

Abstract
Context:
The lack of thorough knowledge regarding morphological and anatomical variations of the root canal system can result in failure to identify all root canals and lead to inadequate instrumentation and consequent failure of the endodontic treatment.
Aims:
The aim of the study was to evaluate the anatomy of single-rooted mandibular canines using micro-computed tomography (micro-CT).
Subjects and Methods:
Eighty mandibular canines were scanned by micro-CT to determine anatomic parameters: Vertucci's classification, number of lateral canals, roundness, and minor and major diameters. The shape of root canal orifices, volume, surface area, and convexity structure model index (SMI) were also evaluated.
Analysis Used:
The CTAn and CTvol software were used to three-dimensional and morphometric analysis.
Results:
All canals were classified as Vertucci Type I. Lateral canals were verified in 42.4% of the roots, in apical third. The canal diameters were decreased near the apex. The cross sections at the cementoenamel junction and 1 mm from the apex were oval in 38.3% and 79.4% of the canals, respectively. The mean canal volumes and surface areas were 11.48 ± 4.41 mm3≥ and 67.29 ± 19.18 mm2, respectively. The SMI values indicated that mandibular canine was approximately rod like.
Conclusions:
The morphology of the root canal of single-rooted canines varied widely at different root levels.
Keywords: Anatomy, canine, micro-computed tomography, root canal
INTRODUCTION
Successful endodontic treatments depend on complete root canal cleaning and shaping, as well as three-dimensional (3D) hermetic root canal system (RCS) filling.[1] The lack of thorough knowledge regarding morphological and anatomical variations of the RCS can result in failure to identify all root canals and lead to inadequate instrumentation and consequent failure of the endodontic treatment.[2] Therefore, the first step in achieving a successful endodontic outcome is an exact RCS evaluation and its anatomical variations.[3]
Several techniques have been applied in the study of RCS morphology. Traditional methods, such as radiography, cross-sectioning, staining and root clearing, scanning electron microscopy, and stereomicroscopy, are either destructive or provide only two-dimensional (2D) information.[4,5,6]
Micro-computed tomography (micro-CT) is a noninvasive, nondestructive, and reproducible method, considered the most accurate method for RCS morphology investigations, and can be applied quantitatively, as well as qualitatively, for the 3D RCS assessments.[5,7,8]
Some studies[6,9] have reported that mandibular canines display a highly variable internal canal configuration. According to Wu et al.,[9] mandibular canines display a high incidence of oval-shaped canals, posing a significant challenge for adequate root canal treatment, since instruments leave behind untouched recesses in the root canal. In addition, other factors that can contribute to differences in internal complexities of the root canal anatomy include ethnic differences, age, gender, and study design.[1,11]
A great morphological variation in this regard is observed in the Brazilian population, as it is considered one of the most heterogeneous populations in the world, with an important genetic contribution from the following main continental groups: Europeans, Africans, Asians, and Native Americans.[12] In this context, the aim of the present study was to evaluate the root canal morphology of single-rooted human mandibular canines in a Brazilian Southeastern subpopulation by micro-CT.
SUBJECTS AND METHODS
Sample selection
This study was approved by the local Ethics and Research Committee. One hundred and thirty extracted human mandibular canines were evaluated. The roots met the following inclusion criteria: fully formed apex, the absence of fractures, and no previous endodontic treatment on the canines.
Micro-computed tomography scanning and analysis
The roots were scanned on a SkyScan 1173 v2 micro-CT (Bruker MicroCT, Kontich, Belgium). The X-ray tube was operated at 50 kV and 160 μA, using a 1 mm thick aluminum filter, 320 ms exposure time, 0.8 rotation step, and 360° rotation. Both the cross-sectional pixel size and intersection distance (resolution) were set at 12.1 μm. These acquisition parameters were used for all scanned specimens. The acquired projection files were reconstructed into a 3D dataset using the NRecon software (v1.6.1.0; Bruker, Kontich, Belgium). Reconstruction parameters included a 50% beam hardening correction, ring artifact correction of 10, and input of fixed contrast limits (0–0.05) for all image stacks.
Morphologic canal parameters were recorded (CTAn v. 1.14.4, Bruker-Microct Kontich, Belgium) and 3D models of the mesial RCSs were obtained and evaluated (CTVol v. 2.2.1, Bruker-Microct, Kontich, Belgium). The registered images were then processed to generate 3D renderings of the external tooth surface and the internal root canal space. During reconstruction, transparency was adjusted, so internal morphology could be visualized.
The following parameters were evaluated: number of canals, root canal configurations according to Vertucci's classification,[13] root length and number and location of lateral canals, the presence of apical delta, perimeter, roundness, and minor and major diameters at cervical, medium, and apical thirds and 1 mm from the foramen. The cross sections of the root canals were classified as round, oval, long oval, or flattened, according to the minor and major diameters of the canals 1 mm from the apex, as described previously by Jou et al.[12] In addition, the number and shape of root canal orifices at the cementoenamel junction (CEJ) level were also evaluated, according to Liu et al.[13] and Johnsen et al.[14] The CTan (Bruker MicroCT, Kontich, Belgium) plug-in 3D analysis and morphometric analyses were applied.
The 3D root canal measurements included volume (mm3≥), surface area (mm2), and convexity structure model index (SMI) from the CEJ to the apex and were also evaluated by the CTan (Bruker MicroCT, Kontich, Belgium).
RESULTS
3D reconstruction of the internal anatomy indicated that all specimens exhibited a single main root canal. Therefore, 100% of the specimens were classified as Vertucci Type I [Figure 1a]. The length of the roots measured from the pulp chamber to the apical foramen ranged from 11.76 to 20.84 mm (15.89 ± 1.96 mm). Lateral canals were verified in 42.4% of the roots, all present in the apical third [Figure 1b]; the apical delta was observed in 19% of canines [Figure 1c].
Figure 1.
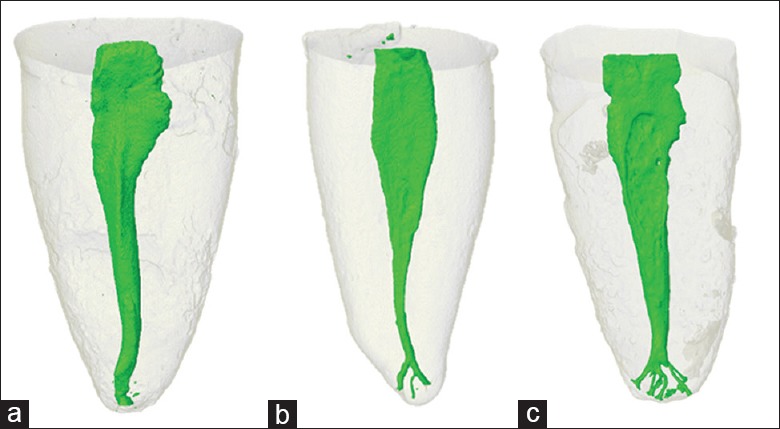
Representative three-dimensional models of mandibular canines. (a) Vertucci type I, (b) lateral canals, (c) apical delta
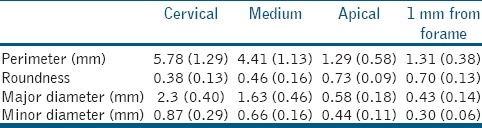
The results of the 2D (perimeter, roundness, and major and minor diameter) analysis are detailed inTable 1.
Table 1.
Morphometric two-dimensional data (means±standard deviation)
Concerning root canal orifice shapes and types at the CEJ level, six different orifice shapes were observed, namely oval (38.3%), Hourglass (30.1%), bowling pin (15%), circular (6.8%), fish (5.8%), and kidney (4%). Triangular orifice shapes were not observed [Figure 2a–f]. Regarding the cross sections 1 mm from the apex, 79.4% were classified as oval, 19.2% were classified as long oval, and 1.4% as flattened canals. No round canals were observed.
Figure 2.
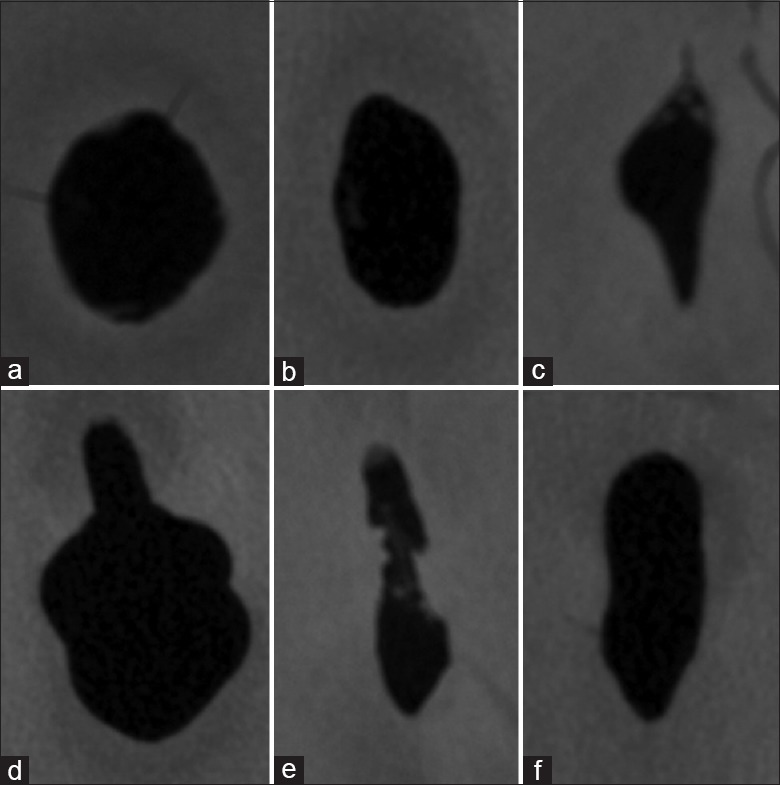
(a-f) Representative images of canal orifice shapes at cementoenamel junction detected in this study: (a) circular, (b) oval, (c) fish, (d) bowling pin, (e) kidney, and (f) hourglass
The mean volume of the mandibular canine canals and surface areas was 11.48 ± 4.41 mm3≥ and 67.29 ± 19.18 mm2, respectively. In the present study, the SMI results indicated that the canine root canal geometry was approximately rod like (SMI = 1.43 ± 1.25).
DISCUSSION
An accurate knowledge on root-canal morphology and its anatomical variations is mandatory for successful root canal treatment.[5,15,16,17] The morphology of single-rooted mandibular canines was evaluated by micro-CT.
It has been reported that the prevalence of type I root canal configurations in mandibular canines ranges from 78% to 98%.[18,19,20] In this study, all evaluated mandibular canines displayed only one main canal and were classified as Vertucci Type I, similar to the study carried out by Versiani et al.[8] The length of the roots measured from the pulp chamber to the apical foramen ranged from 11.76 to 20.84 mm (15.89 ± 1.96 mm), similar with other studies.[9,21,22]
Lateral canals were verified in 42.4% of the roots, all in the apical third. Somalinga Amardeep et al.[18] observed a frequency of 12.8% of apical lateral canals by cone-beam CT analysis, while Versiani et al.[5,16] detected accessory canals located at the middle (4%) and apical thirds (65%). This discrepancy between studies may be due to differences in populations, evaluation techniques, and/or sample size. However, these results confirm the evidence that lateral canals are most prevalent in the apical third in mandibular canines.
The apical third is considered the most complex RCS structure, rendering it difficult to shape and clean completely when lateral canals, apical deltas, and many apical foramina are present.[7] Therefore, the findings of the present study reinforce the importance of chemical disinfection in these regions and the need for additional disinfection measures such as intracanal medication and the use of active irrigation methods.
The root canals of the evaluated mandibular canines were wider mesiodistally compared to buccolingually, mainly in the cervical third. The perimeter and major and minor diameter results reflected this morphological feature, higher in the cervical compared to the middle and apical thirds [Table 1], similar to the results reported by Versiani et al.[5,15]
Canals may present different shapes in cross sections at different root levels in a same tooth.[4] In the present study, cross sections were evaluated applying three parameters: at the CEJ level, 1 mm from the apex, and roundness. In both cross sections, most canines were classified as displaying oval canals (38.3% and 79.4%, respectively). Roundness increased in the apical third [Table 1], indicating that the apical third was more oval compared to the middle and cervical thirds, similar to reported by Versiani et al.[8] Oval-shaped canals are often poorly cleaned and disinfected, since rotary instrumentation usually sculpts a round cross-sectional shape, which leaves behind untouched recesses in the extremities of the largest diameter of the oval canal.[7]
The surface area and volume of the canines were measured to determine the SMI, which is the change in surface area with infinitesimal enlargements of the surface when the change in volume is related to surface area changes. This 3D parameter, which involves the measurement of surface convexity, is classified as plate (SMI = 0), cylindrical (SMI = 3), or variable (intermediate values).[9] In the present study, SMI results indicated that the mandibular canine root canal geometry was approximately rod like (SMI = 1.43 ± 1.25), in contrast with the study carried out by Versiani et al.[5] Thus, discrepancy between studies, as stated previously, may be due to differences in populations and/or sample size.
CONCLUSIONS
The root canal of single-rooted canines evaluated in the present study was classified as Vertucci type I. However, canine morphology varied widely at different root levels. The high frequency of lateral canals in the apical third (42.2%), apical delta (19%), apical foramen (10%), and oval-shaped cross sections at CEJ and 1 mm from the apex (38.3% and 79.4%, respectively) highlight the anatomic complexity of mandibular canines.
Financial support and sponsorship
This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nivel Superior.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
To the Conselho Nacional de Desenvolvimento Científico e Tecnológico and Coordenação de Aperfeiçoamento de Pessoal de Nivel Superior, both Brazilian Funding Agencies.
REFERENCES
- 1.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 2.de Pablo OV, Estevez R, Péix Sánchez M, Heilborn C, Cohenca N. Root anatomy and canal configuration of the permanent mandibular first molar: A systematic review. J Endod. 2010;36:1919–31. doi: 10.1016/j.joen.2010.08.055. [DOI] [PubMed] [Google Scholar]
- 3.Fan B, Yang J, Gutmann JL, Fan M. Root canal systems in mandibular first premolars with C-shaped root configurations. Part I: Microcomputed tomography mapping of the radicular groove and associated root canal cross-sections. J Endod. 2008;34:1337–41. doi: 10.1016/j.joen.2008.08.006. [DOI] [PubMed] [Google Scholar]
- 4.Marceliano-Alves M, Alves FR, Mendes Dde M, Provenzano JC. Micro-computed tomography analysis of the root canal morphology of palatal roots of maxillary first molars. J Endod. 2016;42:280–3. doi: 10.1016/j.joen.2015.10.016. [DOI] [PubMed] [Google Scholar]
- 5.Versiani MA, Pécora JD, Sousa-Neto MD. The anatomy of two-rooted mandibular canines determined using micro-computed tomography. Int Endod J. 2011;44:682–7. doi: 10.1111/j.1365-2591.2011.01879.x. [DOI] [PubMed] [Google Scholar]
- 6.Acar B, Kamburoğlu K, Tatar İ, Arıkan V, Çelik HH, Yüksel S, et al. Comparison of micro-computerized tomography and cone-beam computerized tomography in the detection of accessory canals in primary molars. Imaging Sci Dent. 2015;45:205–11. doi: 10.5624/isd.2015.45.4.205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Peters OA, Laib A, Rüegsegger P, Barbakow F. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J Dent Res. 2000;79:1405–9. doi: 10.1177/00220345000790060901. [DOI] [PubMed] [Google Scholar]
- 8.Versiani MA, Pécora JD, Sousa-Neto MD. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int Endod J. 2013;46:800–7. doi: 10.1111/iej.12061. [DOI] [PubMed] [Google Scholar]
- 9.Wu MK, R'oris A, Barkis D, Wesselink PR. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:739–43. doi: 10.1067/moe.2000.106344. [DOI] [PubMed] [Google Scholar]
- 10.Alkaabi W, AlShwaimi E, Farooq I, Goodis HE, Chogle SM. A micro-computed tomography study of the root canal morphology of mandibular first premolars in an emirati population. Med Princ Pract. 2017;26:118–24. doi: 10.1159/000453039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Silva EJ, Nejaim Y, Silva AI, Haiter-Neto F, Zaia AA, Cohenca N, et al. Evaluation of root canal configuration of maxillary molars in a Brazilian population using cone-beam computed tomographic imaging: An in vivo study. J Endod. 2014;40:173–6. doi: 10.1016/j.joen.2013.10.002. [DOI] [PubMed] [Google Scholar]
- 12.Jou YT, Karabucak B, Levin J, Liu D. Endodontic working width: Current concepts and techniques. Dent Clin North Am. 2004;48:323–35. doi: 10.1016/j.cden.2003.12.006. [DOI] [PubMed] [Google Scholar]
- 13.Liu N, Li X, Liu N, Ye L, An J, Nie X, et al. A micro-computed tomography study of the root canal morphology of the mandibular first premolar in a population from Southwestern China. Clin Oral Investig. 2013;17:999–1007. doi: 10.1007/s00784-012-0778-1. [DOI] [PubMed] [Google Scholar]
- 14.Johnsen GF, Dara S, Asjad S, Sunde PT, Haugen HJ. Anatomic comparison of contralateral premolars. J Endod. 2017;43:956–63. doi: 10.1016/j.joen.2017.01.012. [DOI] [PubMed] [Google Scholar]
- 15.Siqueira JF, Jr, Pérez AR, Marceliano-Alves MF, Provenzano JC, Silva SG, Pires FR, et al. What happens to unprepared root canal walls: A correlative analysis using micro-computed tomography and histology/scanning electron microscopy. Int Endod J. 2018;51:501–8. doi: 10.1111/iej.12753. [DOI] [PubMed] [Google Scholar]
- 16.Kaffe I, Kaufman A, Littner MM, Lazarson A. Radiographic study of the root canal system of mandibular anterior teeth. Int Endod J. 1985;18:253–9. doi: 10.1111/j.1365-2591.1985.tb00452.x. [DOI] [PubMed] [Google Scholar]
- 17.Oliveira SH, Iorio LS. Internal anatomy study of mandibular canines. Cienc Odontol Bras. 2007;10:37–42. [Google Scholar]
- 18.Somalinga Amardeep N, Raghu S, Natanasabapathy V. Root canal morphology of permanent maxillary and mandibular canines in Indian population using cone beam computed tomography. Anat Res Int. 2014;2014:731–859. doi: 10.1155/2014/731859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Siqueira JF, Jr, Araújo MC, Garcia PF, Fraga RC, Dantas CJ. Histological evaluation of the effectiveness of five instrumentation techniques for cleaning the apical third of root canals. J Endod. 1997;23:499–502. doi: 10.1016/S0099-2399(97)80309-3. [DOI] [PubMed] [Google Scholar]
- 20.Piasecki L, Carneiro E, da Silva Neto UX, Westphalen VP, Brandão CG, Gambarini G, et al. The use of micro-computed tomography to Determine the accuracy of 2 electronic apex Locators and anatomic variations affecting Their precision. J Endod. 2016;42:1263–7. doi: 10.1016/j.joen.2016.04.024. [DOI] [PubMed] [Google Scholar]
- 21.Paqué F, Balmer M, Attin T, Peters OA. Preparation of oval-shaped root canals in mandibular molars using nickel-titanium rotary instruments: A micro-computed tomography study. J Endod. 2010;36:703–7. doi: 10.1016/j.joen.2009.12.020. [DOI] [PubMed] [Google Scholar]
- 22.Lacerda MF, Marceliano-Alves MF, Pérez AR, Provenzano JC, Neves MA, Pires FR, et al. Cleaning and shaping oval canals with 3 Instrumentation systems: A Correlative micro-computed tomographic and histologic study. J Endod. 2017;43:1878–84. doi: 10.1016/j.joen.2017.06.032. [DOI] [PubMed] [Google Scholar]