

Abstract
Objective
The aim of this study is to evaluate the efficacy and safety of a topical formulation containing lidocaine plus diclofenac (CLIFE1) compared to lidocaine (CLIFE2), to decrease pain in benign anorectal surgery (BARS) to date not evaluated. More than 50% of patients undergoing BARS, especially hemorrhoidectomy, suffer from moderate and severe postoperative pain. This remains an unresolved problem that could be addressed with the new CLIFE1 topical treatment.
Methods
A multicenter, randomized double-blind, active-controlled parallel-group superiority trial, was conducted in two Spanish hospitals. Patients undergoing BARS (hemorrhoids, anal fistula and anal fissure) were randomized at the end of surgery at a 1:1 ratio to receive first dose either CLIFE1 (n = 60) or CLIFE2 (n = 60) anorectal topical treatment, and after every 12 h for the first three postoperative days and once a day from the fourth to sixth. The primary outcome was average of pain decrease after topical treatment, measured with visual analogue scale (VAS) by the patients themselves, the evening in the surgery day and four times daily for the first three postoperative days.
Results
The results of 120 patients included out of 150 selected undergoing BARS show a decrease in pain after CLIFE1 topical treatment (7.47 ± 13.09) greater than with CLIFE2 (4.38 ± 6.75), difference −3.21 95% CI (−5.75; −0.68), p = 0.008, decreasing significantly postoperative pain ( ≥ 9 mm, VAS) in 35% of patients undergoing benign anorectal surgery, compared to 18.33 % treated with lidocaine.
Conclusions
The CLIFE1 topical treatment shows better analgesic efficacy than CLIFE2 in BARS.
Introduction
Reducing the high incidence of pain is a priority of health plans in Western countries1,2. More than 70% of patients undergoing surgery suffer moderate or severe postoperative pain, according to the surgical procedure3 even when they receive painkillers4. In benign anorectal surgery 50% of patients suffer from a higher level of pain than expected5,6 after hemorrhoidectomy7.
Sustained episodes of moderate and severe pain after surgery increase morbidity8 and risk to develop a chronic postoperative pain syndrome9,10. Despite postoperative pain remains an important unresolved issue11,12 that causes expense and patient dissatisfaction13, this problem has been addressed in the same manner over the last twenty years 14. Therefore this situation calls for multimodal pain management15, choosing medication, dosing regimens and route of administration in an individualized way to optimize efficacy and minimize adverse effects16, as the Practice Guidelines for Acute Postoperative Pain of the American Society of Anesthesiologists (ASA) recommends17.
Given postoperative pain in benign anorectal surgery (BARS) has not been solved in its entirety, some authors have used balms, creams and ointments18 that contain nifedipine19, diltiazem20, botulinum toxin21, or nitroglycerin22 in order to reduce spasms of the anal sphincter. It has also been used topical metronidazole ointment to decrease exacerbated pain from the third day onwards post-hemorrhoidectomy23. All these topical treatments help to reduce pain however they are not exempt from side effects such as headache, denervation, orthostatic hypotension or bradycardia24,25.
Other authors compare topical lidocaine alone26,27 or lidocaine plus prilocaine (EMLA cream)28 with a rectal diclofenac suppository administered in one dose by the surgeon at the end of hemorrhoidectomy. The results show higher analgesic efficacy for EMLA after the first two hours post-hemorrhoidectomy, however diclofenac is more effective in the evening after surgery and in the morning of the day after, as well as in reducing urinary retention events29.
Both lidocaine30 and diclofenac31–33 have analgesic, anti-inflammatory, and antibiotic effects. These properties are suitable to treat three postoperative pain components in BARS: nociceptive pain (somatic and visceral), inflammatory, and pain provoked by superinfection of the contaminated area34.
Postoperative pain management can be optimized by taking into consideration its physiopathology depending on the surgical procedure and the operated area. Thus including topical treatments within multimodal analgesic management in BARS aligns with PROSPECT group recommendations. These aim to improve postoperative pain analgesia and minimize side effects such as somnolence, dizziness, sickness and vomiting according to patient preferences.
Evidence shows that current postoperative pain management can be optimized by taking into account the pain causes and the operated area in each surgical procedure as the PROSPECT group recommends35. This new approach that incorporates topical analgesia within the multimodal strategy respecting patient preferences (like having a slight discomfort but without side effects such as drowsiness, dizziness or vomiting)36 meets their recommendations.
Since lidocaine and diclofenac have a synergistic analgesic effect37 and its combination has not been evaluated in postoperative pain so far, the double-blind randomized clinical trial “CLIFE-2010FV” was introduced to demonstrate that a fixed-dose combination of diclofenac sodium plus lidocaine (CLIFE1), is more effective than lidocaine alone (CLIFE2) to treat pain after BARS during the first postoperative week.
Methods
Ethics and Trial Registration
The CLIFE-2010FV clinical trial was conducted in 2 hospital centers [Viladecans Hospital (HV) and Bellvitge University Hospital (HUB)] from August 2011 to December 2013. The study was approved by the Ethics Committee of HUB (Comité Ético del HUB) and the Spanish Agency of Medicines and Medical Devices (la Agencia Española del Medicamento y Productos Sanitarios-AEMPS). All participants signed the informed consent form. The statistical plan and protocol are available in Supplement 1 and 2, respectively.
Study Design
The CLIFE-2010FV study design includes a multicenter, double-blind, randomized controlled clinical trial with parallel group superiority of CLIFE1 topical treatment (lidocaine plus diclofenac) versus CLIFE2 topical treatment (lidocaine) for postoperative pain treatment in benign anorectal surgery (BARS). The randomization was centralized and based on a computer-generated list with a 1:1 randomization ratio in blocks of 4 and stratified by center and surgery procedure to obtain two balanced arms, minimizing the confounding factors due to different levels of pain after BARS (fissurectomy, fistulectomy and hemorrhoidectomy surgeries).
Participants/Patients
All adult patients who participated in the study met the following inclusion criteria: patients undergoing BARS–hemorrhoidectomy (Milligan-Morgan technique), anal fissure (internal lateral sphincterotomy) or fistula surgery (fistulectomy) under lidocaine spinal anesthesia according to standard protocol. Patients with one of the following exclusion criteria were removed: pregnancy, incomplete spinal anesthesia, general anesthesia, the presence of allergy or intolerance to topical treatment ingredients, gastrointestinal inflammatory illness or active channel blockers).
Intervention
The patients were randomized to receive one of the two topical treatments in semi-solid formulation with an application on the anorectal area in an identical manner for both study groups. CLIFE1 topical treatment was composed of 15 grams of a fixed-dose combination containing 0.5% sodium diclofenac and 2% lidocaine (hydrochloride), and CLIFE2 topical treatment consisted of 15 grams of 2% lidocaine (hydrochloride). The study starts when the surgeon administrates the first topical treatment dose at the end of surgery, the subsequent doses are administrated by the patient in an identical manner as follows: once in the evening of the surgery day, twice daily (morning and evening) for the first three postoperative days, and one dose in the evening from the fourth to the sixth. In addition to the topical study treatment, all patients received the usual postoperative analgesia if there was any discomfort or pain (paracetamol / metamizole every 8 h, dolantine parenterally as rescue medication during hospitalization and trometamol orally at home).
Randomization was blinded for patients, surgeons, anesthesiologists and nurses who participated in the trial. They all followed the protocol, recorded data that were checked by external monitoring. All patients followed identical protocol of hygiene, postoperative surgical wound care and diet to avoid constipation.
Primary Efficacy Outcome
The primary variable is the mean of reduction in pain (pre-post topical treatment). Pain reduction is measured by calculating the difference in millimeters between the pain evaluated by the patient before and after each dose of topical treatment for the first three postoperative days and in the afternoon of the day of surgery, with the visual analog scale (VAS) (score range from 1 to 100 mm)38 and registered by the patient in the Self-Evaluation Pain Journal (Cuaderno de Autoevaluación del Dolor, CAD). Moreover, considering clinically relevant a pain reduction of at least 9 mm (value greater than 30% of the average VAS across all patients studied)39–41.
Secondary Outcomes
The following secondary variables were considered:
- Area under the curve (AUC) of the pain reduction on the first six postoperative days; from the fourth to the sixth day.
- Probability of reducing the pain intensity with the topical treatment, from severe (VAS > 75) to moderate (VAS 45–74) or mild (0–44)42. The pain relief after every topical treatment dose according to this relief scale [no relief (1), mild (2), moderate (3), important (4), complete (5)].
- Satisfaction survey in regard to the topical treatment effectiveness.
- Oral and parenteral analgesia consumption as usual and the rescue medication, at the hospital and at home.
- Clinical Global Impression Scale43 evaluation by the researcher.
- Time to the first void (TTFV) and adverse effects (AE), related or not with the topical treatment.
Data Collection
Patients scored pain intensity according to VAS scale, daily before and 45 min after the topical treatment (a timer was used after the topical treatment was applied), during the first postoperative week and they registered it in the Self-Evaluation Pain Journal (CAD).
The researcher during the final trial visit (on the seventh day) checked as follows: pain relief scores after every topical treatment dose, the TTFV, the patient satisfaction survey, the medication consumption of the topical treatment study, oral and parenteral analgesia and rescue medication, as well as concomitant medication according to specific patient conditions. The researcher also assessed the clinical Global Impression score, adverse effects, physical exam results, lab tests and electrocardiogram (EKG).
Sample Size
Sample size was calculated to detect a reduction of pain intensity of 20 units (SD 30) considering VAS scale (score range from 1 to 100), during the first three postoperative days with a two-sided for 5% significance level and a power of 80%, a sample size of 60 patients per group was necessary given an anticipated dropout rate of 10%.
Statistical Methods
The means (standard deviation), the absolute frequencies and percentages were calculated to describe the quantitative and qualitative variables, respectively.
A comparative analysis was conducted to evaluate differences between the quantitative variables of the two groups (CLIFE1, lidocaine plus diclofenac/CLIFE2, lidocaine) based on the Mann–Whitney U test. Analysis of the qualitative variables based on the Chi-squared independence test and the calculation of a 95% confidence interval (95% CI) for parameters corresponding to the effect.
In order to evaluate the probability of change from a higher pain level to a lower after topical treatment, stratification was predetermined according to a three-level pain score range (0–44, 45–74, and>75) and measured with VAS scale. Relative risk (RR) of the likelihood of improvement or get worse was calculated to compare the efficacy of the two topical treatments. These probabilities were obtained calculating the number of times that a decrease of pain was observed (from severe to moderate or mild pain and from moderate to mild pain), comparing the probability of progressing from a higher pain level to a lower pain level in each of both groups.
The area under the curve (AUC) of pain reduction according to VAS scale (0–100) was calculated for each patient, using the trapezoidal rule, analyzing the difference between groups using a Mann–Whitney test.
Cumulative distribution curves based on the methodology proposed by Farrar41 were drawn for each group during the first three and six postoperative days to compare the efficacy of topical treatment between both groups CLIFE1 and CLIFE2. On the x-axis, cut-off points (%) were represented based on 100% in reference to the maximum decrease of pain intensity in VAS scale (before/after topical treatment). On the y-axis, representing the proportion of patients (responders). The difference on the proportion of responders between both groups was specifically assessed at a 30% of pain decrease using a chi-squared test.
A logistic regression model was constructed to analyze the subgroups according to surgery type and the relative risk of reducing pain in at least 9 mm after topical treatment, adjusted by gender and surgery type. A chi-squared test was also used to assess significance.
A 5% significance level (p = 0.05) established and 95% CI were conveniently computed.
All analyses were performed using the R program. The efficacy analysis of the primary variable in per-intent-to-treat population was carried out, as well as a sensitivity analysis in per-protocol population.
Results
A total of 120 patients out of 150 selected undergoing BARS were included, of which 12 were excluded (6 per group) from the efficacy analysis per protocol (PP) (refer to the flow diagram of the study in Fig. 1).
Fig. 1.

Flow diagram Assessed for eligibility (n = 150). Flowchart of patients through the trial
The demographic and clinical baseline characteristics, as well as surgery type were distributed homogeneously in both groups, except gender (Table 1).
Table 1.
Demographic and clinical characteristics of the patients
| Characteristics | Overall (n = 120) | CLIFE1 (Lidocaine plus diclofenac) (n = 60) | CLIFE2 (Lidocaine) (n = 60) | p-value |
|---|---|---|---|---|
| Gender | ||||
| Male, n (%) | 72 (60.00) | 30 (50.00) | 42 (70.00) | 0.04a |
| Female, n (%) | 48 (40.00) | 30 (50.00) | 18 (30.00) | |
| Caucasian, n (%) | 116 (96.6) | 56 (93.33) | 60 (100.00) | 0.13a |
| Age, year mean (SD) | 47.55 (12.39) | 47.37 (11.79) | 47.73 (11.79) | 0.72b |
| BMI, kg/m2, mean (SD) | 26.46 (5.30) | 25.62 (5.99) | 27.31 (5.99) | 0.07b |
| ASA | ||||
| I, n (%) | 56 (46.66) | 30 (50.00) | 26 (43.33) | 0.24a |
| II, n (%) | 62 (51.66) | 28 (46.67) | 34 (56.66) | |
| III, n (%) | 2 (1.66) | 2 (3.33) | 0 (0.00) | |
| Type of surgery, n (%) | ||||
| Hemorrhoids, n (%) | 73 (60.83) | 36 (49.32) | 37 (50.68) | 0.66c |
| ♀ | 34 (46.57) | 22 (64.71) | 12 (35.29) | |
| ♂ | 39 (53.42) | 14 (35.90) | 25 (64.10) | |
| Anal fistula, n (%) | 34 (28.33) | 16 (47.06) | 18 (52.94) | |
| ♀ | 11 (32.35) | 6 (54.55) | 5 (45.45) | |
| ♂ | 23(67.64) | 10 (43.48) | 13 (56.52) | |
| Anal fissure, n (%) | 13 (10.83) | 8 (61.54) | 5 (38.46) | |
| ♀ | 3 (23.07) | 2 (66.67) | 1 (33.33) | |
| ♂ | 10 (76.92) | 6 (60.00) | 4 (40.00) | |
| Surgery time, min, mean (SD) | 18.79 (10.81) | 19.92 (10.16) | 17.67 (10.16) | 0.25b |
| Spinal lidocaine, mg, mean (SD) | 29.03 (11.99) | 29.53 (12.21) | 28.53 (12.21) | 0.55b |
SD standard deviation, BMI body mass index, ASA American Society of Anesthesiology, ♀ Female, ♂ Male
aObtained with the Chi-squared test (Pearson)
bObtained with the Mann–Whitney U test
cObtained with the Chi-squared independence test
The postoperative pain average of the total population included and the patients undergoing hemorrhoidectomy was below 30 mm (VAS scale 1–100).
Primary Outcomes
The average reduction in pain intensity (VAS scale) after topical treatment in the three first post-surgery days, is higher with the topical treatment CLIFE1 (diclofenac plus lidocaine) (7.47 ± 13.09) than topical treatment CLIFE2 (lidocaine) (4.38 ± 6.75), difference: −3.21, 95% confidence interval (95% CI): −5.75; −0.68, p = 0.008, adjusted p = 0.01.
The Area under the curve (AUC) analysis of pain reduction (VAS) post-treatment in the first three postoperative days also shows greater efficacy for CLIFE1 than for CLIFE2 in the intention-to-treat analysis (difference −17.53; 95% CI −33.20; −1.84; p = 0.02) (Table 2).
Table 2.
Effectiveness analysis, reduction of pain after topical treatment, according to VAS
| CLIFE1 (Lidocaine plus diclofenac) | CLIFE2 (Lidocaine) | Difference (95% CI) | p-valuea | |
|---|---|---|---|---|
| Intention-to-treat population | (n = 60) | (n = 60) | ||
| Reduction in pain after topical treatment (VAS) | ||||
| First 3 postoperative days, mean (SD) | 7.47 (13.09) | 4.38 (6.75) | −3.21 (−5.75; −0.68) | 0.008 |
| First 6 postoperative days, mean (SD) | 8.08 (14.50) | 4.26 (6.55) | −3.92 (−6.62; −1.22) | 0.004 |
| Reduction in pain after topical treatment (AUC) | ||||
| First 3 postoperative days, mean (SD) | 45.69 (45.15) | 28.16 (41.51) | −17.53 (−33.20; −1.84) | 0.02 |
| First 6 postoperative days, mean (SD) | 73.10 (74.77) | 40.38 (58.72) | −32.72 (−57.04; −8.40) | 0.006 |
| Per-protocol population | (n = 54) | (n = 54) | ||
| Reduction in pain after topical treatment (VAS) | ||||
| First 3 postoperative days, mean (SD) | 7.71 (13.20) | 4.9 (5.96) | −2.82 (−5.39; −0.24) | 0.03 |
| First 6 postoperative days, mean (SD) | 8.4 (14.73) | 4.76 (5.72) | −3.65 (−6.42; −0.89) | 0.01 |
| Reduction in pain after topical treatment (AUC) | ||||
| First 3 postoperative days, mean (SD) | 47.05 (46.05) | 30.71 (38.12) | −16.34 (−32.47; −0.20) | 0.047 |
| First 6 postoperative days, mean (SD) | 75.80 (76.47) | 43.94 (52.95) | −31.86 (−56.98; −6.72) | 0.01 |
SD standard deviation, AUC area under the curve, VAS visual analog scale
aObtained from Mann–Whitney U test
In the Fig. 2 it is observed that the relative risk of decreasing pain in at least 9 mm is almost double with the topical treatment CLIFE1 in the first three postoperative days and double in the first six days compared to the topical treatment CLIFE2 (in per-protocol population).
Fig. 2.
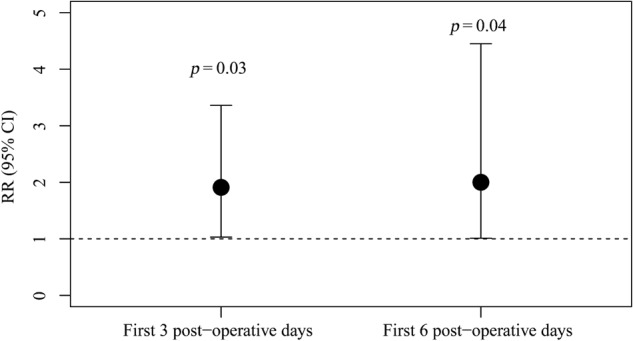
Effectiveness analysis, reduction of pain after topical treatment ≥ 9 mm VAS
The data shows that 35% of patients treated with topical treatment CLIFE1 had a statistically significant reduction ≥ 9 mm compared to 18.33% of patients treated with CLIFE2, RR = 1,91, 95% CI (1.01; 3.60), p = 0.03) (Table 3).
Table 3.
Effectiveness analysis, reduction of pain after topical treatment ≥ 9 mm VAS
| CLIFE1 (Lidocaine plus diclofenac) | CLIFE2 (Lidocaine) | RR | (95% CI) | p-valuea | |
|---|---|---|---|---|---|
| Intention-to-treat population | (n = 60) | (n = 60) | |||
| Reduction in pain after topical treatment ≥ 9 mm VAS | |||||
| First 3 postoperative days, n (%) | 21 (35) | 11 (18.33) | 1.91 | (1.01; 3.60) | 0.03 |
| First 6 postoperative days, n (%) | 19 (31.67) | 10 (16.67) | 1.9 | (0.97; 3.74) | 0.05 |
| Per-protocol population | (n = 54) | (n = 54) | |||
| Reduction in pain after topical treatment ≥ 9 mm VAS | |||||
| First 3 postoperative days, n (%) | 20 (37.03) | 10 (18.52) | 1.91 | (1.03; 3.86) | 0.03 |
| First 6 postoperative days, n (%) | 28 (33.33) | 9 (16.67) | 2 | (1.01; 4.05) | 0.04 |
VAS visual analog scale, RRrelative risk
aObtained from Chi-squared test
The maximum pain reduction value obtained is 83 mm of VAS (100%). The proportion of patients that show a greater cumulative reduction of pain (%) after the topical treatment CLIFE1 is always higher for any value of pain reduction than after the topical treatment CLIFE2 in the first three and six postoperative days (in the Fig. 3 it is observed by way of example: 30% of pain reduction affects 40% of patients treated with CLIFE1 and 20% of patients with CLIFE2, being this difference statistically significant, p = 0.02)41.
Fig. 3.

Cumulative distribution function curve for the two groups, during first three and six postoperative days41
The probability of progressing from a high pain level to a lower, according to VAS cut-offs (pain mild ≤ 44; moderate 45-74 and severe ≥ 75), is 1.43-fold higher in CLIFE1 topical treatment than in CLIFE2 (RR = 1.43, 95% CI 0.98; 2.09; p = 0.06).
Similar results are observed when the population is analyzed per-protocol. Results obtained when considering pain improvement at baseline and after day 1 to 6 are shown in Supplementary Table 1, likewise VAS average values on each of the timed points evaluated (before and 45 min after topical treatment) are shown in Supplementary Table 2, both suggesting an accumulative effect.
Secondary Outcomes
The average reduction in pain level, after topical treatment in the first six postoperative days, is significantly higher in the group treated with CLIFE1 (8.08 ± 14.50) than in the group CLIFE2 (4.26 ± 6.55) difference −3.92; 95% CI −6.62; −1.22; p = 0.004.
In the AUC analysis of pain reduction (VAS) after topical treatment in the first six postoperative days, showing also greater efficacy for CLIFE1 than for group CLIFE2, difference −32.72; 95% CI −57.04; −8.40; p = 0.006.
Moreover, the proportion of patients who show greater reduction in pain intensity for any difference evaluated, was higher in treatment CLIFE1 than in CLIFE2 for the first six days after surgery (Fig. 3)41
A higher reduction in pain levels is consistently observed after all the administrations of topical treatment CLIFE1 in BARS, without any change when stratifying by gender.
Analysis of subgroups by surgery
Patients undergoing hemorrhoidectomy have a higher postoperative pain level and also show greater pain reduction with the topical treatment CLIFE1 than with CLIFE2, difference −4.11, 95% CI −7.94, −0.29, p = 0.04, compared to those undergoing fissurectomy or fistulectomy, in which there is no statistically significant difference between topical treatments (Table 4).
Table 4.
Pain reduction with topical treatment according to surgery type: fissure, fistula, hemorrhoids
| Hemorrhoids | Fistulas | Fissures | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CLIFE1 | CLIFE2 | Difference (95% CI) | p-valuea | CLIFE1 | CLIFE2 | Difference (95% CI) | p-valuea | CLIFE1 | CLIFE2 | Difference (95% CI) | p-valuea | |
| Pain reduction after topical treatment (VAS) | ||||||||||||
| First 3 postoperative days, mean (SD) | 9.22 (15.00) | 6.24 (8.05) | −2.94 (-0.56;0.68) | 0.07 | 4.78 (8.63) | 1.98 (2.13) | −3.39 (−0.95;0.17) | 0.31 | 3.80 (7.38) | 0.79 (2.10) | −3.01 (−7.4;1.44) | 0.27 |
| First 6 postoperative days, mean (SD) | 9.93(16.34) | 5.72 (7.98) | −4.12 (−7.94;−0.28) | 0.04 | 5.65 (10.97) | 2.59 (2.19) | −3.62 (−7.8;0.58) | 0.29 | 2.98 (6.34) | 1.01 (1.72) | −1.97 (−.44;1.46) | 0.24 |
SD standard deviation, VAS visual analog scale
aObtained from Mann–Whitney U test
The stratified analysis presents similar efficacy in both genders, however it does not have sufficient statistical power to assess whether different levels of efficacy are associated to gender.
When adjusting by gender and surgery type displays a significant pain reduction of at least 9 mm of VAS, but only in women undergoing hemorrhoidectomy (73% with the topical treatment CLIFE1 compared to 32% with CLIFE2 [RR 2.30, 95% CI 1.08;4.90, p = 0.03] using data from the first six days.
The average perceived relief of pain is similar in patients in both groups. However, when pain level before topical treatment was between 40 and 70 mm (VAS scale), the relief level was significantly higher for the CLIFE1 group.
The clustering of patients who suffer a moderate or total pain relief on the seventh day reveal that 91% of the patients belong to CLIFE1 and 74% to CLIFE2 (p = 0.02). There was no significant difference in the evaluation of the Global Clinical Impression scale or the use of rescue analgesia between the two groups.
The satisfaction survey does not show statistically significant differences between topical treatments (90% satisfied or very satisfied in both groups), however there is a higher percentage of patients who report painless or slight discomfort in the group CLIFE1 (17%) compared to CLIFE2 (13%), while the 1% of dissatisfied patients belonged to the latter.
Time to First Void (TTFV)
There is no statistical significant difference in the TTFV between topical treatment groups [TTFV CLIFE1 = 282.66 (SD,132.47) minutes, TTFV CLIFE2 = 280.49 (SD, 132.47) minutes, p < 0.53], no correlation observed between TTFV and pain level. Nevertheless, TTFV was significantly lower in patients undergoing hemorrhoidectomy (three hemorrhoids) with topical treatment CLIFE1 than with CLIFE2 [CLIFE1 = 241.5 ± 131.95 min, p < 0.05; TTFV CLIFE2 = 473.67 ± 131.95 min].
Safety Evaluation
Both topical treatments are safe from the day of surgery until the seventh postoperative day. Nobody in either group had any adverse effects related with the topical treatment nor any sequels.
Discussion
The results of this clinical trial show that the topical treatment with a combination of a non-steroidal anti-inflammatory drug (NSAID) -diclofenac sodium plus a local anesthetic -lidocaine (CLIFE1) presents greater analgesic efficacy than the topical treatment with lidocaine alone (CLIFE2) during the first three postoperative days in benign anorectal surgery (BARS) and throughout the entire first week.
It should be highlighted the consistency of efficacy results that display analgesic advantage of the topical treatment CLIFE 1, exhibiting a greater pain reduction for any cut-off point, a larger percentage of patients who diminish 20% of pain intensity, (61% in patients with CLIFE1 treatment versus 32% of patients with CLIFE2 treatment, during first postoperative week)41 and a higher percentage of patients who reduce pain intensity in 9 mm or more of VAS (35% of patients in CLIFE1 versus 18.3% in CLIFE2)39,40.
The topical treatment CLIFE1 capitalizes on the analgesic synergy37, anti-inflammatory, and anti-microbial action of lidocaine and diclofenac30–33 to prevent sustained episodes of moderate and severe pain in hemorrhoids surgery, which is caused by the nociceptive stimulation of the surgical incision, its inflammation, the anal sphincter spasm and bacterial superinfection.
The new topical analgesic CLIFE1 is an instrument that allows postoperative analgesia specific in BARS, as it exhibits greater efficacy in painful surgical procedures like hemorrhoidectomy, in which postoperative pain remains an unsolved problem and affects more than 50% of patients, who would benefit from the topical treatment that addresses the problematic of the surgical wound, as the group PROSPECT recommends35.
There are no available studies with the new topical treatment CLIFE1 in BARS. However, there are studies in which topical lidocaine shows greater pain reduction than placebo, and combined with prilocaine (EMLA cream)28 provides earlier analgesia (two hours after the surgery) than a single dose of diclofenac post-hemorrhoidectomy. Likewise, diclofenac presents more effective late analgesia in the evening of surgery day and the day after. These results suggest that the analgesic superiority shown by the new topical treatment CLIFE1 compared to CLIFE2 (lidocaine) is underestimated, since lidocaine has an analgesic effect unlike a placebo. Thus the topical treatment CLIFE1 use proposal combines the analgesic effect of both early analgesia (lidocaine) and late analgesia (diclofenac), which is beneficial to treat postoperative pain after BARS.
The time to first void (TTFV) is similar in both topical treatment groups. However, when stratifying by gender and surgery type, women operated of three hemorrhoidal packs who received topical treatment CLIFE1 significantly diminish the TTFV (at almost half) versus the ones who are under CLIFE2. These results coincide with other studies which show a correlation between pain and micturition difficulties44, as well as with one study that displays a pain reduction and minor percentage of post-hemorrhoidectomy urinary retention, after a dose of rectal diclofenac administered by the surgeon at the end of the hemorrhoidectomy29.
The topical analgesia CLIFE1 has the advantage of being self-administered either at the hospital or at home during the first postoperative week, unlike the liposomal bupivacaine infiltration after hemorrhoidectomy, which is done by the surgeon in the operating room and its analgesic efficacy is limited to the first 72 postoperative hours with doses greater or equal to 260 mg, which causes greater side effects45,46.
The safety of the topical treatment CLIFE1 without side effects and the easy handling process by the patient themselves facilitate the treatment and the monitoring over a longer period if need be. While also avoiding hassles and complications derived from analgesic techniques with perfusion by catheter in the surgical wound15 which could require hospitalization or special care at home16.
Patients were randomly assigned to each topical treatment (CLIFE1 and CLIFE2) by surgery type to ensure an even distribution in each of the three surgical procedures (anal fistulectomy, anal fissurotomy and hemorrhoidectomy) with the same number of patients in each treatment group.
The number of patients undergoing hemorrhoidectomy was sufficient to identify the differences between both topical treatments studied, nonetheless the main limitation of this trial stems from the insufficient number of patients operated with fistulectomy and specially the scarce number of patients undergoing anal fissurotomy, as in none of these two surgical procedures the minimum potency to detect differences was reached.
Another limitation is the comparison of the topical treatment CLIFE1 under study with topical lidocaine instead of comparing it with placebo. This was dismissed in order to offer all patients some benefits with the topical treatment, regardless of which treatment was administered/assigned randomly and double-blind, which probably minimized the difference between topical treatments.
New studies with topical treatment CLIFE1 in BARS that include a larger number of patients and centers must be carried out to confirm and extrapolate our results to other settings, as part of a multimodal analgesic strategy to decrease postoperative pain, capitalizing on the synergistic action between diclofenac and lidocaine37 with minor adverse effects than the non-steroidal anti-inflammatory oral treatment47.
In conclusion, the new topical treatment with a formulation containing diclofenac plus lidocaine (CLIFE1) is shown to be safe and more effective than the topical treatment with lidocaine alone (CLIFE2) in the first three postoperative days and throughout the first week following BARS.
Study Highlights
WHAT IS CURRENT KNOWLEDGE
In benign anorectal surgery (BARS) 50% of patients suffer from a higher level of pain than expected, after hemorrhoidectomy.
Post-hemorrhoidectomy pain remains an unsolved problem notwithstanding the treatment with various balms, creams and ointments to reduce spasms of the anal sphincter.
WHAT IS NEW HERE
Topical analgesia with CLIFE1 gel (diclofenac plus lidocaine) takes into consideration the physiopatology of postoperative pain in BARS and is more effective than lidocaine gel.
TRANSLATIONAL IMPACT
Topical analgesia with CLIFE1 gel is clinically indicated to decrease pain after BARS, increasing patient satisfaction
Electronic supplementary material
Acknowledgements
We thank the operating room nurses of Hospital de Viladecans-HV and Hospital Universitari de Bellvitge-HUB, especially to Dr. Carmen López, Cristina Garzón and Anna Arellano for their professionalism and hard work coordinating, collecting data and monitoring patients during the first postoperative week they did support. We thank the entire CLIFE project field development team for their collaboration, including Igarreta MD, Dr. Martinez M, Aniorte MJ, Alvarez M, Rivilla P, Navarro A, López R, Beltran M, Guardado M, Minguzzi RM, Dr. Lopes P, Llauradó S, Mallol M, Nicolàs N, Frustrán N, Llorente MT, Lozano L, Quiñones C, Quillamon E, Vallejo L, Dr. Fraccalvieri D, Dr. Frago R, Dr. González D, Kaptoul D, Dr. Vallet J, Dr. Gil V, Dr. Sueiras A, and Vidal E. We thank Natalia Carrasco and Tomàs Casasin for their technical and regulatory collaboration. We thank Dr. Felip Pi for his support on the project from the initial stages. He was crucial to making it a reality. We thank the operating room secretaries, especially Conchi de Luis, for their collaboration. We are grateful to Dr. Montserrat Oliveras, Director of Viladecans Hospital for their organizational support, and Dr. Jaume Roigé, Head of the Anesthesiology Department. We are grateful to the following institutions for their support in this project:Department of Health (Ministerio de Sanidad), Social and Equality Services (Servicios Sociales e Igualdad) of Spain. ACCIÓ (Government of Catalunya- ACCIÓ, Generalitat de Catalunya). Carlos III Health Institute (Instituto de Salud Carlos III). European Regional Development Fund, ERDF (Fondo Europeo de Desarrollo Regional, FEDER). Viladecans Hospital (Hospital de Viladecans), Bellvitge Institute for Biomedical Investigation (IDIBELL), UICEC and Drug Development Services, UB (Servei de Desenvolupament del Medicament, UB). Funding: The Department of Health, Social and Equality Services of Spain and the Carlos III Health Institute funded the project through a competitive public tender. ACCIÓ (Government of Catalunya- ACCIÓ, Generalitat de Catalunya). European Regional Development Fund, ERDF (Fondo Europeo de Desarrollo Regional, FEDER). Centres de Recerca de Catalunya (CERCA)
Competing interests
Guarantor of the article The corresponding author Dr María José Linares Gil, assumes full responsibility for the study, has had access to the data, has control of the decision to publish and guarantees all authors have reviewed the final manuscript.
Specific author contributions MJL.L-G All authors meet the authorship ICMJE criteria, have made substantial contributions and have given final approval of the version to be published. Linares-Gil MJ, MD. PhD: Conception/Design, acquisition, obtaining funding, analysis or interpretation of data, drafting of the manuscript, critical revision of the manuscript for important intellectual content, and corresponding author. She has approved the final draft submitted. Valls J, BSc. PhD: Statistical analysis, acquisition, analysis or interpretation of data, drafting of the manuscript and critical revision of the manuscript for important intellectual content. He has approved the final draft submitted. Hereu-Boher P, MD PhD: Acquisition, analysis or interpretation of data, drafting of the manuscript and critical revision of the manuscript for important intellectual content. She has approved the final draft submitted. Nebot FJ, MD: Obtaining funding, acquisition, analysis or interpretation of data, drafting of the manuscript. He has approved the final draft submitted. De-Ramón B, MD PhD: Obtaining Funding, acquisition, analysis or interpretation of data, drafting of the manuscript. She has approved the final draft submitted. Díez-Munió E, B Pharm: Acquisition, tecnical and regulatory support, analysis or interpretation of data, drafting of the manuscript. She has approved the final draft submitted. Sanzol R, MD: Obtaining Funding, acquisition, analysis or interpretation of data, drafting of the manuscript. She has approved the final draft submitted. De-Oca FJ, MD PhD: Obtaining funding, acquisition, analysis or interpretation of data, drafting of the manuscript. He has approved the final draft submitted. Pérez-Lozano P, PhD: Obtaining funding, acquisition, analysis or interpretation of data, drafting of the manuscript. She has approved the final draft submitted. Suñé-Negre JM, PhD: Obtaining funding, acquisition, analysis or interpretation of data and drafting of the manuscript. He has approved the final draft submitted. García-Montoya E, PhD: Obtaining funding, acquisition, analysis or Interpretation of data and drafting and critical revision of the manuscript for important Intellectual content. She has approved the final draft submitted.
Financial support All these public institutions have collaborated funding the study through a competitive grant process yet the work has been completely independent from the fund sources. The Department of Health, Social and Equality Services of Spain and the Carlos III Health. Institute funded the project through a competitive public tender. ACCIO (Government of Catalunya- ACCIO, Generalitat de Catalunya). European Regional Development Fund, ERDF (Fondo Europeo de Desarrollo Regional, FEDER). CERCA (Centres de Recerca de Catalunya).
Potential competing interests Dr. Linares-Gil is the inventor of a patent null pending. The remaining authors declare that they have no conflict of interest.
Footnotes
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
The online version of this article (10.1038/s41424-018-0075-7) contains supplementary material, which is available to authorized users.
References
- 1.Dzau VJ, Pizzo PA. Relieving pain in America: insights from an institute of medicine committee. JAMA. 2014;312:1507–1508. doi: 10.1001/jama.2014.12986. [DOI] [PubMed] [Google Scholar]
- 2.Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11:770. doi: 10.1186/1471-2458-11-770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sommer M, et al. The prevalence of postoperative pain in a sample of 1490 surgical inpatients. Eur. J. Anaesthesiol. 2008;25:267–274. doi: 10.1017/S0265021507003031. [DOI] [PubMed] [Google Scholar]
- 4.Warfield AC, Kahn HC. Acute Pain Management: Programs in U.S. Hospitals and Experiences and Attitudes among U.S. Adults. Anesthesiology. 1995;83:1090–1094. doi: 10.1097/00000542-199511000-00023. [DOI] [PubMed] [Google Scholar]
- 5.Kushwaha R, Hutchings W, Davies C, Rao NG. Randomized clinical trial comparing day-care open haemorrhoidectomy under local versus general anaesthesia. BJS. 2008;95:555–563. doi: 10.1002/bjs.6113. [DOI] [PubMed] [Google Scholar]
- 6.Mehigan BJ, Monson JRT, Hartley JE. Stapling procedure for haemorrhoids versus Milligan-Morgan haemorrhoidectomy: randomised controlled trial. Lancet. 2000;355:782–785. doi: 10.1016/S0140-6736(99)08362-2. [DOI] [PubMed] [Google Scholar]
- 7.Gerbershagen HJ, et al. Pain Intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118:934–944. doi: 10.1097/ALN.0b013e31828866b3. [DOI] [PubMed] [Google Scholar]
- 8.Sinatra R. Causes and consequences of inadequate management of acute pain. Pain Med. 2010;11:1859–1871. doi: 10.1111/j.1526-4637.2010.00983.x. [DOI] [PubMed] [Google Scholar]
- 9.Tighe P, et al. Acute pain medicine in the United States: a status report. Pain Med. 2015;16:1806–1826. doi: 10.1111/pme.12760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cheetham MJ, Mortensen NJ, Nystrom PO, Kamm MA, Phillips RK. Persistent pain and faecal urgency after stapled haemorrhoidectomy. Lancet. 2000;356:730–733. doi: 10.1016/S0140-6736(00)02632-5. [DOI] [PubMed] [Google Scholar]
- 11.Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth. Analg. 2003;97:534–540. doi: 10.1213/01.ANE.0000068822.10113.9E. [DOI] [PubMed] [Google Scholar]
- 12.White PF, Kehlet H. Improving postoperative pain management what are the unresolved issues? Anesthesiology. 2010;112:220–225. doi: 10.1097/ALN.0b013e3181c6316e. [DOI] [PubMed] [Google Scholar]
- 13.Gan TJ, Habib AS, Miller TE, White W, Apfelbaum JL. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr. Med. Res. Opin. 2014;30:149–160. doi: 10.1185/03007995.2013.860019. [DOI] [PubMed] [Google Scholar]
- 14.Correll DJ, Vlassakov KV, Kissin I. No evidence of real progress in treatment of acute pain, 1993-2012: scientometric analysis. J. Pain Res. 2014;7:199–210. doi: 10.2147/JPR.S60842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vadivelu N, Kai AM, Kodumudi V, Berger JM. Challenges of pain control and the role of the ambulatory pain specialist in the outpatient surgery setting. J. Pain Res. 2016;9:425–435. doi: 10.2147/JPR.S86579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wu CL, Raja SN. Treatment of acute postoperative pain. Lancet. 2011;377:2215–2225. doi: 10.1016/S0140-6736(11)60245-6. [DOI] [PubMed] [Google Scholar]
- 17.Apfelbaum JL, et al. Practice guidelines for acute pain management in the perioperative setting: An updated report by the American society of anesthesiologists task force on acute pain management. Anesthesiology. 2012;116:248–273. doi: 10.1097/ALN.0b013e31823c1030. [DOI] [PubMed] [Google Scholar]
- 18.Rahimi R, Abdollahi M. A systematic review of the topical drugs for post hemorrhoidectomy pain. Int. J. Pharmacol. 2012;8:628–637. doi: 10.3923/ijp.2012.628.637. [DOI] [Google Scholar]
- 19.Agrawal V, Kaushal G, Gupta R. Randomized controlled pilot trial of nifedipine as oral therapy vs topical application in the treatment of fissure-in-ano. AJS. 2013;206:748–751. doi: 10.1016/j.amjsurg.2013.05.003. [DOI] [PubMed] [Google Scholar]
- 20.Amoli HA, Notash AY, Shahandashti FJ, Kenari AY, Ashraf H. A randomized, prospective, double-blind, placebo-controlled trial of the effect of topical diltiazem on post-haemorrhoidectomy pain. Colorectal Dis. 2011;13:328–332. doi: 10.1111/j.1463-1318.2009.02138.x. [DOI] [PubMed] [Google Scholar]
- 21.Patti R, et al. Improvement of wound healing after hemorrhoidectomy: a double-blind, randomized study of botulinum toxin injection. Dis. Colon Rectum. 2005;48:2173–2179. doi: 10.1007/s10350-005-0179-5. [DOI] [PubMed] [Google Scholar]
- 22.Hwang DY, Yoon SG, Kim HS, Lee JK, Kim KY. Effect of 0.2 percent glyceryl- trinitrate ointment on wound healing after a hemorrhoidectomy: results of a randomized, prospective, double-blind, placebo-controlled trial. Dis. Colon Rectum. 2003;46:950–954. doi: 10.1007/s10350-004-6692-0. [DOI] [PubMed] [Google Scholar]
- 23.Ala S, Saeedi M, Eshghi F, Mirzabeygi P. Topical metronidazole can reduce pain after surgery and pain on defecation in postoperative hemorrhoidectomy. Dis. Colon Rectum. 2008;51:235–238. doi: 10.1007/s10350-007-9174-3. [DOI] [PubMed] [Google Scholar]
- 24.Kocher HM, Steward M, Leather AJM, Cullen PT. Randomized clinical trial assessing the side effects of glyceryl trinitrate and diltiazem hydrochloride in the treatment of chronic anal fissure. BJS. 2002;89:413–417. doi: 10.1046/j.0007-1323.2001.02042.x. [DOI] [PubMed] [Google Scholar]
- 25.Brisinda G, Cadeddu F, Brandara F, Marniga G, Maria G. Randomized clinical trial comparing botulinum toxin injections with 0·2 per cent nitroglycerin ointment for chronic anal fissure. BJS. 2007;94:162–167. doi: 10.1002/bjs.5514. [DOI] [PubMed] [Google Scholar]
- 26.Perrotti P, Dominici P, Grossi E, Cerutti R, Antropoli C. Topical nifedipine with lidocaine ointment versus active control for pain after hemorrhoidectomy: results of a multicentre, prospective, randomized, double-blind study. Can. J. Surg. 2010;53:17–24. [PMC free article] [PubMed] [Google Scholar]
- 27.Rafiei M, Dehkhoda S, Ghergherehchi M, Shahvaraninasab A. Comparison of post- operative analgesia with preoperative topical lidocaine gel and lubricant gel in hemorrhoidectomy operation. Iran. J. Surg. 2008;15:28–33. [Google Scholar]
- 28.Rahimi M, Kazemeini AR, Pourtabatabaei N, Honarmand AR. Comparison of topical anesthetic cream (EMLA) and diclofenac suppository for pain relief after hemorrhoidectomy: a randomized clinical trial. Surg. Today. 2012;42:1201–1205. doi: 10.1007/s00595-012-0222-9. [DOI] [PubMed] [Google Scholar]
- 29.Placer GC, et al. Una sola dosis de diclofenaco intrarrectal reduce la retención urinaria tras la cirugía de las hemorroides. Resultados de un estudio clínico controlado y aleatorizado. Cir. Esp. 2008;83:301–305. doi: 10.1016/S0009-739X(08)70580-3. [DOI] [PubMed] [Google Scholar]
- 30.Cassuto J, Sinclair R, Bonderovic M. Anti-inflammatory properties of local anesthetics and their present and potential clinical implications. Acta Anaesthesiol. Scand. 2006;50:265–282. doi: 10.1111/j.1399-6576.2006.00936.x. [DOI] [PubMed] [Google Scholar]
- 31.Riordan JT, et al. Alterations in the transcriptome and antibiotic susceptibility of Staphylococcus aureus grown in the presence of diclofenac. Ann. Clin. Microbiol. Antimicrob. 2011;10:30. doi: 10.1186/1476-0711-10-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Reliski A, Dbrowiecki S, Gowacka K. The impact of diclofenac and ibuprofen on biofilm formation on the surface of polypropylene mesh. Hernia. 2015;19:179–185. doi: 10.1007/s10029-013-1200-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mazumdar K, Dastidar SJ, Park JH, Dutta NK. The anti-inflammatory non-antibiotic helper compound diclofenac: an antibacterial drug target. Eur. J. Clin. Microbiol. Infect. Dis. 2009;28:881–891. doi: 10.1007/s10096-009-0739-z. [DOI] [PubMed] [Google Scholar]
- 34.Molloy RG, Kingsmore D. Life threatening pelvic sepsis after stapled haemorrhoidectomy. Lancet. 2000;355:810. doi: 10.1016/S0140-6736(00)02208-X. [DOI] [PubMed] [Google Scholar]
- 35.Gray A, Kehlet H, Bonnet F, Rawal N. Therefore, postoperative pain management protocols may be optimised by examining procedure-specific outcomes. BJA. 2005;94:710–714. doi: 10.1093/bja/aei144. [DOI] [PubMed] [Google Scholar]
- 36.Gan TJ, et al. Patient preferences for acute pain treatment. Br. J. Anaesth. 2004;92:681–688. doi: 10.1093/bja/aeh123. [DOI] [PubMed] [Google Scholar]
- 37.Liedtke RK. Pharmacological concept for topical synergistic analgesia of peripheral neuromuscular pain. Arzneimittelforschung. 2006;56:108–114. doi: 10.1055/s-0031-1296710. [DOI] [PubMed] [Google Scholar]
- 38.Hjermstad MJ, et al. Studies are comparing numerical rating scales, verbal rating scales, and visual analog scales for assessment of pain intensity in adults: a systematic literature review. J. Pain. Symptom Manag. 2011;41:1073–1093. doi: 10.1016/j.jpainsymman.2010.08.016. [DOI] [PubMed] [Google Scholar]
- 39.Todd KH, Funk KG, Funk JP, Bonacci R. Clinical significance of reported changes in pain severity. Ann. Emerg. Med. 1996;27:485–489. doi: 10.1016/S0196-0644(96)70238-X. [DOI] [PubMed] [Google Scholar]
- 40.Olsen MF, et al. Pain relief that matters to patients: systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC Med. 2017;15:1–18. doi: 10.1186/s12916-016-0775-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Farrar JT. Advances in clinical research methodology for pain clinical trials. Nat. Med. 2010;16:1284–1293. doi: 10.1038/nm.2249. [DOI] [PubMed] [Google Scholar]
- 42.Hirschfeld G, Zernikow B. Variability of “optimal” cut points for mild, moderate, and severe pain: neglected problems when comparing groups. Pain. 2013;154:154–159. doi: 10.1016/j.pain.2012.10.008. [DOI] [PubMed] [Google Scholar]
- 43.Spearing MK, Post RM, Leverich GS, Brandt D, Nolen W. Modification of the global clinical impressions (CGI) scale for use in bipolar illness (BP): the CGI-BP. Psychiatry Res. 1997;73:159–171. doi: 10.1016/S0165-1781(97)00123-6. [DOI] [PubMed] [Google Scholar]
- 44.Toyonaga T, et al. Postoperative urinary retention after surgery for benign anorectal disease: potential risk factors and strategy for prevention. Int. J. Colorectal Dis. 2006;21:676–682. doi: 10.1007/s00384-005-0077-2. [DOI] [PubMed] [Google Scholar]
- 45.Gorfine SR, et al. Bupivacaine extended-release liposome injection for prolonged postsurgical analgesia in patients undergoing hemorrhoidectomy:a multicenter, randomized, double-blind, placebo-controlled trial. Dis. Colon Rectum. 2011;54:1552–1559. doi: 10.1097/DCR.0b013e318232d4c1. [DOI] [PubMed] [Google Scholar]
- 46.Hu DD, Singla EO, Kramer WG, Hadzic A. Pharmacokinetic profile of liposome bupivacaine injection following a single administration at the surgical site. Clin. Drug. Investig. 2013;33:109–115. doi: 10.1007/s40261-012-0043-z. [DOI] [PubMed] [Google Scholar]
- 47.Kienzle JL, Gold M, Nollevaux F. Systemic bioavailability of topical diclofenac sodium gel 1% versus oral diclofenac sodium in healthy volunteers. J. Clin. Pharmacol. 2010;50:50–61. doi: 10.1177/0091270009336234. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.