

Abstract
Rationale:
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative multisystem disorder, presenting with limb or bulbar onset. To date, there is no cure for ALS. At some stage of the disease, patients may complain of breathlessness due to respiratory failure, thus needing a noninvasive mechanical ventilation (NIMV) support. However, breathlessness is a symptom that may be induced by different causes that must be taken into consideration in ALS management.
Patients concerns:
We report the case of an 81-year-old man, with a spinal onset ALS, who was admitted to our clinic to start NIMV because of respiratory involvement. After 3 weeks from NIMV performed at night time, with beneficial effects, he suddenly complained of breathlessness even at rest and in standing position.
Diagnosis:
Respiratory and cardiac assessments did not show new clinical events, indicating the worsening respiratory function. Due to a history of osteoporosis which was treated with biphosphonates and even though no previous bone trauma or falls were reported, we performed a spine computed tomography scan. The findings indicated multiple dorsal vertebral fractures which was a probable cause for breathlessness.
Interventions and outcomes:
Considering the neurodegenerative disease associated to respiratory failure, the cardiovascular risk factors and the age, the patient refused to undergo a surgery with kyphoplasty. A spine support was then prescribed, together with analgesic medications, with significant alleviation of pain and breathlessness.
Lessons:
The occurrence of breathlessness in a patient with ALS cannot always be related to the bulbar involvement. Other causes should be taken into account, especially when there is sudden worsening of symptoms in spite of good clinical response and compliance to NIMV treatment.
Keywords: amyotrophic lateral sclerosis, breathlessness, noninvasive mechanical ventilation, osteoporosis
1. Introduction
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative multisystem disorder, characterized by loss of cortical, brainstem and spinal motorneurons,[1] usually sparing cognitive, sensory, sexual, and sphincterial functions.[2] The main ALS presentations are the Limb-onset (70%), that is the most typical form, and the Bulbar-onset (25%), characterized by speech and swallowing difficulties. About 1% to 40% of patients with ALS may exhibit mild cognitive impairment with the clinical features of a fronto-temporal dementia.[3] Regardless of whether the onset of ALS is bulbar or spinal, most of the patients develop bulbar dysfunction as the disease progresses, until they become dependent on continuous noninvasive mechanical ventilation (NIMV).[4] Death usually results from respiratory failure due to denervation weakness in respiratory muscles,[5,6] besides pneumonia and/or aspiration pneumonia.[7] To date, there is no cure for ALS. NIMV has demonstrated to be useful to extend survival and relieve symptoms both related to respiratory impairment and muscle weakness and wasting.[5,8]
Osteoporosis is a disorder of the skeletal system where bone microarchitecture is affected and bone mass reduced. By definition, osteoporosis is present when bone mineral density is measured as 2.5 standard deviations or more below the mean of the young adult reference range.[9] Osteoporosis affects more than 200 million individuals worldwide,[10] and about 9 million osteoporotic fractures are noted each year.[11] Several risk factors have been considered responsible for osteoporosis, including lack of physical activity, calcium or vitamin D deficiency, female gender, age, smoking, and alcohol.[12] Moreover, several metals with neurotoxic properties affect bone mineralization and the hypothesis that such metals concurrently affect the skeletal and the nervous system has been shown.[12] However, literature on the coexistence of osteoporosis and ALS is scarce, and even in the clinical practice, such association has been rarely taken into consideration.
Herein, we report the case of an 81-year-old man affected by spinal onset ALS complicated by respiratory failure on NIMV, complaining sudden breathlessness and axial muscles weakness with back pain, not related to ALS muscle weakness, and wasting, but due to hidden multiple vertebral fractures.
2. Case report
The patient is an 81-year-old man, with a limb onset diagnosis of spinal ALS, since 3 years. Symptoms onset consisted of easy fatigability, progressive left lower limb weakness, and wasting with increasing difficulties in ambulation and frequent falls, and back pain. During the years, he developed respiratory failure so that he was admitted to our clinic to start NIMV. After 2 weeks from NIMV performed at night time, with a good compliance and clinical response, he suddenly started to complain fatigue worsening, even during speech, and breathlessness even at rest and in orthostatic position. Because of these symptoms, he underwent a thorax computed tomography (CT) scan, a specific investigation for respiratory problems, including arterial blood analysis and polysomnography, with a mild worsening of the respiratory picture as compared with the evaluations performed after 2 weeks from NIMV adaptation (Table 1). A cardiac investigation confirmed the previous ischemic heart disease with no new clinical events. Since he had a history of osteoporosis, treated with biphosphonates, even though no previous bone trauma or falls were reported, we decided to perform a spine CT scan, which showed multiple dorsal vertebral fractures. A bone densitometry was performed, revealing a low trabecular bone score (TBS), although the bone density was more severely affected T-score 2.8 (Fig. 1). Considering the neurodegenerative disease associated to respiratory failure, the cardiovascular risk factors, and the age, the patient refused to undergo surgery with kyphoplasty. A spine support was then prescribed (that the patient had to wear every time he reached the standing position), together with analgesic medications, thus alleviating pain and, consequently, breathlessness. Informed written consent was obtained from the patient for publication of this case report and accompanying images.
Table 1.
Arterial blood analysis and polysomnography before (T0), 15 (T15), and T30 days after noninvasive mechanical ventilation adaptation.
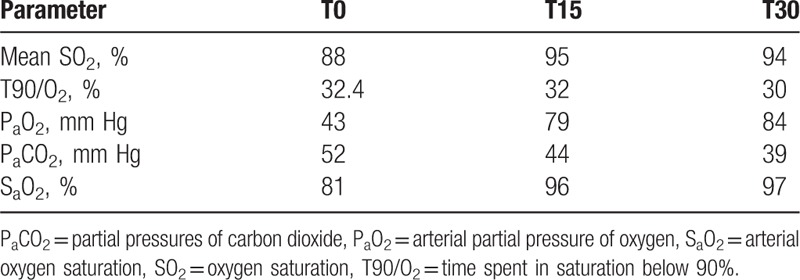
Figure 1.
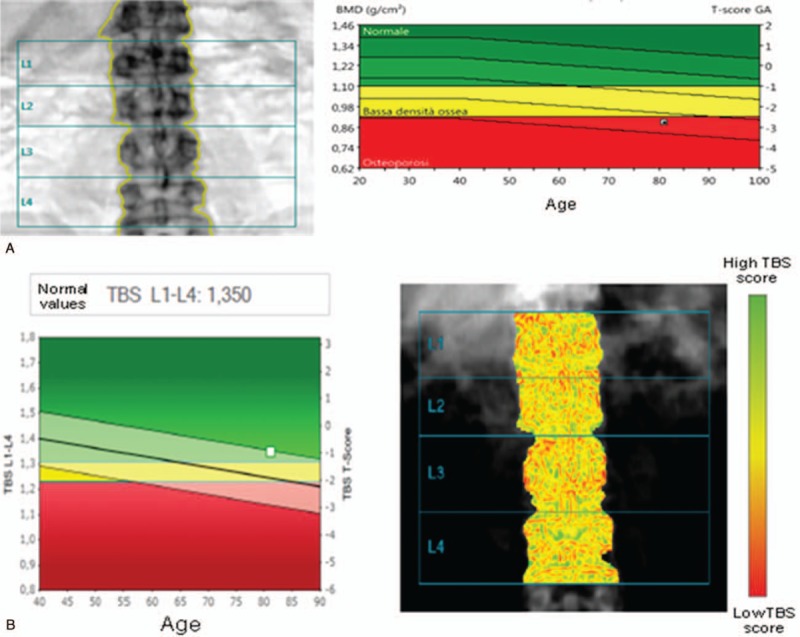
(A) Computerized bone mineralometry at L1-L4 level shows severe osteoporosis, with a very low bone mineral density score (0.889 g/cm2). (B) The bone composition and structure is also altered, as shown by the trabecular bone score (1.350), evaluated at L1-l4 level.
3. Discussion
The ALS is a progressive multisystem neurodegenerative disorder, characterized by loss of cortical motor neurons, brain stem, and spinal cord.[2] Bone mineral loss has been noted in ALS[13] and aberrant calcium metabolism and vertebral anomalies have been detected in a few patients with ALS.[14] There are some common features that may link ALS and osteoporosis, including the influence of several neurotoxic metals, such as lead,[10,15] and the age at onset.[1,16] Moreover, reduced mobility and weight loss due to ALS may worsen or induce osteoporosis.[16,17] In our case, it is worthy to note that, even though the Z-score at bone densitometry was suggestive for dorsal column osteoporosis associated to fractures, the TBS was normal, suggesting that the bone structure was still preserved (Fig. 1). Indeed, the FRAX algorithm, usually applied to estimate fracture risk, may be related to the neurodegenerative disease and the associated reduced muscle sustain and strength, which made the column instable. Moreover, in our patient, the back pain was initially attributed to axial muscle weakness and wasting, and breathlessness was related to a worsening of respiratory functions. After ruling out such hypothesis, considering that there was no worsening of the respiratory picture as compared with the evaluations performed after 2 weeks from NIMV adaptation, we concluded that breathlessness worsening was not related to the respiratory failure, but to the concurrent pain due to the underlying vertebral fractures, which limited chest mobility during normal breathing.
In conclusion, in patients with ALS and respiratory involvement, who complain of fatigue and breathlessness with a sudden worsening, associated to pain, we suggest to rule out the presence/worsening of osteoporosis and to carry out the proper rehabilitation and medication program.
Author contributions
Conceptualization: Simona Portaro, Maria Elena Santoro.
Data curation: Elisabetta Morini, Maria Accorinti, Antonino Naro.
Investigation: Elisabetta Morini, Pietro Marzullo.
Methodology: Maria Accorinti.
Supervision: Rocco Salvatore Calabrò.
Validation: Rocco Salvatore Calabrò.
Visualization: Rocco Salvatore Calabrò.
Writing – original draft: Simona Portaro, Maria Elena Santoro.
Writing – review & editing: Maria Accorinti, Antonino Naro, Rocco Salvatore Calabrò.
Footnotes
Abbreviations: ALS = amyotrophic lateral sclerosis, NIMV = noninvasive mechanical ventilation, TBS = trabecular bone score.
The authors have no funding and conflicts of interest to disclose.
References
- [1].Calvo AC, Manzano R, Mendonça DMF, et al. Amyotrophic lateral sclerosis: a focus on disease progression. Biomed Res Int 2014;2014:925101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Yoshizawa K, Yasuda N, Fukuda M, et al. Syntactic comprehension in patients with amyotrophic lateral sclerosis. Behav Neurol 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Consonni M, Iannaccone S, Cerami C, et al. The cognitive and behavioural profile of amyotrophic lateral sclerosis: application of the consensus criteria. Behav Neurol 2013;27:143–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Hadjikoutis S, Wiles CM. Respiratory complications related to bulbar dysfunction in motor neuron disease. Acta Neurol Scand 2001;103:207–13. [PubMed] [Google Scholar]
- [5].Bach JR. Amyotrophic lateral sclerosis: predictors for prolongation of life by noninvasive respiratory aids. Arch Phys Med Rehab 1995;76:828–32. [DOI] [PubMed] [Google Scholar]
- [6].Lyall RA, Donaldson N, Polkey MI, et al. Respiratory muscle strength and ventilatory failure in amyotrophic lateral sclerosis. Brain 2001;124:2000–13. [DOI] [PubMed] [Google Scholar]
- [7].Pisa FE, Logroscino G, Giacomelli Battiston P, et al. Hospitalizations due to respiratory failure in patients with amyotrophic lateral sclerosis and their impact on survival: a population-based cohort study. BMC Pulm Med 2016;16:136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Bourke SC, Tomlinson M, Williams TL, et al. Effects of non-invasive ventilation on survival and quality of life in patients with amyotrophic lateral sclerosis: a randomised controlled trial. Lancet Neurol 2006;5:140–7. [DOI] [PubMed] [Google Scholar]
- [9].Kanis JA. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report, WHO Study Group. Osteoporos Int 1994;4:368–81. [DOI] [PubMed] [Google Scholar]
- [10].Aaseth J, Boivin G, Andersen O. Osteoporosis and trace elements – an overview. J Trace Elem Med Biol 2012;26:149–52. [DOI] [PubMed] [Google Scholar]
- [11].Cooper C, Cole ZA, Holroyd CR, et al. Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int 2011;22:1277–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Roos PM. Osteoporosis in neurodegeneration. J Trace Elem Med Biol 2014;28:418–21. [DOI] [PubMed] [Google Scholar]
- [13].Sato Y, Honda Y, Asoh T, et al. Hypovitaminosis D and decreased bone mineral density in amyotrophic lateral sclerosis. Eur Neurol 1997;37:225–9. [DOI] [PubMed] [Google Scholar]
- [14].Mallette LE, Patten B, Cook JD, et al. Calcium metabolism in amyotrophic lateral sclerosis. Dis Nerv Syst 1977;38:457–61. [PubMed] [Google Scholar]
- [15].Chen X, Wang K, Wang Z, et al. Effects of lead and cadmium co-exposure on bone mineral density in a Chinese population. Bone 2014;63:76–80. [DOI] [PubMed] [Google Scholar]
- [16].D’Amelio P, Isaia GC. Male osteoporosis in the elderly. Int J Endocrinol 2015;5:907689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Vescini F, Attanasio R, Balestrieri A, et al. Italian association of clinical endocrinologists (AME) position statement: drug therapy of osteoporosis. J Endocrinol Invest 2016;39:807–34. [DOI] [PMC free article] [PubMed] [Google Scholar]