

Supplemental Digital Content is available in the text.
Abstract
Background:
Breast animation deformity has sparked a reappraisal of the prepectoral implant placement in breast reconstruction. Our approach for direct-to-implant breast reconstruction (DIR) has evolved from a dual plane muscle/mesh coverage to a simple prepectoral hammock covering just the inferolateral part of the implant without the muscle. The aim of this study was to test the procedure in a prospective case series with emphasis on reconstructive outcome.
Methods:
Twenty-seven patients undergoing nipple- or skin-sparing mastectomy without subsequent radiation therapy requesting a primary implant-based reconstruction were included from May 2016 to April 2017. Median age was 46 years (25–67). We registered comorbidities, complications, and long-term results of successful or failed reconstruction.
Results:
Forty-seven DIR in 27 women, 20 bilateral, 7 unilateral. The median body mass index was 24 (17–31). The median time for mastectomy and DIR was 103 minutes (60–150). The inferolateral hammock consisted of Meso Biomatrix (34), Strattice (11), and Vicryl (2). The median implant size was 260 cc (140–345). Four complications (14%), 2 hematomas, 1 seroma, and 1 infection with partial nipple necrosis were all salvaged and reconstruction completed successfully. The median follow-up was 11 months (7–17).
Conclusion:
The prepectoral inferolateral hammock, a swift one-stage procedure with a quick recovery, creates promising results in the presence of an adequate skin flap. The simplicity of the method has made it the authors first choice for DIR.
INTRODUCTION
Implant-based breast reconstruction has evolved at a rapid pace over the last decade.1 The dual plane hammock of acellular dermal matrix (ADM) and pectoralis major muscle facilitated direct-to-implant reconstruction (DIR); now increasingly performed in combination with a biologic or synthetic mesh following skin- or nipple-sparing mastectomy.2–8 Recent focus on breast animation deformity has caused a shift toward less or no muscle involvement.9–15 Preliminary reports of successful prepectoral reconstructions consisting of variations of a full wrap around ADMs or deepithelialized inferior dermal flaps all favor the site change and indicate the importance of a full ADM coverage.14–18 We question the importance of full ADM coverage in DIR and feel strongly that the main purpose of the hammock is to provide an inferolateral support to the implant, alleviating the incision and recovering mastectomy skin flap.19–21 The aim of this feasibility study was to examine if prepectoral DIR could safely be achieved with a simple method of infero-laterally placed hammock using a single sheet of acellular matrix or mesh.
PATIENTS AND METHODS
We performed DIR in 27 women undergoing nipple-sparing or skin-sparing mastectomy without subsequent radiation therapy at Telemark Hospital, Norway, from June 2016 to April 2017. All operations were performed by the same team consisting of 1 breast surgeon and 1 plastic surgeon. The exclusion criteria were invasive cancer and planned postoperative radiation therapy. The median age was 46 years, range 25–67. We registered known risk factors and comorbidities, diabetes, hypertension, and smoking habits. Our primary outcome measure was the number of successfully completed reconstructions. The secondary outcome was complications: infection, hematoma, skin necrosis, and wound dehiscence. The study was performed in accordance with the principles outlined in the Declaration of Helsinki, and informed consent of participation was obtained.
Operative Technique
Mastectomy, either skin sparing (SSM) or nipple sparing (NSM) was carried out as we have previously described aided by hydrodissection.19,20 The inferolateral inframammary incision is our preferred approach to NSM, SSM is performed through a short periareolar incision extended laterally as required. Skin flaps were evaluated and deemed sufficient relying upon clinical observation. The mesh used for the hammock was either biologic or synthetic; 10 × 16 cm sheet of Meso Biomatrix Porcine-derived acellular peritoneal matrix, 8 × 16 cm sheet of Strattice Porcine derived ADM or 15 × 15 cm sheet of Vicryl, polyglactin absorbable net. The mesh was sutured with a running absorbable 2.0 suture along the lateral border of the intact pectoralis major muscle to define the lateral boundary of the breast reconstruction, to medialize the implant and prevent it from lateral migration (see video, Supplemental Digital Content 1, which displays a postoperative animation video of the patient. This video is available in the “Related Videos” section of the Full-Text article at PRSGlobalOpen.com or at http://links.lww.com/PRSGO/A860). The mesh was then inserted medially with a single 2.0 absorbable suture. One closed suction drain was placed laterally and upward along the superior implant border of each breast. The desired implant was placed into the hammock “pocket” in a craniocaudal direction before closing the hammock inferiorly using 2 or 3 interrupted absorbable 2.0 sutures along the inframammary fold. As a result, only about two-thirds of the bottom and lateral part of the implant is covered by the hammock depending on the size of the implant. The skin incision was closed in 2 layers with absorbable 3.0 monofilament sutures. Patients were hospitalized overnight and drain(s) kept until the daily production was less than 30 ml/24 hours. We used 1 perioperative dose of antibiotics and prescribed prophylactic oral Dicloxacillin 500 mg capsules 4 times per day until drains were removed.
Video Graphic 1.

See video, Supplemental Digital Content 1, which displays a postoperative animation video of the patient. This video is available in the “Related Videos” section of the Full-Text article at PRSGlobalOpen.com or at http://links.lww.com/PRSGO/A860.
RESULTS
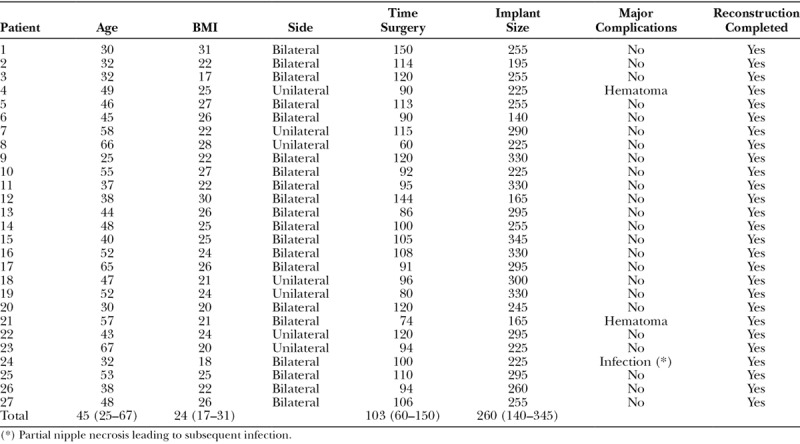
We used the prepectoral inferolateral hammock DIR method in 47 breasts of 27 women (Table 1). The reconstructions were bilateral in 20 cases and unilateral in 7. The mastectomies were prophylactic in 21 patients and therapeutic in 6; 42 NSM and 5 SSM. The hammock consisted of; Meso Biomatrix in 17 cases, Strattice in 9 cases and Vicryl in 1 case. The implants used were anatomical Mentor implants in 25 cases (41 breasts) and round shape Motiva Silk Surface in 3 cases (6 breasts). The median implant size was 260 cc (140–345). The median time for the procedure, mastectomy and immediate breast reconstruction, was 103 minutes (60–150). The median body mass index (BMI) was 24 (17–31). Three patients had major complications, 2 were reoperated for early postoperative hematoma and one due to a partial nipple necrosis and subsequent infection and was successfully salvaged with implant exchange and antibiotic treatment. One patient had a minor complication, a delayed wound dehiscence, which was resutured in the outpatient clinic: the patient was an abstaining smoker and the only smoker in this series. None of the included patients had hypertension, diabetes, or other comorbidities. The patients were discharged after an average of 2 days (1–4), and the drains were removed after 8 days (4–20). The median follow-up was 360 days, range 244–530 days.
Table 1.
Patient Demographic Data Are Displayed
DISCUSSION
In this series of 47 of prepectoral DIR, we have successfully used the inferolateral single sheet partial hammock to support of the implant in a one-stage approach, as opposed to recent articles presenting experience with a two-stage procedure and total coverage of the implant.11,14–17 The simplicity of the reconstruction enabled us to complete a bilateral mastectomy and DIR in a median time of 103 minutes or less than 2 hours in the majority of our cases with consistent results and no animation (Fig. 1; see video, Supplemental Digital Content 2, which displays a inferolateral Hammock reconstruction in 10 minutes. Operative procedure demonstrating DIR with inferolateral 8 × 16 cm Strattice Hammock and 330 cc moderate profile anatomical Mentor implant. This video is available in the “Related Videos” section of the Full-Text article at PRSGlobalOpen.com or at http://links.lww.com/PRSGO/A849). This is largely due to the simple and fast suturing of the mesh along the lateral pectoral border and inframammary fold as demonstrated in the operative video (Supplemental Digital Content 1). We recorded the time for 3 consecutive reconstructions in preparation of this article using a stop watch and confirmed that the time that it took to suture the mesh and place the implant was 5 minutes, leaving up to 5 minutes to close the incision, and thus complete the reconstruction in less than 10 minutes. We used 2 types of acellular meshes of porcine origin; one dermal and the other peritoneal and were unable to identify any difference in our patients’ outcome based on the different mesh types used in the hammock. We cannot make any assumptions in terms of the importance of total or partial mesh coverage, biological or synthetic, as this was not the aim of this study and would need to be tested in a comparative study.
Fig. 1.

The patient demonstrated in the operative video; a 43-year-old BRCA1 woman with preoperative (A–C) and 1-year postoperative (D–F) photographs after bilateral nipple-sparing mastectomy using inframammary fold incisions with immediate, permanent implant reconstruction using the 10-minute hammock reconstruction.
Video Graphic 2.

See video, Supplemental Digital Content 2, which displays a inferolateral Hammock reconstruction in 10 minutes. Operative procedure demonstrating DIR with inferolateral 8 × 16 cm Strattice Hammock and 330 cc moderate profile anatomical Mentor implant. This video is available in the “Related Videos” section of the Full-Text article at PRSGlobalOpen.com or at http://links.lww.com/PRSGO/A849.
The patient sample of this study was highly selected and consists largely of healthy women requesting prophylactic NSM and DIR, an optimal group of patients to test technical refinements and minimize possible confounders at the same time. We have previously published our experience regarding the importance of patient selection and how to overcome the challenge of large and ptotic breasts to make the mastectomy and DIR as safe as possible.19–21
We notice that patients reconstructed by this simple single sheet prepectoral DIR technique seem to experience no breast animation deformity, less postoperative pain, shorter time with drains, and quicker recovery and good cosmetic outcomes, which is in accordance with recently published reports of similar muscle sparing or prepectoral implant-based reconstructions.11,14–17 One down side is a risk of developing implant visibility over time, particularly in patients with low BMI, which we have observed in 4 (15%) patients so far. Similar findings have been reported by Lee et al.22 in 2012 and Sbitany et al.15 in 2017.
Long-term experience from breast augmentation indicates that there is a 2-fold increase in the risk of visible capsular contraction with subglandular compared with submuscular breast implant location.23 This may also turn out to be the case following breast reconstruction; however, we cannot expect to be able to answer the question regarding the risk of developing capsular contracture any time soon as the cumulative risk peaks after 5 years.24
Although the existing literature largely supports the advantage of a total coverage of the implant using a biologic acellular matrix sheet, this 1 year follow-up seems to indicate a satisfying outcome despite only a partial coverage.11,14–17
There are still many unanswered questions regarding the use of mesh for breast reconstruction and where to place the implant for optimal results. One important question is if the aesthetic results will be comparable with other reconstructive methods in the long run? This, however, requires comparative studies with a longer follow-up.
CONCLUSIONS
The partial implant coverage using a prepectoral inferolateral hammock technique is a simple, fast, and reliable method of DIR. The patients seem to experience less postoperative pain, shorter time with drains, and quicker recovery than we have experienced following the dual-plane DIR. The cosmetic outcomes seem to be just as favorable as other types of DIR that we have used over time. Patient selection is important as the thickness of the mastectomy flaps and comorbidity does play an important role for the successful outcome. Further studies and longer follow-up are required to compare long-term risks of capsular contracture, implant visibility, and the significance of different degrees of mesh coverage of the implant in different types of immediate breast reconstructive techniques.
Supplementary Material
Footnotes
Published online 2 October 2018.
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors’ institutions.
Supplemental digital content is available for this article. Clickable URL citations appear in the text.
REFERENCES
- 1.Spear SL. Underpromise. Plast Reconstr Surg. 2016;137:1961. [DOI] [PubMed] [Google Scholar]
- 2.Colwell AS, Damjanovic B, Zahedi B, et al. Retrospective review of 331 consecutive immediate single-stage implant reconstructions with acellular dermal matrix: indications, complications, trends, and costs. Plast Reconstr Surg. 2011;128:1170. [DOI] [PubMed] [Google Scholar]
- 3.Salzberg CA, Ashikari AY, Koch RM, et al. An 8-year experience of direct-to-implant immediate breast reconstruction using human acellular dermal matrix (AlloDerm). Plast Reconstr Surg. 2011;127:514. [DOI] [PubMed] [Google Scholar]
- 4.Dieterich M, Paepke S, Zwiefel K, et al. Implant-based breast reconstruction using a titanium-coated polypropylene mesh (TiLOOP Bra): a multicenter study of 231 cases. Plast Reconstr Surg. 2013;132:8e. [DOI] [PubMed] [Google Scholar]
- 5.Meyer Ganz O, Tobalem M, Perneger T, et al. Risks and benefits of using an absorbable mesh in one-stage immediate breast reconstruction: a comparative study. Plast Reconstr Surg. 2015;135:498e. [DOI] [PubMed] [Google Scholar]
- 6.Rodriguez-Unda N, Leiva S, Cheng HT, et al. Low incidence of complications using polyglactin 910 (Vicryl) mesh in breast reconstruction: a systematic review. J Plast Reconstr Aesthet Surg. 2015;68:1543. [DOI] [PubMed] [Google Scholar]
- 7.Salzberg CA. Direct-to-implant breast reconstruction. Clin Plast Surg. 2012;39:119. [DOI] [PubMed] [Google Scholar]
- 8.Salzberg CA, Ashikari AY, Berry C, et al. Acellular dermal matrix-assisted direct-to-implant breast reconstruction and capsular contracture: a 13-year experience. Plast Reconstr Surg. 2016;138:329. [DOI] [PubMed] [Google Scholar]
- 9.Becker H, Fregosi N. The impact of animation deformity on quality of life in post-mastectomy reconstruction patients. Aesthet Surg J. 2017;37:531. [DOI] [PubMed] [Google Scholar]
- 10.Hammond DC, Schmitt WP, O’Connor EA. Treatment of breast animation deformity in implant-based reconstruction with pocket change to the subcutaneous position. Plast Reconstr Surg. 2015;135:1540. [DOI] [PubMed] [Google Scholar]
- 11.Kobraei EM, Cauley R, Gadd M, et al. Avoiding breast animation deformity with pectoralis-sparing subcutaneous direct-to-implant breast reconstruction. Plast Reconstr Surg Glob Open. 2016;4:e708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bracaglia R, Tambasco D, Gentileschi S, et al. Triple-plane technique for breast augmentation: solving animation deformities. Aesthetic Plast Surg. 2013;37:715. [DOI] [PubMed] [Google Scholar]
- 13.Spear SL, Schwartz J, Dayan JH, et al. Outcome assessment of breast distortion following submuscular breast augmentation. Aesthetic Plast Surg. 2009;33:44. [DOI] [PubMed] [Google Scholar]
- 14.Sigalove S, Maxwell GP, Sigalove NM, et al. Prepectoral implant-based breast reconstruction: rationale, indications, and preliminary results. Plast Reconstr Surg. 2017;139:287. [DOI] [PubMed] [Google Scholar]
- 15.Sbitany H, Piper M, Lentz R. Prepectoral breast reconstruction: a safe alternative to submuscular prosthetic reconstruction following nipple-sparing mastectomy. Plast Reconstr Surg. 2017;140:432. [DOI] [PubMed] [Google Scholar]
- 16.Reitsamer R, Peintinger F. Prepectoral implant placement and complete coverage with porcine acellular dermal matrix: a new technique for direct-to-implant breast reconstruction after nipple-sparing mastectomy. J Plast Reconstr Aesthet Surg. 2015;68:162. [DOI] [PubMed] [Google Scholar]
- 17.Becker H, Lind JG, 2nd, Hopkins EG. Immediate implant-based prepectoral breast reconstruction using a vertical incision. Plast Reconstr Surg Glob Open. 2015;3:e412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ross GL. One stage breast reconstruction following prophylactic mastectomy for ptotic breasts: the inferior dermal flap and implant. J Plast Reconstr Aesthet Surg. 2012;65:1204. [DOI] [PubMed] [Google Scholar]
- 19.Gunnarsson GL, Børsen-Koch M, Wamberg P, et al. How to perform a NAC sparing mastectomy using an ADM and an implant. Gland Surg. 2014;3:252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gunnarsson GL, Børsen-Koch M, Arffmann S, et al. Successful breast reconstruction using acellular dermal matrix can be recommended in healthy non-smoking patients. Dan Med J. 2013;60:A4751. [PubMed] [Google Scholar]
- 21.Gunnarsson GL, Bille C, Reitsma LC, et al. Prophylactic nipple-sparing mastectomy and direct-to-implant reconstruction of the large and ptotic breast: is preshaping of the challenging breast a key to success? Plast Reconstr Surg. 2017;140:449. [DOI] [PubMed] [Google Scholar]
- 22.Lee JH, Lee PK, Oh DY, et al. Subpectoral-subfascial breast augmentation for thin-skinned patients. Aesthetic Plast Surg. 2012;36:115. [DOI] [PubMed] [Google Scholar]
- 23.Egeberg A, Sørensen JA. The impact of breast implant location on the risk of capsular contraction. Ann Plast Surg. 2016;77:255. [DOI] [PubMed] [Google Scholar]
- 24.Araco A, Gravante G, Araco F, et al. A retrospective analysis of 3,000 primary aesthetic breast augmentations: postoperative complications and associated factors. Aesthetic Plast Surg. 2007;31:532. [DOI] [PubMed] [Google Scholar]