

Abstract
Direct perfluorocarbon liquid (PFCL)-silicone oil exchange presents its own set of challenges in the micro incision vitreous surgery era. We propose a simple bimanual technique to circumvent this problem. Thirteen eyes of patients with retinal detachment associated with giant retinal tears underwent vitrectomy followed by self-retaining endo illuminator (Chandelier) assisted direct PFCL-silicone exchange. No intra or postoperative complications related to the surgical technique were noted. All patients had attached retinas and satisfactory visual recovery at 6 months. Direct bimanual PFCL silicone oil exchange using a Chandelier seems to be a safe and effective technique.
Keywords: Chandelier, giant tear retina, perfluorocarbon liquid, silicone oil
Giant retinal tears (GRTs) are defined as full-thickness circumferential tears of more than 90° of the retina associated with vitreous detachment.[1,2,3] Their management poses significant challenges owing to the many complications and technical difficulties. Best success rates of re-attachment and least chances of slippage of the GRT edge have been reported using silicone oil as tamponade.[4] Perfluorocarbon liquids (PFCLs) revolutionized the management of GRTs, and the advent of small gauge vitrectomy techniques have further optimized the treatment outcomes. Microincision vitreous surgery (MIVS) has been reported as a successful modality to treat these cases.[5] PFCL-silicone oil exchange using MIVS is challenging.
We included 13 patients with RD associated with GTR in our study. The extent of GTR ranged from 90° to 180°. In total, 23% (3 of 13) patients had 3 clock hours of GTR (90°) and 76.92% (10 of 13) had 6 clock hours of GTR (180°). Totally, 15% (2 of 13) patients had superior GTRs (10 o′clock to 1 o′clock) and 84.6% (11 of 13) patients had temporal GTRs (6 o′clock to 12 o′clock) [Fig. 1]. None of the patients had inferior configuration of GTRs.
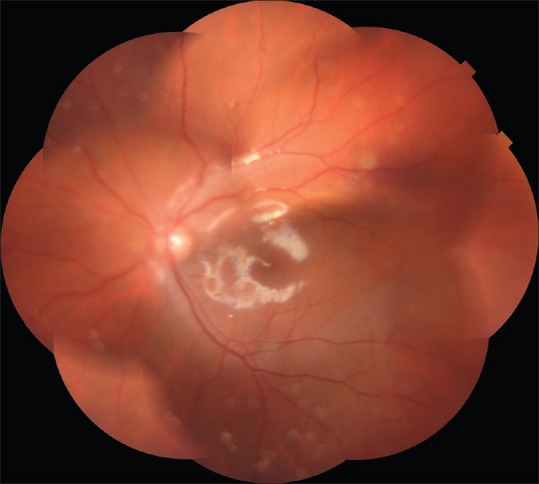
Figure 1.
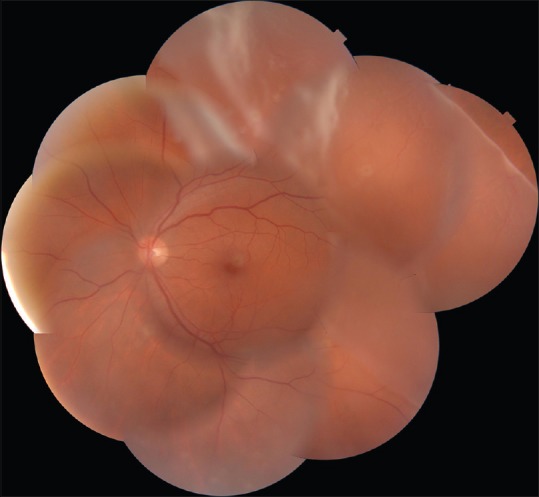
Representative preoperative fundus photograph showing a temporal GTR superotemporally. The GTR extended from 2 ′o clock to 5 ′o clock, however, the complete edge of the temporal GTR could not captured owing to peripheral location of the tear)
Technique
We used a bimanual technique for direct PFCL-silicone oil exchange in 13 eyes of patients with retinal detachment with GTR. All the eyes underwent 25-gauge pars plana vitrectomy. After removal of the vitreous, PVR membranes, if present, were removed with an end-grasping forceps ensuring a traction free GRT edge. Base excision was done with depression. PFCL [perfluoro-n-octane (PFO)] (Auro octane; Aurolabs, Madurai, India) was used in all cases to flatten the retina [Fig. 2].
Figure 2.
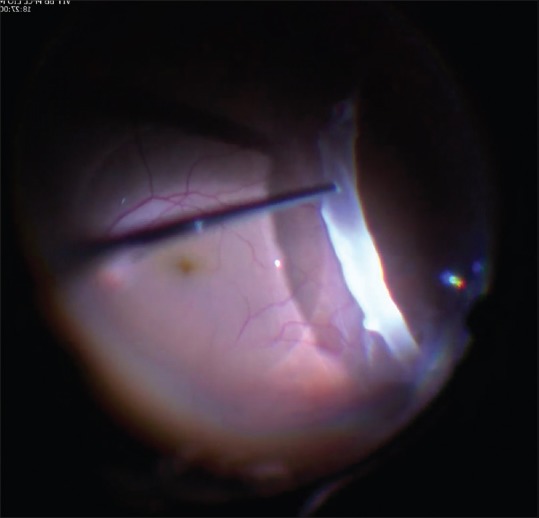
Intraoperative photograph showing perfluorocarbon liquid bubble in situ. The temporal edge of the GTR is seen clearly in the photograph
After reattachment, four rows of confluent laser spots using a 25-gauge endophotocoagulation probe were applied around all GRTs as well as 360° [Fig. 3]. A Chandelier (Alcon Fort Worth, TX) was inserted, the infusion cannula was clamped and direct PFCL-silicone oil exchange was done with flute needle in dominant hand and silicon oil injection in non-dominant hand. 1300-centistoke silicone oil (Aurosil; Aurolabs) was used for tamponade [Fig. 4 and Video 1].
Figure 3.
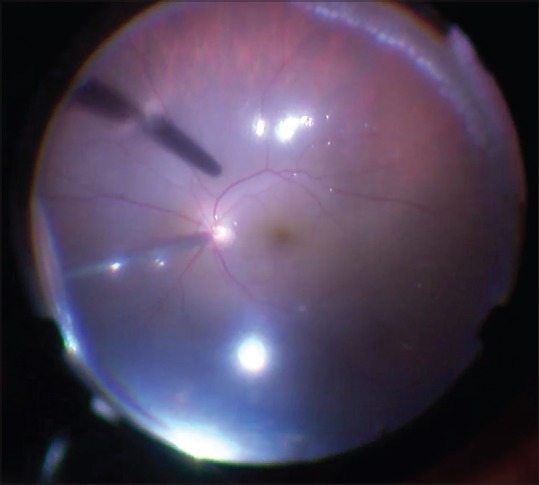
Intraoperative picture showing settled retina with laser marks at edge of GTR
Figure 4.
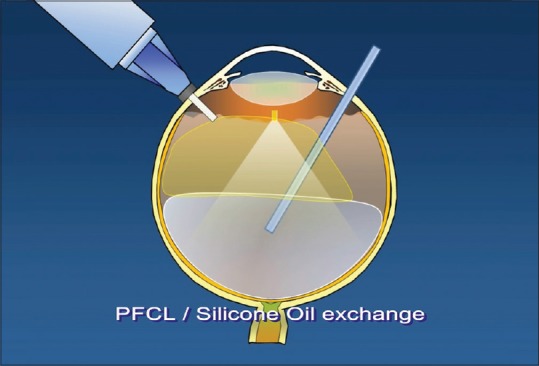
Representative picture showing chandelier assisted direct perfluorocarbon liquid-silicone oil exchange. Superiorly illumination provided by the chandelier is seen. The flute needle is kept in the dominant hand, and the tip is seen to be within the perfluorocarbon liquid bubble. The silicone oil is being injected into the eye through the other port and is seen entering the vitreous cavity above the perfluorocarbon liquid bubble
Postoperatively, the retina was attached in all eyes [Fig. 5]. Preoperative Best Corrected Visual Acuity (BCVA) was 1.75+/–0.99. At 2 months, BCVA improved to 0.79+/–0.63 (P = 0.007). At 6 months, BCVA improved to 0.48+/–0.38 (P = 0.001). Two or more line improvement was seen in 76.9% patients at 6 months, 15.4% patients had stable vision and 7.7% showed two line worsening.
Figure 5.
Postoperative picture showing well attached retina with silicon oil in situ (the GTR edge cannot be seen owing to peripheral location of the lasered tear)
Discussion
With 20-gauge vitrectomy systems, silicone oil syringe was previously directly connected to the sutured infusion.[6]
In MIVS cases, where silicone oil is directly connected to the infusion,[7] the infusion line could slip out of the cannula owing to back-pressure exerted on the small gauge system. Current technique involves an assistant holding the syringe at site of infusion cannula after disconnecting the infusion line. However, the syringe could still slip out of the infusion, even with the assistant.
Direct exchange is surgeon-controlled without undue distortion of the globe (if syringe is held too tightly by an assistant), is quicker and leads to complete vitreous fill. In addition, no slippage of retinal tear or intra-ocular pressure (IOP) related issues were noted perioperatively. None of the cases required fluid air exchange (Indirect Exchange).
Disadvantages of this technique would include the additional cost incurred, along with complications related to making the fourth port. Inserting and moving an endoilluminator into the vitreous cavity could increase the risk of retinal tears related to sclerotomy site, lenticular damage, or posterior capsular tears.[8] Removal or movement of the Chandelier can rarely lead to hyphema due to bleed from sclerotomy site or hitting the root of iris. However, no complication was observed in our study.
Conclusion
We conclude that direct PFCL-silicone oil exchange for RD with GTR seems to be a safe and effective technique with minimal intraoperative and postoperative complications.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video Available on: www.ijo.in
References
- 1.Schepens CL, Dobble JG, Mcmeel JW. Retinal detachments with giant breaks: Preliminary report. Trans Am Acad Ophthalmol Otolaryngol. 1962;66:471–9. [PubMed] [Google Scholar]
- 2.Ang GS, Townend J, Lois N. Epidemiology of giant retinal tears in the United Kingdom: The British giant retinal tear epidemiology eye study (BGEES) Invest Ophthalmol Vis Sci. 2010;51:4781–7. doi: 10.1167/iovs.09-5036. [DOI] [PubMed] [Google Scholar]
- 3.Ghosh YK, Banerjee S, Savant V, Kotamarthi V, Benson MT, Scott RA, et al. Surgical treatment and outcome of patients with giant retinal tears. Eye (Lond) 2004;18:996–1000. doi: 10.1038/sj.eye.6701390. [DOI] [PubMed] [Google Scholar]
- 4.Dabour SA. The outcome of surgical management for giant retinal tear more than 180°. BMC Ophthalmol. 2014;14:86. doi: 10.1186/1471-2415-14-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kumar V, Kumawat D, Bhari A, Chandra P. Twenty-five-gauge pars plana vitrectomy in complex retinal detachments associated with giant retinal tear. Retina. 2018;38:670–7. doi: 10.1097/IAE.0000000000001592. [DOI] [PubMed] [Google Scholar]
- 6.Han DP, Rychwalski PJ, Mieler WF, Abrams GW. Management of complex retinal detachment with combined relaxing retinotomy and intravitreal perfluoro-n-octane injection. Am J Ophthalmol. 1994;118:24–32. doi: 10.1016/s0002-9394(14)72838-7. [DOI] [PubMed] [Google Scholar]
- 7.Barca F, Caporossi T, Rizzo S. Silicone oil: Different physical proprieties and clinical applications. Biomed Res Int 2014. 2014:502143. doi: 10.1155/2014/502143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kim KH, Sohn HJ, Song HJ, Lee DY, Nam DH. Surgeon-controlled-endoillumination-guided irrigation and aspiration during combined 23-gauge sutureless vitrectomy and cataract surgery in eyes with poor fundus reflex. J Cataract Refract Surg. 2010;36:2028–31. doi: 10.1016/j.jcrs.2010.10.004. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.