

Abstract
The representation of place is a key theoretical advancement that Geographic Information Science can offer to improve the understanding of environmental determinants of health, but developing robust computational representations of place requires a substantial departure from conventional notions of geographic representation in Geographic Information Systems (GIS). Unlike conventional GIS representations based on either objects or locations, we suggest place representation should incorporate dynamic subjective, experiential, and relational aspects of place, as the influence of place on health behavior concerns not only the features that can be objectively observed at a particular location but also the environmental perceptions of the individual, as molded by biological, social, and experiential characteristics. In addition, assessments of environmental exposures on health outcomes should focus on individuals’ time-activity patterns and microenvironment profiles, which form a potentially unique personalized exposure environment for each individual. Addressing these representational challenges via collaborative research has the potential to advance both Geographic Information Science and health research.
1 Introduction
This is an article about investigating the role of place in human health, and how Geographic Information Scientists can contribute to this investigation. We argue that theoretical advances in Geographic Information Science are key to addressing some of the most pressing challenges in health science. One concern, however, is that intersections with other fields outside of Geographic Information Science are often considered ‘applied GIS’ and relegated to second class status, a designation that has stunted the growth of our field, while other fields have made substantial theoretical advances on topics that are clearly within the realm of Geographic Information Science. This sentiment was captured eloquently by Jerry Dobson (2016) in his statement that “…geographic information scientists routinely create immensely valuable insights, data, methods, techniques, and tools that clearly advance science, but it’s mainly other disciplines that apply them to science theory…if we don’t use it ourselves, then we become merely the clerks of science” (emphasis ours). The consequence of this viewpoint is that the potential contribution of Geographic Information Science to major scientific and policy-relevant investigations is going unfulfilled. We certainly see this limitation in our own research on place and health, as it relates to topics associated with health behaviors, such as substance use, and exposure to environmental hazards, such as air pollution.
We note that health researchers have increasingly embraced Geographic Information Systems (GIS) and related geographic methods and technologies as they have become more accessible and more well-known (Richardson et al., 2013). Quantitative geographic approaches to health have expanded from a focus on the geographic distribution of disease to examinations of neighborhood effects on health to more theoretically informed models of the mediated and moderated mechanisms of how geographic contexts affect health outcomes (Diez-Roux and Mair, 2010; Macintyre et al., 2002; Rosenberg, 2016). Geospatial technologies have facilitated new health research incorporating individuals’ daily movements and georeferenced survey data on individuals’ health perceptions and behaviors.
Much of this quantitative, geographically oriented health research, however, remains rooted in a definition of place based on objectively defined observations of geographic context, such as the socioeconomic character of neighborhoods derived from census data. Of health research that incorporates individual perceptions of place, for example via survey data capturing the perception of neighborhood social cohesion or access to healthy food or recreation, the geographic aspect is often limited to georeferecing at the home location. This stands in contrast to the humanistic notion of place as a subjective and experiential relation that occurs between a person and location, and which has long been proposed as a key ingredient to understanding how place affects health (Kearns, 1993; Kearns and Moon, 2002). One simple and compelling reason for the sparsity of quantitative health research that incorporates this humanistic perspective on place is the lack of accessible place-based computational models and analytical tools in GIS – conventional GIS representations were simply not developed to support subjective and experiential notions of place, a critique also notably voiced by researchers interested in geographic issues of power relations, social justice, and the lived experience of individuals (Pickles, 1995; Crampton, 2010).
In the present paper we propose that the representation of place, as a dynamic, subjective, experiential, and relational entity, is a key theoretical advancement that Geographic Information Science can offer to improve the understanding of environmental determinants of health. We note that advancements in the capabilities and accessibility of GIS, GPS, and spatial statistics have led to a rapid expansion in the breadth and sophistication of health geography research over the past 20 years. Likewise, the development of a place-based GIS that supports the representation of human perceptions, experiences, and interactions with the environment would open the door to new lines of health geography research in the future, particularly those relating to health behaviors, environmental exposures, and interactions between individual and environmental mechanisms of disease. Developing robust computational representations of place, however, requires a substantial departure from conventional notions of representation in GIS. Here, we review research that introduces place representation into GIS-based health research, and offer several challenges to the Geographic Information Science community that we see as key to moving the place and health research agenda forward.
2 The Challenge of Representing Place in GIS and Health Geography
Arguably, the primary project, or mission, of the field of Geographic Information Science is geographic representation – the symbolic embodiment of the geographic world. We acknowledge that this idea is not particularly new. The idea of Digital Earth as described by Vice President Al Gore (1998) captures some of this idea, and indeed has been previously suggested as the grand challenge of Geographic Information Science (Goodchild, 2008), though the idea of Digital Earth would seem to focus somewhat explicitly on physical earth systems, as opposed to social or cultural characteristics. While the project of representation in Geographic Information Science is clearly oriented towards computational representation, it also encompasses visual and cognitive representation, as well as the societal and cultural implications of the ways in which geographic information is represented and used. The project of representation can also be interpreted to encompass geographic analysis, where statistical models, computational simulations, and data mining algorithms can be considered representations of real world phenomena, formalized as a set of rules or equations.
Some geographic things are harder to represent than others. Geographic objects which are simple, have a clear physical manifestation, have crisp boundaries, and do not typically change over time, such as parcel boundaries, are fairly easy to represent. Entities which are similar, but move through space over time, as with cars and other vehicles, are somewhat more difficult to represent, but the conceptual nature of representation is still straightforward. Representations get more difficult with geographic entities which can be conceptualized as a process, however, such as a traffic jam, which, while conceptualized as a single geographic entity, can simultaneously be conceptualized as composed of multiple moving objects, i.e. individual vehicles. Representation becomes even more challenging when the represented phenomenon is semantically ambiguous, as with a process such as gentrification, which is typically inferred indirectly from several separate, yet related occurrences, such as the opening of fancy coffee shops or a rapid increase in real estate prices due to speculation.
The representation of place in Geographic Information Science, however, is more challenging than any of these previously mentioned phenomena. Take, for instance, the representation of a ‘risky place’ or a ‘dangerous neighborhood.’ To some, such a designation might conjure in the mind a poor urban neighborhood, with physical indicators such as vacant housing, abandoned cars, graffiti, and liquor stores. Such are the features found in the image appearing on the cover of the American Journal of Psychiatry to depict risky urban environments, intended as an illustration of our research on neighborhood risks for substance use (Stahler et al., 2009). However, despite this depiction of, arguably, prototypical signifiers of urban neighborhood disadvantage and disorder, ascribing concepts of risk and danger to locations is not so simple. Consider a related research project where we asked approximately 250 adolescents residing in inner-city Philadelphia to name both a safe place they frequented as well as a risky place, where risk was defined as the likelihood of engaging in harmful behavior such as drug use or violence (Mennis and Mason, 2011). The most commonly named risky place turned out to be The Gallery, an indoor shopping mall in downtown Philadelphia which was a known gathering place for youth. Many subjects intimated that it was risky because of potential violence that could occur when different groups of youth intermixed in an unsupervised environment. One might conclude that The Gallery is a dangerous place. This was contradicted, however, by the fact that among the places listed by the adolescents as their safe place, The Gallery was also the most commonly named.
So, is The Gallery a risky place or a safe place? As it turns out, it depends to whom the question is asked, and this gets at the heart of why it is so challenging to represent place in Geographic Information Science. Unlike many geographic phenomena represented in GIS, such as parcel boundaries or elevation, place can be considered not an objective characteristic of a location to be observed, but a subjective experience that is created and interpreted (Elwood et al., 2013; Winter and Freksa, 2012). Thus, concepts such as ‘risky’ and ‘dangerous’ may not necessarily be qualities of locations themselves, but rather emerge from an individual’s subjective interpretations of that location. Such interpretations are derived in part from the characteristics and prior experiences of the individual. Therefore, computational representations of place need not conform to the object- or location-based conceptual models, where attributes are assigned to objects tethered to a location, or to locations directly themselves, that form the basis of computational representational structures in GIS.
Instead, the meaning of place can be considered to be subjective, experiential, and relational – it emerges from the interplay between a person and a location. The relational nature of place has been demonstrated in empirical research on place attachment (Brown et al., 2015) and is a feature in longstanding ideas about place in humanist geography. As Yi-Fu Tuan (1977) said, “Place may be said to have ‘spirit or ‘personality’ but only human beings can have a sense of place.” Importantly, subjective experiences and perceptions of one’s environment are no less relevant to understanding place than the physical features of the environment which can be readily observed visually. Indeed, when considering health behaviors, subjective experiences and perceptions may be more important than what can be ‘objectively’ observed via, say, census data, administrative data, business listings, or remotely sensed imagery. This idea is captured by sociologist Robert Sampson (2012) in his statement about the effect of neighborhood disorder on economic outcomes, “If you think something’s real, its consequences are real…shared perceptions of disorder lead to future rates of poverty. What this suggests is that perceptions, not just the reality of how many broken windows or broken beer bottles there are in the street really matter.”
In addition, the particular locations that hold meaning and are thus influential for an individual can be unique to each person; Each person has their own set of specific locations that compose their activity space – their home, the homes of their close friends and family, their workplace, and other places that serve particular functions such as shopping and leisure. This is of particular concern for investigations of place and health, where one is concerned with how characteristics of the environment influence individual health behaviors and outcomes (Kwan, 2009, Spielman and Yoo, 2009). Measurements of environmental exposure to health determinants can vary considerably according to an individual’s activities and movements over time. Thus, place representation in GIS ought to be concerned not only with the subjective and relational experience of place that can vary among individuals at a specific location in space, but also with the dynamic personalized expression of an individual’s activity space that determines the set of potential environmental exposures that is unique to each individual.
3 Theorizing and Capturing Place-Meaning and Health Behavior
A number of previous researchers have offered conceptual frameworks for how geographic characteristics influence a variety of health outcomes. In the context of substance use, Galea et al. (2005) describe how individual risky behaviors can be seen as a product of contextual characteristics, such as social norms and neighborhood disadvantage, which can influence substance use behaviors through mediating factors such as social networks and supports, all of which are influenced by policy and regulatory environments. In a similar manner, Northridge et al. (2003) distinguish between health factors at the macro level (e.g. climate and legal codes), community level (e.g. the built environment), and individual level (e.g. health behaviors).
Gee and Payne-Sturges (2004) describe a conceptual model of geographic factors and health with a focus on health disparities, in which they assert that residential segregation produces disparate exposures to community level stressors and resources that consequently impact individual level stress and related health outcomes. A somewhat similar perspective is offered by Diez-Roux and Mair (2010) who emphasize that residential segregation and associated inequalities in resource distribution result in differential exposure to physical and social neighborhood environments and, consequently, psychological stress and health behaviors. They note that these psychological states and behaviors can serve as mediators for each other, such as where stress precipitates a negative health behavior like smoking.
While these conceptual frameworks incorporate the idea that the effect of contextual characteristics on health outcomes are mediated and moderated by individual level characteristics, they tend to focus on objectively measurable characteristics of the environment, such as regulations or community level economic disadvantage, rather than on individuals’ perceptions of the environment, such as feelings of fear, safety, discrimination, or the types of social relationships that occur in particular places. Not surprisingly, geographers have offered some interpretations in this regard. The integration of humanistic notions of place with health research was described by Gesler (1992) through the concept of therapeutic landscapes, where landscapes are seen to confer health benefits (and risks) via not only structural forces, such as legacies of discrimination that have produced residential segregation, but also through the rituals, symbols, feelings of attachment, and personal experiences that tie an individual to a place.
Conradson (2005) argues for a relational interpretation of therapeutic landscapes – that the qualities of health risk and protection associated with a particular place should be seen as “…something that emerges through a complex set of transactions between a person and their broader socio-environmental setting.” (p. 338). This idea was also elucidated by Cummins et al. (2007), who emphasize the importance of investigating the unique and personalized exposures of individuals to place characteristics, and note that contextual effects operate at different spatial scales. They contrast what they call the conventional analytical approach, which emphasizes static and objectively defined measures of people and their environment, with the ‘relational’ approach, which emphasizes dynamic and relative measures of how people interact with their environment and each other. A related argument was made more recently by Wiese et al. (2018) who point out that representations of identity which assume static and immutable characteristics (e.g. race, gender), as is typical in medicine, would be improved by incorporating biographical characteristics that acknowledge the fluid and dynamic nature of identity and its relationship with health.
Building on this previous research, our view of how subjective and relational notions of place can be conceptualized to influence health behavior can be summarized as 1) through the physical, social, and emotional character of the places people encounter in their everyday lives, 2) as mediated by individuals’ interpretations of those places, and 3) where those interpretations are molded by individual characteristics and prior personal experiences. This interpretation fits not only with humanistic geography perspectives on the subjective experience of place as articulated by scholars such as Tuan (1977), but also with the social-ecological model of human development as proposed by Bronfrenbrenner (1979). This influential theoretical model situates the individual as residing within a set of nested contextual social and physical environments, termed the microsystem, mesosystem, exosystem, and macrosystem, in order of proximal to distal associations with the individual. Characteristics of these contexts include family, peers, and school within the microsystem to socioeconomic features of the neighborhood, the media, and cultural ideologies at the more distal levels.
Figure 1 presents a diagram of a conceptual model of place and health behavior, which provides examples of some of the mediated and moderated pathways through which neighborhood characteristics can influence health behaviors. It is not intended as a comprehensive framework but as an example of how place effects on health may be conceptualized. Here, we begin with the idea of a chain of causation that starts with place characteristics on the left side of the diagram, which influence an individual’s psychological state, which consequently influences a health behavior; i.e. the influence of place on health behavior is mediated by an individual’s psychological state. For example, exposure to community violence may cause psychological stress that causes substance use as a coping mechanism. That mediated relationship can be moderated, however, by other characteristics of the individual, such as their racial or ethnic identity, gender, prior life experiences, and their family and peer social contexts. For instance, given the example of substance use, the mediated effect of community violence on substance use via stress may differ depending on the level of family support to abstain from substance use.
Figure 1.
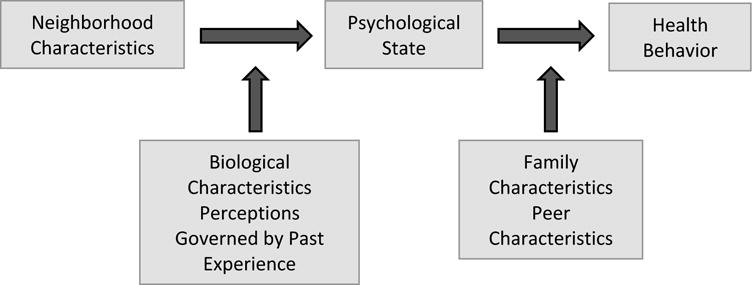
Conceptual model of mediating and moderating factors in how place can influence a health behavior.
Of course, neighborhood, biological, and social characteristics can also have direct effects on psychological state and health behaviors. For example, an individual’s past experiences can influence their psychological state, and family and social characteristics can directly affect health behaviors, e.g. an individual is more likely to use substances if their close friends are substance users. And these relationships among different characteristics can also occur in different directions. For instance, health behaviors can influence family and peer relationships, as with a situation in which an individual’s substance abuse disrupts family cohesion or causes psychological stress due to feelings of guilt or shame.
It is also important to point out the difference between mechanisms of influence and selection. Thus far we have described the conceptual model as consisting of contextual influences on psychological state and consequently health behavior, but individuals also choose where to live and spend their time, and with whom to be friends. These choices are also influenced by psychological state and health behaviors. For example, not only might an individual be influenced by their peers to use substances, but substance-using individuals might choose other substance users as friends.
One approach to capturing individual level data on subjective and relational experiences of place is through the extension of Ecological Momentary Assessment (EMA) to Geographic EMA, or GEMA. For readers unfamiliar with conventional EMA, it is a data collection technique that involves repeated sampling of participant’s behaviors, moods, social interactions, and experiences in real time, and in a subject’s natural environment, often delivered via brief surveys over a mobile phone (Shiffman et al., 2008). EMA has been widely used in ecological studies of health behaviors, including substance use, healthy eating, and exercise. Given that most mobile phones now have GPS technology embedded, it is possible to integrate the EMA survey methodology with synchronous location data to yield a rich spatial data set of locations with linked EMA responses. These ‘EMA locations’ can be considered the expression of an individual’s activity space, and can be linked to other geographic data from government censuses, business listings, remotely sensed imagery, and so on using GIS software, in order to investigate the influence of exposure to environmental characteristics on health (Kirchner and Shiffman, 2016). Though still in its infancy, GEMA has been used to investigate the influence of place characteristics on a variety of health indicators and outcomes, including psychological stress (Mennis et al., 2016), craving among recovering heroin uses (Epstein et al., 2014), alcohol use (Freisthler et al., 2014), and smoking (Kirchner et al., 2013).
We acknowledge that those in the Geographic Information Science community might think of collecting location information via mobile phones, in concert with EMA, as a technical, incremental advance. However, GEMA offers unprecedented opportunities to capture the personalized and subjective aspects of place for studies of health. Notably, it provides a means to connect momentary and in-situ information on an individual’s perceptions of their social and physical environment with their physical location. Kirchner and Shiffman (2016) state that GEMA is “most useful for the study of ‘places’ imbued with meaning by subjects – representing each subject’s personal eco-system” [emphasis ours]. This idea closely adheres to the humanistic geography perspective on place, where the meaning of place is actively constructed by individuals through their experiences and interactions with the features and people at a location. It also echoes theory regarding computational and visual representation in cartography and GIS, where the meaning of cartographic and GIS database symbols can be viewed in part as a process where the map reader or GIS software user brings their own prior experiences and cognitive interpretive framework to bear on understanding geographic representations encoded in maps and GIS databases (MacEachren, 1995; Peuquet, 2002).
4 Capturing Time-Activity Patterns using Personal Location Data
The significance of time-activity patterns, i.e. the locations and durations of time one spends at various places throughout daily life, have long been recognized as key to understanding environmental exposures linked to disease. Advanced technologies in sensing devices, such as GPS and accelerometers, that facilitate monitoring time-activity patterns at the individual level are now readily available. These light-weight and relatively low-cost devices have made it possible to accurately record individuals’ movements and infer their activities, enabling researchers to assess the influence of specific locations on health outcomes and behaviors. Examples include empirical studies on physical activity and the built environment (Kerr et al., 2011; Krenn et al., 2011; Saelens et al., 2003) and infectious disease transmission (Vazquez-Prokopec et al., 2013; Wesolowski et al., 2012), as well as environmental exposure (Nyhan et al., 2016, Rabinovitch et al., 2016). These developments in monitoring also align with research initiatives from the environmental health sciences on what has been termed the ‘exposome,’ the totality of an individual’s environmental exposures over the lifespan, which been recognized as key component to understanding chronic diseases (Wild, 2005), and which has recently been extended to the realm of GIS-based health research (Jacquez et al., 2015; Stahler et al., 2013).
In personal exposure assessment, the significance of activity space-based air pollution exposure estimates has long been recognized (Duan, 1982). One common traditional approach is to compile a person’s time-activity pattern based on personal diaries which record the location and times of daily activities, in combination with a direct or indirect measure of environmental air pollution concentrations. Diaries provide information on the time spent at various locations, so called ‘microenvironments,’ throughout the day. In the context of analyses of air pollution exposure, the microenvironment refers to a setting with homogeneous air quality, i.e. a spatial extent within which the air quality is assumed to be constant, and is a key concept underlying various models for human exposure to air pollution.
The individual’s exposure calculated as a time-weighted average of microenvironment air pollution concentrations can also be used to estimate the average exposure over a target population of interest in a model-based approach. Thus, misspecification of the microenvironment type in epidemiological studies is of great concern in exposure estimates (Spiegelman, 2010). A typical example of misspecification of the microenvironment is found in both time-series analyses of acute health effects and cohort studies of long-term health effects, where exposure was estimated at the location of participants’ residence. This is problematic because adults in the U.S. spend, on average, about half of their day away from home, and almost half of adult workers commute 25 minutes or more (Bureau of Labor Statistics, 2007). Many epidemiological studies have also shown that errors induced by using residence-based estimates of human health exposure to ambient air pollution serve to potentially underestimate health effects (Armstrong et al., 1998; Jerrett, et al., 2005; Miller et al., 2007; Navidi et al., 1995; Setton et al., 2011; Wilson, et al., 2005).
This issue of properly quantifying environmental exposure for health analyses has been identified by Kwan (2012) as the Uncertain Geographic Context Problem (UGCoP), the idea that the results of analyses of area-based characteristics on individual outcomes, as occurs with many studies of place and health, can differ depending on the delineation of the area based units. In studies of place and health, the UGCoP typically manifests as a problem of measuring the exposure of an individual to environmental characteristics. Efforts to address the issues of exposure misclassification and measurement error have typically been limited to fixing the problems at the stage of statistical analysis rather than improving the methodology of the exposure assessment itself. Moreover, most complex statistical methods developed to correct for such error and bias are based on strict assumptions of random error (Carroll et al., 2006; Spiegelman, 2010; Zeger et al., 2000), which are not generally applicable in practice.
In theory, microenvironments are a four-dimensional space-time concept, which allows researchers to utilize an individual’s time-activity pattern to capture exposure at the microenvironment level. We argue that this dynamic conceptualization of significant locations of individuals is likely to reduce exposure misclassification in epidemiological studies while at the same facilitating efficiency in individual level exposure sampling and monitoring efforts.
Researchers in Geographic Information Science have made key advances on monitoring human mobility using geospatial technologies, and have developed new methods and concepts for monitoring the movements of individuals and their everyday exposure to environmental air pollution in space and time (Glasgow et al., 2016; Park et al., 2017; Steinle et al., 2013;). As shown in Yoo et al. (2015), the time-location data obtained from participants’ GPS-equipped smart phones could be used to develop mobility-based estimates of individual exposures to ambient air pollution. Similarly, the classification of activities based on GPS tracking data can be used to improve the estimation of indoor air quality, given that the indoor air quality of a location is dynamic and changing over time, and is dependent on the activities that occur at that location and time. For example, pollutant concentration levels at a particular location, such as a home, are higher when cooking activities occur as compared to during other activities, such as reading or sleeping. This is important because individuals spend up to 90% of their time indoors. Combined with state-of-the-art techniques, such as a random forest decision tree model (Yoo and Eum, 2016; Wu, et al., 2011), the concepts from classical time-geography, such as a space-time prism, have the potential to offer an efficient means of quantifying and summarizing individuals’ time-activity patterns (Miller, 2007). A better understanding of human spatial behaviors, captured through time-activity pattern monitoring, can assist investigators to identify the optimal number and types of key microenvironments for environmental exposure assessment at the individual level (Branco et al., 2014).
5 Challenges and Opportunities for Geographic Information Science
We suggest five challenges for the Geographic Information Science community to advance its contribution to the study of place and health. First, the development of sophisticated and coherent computational models of humanistic aspects of place, a ‘platial’ GIS (Goodchild, 2015), is sorely needed. We note recent Geographic Information Science research on extracting place information from linguistic descriptions, formalizing computational notions of place, spatializing sense of place characteristics, georeferencing place data, and reasoning with place data (Acedo et al., 2017; Gao et al. 2013; Mackaness and Chaudhry, 2013; Scheider and Janowicz 2014; Vasardani et al. 2013). Much of this research, however, addresses relatively constrained computational research questions, such as techniques for extracting place-names from social media data. We suggest that this research can be leveraged to develop a more comprehensive framework for the computational representation of the dynamic, subjective, experiential, and relational aspects of place. This perspective on place representation also aligns with the set of emerging themes in Geographic Information Science research elicited by Sui (2015), which emphasize narrative and synthetic approaches. Similarly, well-defined models of the personalized activity spaces of individuals would allow investigators to save the time and resources needed to measure environmental exposure at the individual level (Jarup, 2004).
The second challenge is to operationalize these computational models of place in integrated geographic data sets which capture activity spaces, social networks, and perceptions and interactions of individuals with place. While we suggest above that GEMA provides one approach for developing such data sets, the integration of geocoded momentary survey responses with more conventional GIS data does not begin to get at the potential for the use of georeferenced imagery, narrative text, social media and other ‘unconventional’ place-based data sets for studies of place and health. Recent advances in qualitative GIS may point some way forward for integrating and encoding these disparate types of place data for health studies (Cope and Elwood, 2009; Kwan and Ding, 2008; Mennis et al., 2013).
The third challenge is to develop geospatial analytical approaches that will enable us to more fully test for cause and effect, and distinguish mechanisms of influence and selection. Traditional GIS applications or spatial modeling in spatial epidemiology have primarily focused on available (collected) data using disease mapping and disease clustering techniques (Lawson 2006). However, the potential of GIS in health research extends beyond its functionality for data storage, retrieval, and presentation in descriptive analysis. Improving the representation of place in GIS will offer support for key health questions, such as the health impacts of unexpected events, such as natural disasters, and the diffusion of disease through social networks or environmental pathways (Bian, 2013; Lawson et al., 2016). Recent advances in dynamic network modeling of linked social-spatial data may offer some way forward here (Andris, 2016; Zhong and Bian, 2016). Additionally, the application of machine learning to space-time trajectory data has enabled researchers to improve their understanding of individuals’ time-activity patterns by classifying a sequence of time-stamped location records (Zheng et al., 2010; Yoo and Eum, 2016). And Bayesian spatial and spatio-temporal geostatistical models (Diggle and Ribeiro 2002; Banerjee et al. 2004; Cressie and Wikle 2011), in combination with the integrated nested Laplace approximations (INLA) approach (Rue et al., 2009), have allowed environmental scientists to estimate air pollutant concentrations along individuals’ space-time trajectories while taking into account uncertainty in the estimations of parameters and predictions.
Statistical mediation and moderation can be used to account for both the complex pathways by which the subjective experience of place influences health as well as the different effects place characteristics may have depending on individual-level characteristics (including one’s prior experiences). Advances in longitudinal modeling, such as with the time varying effect model (TVEM) which assesses temporal fluctuations in relationships among variables (Li et al., 2017), can be extended to incorporate place-based characteristics (Mason et al., 2016). Other relevant advances include the development of mediated and moderated multilevel longitudinal growth models for analyzing EMA data (Bolger and Laurenceau, 2013), and techniques for disaggregating within- and between-person effects in multilevel longitudinal data analysis (Curran and Bauer, 2011). To our knowledge, however, it is rare, to see such techniques applied to repeated sampling designs where multiple within-subject observations are acquired both over time and throughout space, as with GEMA-based studies. The development of accessible software tools for applying these types of analytical techniques to such data would represent a substantial advance in the ability to disentangle mechanisms of influence and selection, as well as composition and context, in analyses of place and health.
The fourth challenge concerns the recent substantial initiatives in the Geographic Information Science community (as well as in health research) on Big Data, or Data Science, as a research paradigm. In a recent keynote presentation to the University Consortium for Geographic Information Science, speaker Damian Gessler (2016) stated that “The advent of Big Data in the early decades of this century may have as large an effect on the century’s science as the advent of grand theories did at the beginning of the previous century.” Mr. Gessler demonstrated the efficacy of big data analytics using a recent video of a rocket manufactured by SpaceX landing on its base on a small platform in the ocean. The video, along with much other research utilizing big data approaches, suggests the power of big data analytics for identifying optimal solutions to well-defined problems, such as those in engineering and business. Given the personalized, subjective, and relational nature of place outlined above, however, challenges remain in applying big data analytics to the understanding of why and how place influences health behaviors and outcomes through the constructed and subjective place-meanings people create. Perhaps the recent interest among Geographic Information Science researchers in the analysis of georeferenced social media data, including text and imagery, offers a way forward in assessing collective and subjective experiences of place. Relatedly, the question of how to integrate the new types, and large quantity, of data obtained from multiple, disparate sources, such as electronic health records, and crowd-sourced and personal location data, remains a challenge.
The fifth challenge is associated with the scale of analysis in health research. A proper representation of space and time in spatial epidemiology is important for data collection and analysis, as it affects interpretations of findings. For example, how often and how long exposure measurements are collected will determine the spatial resolution of microenvironments over which personal exposure is assessed. While the issue of scale is widely recognized as one of the most fundamental issues in Geographic Information Science (Goodchild, 2001), most GIS-based health research addressing issues of scale have focused on sparse data interpolation or missing data imputation, as with aggregate data made available only over aggregated time periods or coarser resolution. Perhaps involving Geographic Information Scientists during the design phase of health research may ameliorate some of the scale-related challenges that often are only discovered during the analysis phase of the project, after the data collection is competed. Research on the implications of the resolution and scope of spatial and temporal sampling frameworks on assessments of personalized environmental exposures to support place and health research is necessary. Simultaneously, a significant challenge of using/collecting personal location data is on the protection of individuals’ privacy. Geographical masking (Armstrong, et.al., 1999) has been proposed to address the issue between data accuracy and personal privacy, but warrants further studies on more rigorous and reliable methods.
6 Beyond the Clerks of Science
In returning to Jerry Dobson’s concern about being the ‘clerks of science,’ we suggest that Geographic Information Science researchers interested in health should not limit themselves to the technical, algorithmic, or computational challenges of health data analysis, but also contribute to the development of theories of the definition and computational representation of place, itself, and its role in health outcomes. Indeed, Geographic Information Science researchers should recognize that substantive theoretical advances in place and health may be made possible by even incremental technological advances in Geographic Information Science, and also that theoretical questions in place and health may help drive advances in Geographic Information Science. Further, the operationalization of theories concerning place and health in novel data and analytical representations is a key contribution to place and health research to which Geographic Information Science researchers are uniquely qualified. Developing more sophisticated computational representations of place that incorporate the subjective and relational aspect of place-meaning would be a key advance in Geographic Information Science that would also contribute to a better understanding of how environmental characteristics interact with biological determinants to influence health outcomes – one of the most pressing contemporary questions in health science.
Importantly, the type of Geographic Information Science research advocated for here is not ‘applied GIS.’ Rather, we are advocating for the development of novel representational and analytical approaches in Geographic Information Science that are necessary to address research questions in the health domain that overlap with longstanding challenges in Geographic Information Science. We would also add that this type of research necessarily demands ‘deep’ collaboration with health researchers, by which we mean a collaborative environment where Geographic Information Science researchers are not the technical problem solvers, data handlers, or analysts on a health research team but actively contribute to the design of the study and the theoretical development of the domain under investigation itself. Conversely, domain health researchers should understand and appreciate that health research that uses cutting edge geospatial technologies can contribute to advancing Geographic Information Science. While admittedly it can take a long time to develop such collaborative relationships and domain knowledge outside of Geographic Information Science, interdisciplinary synthesis has often been at the heart of scientific innovation, Geographic Information Science included.
Acknowledgments
We would like to thank Dr. John Wilson for the invitation to present the Transactions in GIS Plenary Presentation at the 2017 American Association of Geographers Annual Meeting, from which this paper was adapted, as well as the anonymous reviewers for their helpful and constructive comments. This research is partially supported by grant R01GM108731 from the National Institute of General Medical Sciences of the National Institutes of Health (NIH/NIGMS) awarded to the second author.
References
- Acedo A, Painho M, Casteylen S. Place and city: Operationalizing sense of place and social capital in the urban context. Transactions in GIS. 2017;21(3):503–520. [Google Scholar]
- Armstrong MP, Rushton G, Zimmerman DL. Geographically masking health data to preserve confidentiality. Statistics in medicine. 1999;18(5):497–525. doi: 10.1002/(sici)1097-0258(19990315)18:5<497::aid-sim45>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- Andris C. Integrating social network data in GISystems. International Journal of Geographical Information Science. 2016;30(10):2009–2031. [Google Scholar]
- Armstrong BG. Effect of measurement error on epidemiological studies of environmental and occupational exposures. Occupational and Environmental Medicine. 1998;55(10):651–656. doi: 10.1136/oem.55.10.651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Banerjee S, Carlin BP, Gelfand AE. Hierarchical modeling and analysis for spatial data. CRC Press; 2014. [Google Scholar]
- Bian L. Spatial approaches to modeling transmission of communicable diseases – a review. Transactions in GIS. 2013;17(1):1–17. [Google Scholar]
- Bolger N, Laurenceau JP. Intensive Longitudinal Methods: An Introduction to Diary and Experience Sampling Research. New York: Guilford Press; 2013. [Google Scholar]
- Branco PTBS, Alvim-Ferraz MCM, Martins FG, Sousa SIV. The microenvironmental modelling approach to assess children’s exposure to air pollution–A review. Environmental Research. 2014;135:317–332. doi: 10.1016/j.envres.2014.10.002. [DOI] [PubMed] [Google Scholar]
- Bronfenbrenner U. The Ecology of Human Development: Experiments by Nature and Design. Cambridge, MA: Harvard University Press; 1979. [Google Scholar]
- Brown G, Raymond CM, Corcoran J. Mapping and measuring place attachment. Applied Geography. 2015;57:42–53. [Google Scholar]
- Department of Labor, editor. Bureau of Labor Statistics. American Time Use Survey. Bureau of Labor Statistics; 2007. [Google Scholar]
- Conradson D. Landscape, care and the relational self: Therapeutic encounters in rural England. Health and Place. 2005;11(4):337–348. doi: 10.1016/j.healthplace.2005.02.004. [DOI] [PubMed] [Google Scholar]
- Cope M, Elwood S, editors. Qualitative GIS: A Mixed Methods Approach. London: Sage; 2009. [Google Scholar]
- Crampton J. Mapping: A Critical Introduction to Cartography and GIS. Oxford and New York: Wiley-Blackwell; 2010. [Google Scholar]
- Cressie N, Wikle CK. Statistics for spatio-temporal data. John Wiley & Sons; 2015. [Google Scholar]
- Cummins S, Curtis S, Diez-Roux AV, Macintyre S. Understanding and representing ‘place’ in health research: a relational approach. Social Science & Medicine. 2007;65(9):1825–1838. doi: 10.1016/j.socscimed.2007.05.036. [DOI] [PubMed] [Google Scholar]
- Curran PJ, Bauer DJ. The disaggregation of within-person and between-person effects in longitudinal models of change. Annual Review of Psychology. 2011;62:583–619. doi: 10.1146/annurev.psych.093008.100356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diez-Roux AV, Mair C. Neighborhoods and health. Annals of the New York Academy of Sciences. 2010;1186:125–145. doi: 10.1111/j.1749-6632.2009.05333.x. [DOI] [PubMed] [Google Scholar]
- Diggle PJ, Ribeiro PJ., Jr Bayesian inference in Gaussian model-based geostatistics. Geographical and Environmental Modelling. 2002;6(2):129–146. [Google Scholar]
- Dobson J. Reinventing GIS and Geography. University Consortium for Geographic Information Science UCGIS; 2016. WWW: http://www.ucgis.org/index.php?option=com_dailyplanetblog&view=entry&year=2017&month=01&day=15&id=5:reinventing-gis-and-geography-by-jerry-dobson, retrieved July 26, 2017. [Google Scholar]
- Duan N. Models for human exposure to air pollution. Environment International. 1982;8(1–6):305–309. [Google Scholar]
- Elwood S, Goodchild M, Sui D. Prospects for VGI research and the emerging fourth paradigm. In: Elwood Sarah, Goodchild Michael F, Sui Daniel., editors. Crowdsourcing Geographic Knowledge: Volunteered Geographic Information (VGI) and Theory and Practice. London: Springer; 2013. [Google Scholar]
- Epstein DH, Tyburski M, Craig IM, Phillips KA, Jobes ML, Vahabzadh M, Mezghanni M, Lin J-L, Furr-Holden CDM, Preston KL. Real-time tracking of neighborhood surroundings and mood in urban drug misusers: Application of a new method to study behavior in its geographical context. Drug and Alcohol Dependence. 2014;134:22–29. doi: 10.1016/j.drugalcdep.2013.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freisthler B, Lipperman-Kreda S, Bersamin M, Gruenewald PJ. Tracking the when, where, and with whom of alcohol use: Integrating ecological momentary assessment and geospatial data to examine risk for alcohol-related problems. Alcohol Research. 2014;36(1):29–38. [PMC free article] [PubMed] [Google Scholar]
- Galea S, Ahern J, Vlahov D. Contextual determinants of drug use risk behavior: A theoretic framework. Journal of Urban Health: Bulletin of the New York Academy of Medicine. 2003;80(4):iii50–iii58. doi: 10.1093/jurban/jtg082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gao S, Janowicz K, McKenzie G, Li L. Toward platial joins and buffers in place-based GIS. Proceedings of SIGSPATIAL ’13: 21st SIGSPATIAL International Conference on Advances in Geographic Information Systems; Orlando, FL, USA. 2013. pp. 42–49. [Google Scholar]
- Gee GC, Payne-Sturges DC. Environmental health disparities: A framework integrating psychosocial and environmental concepts. Environmental Health Perspectives. 2004;112(17):1645–1653. doi: 10.1289/ehp.7074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gesler WM. Therapeutic lanscapes: Medical issues in light of the new cultural geography. Social Science and Medicine. 1992;34(7):735–746. doi: 10.1016/0277-9536(92)90360-3. [DOI] [PubMed] [Google Scholar]
- Gessler D. Keynote Presentation. University Consortium for Geographic Science Annual Symposium; Scottsdale, AZ. May 25.2016. [Google Scholar]
- Glasgow ML, Rudra CB, Yoo EH, Demirbas M, Merriman J, Nayak P, Mu L. Using smartphones to collect time–activity data for long-term personal-level air pollution exposure assessment. Journal of Exposure Science and Environmental Epidemiology. 2016;26(4):356–364. doi: 10.1038/jes.2014.78. [DOI] [PubMed] [Google Scholar]
- Goodchild MF. Models of scale and scales of modeling. In: Tate NJ, Atkinson PM, editors. Modelling Scale in Geographical Information Science. John Wiley & Sons; Chichester, UK: 2001. pp. 3–10. [Google Scholar]
- Goodchild MF. Geographic information science: the grand challenges. In: Wilson JP, Fotheringham AS, editors. Handbook of Geographic Information Science. Malden, MA: Blackwell; 2008. pp. 596–608. [Google Scholar]
- Goodchild MF. Space, place and health. Annals of GIS. 2015;21:97–100. [Google Scholar]
- Gore A. The Digital Earth: Understanding our Planet in the 21st Century. Presented at the California Science Center, Los Angeles, California, January. 1998;31:1998. [Google Scholar]
- Jacquez GM, Sabel CE, Shi C. Genetic GIScience: Toward a place-based synthesis of the genome, exposome, and behavome. Annals of the Association of American Geographers. 2015;105(3):454–472. doi: 10.1080/00045608.2015.1018777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jarup L. Health and environment information systems for exposure and disease mapping, and risk assessment. Environmental Health Perspectives. 2004;112(9):995. doi: 10.1289/ehp.6736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jerrett M, Burnett RT, Ma R, Pope CA, III, Krewski D, Newbold KB, Thurston G, Shi Y, Finkelstein N, Calle EE, Thun MJ. Spatial analysis of air pollution and mortality in Los Angeles. Epidemiology. 2005;16(6):727–736. doi: 10.1097/01.ede.0000181630.15826.7d. [DOI] [PubMed] [Google Scholar]
- Kearns R. Place and health: towards a reformed medical geography. The Professional Geographer. 1993;45:139–47. [Google Scholar]
- Kearns R, Moon G. From medical to health geography: novelty, place and theory after a decade of change. Progress in Human Geography. 2002;26:605–625. [Google Scholar]
- Kirchner TR, Cantrell J, Anesetti-Rothermel A, Ganz O, Vallone DM, Abrams DB. Geospatial exposure to point-of-sale tobacco. American Journal of Preventive Medicine. 2013;45(4):379–385. doi: 10.1016/j.amepre.2013.05.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kerr J, Duncan S, Schipperjin J. Using global positioning systems in health research: a practical approach to data collection and processing. American Journal of Preventive Medicine. 2011;41(5):532–540. doi: 10.1016/j.amepre.2011.07.017. [DOI] [PubMed] [Google Scholar]
- Krenn PJ, Titze S, Oja P, Jones A, Ogilvie D. Use of global positioning systems to study physical activity and the environment: a systematic review. American Journal of Preventive Medicine. 2011;41(5):508–515. doi: 10.1016/j.amepre.2011.06.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwan MP. From place-based to people-based exposure measures. Social Science and Medicine. 2009;69:1311–1313. doi: 10.1016/j.socscimed.2009.07.013. [DOI] [PubMed] [Google Scholar]
- Kwan MP. The uncertain geographic context problem. Annals of the Association of American Geographers. 2012;102(5):958–968. [Google Scholar]
- Kwan MP, Ding G. Geo-narrative: extending geographic information systems for narrative analysis in qualitative and mixed-method research. The Professional Geographer. 2008;60(4):443–465. [Google Scholar]
- Lawson AB. Statistical Methods in Spatial Epidemiology. John Wiley & Sons; 2006. [Google Scholar]
- Lawson AB, Banerjee S, Haining RP, Ugarte MD, editors. Handbook of Spatial Epidemiology. CRC Press; 2016. [Google Scholar]
- Li R, Dziak JJ, Tan X, Huang L, Wagner AT, Yang J. TVEM (time-varying effect model) SAS macro users’ guide (Version 3.1.1) University Park: The Methodology Center, Penn State; 2017. Retrieved from http://methodology.psu.edu (last accessed December 28, 2017) [Google Scholar]
- MacEachren AM. How Maps Work: Representation, Visualization, and Design. New York: Guilford Press; 1995. [Google Scholar]
- Mackaness WA, Chaudhry O. Assessing the veracity of methods for extracting place semantics from Flickr tags. Transactions in GIS. 2013;17(4):544–562. [Google Scholar]
- Macintyre S, Ellaway A, Cummins S. Place effects on health: how can we conceptualise, operationalise and measure them? Social Science & Medicine. 2002;55:125–139. doi: 10.1016/s0277-9536(01)00214-3. [DOI] [PubMed] [Google Scholar]
- Mason MJ, Mennis J, Zaharakis N, Way T. The dynamic role of urban neighborhood effects in a text-messaging adolescent smoking intervention. Nicotine and Tobacco Research. 2016;18(5):1039–1045. doi: 10.1093/ntr/ntv254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mennis J, Mason MJ. People, places, and adolescent substance use: Integrating activity space and social network data for analyzing health behavior. Annals of the Association of American Geographers. 2011;101:272–291. [Google Scholar]
- Mennis J, Mason MJ, Cao Y. Qualitative GIS and the visualization of narrative activity space data. International Journal of Geographical Information Science. 2013;27(2):267–291. doi: 10.1080/13658816.2012.678362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mennis J, Mason M, Light J, Rusby J, Westling E, Way T, Zahakaris N, Flay B. Does substance use moderate the association of neighborhood disadvantage with perceived stress and safety in the activity spaces of urban youth? Drug and Alcohol Dependence. 2016;165:288–292. doi: 10.1016/j.drugalcdep.2016.06.019. [DOI] [PubMed] [Google Scholar]
- Miller H. Place-based versus people-based geographic information science. Geography Compass. 2007;1(3):503–535. [Google Scholar]
- Miller KA, Siscovick DS, Sheppard L, Shepherd K, Sullivan JH, Anderson GL, Kaufman JD. Long-term exposure to air pollution and incidence of cardiovascular events in women. New England Journal of Medicine. 2007;356:447–458. doi: 10.1056/NEJMoa054409. [DOI] [PubMed] [Google Scholar]
- Navidi W, Lurmann F. Measurement error in air pollution exposure assessment. Journal of Exposure Analysis and Environmental Epidemiology. 1995;5(2):111–124. [PubMed] [Google Scholar]
- Northridge ME, Sclar ED, Biswas P. Sorting out the connections between the built environment and health: A conceptual framework for navigating pathways and planning healthy cities. Journal of Urban Health: Bulletin of the New York Academy of Medicine. 2003;80(4):556–568. doi: 10.1093/jurban/jtg064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyhan M, Grauwin S, Britter R, Misstear B, McNabola A, Laden F, Ratti C. Exposure Track” The Impact of Mobile-Device-Based Mobility Patterns on Quantifying Population Exposure to Air Pollution. Environmental science & technology. 2016;50(17):9671–9681. doi: 10.1021/acs.est.6b02385. [DOI] [PubMed] [Google Scholar]
- Park YM, Kwan MP. Individual exposure estimates may be erroneous when spatiotemporal variability of air pollution and human mobility are ignored. Health & Place. 2017;43:85–94. doi: 10.1016/j.healthplace.2016.10.002. [DOI] [PubMed] [Google Scholar]
- Peuquet DJ. Representations of Space and Time. New York: Guilford Press; 2002. [Google Scholar]
- Pickles J, editor. Ground Truth: The Social Implications of Geographic Information Systems. New York: Guilford; 1995. [Google Scholar]
- Rabinovitch N, Adams CD, Strand M, Koehler K, Volckens J. Within-microenvironment exposure to particulate matter and health effects in children with asthma: a pilot study utilizing real-time personal monitoring with GPS interface. Environmental Health. 2016;15(1):96. doi: 10.1186/s12940-016-0181-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richardson DB, Volkov ND, Kwan MP, Kaplan RM, Goodchild MF, Croyle RT. Spatial turn in health research. Science. 2013;339(6126):1390–1392. doi: 10.1126/science.1232257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenberg M. Health geography II: ‘Dividing’ health geography. Progress in Human Geography. 2016;40:546–554. [Google Scholar]
- Rue H, Martino S, Chopin N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. Journal of the royal statistical society: Series b (statistical methodology) 2009;71(2):319–392. [Google Scholar]
- Saelens BE, Sallis JF, Black JB, Chen D. Neighborhood-based differences in physical activity: an environment scale evaluation. American Journal of Public Health. 2003;93(9):1552–1558. doi: 10.2105/ajph.93.9.1552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scheider S, Janowicz K. Place reference systems: A constructive activity model of reference to places. Journal of Applied Ontology. 2014;9:97–127. [Google Scholar]
- Setton E, Marshall JD, Brauer M, Lundquist KR, Hystad P, Keller P, Cloutier-Fisher D. The impact of daily mobility on exposure to traffic-related air pollution and health effect estimates. Journal of Exposure Science and Environmental Epidemiology. 2011;21(1):42. doi: 10.1038/jes.2010.14. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annual Review of Clinical Psychology. 2008;4:1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415. [DOI] [PubMed] [Google Scholar]
- Shoval N, Kwan MP, Reinau KH, Harder H. The shoemaker’s son always goes barefoot: Implementations of GPS and other tracking technologies for geographic research. Geoforum. 2014;51:1–5. [Google Scholar]
- Spiegelman D. Approaches to uncertainty in exposure assessment in environmental epidemiology. Annual Review of Public Health. 2010;31:149–163. doi: 10.1146/annurev.publhealth.012809.103720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sui D. Emerging GIS themes and the six senses of the new mind: Is GIS becoming a liberation technology? Annals of GIS. 2015;21:1–13. [Google Scholar]
- Stahler GJ, Mennis J, Baron D. Geospatial technology and the exposome: New perspectives on addiction. American Journal of Public Health. 2013;103(8):1354–1356. doi: 10.2105/AJPH.2013.301306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stahler G, Mennis J, Cotlar R, Baron D. The influence of the neighborhood environment on treatment continuity and rehospitalization for dually diagnosed patients discharged from acute inpatient care. The American Journal of Psychiatry. 2009;166(11):1258–1268. doi: 10.1176/appi.ajp.2009.08111667. [DOI] [PubMed] [Google Scholar]
- Spielman SE, Yoo EH. The spatial dimensions of neighborhood effects. Social science & medicine. 2009;68(6):1098–1105. doi: 10.1016/j.socscimed.2008.12.048. [DOI] [PubMed] [Google Scholar]
- Steinle S, Reis S, Sabel CE. Quantifying human exposure to air pollution—moving from static monitoring to spatio-temporally resolved personal exposure assessment. Science of the Total Environment. 2013;443:184–193. doi: 10.1016/j.scitotenv.2012.10.098. [DOI] [PubMed] [Google Scholar]
- Tuan YF. Space and Place: The Perspective of Experience. University of Minnesota Press; Minneapolis, MN: 1977. [Google Scholar]
- Vasardani M, Winter S, Richter KF. Locating place names from place descriptions. International Journal of Geographical Information Science. 2013;27:2509–2532. [Google Scholar]
- Vazquez-Prokopec GM, Bisanzio D, Stoddard ST, Paz-Soldan V, Morrison AC, Elder JP, Ramirez-Paredes J, Halsey ES, Kochel TJ, Scott TW, Kitron U. Using GPS technology to quantify human mobility, dynamic contacts and infectious disease dynamics in a resource-poor urban environment. PloSONE. 2013;8(4):e58802. doi: 10.1371/journal.pone.0058802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wesolowski A, Eagle N, Tatem AJ, Smith DL, Noor AM, Snow RW, Buckee CO. Quantifying the impact of human mobility on malaria. Science. 2012;338(6104):267–270. doi: 10.1126/science.1223467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiese D, Escobar JR, Hsu Y, Kulathinal RJ, Hayes-Conroy A. The fluidity of biosocial identity and the effects of place, space, and time. Social Science and Medicine. 2018;198:46–52. doi: 10.1016/j.socscimed.2017.12.023. [DOI] [PubMed] [Google Scholar]
- Wild CP. Complementing the genome with an ‘exposome’: The outstanding challenge of environmental exposure measurement in molecular epidemiology. Cancer Epidemioloyg Biomarkers and Prevention. 2006;14(8):1847–1850. doi: 10.1158/1055-9965.EPI-05-0456. [DOI] [PubMed] [Google Scholar]
- Wilson JG, Kingham S, Pearce J, Sturman AP. A review of intraurban variations in particulate air pollution: Implications for epidemiological research. Atmospheric Environment. 2005;39(34):6444–6462. [Google Scholar]
- Winter S, Freksa C. Approaching the notion of place by contrast. Journal of Spatial Information Science. 2012;5:31–50. [Google Scholar]
- Wu J, Jiang C, Houston D, Baker D, Delfino R. Automated time activity classification based on global positioning system (GPS) tracking data. Environmental Health. 2011;10(1):101. doi: 10.1186/1476-069X-10-101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yoo E, Rudra C, Glasgow M, Mu L. Geospatial estimation of individual exposure to air pollutants: moving from static monitoring to activity-based dynamic exposure assessment. Annals of the Association of American Geographers. 2015;105(5):915–926. [Google Scholar]
- Yoo E, Eum YS. Using GPS-enabled mobile phones to characterize individuals’ activity patterns for epidemiology applications. International Conference on GIScience Short Paper Proceedings. 2016;1(1) [Google Scholar]
- Zheng Y, Xie X, Ma WY. Geolife: A collaborative social networking service among user, location and trajectory. IEEE Data Engineering Bulletin. 2010;33(2):32–39. [Google Scholar]
- Zhong S, Bian L. A location-centric network approach to analyzing epidemic dynamics. Annals of the Association of American Geographers. 2016;106(2):480–488. doi: 10.1080/00045608.2015.1113113. [DOI] [PMC free article] [PubMed] [Google Scholar]