

Abstract
Successful treatment of the painful neuroma is a particular challenge to the nerve surgeon. Historically, symptomatic neuromas have primarily been treated with excision and implantation techniques, which are inherently passive and do not address the terminal end of the nerve. Over the past decade, the surgical management of neuromas has undergone a paradigm shift synchronous with the development of contemporary techniques aiming to satisfy the nerve end. In this article, we describe the important features of surgical treatment, including the approach to diagnosis with consideration of neuroma type and the decision of partial versus complete neuroma excision. A comprehensive list of the available surgical techniques for management following neuroma excision is presented, the choice of which is often predicated upon the availability of the terminal nerve end for reconstruction. Techniques for neuroma reconstruction in the presence of an intact terminal nerve end include hollow tube reconstruction and auto- or allograft nerve reconstruction. Techniques for neuroma management in the absence of an intact or identifiable terminal nerve end include submuscular or interosseous implantation, centro-central neurorrhaphy, relocation nerve grafting, nerve cap placement, use of regenerative peripheral nerve interface, “end-to-side” neurorrhaphy, and targeted muscle reinnervation. These techniques can be further categorized into passive/ablative and active/reconstructive modalities. The nerve surgeon must be aware of available treatment options and should carefully choose the most appropriate intervention for each patient. Comparative studies are lacking and will be necessary in the future to determine the relative effectiveness of each technique.
BACKGROUND
The physiologic response to nerve injury varies depending on the degree and type of neuronal damage, surrounding micro- and macro-environment, patient physiology, and other factors.1 Following injury to a peripheral nerve, the proximal nerve stump invariably attempts to regenerate toward its distal target. If this process is disorganized or incomplete, it may result in the formation of a neuroma, a growth or tumor of nerve tissue that may become painful.2–4 Pain resulting from symptomatic neuroma can be debilitating and cause significant morbidity with an associated socioeconomic impact. Symptoms of a neuroma include pain (usually sharp or burning), paresthesias, numbness, cold intolerance, and electrical sensitivity, among others.5,6
Many interventions for traumatic neuroma have been described.7 A number of nonsurgical treatments have been advocated including pain medications, radiofrequency ablation, neuromodulation, and desensitization.8–10 Unfortunately, pharmacotherapy alone or other symptomatic treatments are often unsatisfactory in the treatment of neuropathic pain.11 Initial surgical treatment of neuroma focused on excision of the injured segment, or alternatively addressing the autonomic nervous system with sympathectomy.12
In the 1980s, Dellon and Mackinnon13 described the results of neuroma excision and implantation of the nerve end within muscle, demonstrating good to excellent results in 82% of patients. Additional authors described the techniques of neuroma excision and implantation within bone14 or veins.15 Despite a modicum of reported success, these techniques have not been found to be universally successful in improving symptoms and simple excision alone seems to be inferior to other surgical techniques.16 The technique of excision and implantation is relatively “passive” in the treatment of neuroma: it involves excision of the diseased nerve segment but does not fundamentally address the regenerative desire of the nerve stump nor does it provide a pathway for neuroma-free regeneration. This can result in recurrence of symptoms and failure to improve pain.
Recent advances in the treatment of symptomatic neuroma have focused on more “active” treatment of the nerve end following neuroma excision, with the goal of satisfying the nerve end and allowing for more physiologic neuronal regeneration.17 There are increasing numbers of contemporary interventions that aim to improve the outcomes for symptomatic neuroma (Fig. 1). This article provides a list of surgical options for the painful neuroma and discusses an algorithm to consider when deciding on the optimal treatment.
Fig. 1.

Categorization of surgical interventions for neuroma into passive/ablative and active/reconstructive techniques.
DIAGNOSIS AND INITIAL APPROACH
The diagnosis of symptomatic neuroma is often straightforward but may be challenging, depending on the clinical presentation. A careful history must be taken and include the mechanism of injury, temporal sequence of pain development, degree of impact and level of dysfunction, and goals of treatment. Most symptomatic neuromas involve pain, dysesthesia, hypesthesia, paresthesia, cold intolerance, and most commonly have a Tinel sign at the neuroma site.5,6
One must first consider the location and type of neuroma, that is, whether it is a stump (end) neuroma or a neuroma in continuity. Stump neuromas are inherently more straightforward from the standpoint of decision-making: there is, by definition, no distal function of the nerve and therefore less chance for potential functional impairment with surgical intervention. Excision of a neuroma in continuity, on the other hand, may have a significant impact on the function of the nerve (potential downside), which necessarily factors into the decision making.
It is imperative to consider both (1) the function of the involved nerve (sensory, motor, mixed) and (2) the degree of residual nerve function and the amount of pain when deciding about surgical intervention. A patient with mild pain and largely preserved neural function may not be the ideal candidate for neuroma excision as intervention could impact the residual nerve function. Conversely, a patient with incapacitating pain resulting from a neuroma of a noncritical sensory nerve may be a more ideal candidate for neuroma excision and reconstruction, as there is less potential functional downside of intervention. Not all patients with even symptomatic neuromas require surgery, and careful consideration should be undertaken of all options.
At the time of surgery, the neuroma is evaluated and a decision about full versus partial excision is made. For stump neuromas, complete excision is almost always performed, but for neuromas in continuity an intraneural neurolysis with selective neuroma excision may be performed to spare residual function,18 or the neuroma may be maintained in part and a bypass nerve graft of the injured (usually sensory) component performed.19
Depending on the clinical scenario, complete excision of the stump neuroma or selective neurectomy of the neuroma in continuity is first performed. Once the neuroma has been excised, the next step is to determine the optimal reconstructive treatment of the nerve stump.
RECONSTRUCTIVE OPTIONS
There are many possible options to address the nerve end following neuroma excision. In general, the surgical options are divided into 2 major categories based on the presence or absence of the distal nerve end (Fig. 2).
Fig. 2.

Surgical options for neuroma treatment based upon availability of distal nerve ending.
If the Distal Nerve End Is Available
If the terminal nerve end is available, it is intuitive and often preferable to attempt nerve reconstruction to reconstitute the original function of the nerve. Following neuroma excision with the presence of healthy and intact proximal and distal nerve ends, the size of the gap will commonly dictate available options. Smaller nerve gaps have more options for reconstruction and most likely a higher probability of success (Fig. 3).
Fig. 3.

Surgical options if distal nerve end is available. A, Neuroma excised (either in-continuity, or terminal neuroma with nearby stump available) B, Options for reconstruction.
Nerve Reconstruction with Hollow Tube Construct
Very small resulting nerve gaps are rare following neuroma excision but, if present, may allow for use of a hollow tube construct (conduit, connector, or similar). Hollow tube assisted nerve reconstruction appears to be most effective for short gaps < 6 mm and small diameter nerves; this technique may provide sufficient nerve regeneration to allow for return of nerve function and obviate development of pain.20,21 However, this technique is not typically possible for neuroma treatment because most gaps following excision are sufficiently large to preclude use. If intervention is performed primarily for pain relief, hollow tube constructs may be considered for longer defects although functional restoration becomes less likely with increasing gap length.
Nerve Reconstruction with Autograft or Allograft
More commonly, neuroma excision with identifiable proximal and distal nerve ends will result in a nerve gap warranting reconstruction with a nerve graft. Both nerve autograft and nerve allograft can be used for this purpose.22 In our experience, most patients with a painful neuroma for which they are undergoing surgical intervention prefer not to have autograft harvested, given the small, but possible, risk of neuropathic pain or symptomatic neuroma at the donor site. Nerve autograft used for reconstruction following excision of a sensory nerve neuroma will inherently trade numbness and pain at 1 site for, at minimum, numbness at the donor site and the potential for additional morbidity.23,24
Nerve allograft may be ideally suited for cases of painful, symptomatic neuroma in which excision of the lesion results in a reconstructable nerve gap. This provides the nerve a biologic pathway through which to grow, and avoids a second surgical site. This technique has been successfully reported in a series of patients with lower extremity neuromas.25 In this study, the authors reviewed 22 patients who underwent allograft reconstruction of lower extremity neuromas with a mean 15 month follow-up, and demonstrated a decrease in ordinal pain score of 2.6 and a 24 and 31 percentage-point decreases in the PROMIS Pain Behavior and Pain interference measures.
If the Distal Nerve End Is Not Available
In many cases of terminal neuromas, the distal nerve is not available for reconstruction. This may occur in cases where the neuroma is extremely distal and the terminal branches are not identifiable, given their small size, and in all cases of amputations where the terminal nerve ends are no longer present. In these situations, it is not possible to perform reconstruction of the native nerve in the absence of a distal target, and one must decide the appropriate technique to address the proximal nerve stump (Fig. 4).
Fig. 4.
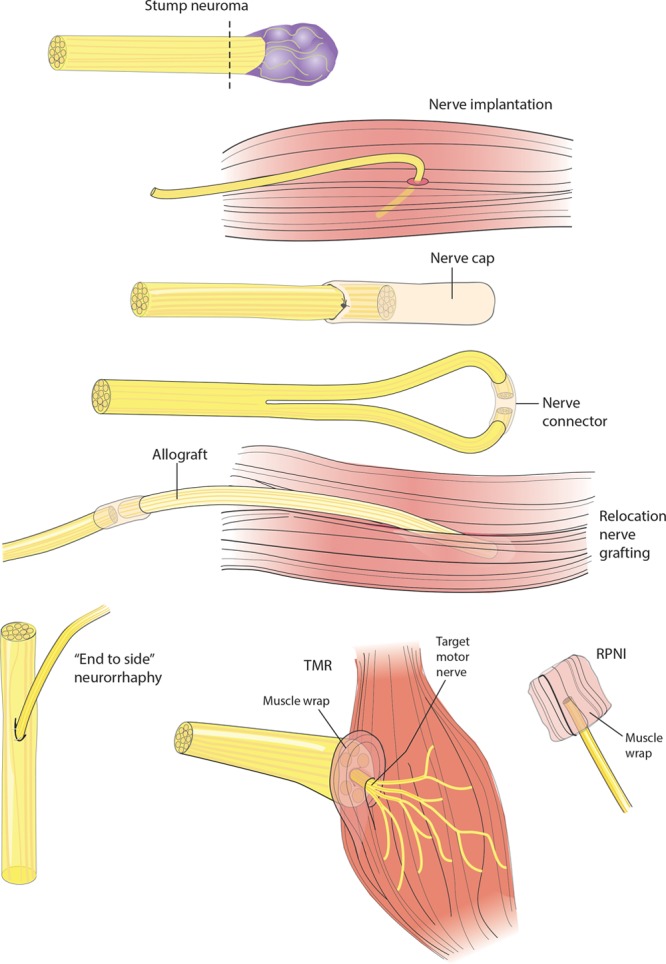
Surgical options if distal nerve end unavailable. Following neuroma excision, options include implantation in muscle, nerve cap, centro-central neurorrhaphy, relocation nerve grafting, “end-to-side” neurorrhaphy, TMR, or use of RPNI.
Implantation of Proximal Nerve Stump into Adjacent Tissues
Implantation of the proximal nerve stump into nearby tissues remains the most commonly performed technique for terminal neuromas. In principle, this technique buries the end of the nerve deeper within the tissues, increasing the distance between the site of axonal sprouting and the cutaneous surface thereby providing additional cushioning and protection for the nerve. The nerve can be implanted within many types of tissue, but is commonly placed within a muscle,13,26 bone,14,27 or inside veins.15 This technique has been shown to be effective for both upper and lower extremity neuromas,28 although it is not universally successful for all patients. Invariably, the end of the nerve will attempt to regrow (albeit in its new position), and may then form a recurrent symptomatic neuroma.
Although this is the surgical technique with the longest track record, it is somewhat simplistic and does not satisfy the nerve end. It is a passive method of treating the nerve end following neuroma excision. There are no randomized trials comparing this technique to others, but there is rationale to believe that it may be inferior to more active methods of neuroma treatment. Traction neurectomy alone appears to have a high rate of symptomatic recurrence.29
Centro-central Neurorrhaphy
Controlling the growth of the terminal nerve end by performing an intraneural fascicular coaptation or neurorrhaphy between adjacent nerves is called a centro-central neurorrhaphy. Technically, this involves a fascicular dissection (for large nerves) or a coaptation (for smaller, ie, digital nerves), often with the use of a hollow tube or nerve graft construct. This technique has been studied experimentally,30 and clinically in the hand31 and lower extremity.32,33 Centro-central neurorrhaphy is currently an uncommonly used technique for neuroma management, and is a passive technique that attempts to facilitate pain relief without directly reconstructing the nerve end.
Relocation Nerve Grafting
Relocation nerve grafting is a technique designed to provide a neural runway for the regenerating nerve, allowing axons to grow through the structure of the endoneurial tubes in the direction of an intentionally less painful destination. This is commonly performed with the use of nerve allograft, which can be size-matched and of sufficient length to allow for dissipated nerve growth through the long graft. A microsurgical coaptation is performed, and the terminal end of the nerve graft is directed away from the painful area or surface. As the nerve regenerates, axons grow through the allograft in an organized, structured way toward the end of the graft. This too is a passive technique, as it is redirects axonal regeneration but does not result in restoration of intended function.
Nerve Cap
Placing a cap on the terminal end of the nerve has been attempted to ameliorate painful regrowth of the nerve end. Many different techniques have been utilized to cap the nerve including the use of synthetic materials and vein,34,35 although this does not seem to be commonly successful with existing materials and unicameral structural capping.36,37 Other studies have presented more promising results, with capping of the nerve end resulting in lower expression of pain markers in a rat model.38 Nerve capping is another passive technique as it is designed to reign in the terminal end of the nerve, but does not provide for reconstruction.
RPNI
The regenerative peripheral nerve interface (RPNI) was designed as an internal signal transduction pathway to optimize prosthetic function. In this system, a free muscle graft is wrapped around the terminal nerve stump, which ultimately becomes innervated by the regenerating nerve and therefore has return of function with less pain.39 This has been studied in the laboratory40–42 and appears to have clinical promise based on a pilot study of 16 amputees, which demonstrated a reduction in both neuroma pain and phantom limb pain.43
This technique also has potential for the treatment of amputees, as the muscle grafts may provide a pathway (through inclusion of denervated muscle and their related neuromuscular junctions) to allow for more focused neural regeneration and potential reduction of associated pain. This is an active technique, as it directs the terminal nerve end into the empty motor endplates of the denervated muscle.
“End-to-side” Neurorrhaphy
Following neuroma excision, the end of the nerve stump may be coapted to the side of an adjacent intact nerve. This may involve the creation of an epineural window or alternatively perineural disruption of the recipient nerve. This was first described as “reverse end-to-side neurotization”44,45 but has also been called “end-to-side nerve repair”46 and “end-to-side neurorrhaphy.”47 This technique is designed to provide a pathway for regenerating axons down the existing runway of an adjacent nerve. It has been shown experimentally to assist with axonal regeneration and may prevent painful neuroma recurrence,46,47 but a number of questions remain about the technical execution and the expectations for destination of the axons. This is considered an active technique, as the neural end is coapted directly to an adjacent nerve.
Targeted Muscle Reinnervation
Targeted Muscle Reinnervation (TMR) was initially described by Kuiken et al.48 as a technique to improve the function of myoelectric prostheses for amputees. In this technique, the blind ends of major peripheral nerves are mobilized and coapted to smaller adjacent motor nerve branches to allow for reinnervation of the newly denervated muscle. This nerve transfer provides a demonstrable function for the mobilized nerves. Fortuitously, this technique appears to have a significant effect on the development of neuroma following nerve transection. This has been studied experimentally49 and has been shown clinically to be an effective treatment for the treatment of postamputation and neuroma pain.50
There are many reasons why TMR holds great promise for the prevention and treatment of neuroma pain.51 Unlike other described techniques, TMR provides a clear purpose for the otherwise undirected nerve ending; it imbues an ultimate function to the nerve and may obviate the disorganized growth typical of undirected nerve endings. It is another active technique to manage the nerve end as it directly restores function to the transected nerve.
DISCUSSION
Pain resulting from a symptomatic neuroma can have a devastating effect on patients, with significant associated dysfunction and disability. Many surgical techniques are available to the nerve surgeon who must decide if surgery is indicated and, if so, what technique to employ. In a recent meta-analysis, Poppler et al.52 reviewed 54 studies and found that surgical treatment was effective in 77% of patients. Historically, surgeons have traditionally performed passive techniques to treat the nerve end, with neuroma excision and implantation or burying of the stump. Contemporary surgical innovations have resulted in more active and reconstructive modalities of treatment, to better satisfy the nerve ending.
The determination about whether to pursue surgical intervention for neuroma is complex and is based upon multiple factors. First, the patient should have an anatomic distribution of pain, with symptoms referable to the specific involved nerve. Second, it is often prudent to confirm that a local anesthetic block is successful in ameliorating symptoms.53 This is performed in an effort to mimic the effect of surgery, and to ensure that there is not overwhelming centralization of pain, which may result in the failure of surgical intervention.
The precise timing and impact of pain centralization is not known, but it is evident that patients with long-standing neuropathic pain—often related to neuroma—are more challenging to treat and may have worse outcomes than those addressed sooner in their clinical course. This is likely the result of significant reorganization of the somatosensory cortex, which occurs after nerve injury and neuroma formation.54,55 Additionally, there appears to be ongoing, progressive cortical reorganization that continues to change over time.56
Once a decision is made for surgery, the preferred surgical technique should be chosen based on the particular clinical scenario. Operative techniques have evolved significantly over time, from initial excision-only and simple burying/implantation techniques to more active management of the nerve end. Although true comparative studies are lacking between techniques, there is rationale to pursue a more dynamic management strategy of the nerve end. Doing this may inherently satisfy the nerve and provide greater impetus for functional regeneration.
There has been an ongoing paradigm shift in the treatment of neuroma, and the nerve surgeon now has a plethora of contemporary tools available to more actively address this problem. Each technique has its own applicability in different clinical scenarios, and the surgeon should carefully consider the patient, anatomic, and surgical factors related to surgical decision making. This conceptual change has been made possible due to new techniques (RPNI and TMR) and new technology (processed nerve allograft, connectors, and conduits), which has provided the nerve surgeon additional options in the armamentarium.
Although new techniques are likely to improve outcomes for patients with symptomatic neuroma, high-level studies comparing techniques are lacking, and there is little objective data to assist surgeons. At this time, scientific rationale, experience, and clinical judgment should facilitate decision-making. Rigorous studies are needed to compare efficacy of given techniques, and to parse the different treatment options and their outcomes. It is possible that a combination of techniques will ultimately be employed to provide the best outcomes for this challenging problem.
Footnotes
Published online 16 October 2018.
Disclosure: Dr. Eberlin serves as a consultant for AxoGen. Dr. Ducic serves as the Medical Director for AxoGen. No funding was received for this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Stokvis A, van der Avoort DJ, van Neck JW, et al. Surgical management of neuroma pain: a prospective follow-up study. Pain. 2010;151:862. [DOI] [PubMed] [Google Scholar]
- 2.Lee SK, Wolfe SW. Peripheral nerve injury and repair. J Am Acad Orthop Surg. 2000;8:243. [DOI] [PubMed] [Google Scholar]
- 3.Fried K, Govrin-Lippmann R, Rosenthal F, et al. Ultrastructure of afferent axon endings in a neuroma. J Neurocytol. 1991;20:682. [DOI] [PubMed] [Google Scholar]
- 4.Vlot MA, Wilkens SC, Chen NC, et al. Symptomatic neuroma following initial amputation for traumatic digital amputation. J Hand Surg Am. 2018;43:86.e1. [DOI] [PubMed] [Google Scholar]
- 5.Geraghty TJ, Jones LE. Painful neuromata following upper limb amputation. Prosthet Orthot Int. 1996;20:176. [DOI] [PubMed] [Google Scholar]
- 6.Stokvis A, Ruijs AC, van Neck JW, et al. Cold intolerance in surgically treated neuroma patients: a prospective follow-up study. J Hand Surg Am. 2009;34:1689. [DOI] [PubMed] [Google Scholar]
- 7.Mackinnon SE. Evaluation and treatment of the painful neuroma. Tech Hand Up Extrem Surg. 1997;1:195. [DOI] [PubMed] [Google Scholar]
- 8.Bennett MI, Simpson KH. Gabapentin in the treatment of neuropathic pain. Palliat Med. 2004;18:5. [DOI] [PubMed] [Google Scholar]
- 9.Restrepo-Garces CE, Marinov A, McHardy P, et al. Pulsed radiofrequency under ultrasound guidance for persistent stump-neuroma pain. Pain Pract. 2011;11:98. [DOI] [PubMed] [Google Scholar]
- 10.Wu J, Chiu DT. Painful neuromas: a review of treatment modalities. Ann Plast Surg. 1999;43:661. [PubMed] [Google Scholar]
- 11.Miyazaki R, Yamamoto T. The efficacy of morphine, pregabalin, gabapentin, and duloxetine on mechanical allodynia is different from that on neuroma pain in the rat neuropathic pain model. Anesth Analg. 2012;115:182. [DOI] [PubMed] [Google Scholar]
- 12.Grant GH. Methods of treatment of neuromata of the hand. J Bone Joint Surg Am. 1951;33-A:841. [PubMed] [Google Scholar]
- 13.Dellon AL, Mackinnon SE. Treatment of the painful neuroma by neuroma resection and muscle implantation. Plast Reconstr Surg. 1986;77:427. [DOI] [PubMed] [Google Scholar]
- 14.Mass DP, Ciano MC, Tortosa R, et al. Treatment of painful hand neuromas by their transfer into bone. Plast Reconstr Surg. 1984;74:182. [DOI] [PubMed] [Google Scholar]
- 15.Herbert TJ, Filan SL. Vein implantation for treatment of painful cutaneous neuromas. A preliminary report. J Hand Surg Br. 1998;23:220. [DOI] [PubMed] [Google Scholar]
- 16.Guse DM, Moran SL. Outcomes of the surgical treatment of peripheral neuromas of the hand and forearm: a 25-year comparative outcome study. Ann Plast Surg. 2013;71:654. [DOI] [PubMed] [Google Scholar]
- 17.Ives GC, Kung TA, Nghiem BT, et al. Current state of the surgical treatment of terminal neuromas. Neurosurgery. 2018. Sep 1;83(3):354. [DOI] [PubMed] [Google Scholar]
- 18.Kline DG, Nulsen FE. The neuroma in continuity. Its preoperative and operative management. Surg Clin North Am. 1972;52:1189. [DOI] [PubMed] [Google Scholar]
- 19.Mackinnon SE, Glickman LT, Dagum A. A technique for the treatment of neuroma in-continuity. J Reconstr Microsurg. 1992;8:379. [DOI] [PubMed] [Google Scholar]
- 20.Boeckstyns ME, Sørensen AI, Viñeta JF, et al. Collagen conduit versus microsurgical neurorrhaphy: 2-year follow-up of a prospective, blinded clinical and electrophysiological multicenter randomized, controlled trial. J Hand Surg Am. 2013;38:2405. [DOI] [PubMed] [Google Scholar]
- 21.Moore AM, Kasukurthi R, Magill CK, et al. Limitations of conduits in peripheral nerve repairs. Hand (N Y). 2009;4:180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ducic I, Mesbahi AN, Attinger CE, et al. The role of peripheral nerve surgery in the treatment of chronic pain associated with amputation stumps. Plast Reconstr Surg. 2008;121:908. [DOI] [PubMed] [Google Scholar]
- 23.IJpma FF, Nicolai JP, Meek MF. Sural nerve donor-site morbidity: thirty-four years of follow-up. Ann Plast Surg. 2006;57:391. [DOI] [PubMed] [Google Scholar]
- 24.Hallgren A, Björkman A, Chemnitz A, et al. Subjective outcome related to donor site morbidity after sural nerve graft harvesting: a survey in 41 patients. BMC Surg. 2013;13:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Souza JM, Purnell CA, Cheesborough JE, et al. Treatment of foot and ankle neuroma pain with processed nerve allografts. Foot Ankle Int. 2016;37:1098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sood MK, Elliot D. Treatment of painful neuromas of the hand and wrist by relocation into the pronator quadratus muscle. J Hand Surg Br. 1998;23:214. [DOI] [PubMed] [Google Scholar]
- 27.Goldstein SA, Sturim HS. Intraosseous nerve transposition for treatment of painful neuromas. J Hand Surg Am. 1985;10:270. [DOI] [PubMed] [Google Scholar]
- 28.Domeshek LF, Krauss EM, Snyder-Warwick AK, et al. Surgical treatment of neuromas improves patient-reported pain, depression, and quality of life. Plast Reconstr Surg. 2017;139:407. [DOI] [PubMed] [Google Scholar]
- 29.Pet MA, Ko JH, Friedly JL, et al. Traction neurectomy for treatment of painful residual limb neuroma in lower extremity amputees. J Orthop Trauma. 2015;29:e321. [DOI] [PubMed] [Google Scholar]
- 30.González-Darder J, Barberá J, Abellán MJ, et al. Centrocentral anastomosis in the prevention and treatment of painful terminal neuroma. An experimental study in the rat. J Neurosurg. 1985;63:754. [DOI] [PubMed] [Google Scholar]
- 31.Kon M, Bloem JJ. The treatment of amputation neuromas in fingers with a centrocentral nerve union. Ann Plast Surg. 1987;18:506. [DOI] [PubMed] [Google Scholar]
- 32.Lidor C, Hall RL, Nunley JA. Centrocentral anastomosis with autologous nerve graft treatment of foot and ankle neuromas. Foot Ankle Int. 1996;17:85. [DOI] [PubMed] [Google Scholar]
- 33.Barberá J, Albert-Pampló R. Centrocentral anastomosis of the proximal nerve stump in the treatment of painful amputation neuromas of major nerves. J Neurosurg. 1993;79:331. [DOI] [PubMed] [Google Scholar]
- 34.Edds MV., Jr Prevention of nerve regeneration and neuroma formation by caps of synthetic resin. J Neurosurg. 1945;2:507. [DOI] [PubMed] [Google Scholar]
- 35.Galeano M, Manasseri B, Risitano G, et al. A free vein graft cap influences neuroma formation after nerve transection. Microsurgery. 2009;29:568. [DOI] [PubMed] [Google Scholar]
- 36.Swanson AB, Boeve NR, Lumsden RM. The prevention and treatment of amputation neuromata by silicone capping. J Hand Surg Am. 1977;2:70. [DOI] [PubMed] [Google Scholar]
- 37.Tupper JW, Booth DM. Treatment of painful neuromas of sensory nerves in the hand: a comparison of traditional and newer methods. J Hand Surg Am. 1976;1:144. [DOI] [PubMed] [Google Scholar]
- 38.Yan H, Zhang F, Kolkin J, et al. Mechanisms of nerve capping technique in prevention of painful neuroma formation. PLoS One. 2014;9:e93973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Woo SL, Urbanchek MG, Cederna PS, et al. Revisiting nonvascularized partial muscle grafts: a novel use for prosthetic control. Plast Reconstr Surg. 2014;134:344e. [DOI] [PubMed] [Google Scholar]
- 40.Sando IC, Leach MK, Woo SL, et al. Regenerative peripheral nerve interface for prostheses control: electrode comparison. J Reconstr Microsurg. 2016;32:194. [DOI] [PubMed] [Google Scholar]
- 41.Irwin ZT, Schroeder KE, Vu PP, et al. Chronic recording of hand prosthesis control signals via a regenerative peripheral nerve interface in a rhesus macaque. J Neural Eng. 2016;13:046007. [DOI] [PubMed] [Google Scholar]
- 42.Woo SL, Urbanchek MG, Leach MK, et al. Quantification of muscle-derived signal interference during monopolar needle electromyography of a peripheral nerve interface in the rat hind limb. Conf Proc IEEE Eng Med Biol Soc. 2014;2014:4382. [DOI] [PubMed] [Google Scholar]
- 43.Woo SL, Kung TA, Brown DL, et al. Regenerative peripheral nerve interfaces for the treatment of postamputation neuroma pain: a pilot study. Plast Reconstr Surg Glob Open. 2016;4:e1038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Isaacs J, Allen D, Chen LE, et al. Reverse end-to-side neurotization. J Reconstr Microsurg. 2005;21:43. [DOI] [PubMed] [Google Scholar]
- 45.Isaacs JE, Cheatham S, Gagnon EB, et al. Reverse end-to-side neurotization in a regenerating nerve. J Reconstr Microsurg. 2008;24:489. [DOI] [PubMed] [Google Scholar]
- 46.Al-Qattan MM. Prevention and treatment of painful neuromas of the superficial radial nerve by the end-to-side nerve repair concept: an experimental study and preliminary clinical experience. Microsurgery. 2000;20:99. [DOI] [PubMed] [Google Scholar]
- 47.Aszmann OC, Korak KJ, Rab M, et al. Neuroma prevention by end-to-side neurorraphy: an experimental study in rats. J Hand Surg Am. 2003;28:1022. [DOI] [PubMed] [Google Scholar]
- 48.Kuiken TA, Li G, Lock BA, et al. Targeted muscle reinnervation for real-time myoelectric control of multifunction artificial arms. JAMA. 2009;301:619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Kim PS, Ko JH, O’Shaughnessy KK, et al. The effects of targeted muscle reinnervation on neuromas in a rabbit rectus abdominis flap model. J Hand Surg Am. 2012;37:1609. [DOI] [PubMed] [Google Scholar]
- 50.Souza JM, Cheesborough JE, Ko JH, et al. Targeted muscle reinnervation: a novel approach to postamputation neuroma pain. Clin Orthop Relat Res. 2014;472:2984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bowen JB, Wee CE, Kalik J, et al. Targeted muscle reinnervation to improve pain, prosthetic tolerance, and bioprosthetic outcomes in the amputee. Adv Wound Care (New Rochelle). 2017;6:261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Poppler LH, Parikh RP, Bichanich MJ, et al. Surgical interventions for the treatment of painful neuroma: a comparative meta-analysis. Pain. 2018;159:214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Curtin C. Pain examination and diagnosis. Hand Clin. 2016;32:21. [DOI] [PubMed] [Google Scholar]
- 54.Simões EL, Bramati I, Rodrigues E, et al. Functional expansion of sensorimotor representation and structural reorganization of callosal connections in lower limb amputees. J Neurosci. 2012;32:3211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Stokvis A, Coert JH, van Neck JW. Insufficient pain relief after surgical neuroma treatment: prognostic factors and central sensitisation. J Plast Reconstr Aesthet Surg. 2010;63:1538. [DOI] [PubMed] [Google Scholar]
- 56.Karl A, Birbaumer N, Lutzenberger W, et al. Reorganization of motor and somatosensory cortex in upper extremity amputees with phantom limb pain. J Neurosci. 2001;21:3609. [DOI] [PMC free article] [PubMed] [Google Scholar]