal lines). In all cases, death was attenuated by enforced expression of FOXM1. c Photographic images of soft-agar plates containing colonies of FOXM1Hi and FOXM1N CAG myeloma cells. Cells were treated with the indicated dose of bortezomib or left untreated. Clonogenic growth expressed as percentage of cells able to form colonies is given in the insets. d Bar diagram depicting soft-agar clonogenicity of FOXM1Hi/FOXM1N CAG or XG1 cells treated with 2 nM Bz or 0.1 μM Dox. Cells left untreated were used as control (Co). The Hi-to-N ratios of the average colony numbers, determined in triplicate experiments, are indicated by vertical numbers next to vertical lines. The ratios reflect the extent by which overexpression of FOXM1 mitigated drug-dependent inhibition of clonogenic growth
Elevation of FOXM1 leads to reduced sensitivity of myeloma xenografts to Bz
To complement the in vitro findings described above with in vivo data, we determined whether upregulation of FOXM1 results in decreased susceptibility of myeloma to proteasome inhibition (PI). We used human-in-mouse myeloma xenografts treated with Bz or left untreated (control) as model system. FOXM1Hi and FOXM1N CAG cells were transferred under the skin of the left and right flank of NSG mice (n = 10), respectively. Treatment of 5 tumor-bearing hosts using daily IP injections of Bz commenced 7 days later. Five tumor-bearing hosts left untreated were used as controls (Fig. 4a). Tumor diameters were measured in 4-day intervals to compare xenograft growth rates. FOXM1Hi tumors harvested on day 30 (study endpoint) were larger than their FOXM1N counterparts in both the Bz treatment arm (15.2 ± 1.97 mm vs 10.4 ± 0.771 mm) and the control arm (19.0 ± 1.31 mm vs 14.0 ± 1.73 mm) arm (Fig. 4b). This was consistent with FOXM1’s growth-promoting activity described above. However, in terms of sensitivity to PI, FOXM1Hi tumors were slightly less responsive (by 10%) than their FOXM1N counterparts on the contralateral side of the same host. Specifically, Bz-dependent growth inhibition of FOXM1Hi tumors at study endpoint (1.32 ± 0.434 g in treated mice vs. 2.40 ± 0.647 g in mice left untreated) amounted to 45%, whereas that of FOXM1N tumors (0.692 ± 0.217 g treated vs 1.54 ± 0.543 g untreated) amounted to 55% (Fig. 4c). This result, however modest it might be, was consistent with published findings that lowering FOXM1 in human cancer cells leads to enhanced PI-induced killing [23].
Fig. 4.
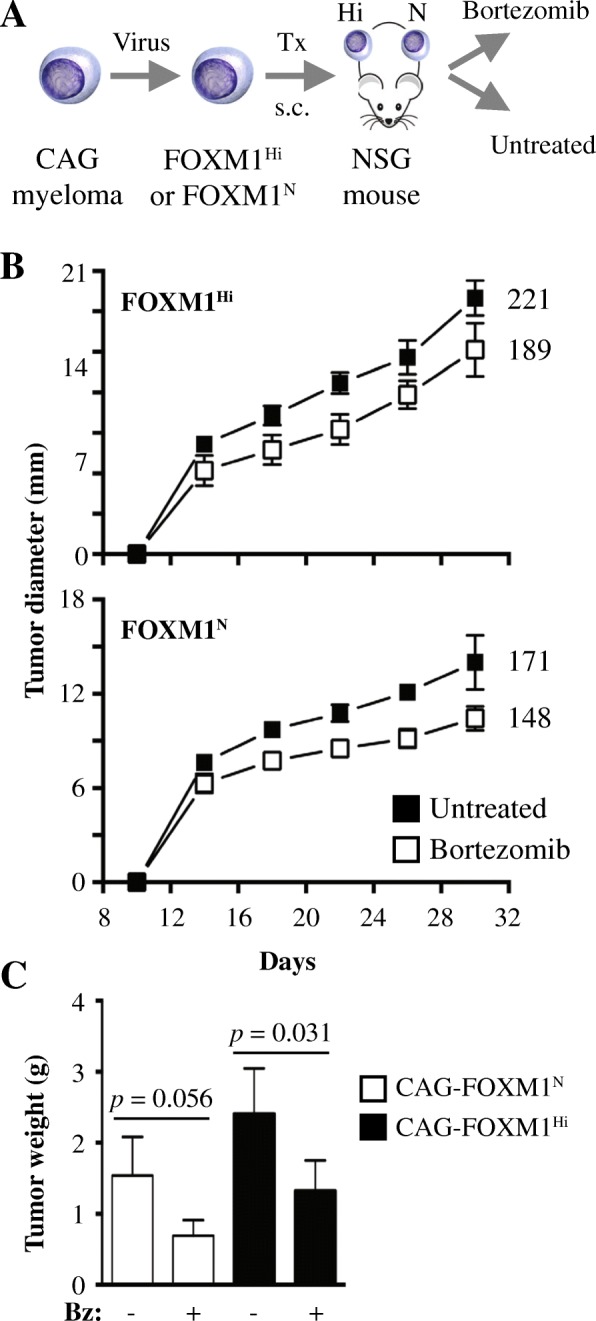
Upregulation of FOXM1 reduces susceptibility of myeloma xenografts to bortezomib in vivo. a Scheme of study design. FOXM1Hi and FOXM1N myeloma cells were generated using lentiviral gene transduction as previously described [12]. Cells were subcutaneously (s.c.) xenografted (Tx) into the right and left flank of NSG mice, respectively. Beginning on day 7 following cell transfer, 5 mice were treated with daily administrations of the proteasome inhibitor, bortezomib (Bz, 1 μg per gram body weight IV), until study termination on day 30. Five mice were left untreated. In all cases, tumor diameters were measured in 4-day intervals using a caliper, starting on day 10 after xenografting. Xenografts were harvested and weighed on a fine balance at study end. b Time course of tumor growth in host mice. Mean tumor diameters (squares) and standard deviations of the mean (short vertical lines with error bars) are plotted. In Bz-treated mice, the area under the curve (AUC) of FOXM1N tumors (148) was 13% smaller than that of FOXM1Hi (171) tumors. In untreated mice, the AUC of FOXM1N tumors (189) was 14% smaller than that of the FOXM1N (221) tumors. c Mean tumor weight at end of study. FOXM1Hi xenografts treated with Bz (1.32 ± 0.434 g) were significantly smaller than their untreated counterparts (2.40 ± 0.647 g) using Mann-Whitney’s t test (p = 0.031). FOXM1N xenografts showed the same trend (1.54 ± 0.543 g vs. 0.692 ± 0.217 g) but missed the 5% threshold of statistical significance (p = 0.056). Median tumor weights in all 4 groups were significantly different by Kruskall-Wallis analysis (p = 0.006)
Binding of FOXM1 to Rb may promote senescence of myeloma cells
Our recent work has implicated the cyclin-dependent kinase 6 (CDK6) / retinoblastoma (Rb) axis in the mechanism by which FOXM1 promotes myeloma [14]. To confirm the co-regulation of FOXM1 protein levels and the tumor suppressor, Rb, in myeloma, we performed triplicate Western analyses of paired FOXM1Hi and FOXM1N tumors (Fig. 5a, left). For sake of comparison to FOXM1Hi, we included FOXM1Lo samples from H929 and ARP1 HMCL cells, in which FOXM1 had been knocked down using lentivirus-delivered RNA interference (Fig. 5a, right). Densitometric analysis of Western blots showed that total Rb and phosphorylated Rb (pRb) were increased in FOXM1Hi cells by 20–40%, with somewhat higher levels seen in XG1 than CAG cells (Fig. 5b, left). Conversely, Rb and pRb were decreased in FOXM1Lo cells (~ 30 to 50%), with the loss of the latter somewhat exceeding that of the former (Fig. 5b, right). Inspired by a large body of evidence that connects the Rb-governed cell fate decision of senescence with important pathways of cancer relapse such as drug resistance, tumor dormancy and tumor stemness [14], we determined whether myeloma cells might express the classic senescence-associated phenotype of β-galactosidase in a FOXM1-dependent manner. Fig. 5c, left shows that FOXM1 knockdown sufficed to induce β-gal activity in myeloma. Furthermore, treatment of cells using Dox caused higher β-gal+ scores in FOXM1N than FOXM1Hi cells (Fig. 5c, right). These findings were consistent with published reports on the role of FOXM1 in suppressing cellular senescence in a variety of solid and liquid neoplasms [24].
Fig. 5.
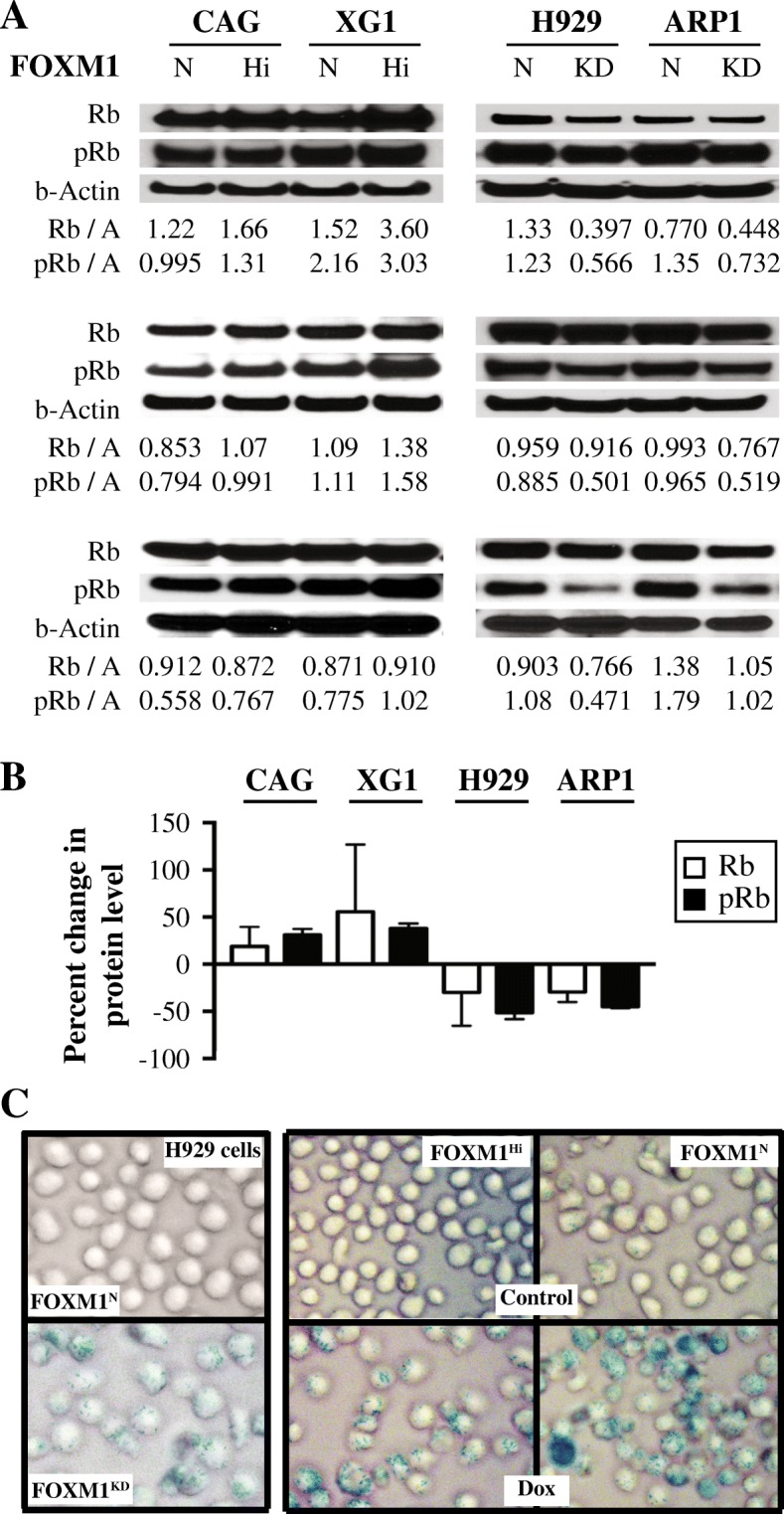
FOXM1/Rb-dependent expression of β-galactosidase in myeloma cells. a Co-immunoprecipitation (Co-IP) result indicating physical interaction of Rb and FOXM1 in CAG and XG1 myeloma cells. Immunoblots using a specific IgG antibody (Ab) to FOXM1 (following IP with Ab to Rb) or Rb (following IP with Ab to FOXM1) are shown on top of each other. The IgG isotype control is labeled “IgG.” Whole cell lysates not subjected to Co-IP (“Input”) were included as an additional control. b Shown on top is a Western blot of total Rb and its activated, phosphorylated form (pRb) in FOXM1Hi and FOXM1N CAG and XG1 myeloma cells. A similar blot containing samples of FOXM1KD and FOXM1N H929 and ARP1 myeloma cells is presented at bottom. The abundance of Rb and pRb, relative to β-actin, was determined using densitometry. The ratios are indicated below the blots. c The upper panel illustrates the elevation of β-galactosidase (β-gal) activity, a classic phenotype of cellular senescence, in FOXM1KD H929 cells (bottom) relative to FOXM1N controls (top). Cells were not treated with drug. This result was confirmed using paired FOXM1KD / FOXM1N ARP1 samples (not shown). Depicted in the lower panel is the increased proportion of β-gal+ XG1 cells following treatment with Dox. FOXM1Hi cells exhibited a lesser increase than FOXM1N cells (not shown). Cells were evaluated using an Olympus BX-51 Light Microscope equipped with an UPLSAPO objective (Olympus) of 40x magnification and 0.95 numerical aperture. The imaging medium was air. The light temperature of the microscope bulb varied between 3000 and 3400 K. Images were acquired with the help of a DP2 digital camera (Olympus) and DP2-BSW imaging software (Olympus), saved as TIF data files, and enhanced—with respect to brightness, contrast, and color balance—using the Adobe Photoshop CS2 Version 9.0.2 software (Adobe Systems, Inc)
Discussion
The main finding of this study is experimental evidence for a role of FOXM1 in advanced myeloma. The new results implicating FOXM1 in drug-resistant disease relapse and the β-gal+ phenotype of cellular senescence agree with the well-known pleiotropic function of the transcription factor in cancer cell biology [25]. In both solid and liquid cancers, FOXM1 governs a wide spectrum of biological processes, including cell cycle progression, DNA damage repair, self-renewal of stem cells [26] and senescence [24] – all involved in tumor progression and the response of malignancies to cytostatic and targeted treatments [27]. In regard to diverse biological functions attributable to FOXM1 in myeloma, the transcription factor seems to resemble well-established “master” transcription factors of myeloma, such as interferon regulatory factor 4 or IRF4 (a.k.a. MUM1) [28] and the myelocytomatosis oncoprotein MYC [29]. To further put FOXM1’s role in myeloma in perspective, it is helpful to recognize that this particular member of the large forkhead box family of proteins is critically involved in the development and outcome of other B-lineage neoplasms; e.g., acute lymphoblastic leukemia [30], diffuse large cell lymphoma [31], chronic lymphocytic leukemia [32] and follicular lymphoma [33]. What is more, an overarching impact of FOXM1 on cancer as a whole has been suggested by a recent pan-cancer meta-analysis of approximately 18 thousand gene expression signatures [34], which identified the FOXM1 regulatory network as a major predictor of adverse outcomes across 39 solid and hematologic malignancies including MM.
Although the molecular mechanism by which FOXM1 promotes drug resistance in myeloma has not yet been elucidated, FOXM1-dependent increases in cell proliferation, NEK2 (NIMA related kinase 2)-dependent CIN (chromosomal instability) and ABC-transporter drug-pump activity may be involved [12]. The latter has been repeatedly implicated in drug-resistant solid cancers; e.g., in retinoblastoma [35], bladder cancer [36] and colorectal cancer [37], in which the heightened drug-efflux activity could be functionally linked to FOXM1-dependent upregulation of ABCC4, ABCG2 and ABCC10, respectively. Also playing a role may be other pathways of drug resistance that operate in solid tumors [38]; e.g., inhibition of ubiquitination-dependent FOXM1 degradation via interacting proteins, such as OTUB1 (OTU deubiquitinase, ubiquitin aldehyde binding 1) [39]; crosstalk of FOXM1 with other cellular signal transduction pathways, such as HGF / Met (hepatocyte growth factor / Met proto-oncogene, receptor tyrosine kinase) [40] and AKT (AKT serine / threonine kinase 1) [41]; and metabolic changes that effect increased oxidative defense capacity, as seen in radio-resistant head and neck squamous cell carcinoma [42]. Targeting the interactions and pathways described above – perhaps in conjunction with targeting FOXM1 directly using established [43] or emerging [44] small-drug inhibitors – may afford the re-sensitization of relapsed FOXM1High myeloma to Bz and other drugs that were effective at earlier stages of myeloma therapy. A variety of molecularly targeted chemo-sensitization approaches of this sort are pursued in myeloma [45] – all attempting to build on findings in B-ALL that demonstrate that drug resistance in malignant B lymphocytes may be overcome by suppression of FOXM1 [46].
Several limitations of our study exist. First among these is the need to confirm the findings on FOXM1-dependent drug resistance in primary tumor cells. Sequential nMM → rMM samples of fractionated malignant bone marrow plasma cells obtained from patients with new and relapsed myeloma may lend themselves to that end. In this context, we should also acknowledge that our xenograft approach for testing the Bz response in vivo was not a true study of cancer relapse; instead, it merely assessed drug-dependent growth inhibition in vivo. Genetically engineered mouse models of human myeloma – in which spontaneously arising tumors can be put into remission using clinically relevant myeloma drugs, and the mice can be kept alive until relapsed tumors require salvage treatment – may mimic the situation of patients with rMM more accurately. Two validated mouse models, designated Vκ-Myc and IL6iMyc, are available for that purpose [47–50]. Another limitation of this study concerns the involvement of cellular senescence in drug-resistant myeloma. Although β-gal activity is a well-established phenotype of cellular senescence in many types of cancer including MM [51, 52], additional research is warranted to demonstrate the mechanistic link to the FOXM1-Rb pathway. Mechanisms of FOXM1-dependent senescence elucidated in neoplasms other than myeloma [53] include enhancement of Bmi-1 expression, as seen in the NIH3T3 model [54]; overexpression of miR-370, observed in AML [55]; and inhibition of the CDK4/6-FOXM1 axis by genetic means, such as enforced expression of miR-506 in ovarian cancer [56], or pharmacologic means, such as small-drug CDK inhibition in neuroblastoma [57].
Conclusion
We now know that FOXM1 is a high-risk myeloma gene in newly diagnosed patients [12] that undergoes further upregulation in the majority of cases upon tumor relapse [13]. FOXM1’s interaction in myeloma cells with NEK2 (NIMA-related kinase 2) and the CDK4/6-Rb-E2F axis [12, 13] is of interest from a therapeutic viewpoint because CDK inhibition may be effective in myeloma [12, 58–60]. Moreover, NEK2 – a well-established transcriptional target of FOXM1 in cancer [61, 62] that has been shown to drive drug resistance in myeloma and other malignancies [63–65] – can be targeted with the help of small compounds that inhibit kinase activity [66] or trigger target degradation indirectly by means of a mechanism that involves the disruption of NEK2 binding to the kinetochore complex component NDC80 / HEC1 [67]. Figure 6 depicts the emerging FOXM1 genetic network in myeloma. Small-drug inhibitors targeting this network may overcome drug resistance in tumors in which the transcription factor is highly expressed.
Fig. 6.
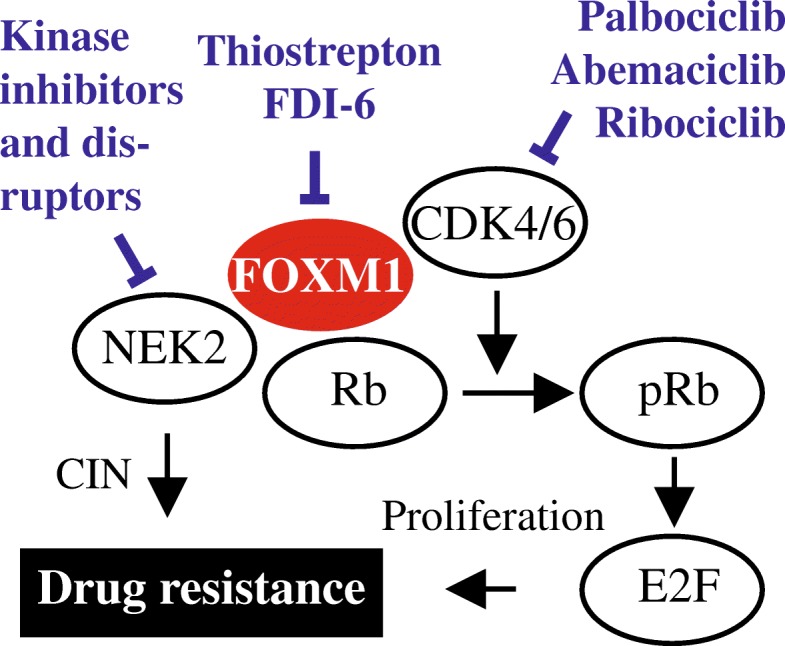
Therapeutic targeting of the FOXM1 genetic network in myeloma. FOXM1 is a proliferation-associated transcription factor that interacts in myeloma cells with the cyclin D-CDK4/6-Rb-E2F pathway, a key regulator of the G1-to-S cell cycle transition. The findings of this study demonstrate that, in addition to cell cycle progression, FOXM1 promotes drug resistance and, possibly, cellular senescence. Another interaction by which FOXM1 may desensitize myeloma to drug inhibition is NEK2. Small-molecule inhibitors of FOXM1, CDK4/6 and NEK2 are indicated. See main text for details
Additional file
Figure S1. Quantitative, reverse transcription (RT) polymerase chain reaction (qRT-PCR) analysis of FOXM1 gene expression in 8 myeloma patients for which 3 sequential CD138+ fractionated bone marrow tumor samples at baseline (white columns, newly diagnosed disease), initiation of HDT (high-dose therapy) and autologous hematopoietic stem cell transplantation (ASCT) therapy (grey columns) and consolidation / maintenance therapy (black columns) were available. In the course of the latter, three patiens (1, 2 and 8) and one patient (7) experienced a clinically significant and incipient FOXM1High relapse, respectively. Total RNA was extracted using Quick-RNA MiniPrep (Zymo Research) and reverse transcribed using oligo dT primers and SuperScript III RT (Invitrogen). Data analysis relied on the ΔΔCt method. Primers were purchased from Integrated DNA Technologies (Coralville, Iowa). Sequences are available upon request. All increases in FOXM1 gene expression are relative to the patient-specific baseline value, which was set at 1. All patients were consented in accordance with rules and regulations of the US Food and Drug Administration and the Declaration of Helsinki. Tumor samples were collected with institutional approval supplied with IRB 201503809 entitled “FOXM1 role in myeloma.” (PDF 1499 kb)
Acknowledgements
Expert technical assistance provided by staff of The University of Iowa Laboratory Animal Care and Resources Facility, Central Microscopy Research Facility, and Flow Cytometry and Genomics Cores is gratefully acknowledged.
Funding
This work was supported by grants from the National Natural Science Foundation of China (NSFC), (81500166, 81600177, 81770220 and 81670200 to YY and CG and by grants from the Natural Science Foundation of Jiangsu Province, BK20160048 to YY and BK20161041 to CG. This work was also supported by NIH R01CA152105 and grants from the Multiple Myeloma Research Foundation, International Myeloma Foundation and American Society of Hematology (ASH) Bridge Funding Program (all to FZ). Additional assistance was provided by NCI Core Grant P30CA086862 in support of The University of Iowa Holden Comprehensive Cancer Center. Support from ASH’s Bridge Grant Program and NIH grants R21CA187388 and R01CA151354 (all to SJ) is also gratefully acknowledged.
Availability of data and materials
Please contact the co-senior authors with requests for data, reagents, constructs, and materials.
Authors’ contributions
CG and XJ carried out bench work and performed in vitro and in vivo studies using myeloma cells. CH and R S carried out histopathologic and statistical analyses. FZ and GT evaluated gene expression and clinical outcome data and provided expertise on myeloma treatment. YY and S J conceived, designed and coordinated the study and drafted the manuscript. All authors read, commented on, and approved the final manuscript.
Ethics approval and consent to participate
The University of Iowa Institutional Review Board approved the study, including the use of de-identified patient tissue samples. All patients provided written informed consent and their anonymity was maintained throughout the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Chunyan Gu, Email: guchunyan346@163.com.
Xuefang Jing, Email: xuefang-jing@uiowa.edu.
Carol Holman, Email: carol-holman@uiowa.edu.
Ramakrishna Sompallae, Email: rama-sompallae@uiowa.edu.
Fenghuang Zhan, Email: fenghuang-zhan@uiowa.edu.
Guido Tricot, Email: guido-tricot@uiowa.edu.
Ye Yang, Phone: 86-25-85811597, Email: yangye876@sina.com.
Siegfried Janz, Phone: (414) 955-5784, Email: sjanz@mcw.edu.
References
- 1.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30. doi: 10.3322/caac.21332. [DOI] [PubMed] [Google Scholar]
- 2.Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos MV, Kumar S, Hillengass J, Kastritis E, Richardson P, et al. International myeloma working group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538–e548. doi: 10.1016/S1470-2045(14)70442-5. [DOI] [PubMed] [Google Scholar]
- 3.Rollig C, Knop S, Bornhauser M. Multiple myeloma. Lancet. 2015;385(9983):2197–2208. doi: 10.1016/S0140-6736(14)60493-1. [DOI] [PubMed] [Google Scholar]
- 4.Barlogie B, Mitchell A, van Rhee F, Epstein J, Morgan GJ, Crowley J. Curing myeloma at last: defining criteria and providing the evidence. Blood. 2014;124(20):3043–3051. doi: 10.1182/blood-2014-07-552059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tang M, Zhao R, van de Velde H, Tross JG, Mitsiades C, Viselli S, Neuwirth R, Esseltine DL, Anderson K, Ghobrial IM, et al. Myeloma cell dynamics in response to treatment supports a model of hierarchical differentiation and clonal evolution. Clin Cancer Res. 2016;22(16):4206–4214. doi: 10.1158/1078-0432.CCR-15-2793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kortum KM, Mai EK, Hanafiah NH, Shi CX, Zhu YX, Bruins L, Barrio S, Jedlowski P, Merz M, Xu J, et al. Targeted sequencing of refractory myeloma reveals a high incidence of mutations in CRBN and Ras pathway genes. Blood. 2016;128(9):1226–1233. doi: 10.1182/blood-2016-02-698092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Weinhold N, Ashby C, Rasche L, Chavan SS, Stein C, Stephens OW, Tytarenko R, Bauer MA, Meissner T, Deshpande S, et al. Clonal selection and double hit events involving tumor suppressor genes underlie relapse from chemotherapy: myeloma as a model. Blood. 2016;128(13):1735–1744. doi: 10.1182/blood-2016-06-723007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Agirre X, Castellano G, Pascual M, Heath S, Kulis M, Segura V, Bergmann A, Esteve A, Merkel A, Raineri E, et al. Whole-epigenome analysis in multiple myeloma reveals DNA hypermethylation of B cell-specific enhancers. Genome Res. 2015;25(4):478–487. doi: 10.1101/gr.180240.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gooding S, Edwards CM. New approaches to targeting the bone marrow microenvironment in multiple myeloma. Curr Opin Pharmacol. 2016;28:43–49. doi: 10.1016/j.coph.2016.02.013. [DOI] [PubMed] [Google Scholar]
- 10.Nikesitch N, Ling SC. Molecular mechanisms in multiple myeloma drug resistance. J Clin Pathol. 2016;69(2):97–101. doi: 10.1136/jclinpath-2015-203414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Miannay B, Minvielle S, Roux O, Drouin P, Avet-Loiseau H, Guerin-Charbonnel C, Gouraud W, Attal M, Facon T, Munshi NC, et al. Logic programming reveals alteration of key transcription factors in multiple myeloma. Sci Rep. 2017;7(1):9257. doi: 10.1038/s41598-017-09378-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gu C, Yang Y, Sompallae R, Xu H, Tompkins VS, Holman C, Hose D, Goldschmidt H, Tricot G, Zhan F, et al. FOXM1 is a therapeutic target for high-risk multiple myeloma. Leukemia. 2016;30(4):873–882. doi: 10.1038/leu.2015.334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gu C, Holman C, Sompallae R, Jing X, Tomasson M, Hose D, Seckinger A, Zhan F, Tricot G, Goldschmidt H, et al. Upregulation of FOXM1 in a subset of relapsed myeloma results in poor outcome. Blood Cancer J. 2018;8(2):22. doi: 10.1038/s41408-018-0060-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.He Z, O'Neal J, Wilson WC, Mahajan N, Luo J, Wang Y, Su MY, Lu L, Skeath JB, Bhattacharya D, et al. Deletion of Rb1 induces both hyperproliferation and cell death in murine germinal center B cells. Exp Hematol. 2016;44(3):161–165. doi: 10.1016/j.exphem.2015.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhan F, Huang Y, Colla S, Stewart JP, Hanamura I, Gupta S, Epstein J, Yaccoby S, Sawyer J, Burington B, et al. The molecular classification of multiple myeloma. Blood. 2006;108(6):2020–2028. doi: 10.1182/blood-2005-11-013458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Seckinger A, Meissner T, Moreaux J, Depeweg D, Hillengass J, Hose K, Reme T, Rosen-Wolff A, Jauch A, Schnettler R, et al. Clinical and prognostic role of annexin A2 in multiple myeloma. Blood. 2012;120(5):1087–1094. doi: 10.1182/blood-2012-03-415588. [DOI] [PubMed] [Google Scholar]
- 17.Hegde NS, Sanders DA, Rodriguez R, Balasubramanian S. The transcription factor FOXM1 is a cellular target of the natural product thiostrepton. Nat Chem. 2011;3(9):725–731. doi: 10.1038/nchem.1114. [DOI] [PubMed] [Google Scholar]
- 18.Mulligan G, Mitsiades C, Bryant B, Zhan F, Chng WJ, Roels S, Koenig E, Fergus A, Huang Y, Richardson P, et al. Gene expression profiling and correlation with outcome in clinical trials of the proteasome inhibitor bortezomib. Blood. 2007;109(8):3177–3188. doi: 10.1182/blood-2006-09-044974. [DOI] [PubMed] [Google Scholar]
- 19.Bergsagel PL, Kuehl WM, Zhan F, Sawyer J, Barlogie B, Shaughnessy J., Jr Cyclin D dysregulation: an early and unifying pathogenic event in multiple myeloma. Blood. 2005;106(1):296–303. doi: 10.1182/blood-2005-01-0034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hose D, Reme T, Hielscher T, Moreaux J, Messner T, Seckinger A, Benner A, Shaughnessy JD, Jr, Barlogie B, Zhou Y, et al. Proliferation is a central independent prognostic factor and target for personalized and risk-adapted treatment in multiple myeloma. Haematologica. 2011;96(1):87–95. doi: 10.3324/haematol.2010.030296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Khongkow P, Gomes AR, Gong C, Man EP, Tsang JW, Zhao F, Monteiro LJ, Coombes RC, Medema RH, Khoo US, et al. Paclitaxel targets FOXM1 to regulate KIF20A in mitotic catastrophe and breast cancer paclitaxel resistance. Oncogene. 2016;35(8):990–1002. doi: 10.1038/onc.2015.152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Halasi M, Gartel AL. Suppression of FOXM1 sensitizes human cancer cells to cell death induced by DNA-damage. PLoS One. 2012;7(2):e31761. doi: 10.1371/journal.pone.0031761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pandit B, Gartel AL. FoxM1 knockdown sensitizes human cancer cells to proteasome inhibitor-induced apoptosis but not to autophagy. Cell cycle (Georgetown, Tex) 2011;10(19):3269–3273. doi: 10.4161/cc.10.19.17735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yao S, Fan LY, Lam EW. The FOXO3-FOXM1 axis: a key cancer drug target and a modulator of cancer drug resistance. Semin Cancer Biol. 2018;50:77–89. doi: 10.1016/j.semcancer.2017.11.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bella L, Zona S, Nestal de Moraes G, Lam EW. FOXM1: a key oncofoetal transcription factor in health and disease. Semin Cancer Biol. 2014;29:32–39. doi: 10.1016/j.semcancer.2014.07.008. [DOI] [PubMed] [Google Scholar]
- 26.Zona S, Bella L, Burton MJ, Nestal de Moraes G, Lam EW. FOXM1: an emerging master regulator of DNA damage response and genotoxic agent resistance. Biochim Biophys Acta. 2014;1839(11):1316–1322. doi: 10.1016/j.bbagrm.2014.09.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Koo CY, Muir KW, Lam EW. FOXM1: from cancer initiation to progression and treatment. Biochim Biophys Acta. 2012;1819(1):28–37. doi: 10.1016/j.bbagrm.2011.09.004. [DOI] [PubMed] [Google Scholar]
- 28.Shaffer AL, Emre NC, Lamy L, Ngo VN, Wright G, Xiao W, Powell J, Dave S, Yu X, Zhao H, et al. IRF4 addiction in multiple myeloma. Nature. 2008;454(7201):226–231. doi: 10.1038/nature07064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Keats JJ, Chesi M, Egan JB, Garbitt VM, Palmer SE, Braggio E, Van Wier S, Blackburn PR, Baker AS, Dispenzieri A, et al. Clonal competition with alternating dominance in multiple myeloma. Blood. 2012;120(5):1067–1076. doi: 10.1182/blood-2012-01-405985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Buchner M, Park E, Geng H, Klemm L, Flach J, Passegue E, Schjerven H, Melnick A, Paietta E, Kopanja D, et al. Identification of FOXM1 as a therapeutic target in B-cell lineage acute lymphoblastic leukaemia. Nat Commun. 2015;6:6471. doi: 10.1038/ncomms7471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Uddin S, Hussain AR, Ahmed M, Siddiqui K, Al-Dayel F, Bavi P, Al-Kuraya KS. Overexpression of FoxM1 offers a promising therapeutic target in diffuse large B-cell lymphoma. Haematologica. 2012;97(7):1092–1100. doi: 10.3324/haematol.2011.053421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Motiwala T, Kutay H, Zanesi N, Frissora FW, Mo X, Muthusamy N, Jacob ST. PTPROt-mediated regulation of p53/Foxm1 suppresses leukemic phenotype in a CLL mouse model. Leukemia. 2015;29(6):1350–1359. doi: 10.1038/leu.2014.341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bisikirska B, Bansal M, Shen Y, Teruya-Feldstein J, Chaganti R, Califano A. Elucidation and pharmacological targeting of novel molecular drivers of follicular lymphoma progression. Cancer Res. 2016;76(3):664–674. doi: 10.1158/0008-5472.CAN-15-0828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gentles AJ, Newman AM, Liu CL, Bratman SV, Feng W, Kim D, Nair VS, Xu Y, Khuong A, Hoang CD, et al. The prognostic landscape of genes and infiltrating immune cells across human cancers. Nat Med. 2015;21(8):938–945. doi: 10.1038/nm.3909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Zhu X, Xue L, Yao Y, Wang K, Tan C, Zhuang M, Zhou F, Zhu L. The FoxM1-ABCC4 axis mediates carboplatin resistance in human retinoblastoma Y-79 cells. Acta Biochim Biophys Sin Shanghai. 2018;50(9):914–920. doi: 10.1093/abbs/gmy080. [DOI] [PubMed] [Google Scholar]
- 36.Roh YG, Mun MH, Jeong MS, Kim WT, Lee SR, Chung JW, Kim SI, Kim TN, Nam JK, Leem SH. Drug resistance of bladder cancer cells through activation of ABCG2 by FOXM1. BMB Rep. 2018;51(2):98–103. doi: 10.5483/BMBRep.2018.51.2.222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Xie T, Geng J, Wang Y, Wang L, Huang M, Chen J, Zhang K, Xue L, Liu X, Mao X, et al. FOXM1 evokes 5-fluorouracil resistance in colorectal cancer depending on ABCC10. Oncotarget. 2017;8(5):8574–8589. doi: 10.18632/oncotarget.14351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wang Y, Wen L, Zhao SH, Ai ZH, Guo JZ, Liu WC. FoxM1 expression is significantly associated with cisplatin-based chemotherapy resistance and poor prognosis in advanced non-small cell lung cancer patients. Lung Cancer. 2013;79(2):173–179. doi: 10.1016/j.lungcan.2012.10.019. [DOI] [PubMed] [Google Scholar]
- 39.Karunarathna U, Kongsema M, Zona S, Gong C, Cabrera E, Gomes AR, Man EP, Khongkow P, Tsang JW, Khoo US, et al. OTUB1 inhibits the ubiquitination and degradation of FOXM1 in breast cancer and epirubicin resistance. Oncogene. 2016;35(11):1433–1444. doi: 10.1038/onc.2015.208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cui J, Xia T, Xie D, Gao Y, Jia Z, Wei D, Wang L, Huang S, Quan M, Xie K. HGF/Met and FOXM1 form a positive feedback loop and render pancreatic cancer cells resistance to Met inhibition and aggressive phenotypes. Oncogene. 2016;35(36):4708–4718. doi: 10.1038/onc.2016.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Wang Y, Zhang W, Wen L, Yang H, Wen M, Yun Y, Zhao L, Zhu X, Tian L, Luo E, et al. FOXM1 confers resistance to gefitinib in lung adenocarcinoma via a MET/AKT-dependent positive feedback loop. Oncotarget. 2016;7(37):59245–59259. doi: 10.18632/oncotarget.11043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Eckers JC, Kalen AL, Sarsour EH, Tompkins VS, Janz S, Son JM, Doskey CM, Buettner GR, Goswami PC. Forkhead box M1 regulates quiescence-associated radioresistance of human head and neck squamous carcinoma cells. Radiat Res. 2014;182(4):420–429. doi: 10.1667/RR13726.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Halasi M, Gartel AL. Targeting FOXM1 in cancer. Biochem Pharmacol. 2013;85(5):644–652. doi: 10.1016/j.bcp.2012.10.013. [DOI] [PubMed] [Google Scholar]
- 44.Wever WJ, Bogart JW, Baccile JA, Chan AN, Schroeder FC, Bowers AA. Chemoenzymatic synthesis of thiazolyl peptide natural products featuring an enzyme-catalyzed formal [4 + 2] cycloaddition. J Am Chem Soc. 2015;137(10):3494–3497. doi: 10.1021/jacs.5b00940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Shah SP, Lonial S, Boise LH. When Cancer fights Back: multiple myeloma, proteasome inhibition, and the heat-shock response. Mol Cancer Res. 2015;13(8):1163–1173. doi: 10.1158/1541-7786.MCR-15-0135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Consolaro F, Basso G, Ghaem-Magami S, Lam EW, Viola G. FOXM1 is overexpressed in B-acute lymphoblastic leukemia (B-ALL) and its inhibition sensitizes B-ALL cells to chemotherapeutic drugs. Int J Oncol. 2015;47(4):1230–1240. doi: 10.3892/ijo.2015.3139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Chesi M, Matthews GM, Garbitt VM, Palmer SE, Shortt J, Lefebure M, Stewart AK, Johnstone RW, Bergsagel PL. Drug response in a genetically engineered mouse model of multiple myeloma is predictive of clinical efficacy. Blood. 2012;120(2):376–385. doi: 10.1182/blood-2012-02-412783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Chesi M, Robbiani DF, Sebag M, Chng WJ, Affer M, Tiedemann R, Valdez R, Palmer SE, Haas SS, Stewart AK, et al. AID-dependent activation of a MYC transgene induces multiple myeloma in a conditional mouse model of post-germinal center malignancies. Cancer Cell. 2008;13(2):167–180. doi: 10.1016/j.ccr.2008.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Duncan K, Rosean TR, Tompkins VS, Olivier A, Sompallae R, Zhan F, Tricot G, Acevedo MR, Ponto LL, Walsh SA, et al. (18)F-FDG-PET/CT imaging in an IL-6- and MYC-driven mouse model of human multiple myeloma affords objective evaluation of plasma cell tumor progression and therapeutic response to the proteasome inhibitor ixazomib. Blood Cancer J. 2013;3:e165. doi: 10.1038/bcj.2013.61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Rutsch S, Neppalli VT, Shin DM, DuBois W, Morse HC, 3rd, Goldschmidt H, Janz S. IL-6 and MYC collaborate in plasma cell tumor formation in mice. Blood. 2010;115(9):1746–1754. doi: 10.1182/blood-2009-08-237941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Delmore JE, Issa GC, Lemieux ME, Rahl PB, Shi J, Jacobs HM, Kastritis E, Gilpatrick T, Paranal RM, Qi J, et al. BET bromodomain inhibition as a therapeutic strategy to target c-Myc. Cell. 2011;146(6):904–917. doi: 10.1016/j.cell.2011.08.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Gorgun G, Calabrese E, Hideshima T, Ecsedy J, Perrone G, Mani M, Ikeda H, Bianchi G, Hu Y, Cirstea D, et al. A novel Aurora-a kinase inhibitor MLN8237 induces cytotoxicity and cell-cycle arrest in multiple myeloma. Blood. 2010;115(25):5202–5213. doi: 10.1182/blood-2009-12-259523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Zeng J, Wang L, Li Q, Li W, Bjorkholm M, Jia J, Xu D. FoxM1 is up-regulated in gastric cancer and its inhibition leads to cellular senescence, partially dependent on p27 kip1. J Pathol. 2009;218(4):419–427. doi: 10.1002/path.2530. [DOI] [PubMed] [Google Scholar]
- 54.Li SK, Smith DK, Leung WY, Cheung AM, Lam EW, Dimri GP, Yao KM. FoxM1c counteracts oxidative stress-induced senescence and stimulates Bmi-1 expression. J Biol Chem. 2008;283(24):16545–16553. doi: 10.1074/jbc.M709604200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Zhang Xiaolu, Zeng Jiping, Zhou Minran, Li Bingnan, Zhang Yuanyuan, Huang Tao, Wang Lixiang, Jia Jihui, Chen Chunyan. The tumor suppressive role of miRNA-370 by targeting FoxM1 in acute myeloid leukemia. Molecular Cancer. 2012;11(1):56. doi: 10.1186/1476-4598-11-56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Liu G, Sun Y, Ji P, Li X, Cogdell D, Yang D, Parker Kerrigan BC, Shmulevich I, Chen K, Sood AK, et al. MiR-506 suppresses proliferation and induces senescence by directly targeting the CDK4/6-FOXM1 axis in ovarian cancer. J Pathol. 2014;233(3):308–318. doi: 10.1002/path.4348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Rader J, Russell MR, Hart LS, Nakazawa MS, Belcastro LT, Martinez D, Li Y, Carpenter EL, Attiyeh EF, Diskin SJ, et al. Dual CDK4/CDK6 inhibition induces cell-cycle arrest and senescence in neuroblastoma. Clin Cancer Res. 2013;19(22):6173–6182. doi: 10.1158/1078-0432.CCR-13-1675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Menu E, Garcia J, Huang X, Di Liberto M, Toogood PL, Chen I, Vanderkerken K, Chen-Kiang S. A novel therapeutic combination using PD 0332991 and bortezomib: study in the 5T33MM myeloma model. Cancer Res. 2008;68(14):5519–5523. doi: 10.1158/0008-5472.CAN-07-6404. [DOI] [PubMed] [Google Scholar]
- 59.Niesvizky R, Badros AZ, Costa LJ, Ely SA, Singhal SB, Stadtmauer EA, Haideri NA, Yacoub A, Hess G, Lentzsch S, et al. Phase 1/2 study of cyclin-dependent kinase (CDK)4/6 inhibitor palbociclib (PD-0332991) with bortezomib and dexamethasone in relapsed/refractory multiple myeloma. Leukemia & lymphoma. 2015;56:3320–3328. doi: 10.3109/10428194.2015.1030641. [DOI] [PubMed] [Google Scholar]
- 60.Kumar SK, LaPlant B, Chng WJ, Zonder J, Callander N, Fonseca R, Fruth B, Roy V, Erlichman C, Stewart AK, et al. Dinaciclib, a novel CDK inhibitor, demonstrates encouraging single-agent activity in patients with relapsed multiple myeloma. Blood. 2015;125(3):443–448. doi: 10.1182/blood-2014-05-573741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Nischalke HD, Schmitz V, Luda C, Aldenhoff K, Berger C, Feldmann G, Sauerbruch T, Spengler U, Nattermann J. Detection of IGF2BP3, HOXB7, and NEK2 mRNA expression in brush cytology specimens as a new diagnostic tool in patients with biliary strictures. PLoS One. 2012;7(8):e42141. doi: 10.1371/journal.pone.0042141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Calvisi DF, Pinna F, Ladu S, Pellegrino R, Simile MM, Frau M, De Miglio MR, Tomasi ML, Sanna V, Muroni MR, et al. Forkhead box M1B is a determinant of rat susceptibility to hepatocarcinogenesis and sustains ERK activity in human HCC. Gut. 2009;58(5):679–687. doi: 10.1136/gut.2008.152652. [DOI] [PubMed] [Google Scholar]
- 63.Zhou W, Yang Y, Xia J, Wang H, Salama ME, Xiong W, Xu H, Shetty S, Chen T, Zeng Z, et al. NEK2 induces drug resistance mainly through activation of efflux drug pumps and is associated with poor prognosis in myeloma and other cancers. Cancer Cell. 2013;23(1):48–62. doi: 10.1016/j.ccr.2012.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Liu X, Gao Y, Lu Y, Zhang J, Li L, Yin F. Upregulation of NEK2 is associated with drug resistance in ovarian cancer. Oncol Rep. 2014;31(2):745–754. doi: 10.3892/or.2013.2910. [DOI] [PubMed] [Google Scholar]
- 65.Marina M, Saavedra HI. Nek2 and Plk4: prognostic markers, drivers of breast tumorigenesis and drug resistance. Front Biosci (Landmark Ed) 2014;19:352–365. doi: 10.2741/4212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Innocenti P, Woodward H, O'Fee L, Hoelder S. Expanding the scope of fused pyrimidines as kinase inhibitor scaffolds: synthesis and modification of pyrido[3,4-d]pyrimidines. Organic & biomolecular chemistry. 2015;13(3):893–904. doi: 10.1039/C4OB02238F. [DOI] [PubMed] [Google Scholar]
- 67.Hu CM, Zhu J, Guo XE, Chen W, Qiu XL, Ngo B, Chien R, Wang YV, Tsai CY, Wu G, et al. Novel small molecules disrupting Hec1/Nek2 interaction ablate tumor progression by triggering Nek2 degradation through a death-trap mechanism. Oncogene. 2015;34(10):1220–1230. doi: 10.1038/onc.2014.67. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Quantitative, reverse transcription (RT) polymerase chain reaction (qRT-PCR) analysis of FOXM1 gene expression in 8 myeloma patients for which 3 sequential CD138+ fractionated bone marrow tumor samples at baseline (white columns, newly diagnosed disease), initiation of HDT (high-dose therapy) and autologous hematopoietic stem cell transplantation (ASCT) therapy (grey columns) and consolidation / maintenance therapy (black columns) were available. In the course of the latter, three patiens (1, 2 and 8) and one patient (7) experienced a clinically significant and incipient FOXM1High relapse, respectively. Total RNA was extracted using Quick-RNA MiniPrep (Zymo Research) and reverse transcribed using oligo dT primers and SuperScript III RT (Invitrogen). Data analysis relied on the ΔΔCt method. Primers were purchased from Integrated DNA Technologies (Coralville, Iowa). Sequences are available upon request. All increases in FOXM1 gene expression are relative to the patient-specific baseline value, which was set at 1. All patients were consented in accordance with rules and regulations of the US Food and Drug Administration and the Declaration of Helsinki. Tumor samples were collected with institutional approval supplied with IRB 201503809 entitled “FOXM1 role in myeloma.” (PDF 1499 kb)
Data Availability Statement
Please contact the co-senior authors with requests for data, reagents, constructs, and materials.