

Abstract
Objectives
The aim of this study is to examine the effectiveness of diverse exercise regimes used in multiple Randomized Control Trials as the only conservative management strategy for increased Cobb angle among Adolescent Idiopathic Scoliosis.
Methods
Database such as Google Scholar, Medline, and BioMed Central was reconnoitered for the purpose of research articles of interest. Studies in which the effects of conservative management of scoliosis on the magnitude of Cobb angle were calculated were scrutinized procedurally, studies fulfilling the inclusion criteria were retrieved and encompassed in the present study.
Result
A total of 698 cases of AIS that were included in 17 controlled trials are part of this meta-analysis. The pool effects were measured using a standardized mean difference between the experimental and control group at 95% of confidence interval using Hedges’g statistics. Outcomes analyzed, reveals favorable for exercises based experimental group in term of standardized mean difference with an impact of 0.42° on random effect model, according to a Cohen’s rule of thumb that depicts a near to moderate effects of exercises based interventions on Cobb angle.
Conclusion
The present study concludes that therapeutic exercise regimes alone have a pivotal role in both decelerating the progression of the curve and reducing the already increased magnitude of the curve.
Keywords: Scoliosis, exercise therapy, cobb angle
Introduction
The conservative, evidence-based medicine in the management of scoliosis has received tremendous input under the term “physiotherapy scoliosis specific exercises” (PSSE) coined by “the society of scoliosis orthopedic rehabilitation and treatment” (SOSORT).[1] During the past decade a call for a change in the management protocol of scoliosis from the different stakeholders including the parents of the children who are not a good candidate for surgery has challenged the previously existed protocol of “wait and see” that far too many doctors use while evaluating candidates having spinal curve in between 10 and 25°.[2] Since then a number of approaches have been developed under PSSE that claims the effectiveness of newly developed exercise regimes in the management of Cobb’s angle, functional capacity and pain among patients with idiopathic scoliosis[3] midst them the most prominent and widely used protocol are the Schroth approach developed by Katharina Schroth in 1920[2,4] besides that there are six other schools that also claims the effectiveness of conservative exercise regimes for the management of the scoliosis curves.
Idiopathic scoliosis is characterized by the lateral deviation of the spine measuring to be >10° using Cobb’s angle in an otherwise healthy individual for which no known etiology has been recognized.[5-8] The deformity progresses with age, and approximately 90% of all the cases are being diagnosed during the age of adolescence (10–19 years).[9] According to Labelle et al. the prevalence of idiopathic scoliosis among adolescence is 2–4% in 2013,[10] while having a 50% higher rate of incidence is found among females than males.[11] Scoliosis causes deformity that not only has cosmetic effects but it can also have compressive effects on internal organs that effect on the patient capacity to work, and in severe cases, it may even lead to cardiorespiratory compromise in the form of cor pulmonale.[12]
While surgical management is specific for the patients having a Cobb’s angle >40°[13] conservative management would be a treatment of choice for patients having Cobb’s angle <25° with a primary aim to curb the progression of the curve and to reduce the magnitude of the lateral deviation of spine (SOSORT guideline committee),[14-17] number of studies conducted globally on effectiveness of conservative management have indicated variance in results based on reduction in Cobb angle and even few studies have exhibited increase in Cobb angle after following recommended treatment protocol. However, it has been noticed by the researcher that sample size is a primary constraint factor of all these studies. Hence, a meta-analysis has been performed to elucidate the inconsistencies found in the previous researches as it provides a strong statistical mechanism for examining the pool effects of independent researches where discrete population sizes are inadequate to provide a strong statistical significance.
Materials and Methods
Identification and eligibility of relevant studies
Database such as Google Scholar, Medline, and BioMed Central was explored for the purpose of research article of interest using the following keywords: Adolescent idiopathic scoliosis and Cobb angle, Adolescent idiopathic scoliosis and SOSORT guidelines, and Cobb angle and Exercise therapy. All those studies in which the effect of conservative management of scoliosis on the magnitude of Cobb angle was calculated were scrutinized procedurally and those studies are fulfilling the inclusion criteria were retrieved and encompassed in the present study.
Inclusion and exclusion criteria
Inclusion criteria embrace all those studies that included only exercise therapy for the conservative management of Adolescent Idiopathic Scoliosis based on different regimes and protocols. All those researches in which surgical interventions were implemented for the correction of the spinal curve or who have taken into account non-idiopathic scoliosis or were conducted before 2005 were excluded from this review.
Data extraction and quality assessment
Data extraction and quality assessment were done on the basis of inclusion and exclusion criteria as per already developed standardized protocols. An assessment form was designed to validate data accuracy by including information from the studies as the first name of the author, year of publication, sample size, and the type of exercise therapy implemented as shown in Table 1.
Table 1.
Represents the detail list of all the studies with author name, year of publication, sample size, and interventional strategies

Data analysis
Analysis was done using MedCalc statistical software. A continuous measure tool (comparing a mean difference between an experimental group and control group) was obtained on a forest plot, and its pooled effects were determined at 95% of confidence interval (CI) using a Hedges’g statistics for the formulation of a standardized mean. For the purpose of interpreting the values obtained on fixed/random model, Cohen’s rule of thumb was applied that states a value of 0.2 reflects small effects, of 0.5 indicates a medium and value >0.8 indicates a large effect. For determining the level of heterogeneity supposition, Cochrane Q was determined. The I2 statistic was applied to quantify inter-study variability having a range of 0–100%, 0% indicating no heterogeneity whereas the increased values indicate a higher level of heterogeneity.
Results
Characteristics of the included studies
A total of 17 randomized control trials were included comprising 698 cases of AIS as a part of this meta-analysis from Google Scholar, Medline, and BioMed Central database. The studies were strictly scrutinized, and only those RCTs were included in which the Cobb angle was measured as a primary outcome in response to exercises. Reference list of all the selected articles was also studied to extract out other relevant articles, through this exercise five more articles were recruited. PRISMA guidelines for the selection of study were followed which was given in Figure 1.
Figure 1.
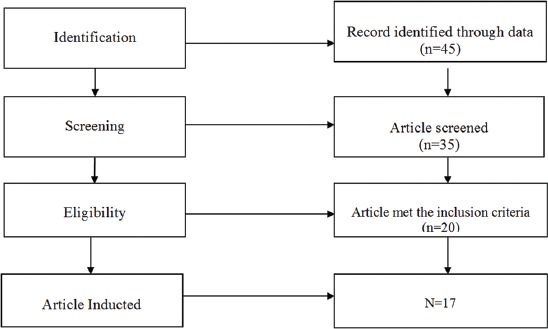
Flow diagram according to PRISMA guidelines
Test for heterogeneity
The Q test and I2 test were calculated to identify the level of heterogeneity, as the values of level of inconsistency were within 95% of CI random effect model was used for assessing the pool effects.
Synthesized findings
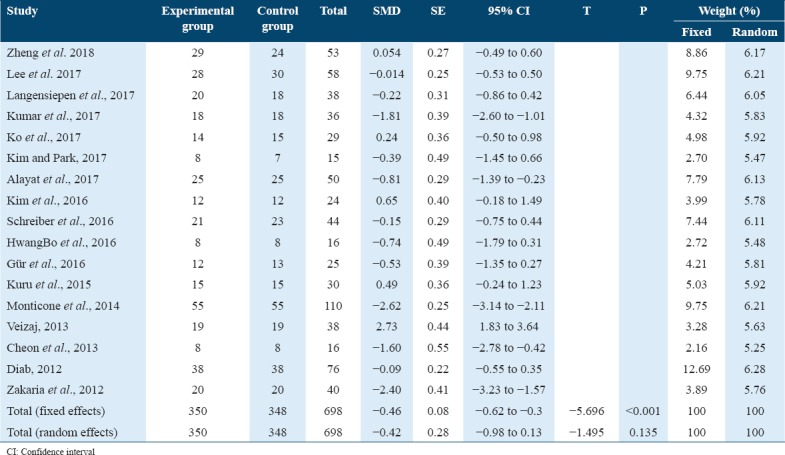
Overall synthesized finding of 17 studies included were found to be in favor of the experimental group. The pool effects of Cobb angle in term of standardized mean difference as obtained in a random effects models showed an impact of 0.42° in favor of exercises based intervention that according to a Cohen rule of thumb depicts a near to moderate effects of exercises based interventions on Cobb angle as shown in Table 2.
Table 2.
Pooled effects of exercise intervention on Cobb angle in term of SMD
Effect of exercise on Cobb angle is also plotted on the forest plot to determine the pooled effects in random and fixed effect model at 95% of CI as shown in Figure 2.
Figure 2.
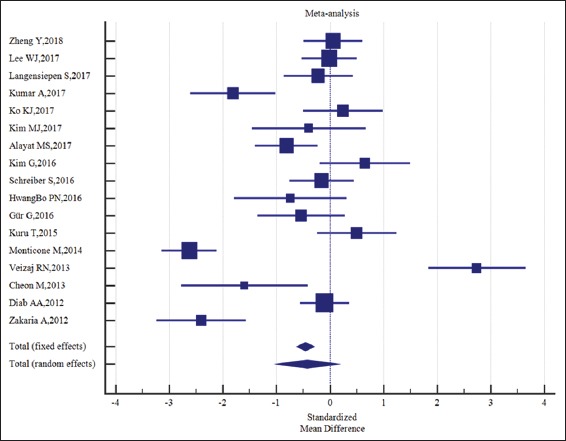
Illustrates the findings of the results of each study and its impact on the pool effects at the given level of confidence interval
Risk of bias
Risk of bias of studies included in this review was assessed on the basis of Cochrane Collaboration tools for assessing the risk of bias as shown in Table 3.
Table 3.
Author judgment regarding risk of bias assessment

Allocation
Random sequence generation
The randomization sequence was generated by the 16 studies[18-34] which illustrates the unknown risk of bias.
Allocation concealment
The concealed allocation in the randomized controlled trials was considered by the 15 studies (Zheng et al.[18] 2018, Lee et al.[19] 2017, Langensiepen et al.[20] 2017, Kumar et al.[21] 2017, Ko et al.[22] 2017, Kim and Park[23] 2017, Alayat et al.[24] 2017, Kim et al.[25] 2016, Schreiber et al.[26] 2016, HwangBo et al.[27] 2016, Gür et al.[28] 2016, Monticone et al.[30] 2014, Veizaj[31] 2013, Diab et al.[33] 2012, and Zakaria et al.[34] 2012). On the contrary, two studies (Kuru et al.[29] 2016 and Cheon et al.[32] 2013) illustrated the unknown allocation approach.
Blinding
Blinding of participants and personnel
Nine out of 17 studies (Zheng et al.[18] 2018, Lee et al.[19] 2017, Langensiepen et al.[20] 2017, Kumar et al.[21] 2017, Alayat et al.[24] 2017, Schreiber et al.[26] 2016, Gür et al.[28] 2016, Kuru et al.[29] 2016, and Monticone et al.[30] 2014) considered the participants and personnel blinding whereas two of the studies (Kim and Park[23] 2017, and Veizaj[31] 2013) showed unknown blinding approach. Six studies (Ko et al.[22] 2017, Kim et al.[25] 2016, HwangBo et al.[27] 2016, Cheon et al.[32] 2013, Diab[33] 2012, and Zakaria et al.[34] 2012) had shown the high risk of bias.
Blinding of outcome assessment
All the 17 studies had considered the blinding of the outcome assessment.
Incomplete outcome data
In the configuration of the risk of bias, all the studies have shown the absolute assessments and analysis of the outcome measures.
Selective reporting
The selective reporting of the outcome measures was also illustrated in all the studies. The author’s judgment of risk of assessment was illustrated in Figure 3.
Figure 3.
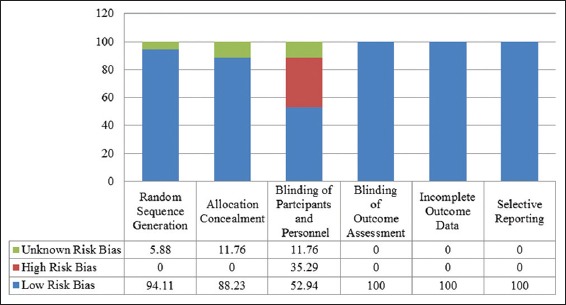
Risk of bias assessment in percentage
Discussion
Multiple AIS management approaches based on different exercises regimes are advocated to be effective in reducing the lateral curve of the spine, over the past decade number of researches have been conducted to quantify the impact of exercises on the Cobb angle providing confronting results. Moreover, with the development of the conservative management guidelines for scoliosis multiple exercise approaches has been identified by practitioners claiming their effectiveness in reducing the progression and decelerating the magnitude of the scoliosis curve, but most of such studies provide low-quality evidence as the protocols applied were on small sample size; further, the researcher has been unable to extract any meta-analysis to filtered the claim of all these randomized controlled trials. This meta-analysis contributes uniquely to increase the statistical strength and to acquire a more comprehensive and reliable interpretation of the findings. The guidelines given until date for the conservative management of AIS are highly dependent on the age of onset and the magnitude of the spinal curve[1] but not so focused on the pooled effects of the specific exercises regimes and their protocols. Hence, most of the studies conducted have utilized different regimes of exercises with varied protocols thus this meta-analysis addresses the need to determine the collective impact of exercises as a management strategy for the lateral spinal curve.
Different studies have provided evidence that conservative management with or without bracing significantly reduces the Cobb’s angle along with the improvement in the functional capacity of the patient.[21,26,29-30] However, Alexi reported the use of bracing alone reduces the Cobb angle by 5°, whereas according to the same study specific exercises strategies were essential only to increase the postural correctness and muscle strength among the patients.[35] On the other hand, a retrospective study conducted in 2009 on the effectiveness of complete conservative treatment for adolescent idiopathic scoliosis based on the guidelines of SOSORT reported a significant reduction in the scoliosis curvature by overall 7.1°, thoracic 7.3°, thoracolumbar 8.4°, and lumbar 7.8°. Moreover, a statistically significant result had also been reported in esthetics index and angle of trunk rotation.[36]
The result of this meta-analysis revealed that exercises based conservative management on the guidelines of SOSORT is effective in the management of Cobb angle with a near to moderate effect size as measured using random effect model.
While deducing the result researcher, acknowledges some limitations as non-availability of satisfactory number of studies as most of the studies available on topic were based on the outcome measures other than Cobb angle which makes the availability of literature on this parameter difficult and in certain cases despite efforts the availability of full-text articles of some literatures were not possible to extract.
The study has combined the impact of exercises regimes on Cobb angle as noted in different RCTs into a single analysis and with a watchful selection of data based on the stringent policy the researcher believes that current meta-analysis would be a knowledgeable tool for the clinicians and would open a door for future researches.
Conclusion
The present study indicates that therapeutic exercises regimes had a pivotal role not only in decelerating the progression of the curve but also indeed effective in reducing the magnitude of the curve.
References
- 1.Negrini S, Aulisa AG, Aulisa L, Circo AB, de Mauroy JC, Durmala J, et al. 2011 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. BMC Scoliosis Spinal Disord. 2012;7:3. doi: 10.1186/1748-7161-7-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Berdishevsky H, Lebel VA, Bettany-Saltikov J, Rigo M, Lebel A, Hennes A, et al. Physiotherapy scoliosis-specific exercises-a comprehensive review of seven major schools. BMC Scoliosis Spinal Disord. 2016;11:20. doi: 10.1186/s13013-016-0076-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Romano M, Minozzi S, Bettany-Saltikov J, Zaina F, Chockalingam N, Kotwicki T, et al. Exercises for adolescent idiopathic scoliosis. Cochrane Database Syst Rev. 2012;8:CD007837. doi: 10.1002/14651858.CD007837.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kuru T, Yilmaz H. Assessment of stress in adolescent idiopathic scoliosis patients while wearing a brace. BMC Scoliosis Spinal Disord. 2012;7:O4. [Google Scholar]
- 5.Negrini S, Donzelli S, Lusini M, Minnella S, Zaina F. The effectiveness of combined bracing and exercise in adolescent idiopathic scoliosis based on SRS and SOSORT criteria: A prospective study. BMC Musculoskelet Disord. 2014;15:263. doi: 10.1186/1471-2474-15-263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Negrini S, Fusco C, Minozzi S, Atanasio S, Zaina F, Romano M, et al. Exercises reduce the progression rate of adolescent idiopathic scoliosis: Results of a comprehensive systematic review of the literature. Disabil Rehabil. 2008;30:772–85. doi: 10.1080/09638280801889568. [DOI] [PubMed] [Google Scholar]
- 7.Negrini S, Grivas TB, Kotwicki T, Rigo M, Zaina F. Guidelines on standards of management of idiopathic scoliosis with corrective braces in everyday clinics and in clinical research: SOSORT Consensus 2008. BMC Scoliosis Spinal Disord. 2009;4:2. doi: 10.1186/1748-7161-4-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Balagué F, Pellisé F. Adolescent idiopathic scoliosis and back pain. BMC Scoliosis Spinal Disord. 2016;11:27. doi: 10.1186/s13013-016-0086-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Konieczny MR, Senyurt H, Krauspe R. Epidemiology of adolescent idiopathic scoliosis. J Child Orthop. 2013;7:3–9. doi: 10.1007/s11832-012-0457-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Labelle H, Richards SB, De Kleuver M, Grivas TB, Luk KD, Wong HK, et al. Screening for adolescent idiopathic scoliosis: An information statement by the scoliosis research society international task force. BMC Scoliosis Spinal Disord. 2013;8:17. doi: 10.1186/1748-7161-8-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kamtsiuris P, Atzpodien K, Ellert U, Schlack R, Schlaud M. Prevalence of somatic diseases in German children and adolescents. Results of the German health interview and examination survey for children and adolescents (KiGGS) Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2006;50:686–700. doi: 10.1007/s00103-007-0230-x. [DOI] [PubMed] [Google Scholar]
- 12.Wong HK, Tan KJ. The natural history of adolescent idiopathic scoliosis. Indian J Orthop. 2010;44:9–13. doi: 10.4103/0019-5413.58601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fazal A, Lakdawala RH. Fourth-generation spinal instrumentation: Experience with adolescent idiopathic scoliosis at a tertiary care hospital in Pakistan. Int J Gen Med. 2012;5:151–5. doi: 10.2147/IJGM.S29236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Abbott A, Möller H, Gerdhem P. CONTRAIS: Conservative Treatment for adolescent idiopathic scoliosis: A randomised controlled trial protocol. BMC Musculoskelet Disord. 2013;14:261. doi: 10.1186/1471-2474-14-261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Alves VL, Avanzi O. Respiratory muscle strength in idiopathic scoliosis after training program. Acta Ortop Bras. 2016;24:296–9. doi: 10.1590/1413-785220162406120752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Arif M, Inam M, Hassan W. Radiographic outcome of adolescent idiopathic scoliosis surgical correction with posterior spinal fusion using pedicle screw and rods fixation. J Surg Pak. 2011;16:118. [Google Scholar]
- 17.Dolan LA, Wright JG, Weinstein SL. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med. 2014;370:681. doi: 10.1056/NEJMc1314229. [DOI] [PubMed] [Google Scholar]
- 18.Zheng Y, Dang Y, Yang Y, Li H, Zhang L, Lou EH, et al. Whether orthotic management and exercise are equally effective to the patients with adolescent idiopathic scoliosis in Mainland China?A randomized controlled trial study. Spine (Phila Pa 1976) 2018;43:E494–503. doi: 10.1097/BRS.0000000000002412. [DOI] [PubMed] [Google Scholar]
- 19.Lee WJ, Ko YM, Park JW. Effect of trunk side shift exercise on the cobb's angle of patients with idiopathic scoliosis. J Korean Med Sci. 2017;29:276–80. [Google Scholar]
- 20.Langensiepen S, Stark C, Sobottke R, Semler O, Franklin J, Schraeder M, et al. Home-based vibration assisted exercise as a new treatment option for scoliosis-a randomised controlled trial. J Musculoskelet Neuronal Interact. 2017;17:259–67. [PMC free article] [PubMed] [Google Scholar]
- 21.Kumar A, Kumar S, Sharma V, Srivastava RN, Gupta AK, Parihar A, et al. Efficacy of task oriented exercise program based on ergonomics on cobb's angle and pulmonary function improvement in adolescent idiopathic scoliosis-a randomized control trial. J Clin Diagn Res. 2017;11:YC01–4. doi: 10.7860/JCDR/2017/27497.10335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ko KJ, Kang SJ. Effects of 12-week core stabilization exercise on the cobb angle and lumbar muscle strength of adolescents with idiopathic scoliosis. J Exerc Rehabil. 2017;13:244–9. doi: 10.12965/jer.1734952.476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kim MJ, Park DS. The effect of schroth's three-dimensional exercises in combination with respiratory muscle exercise on cobb's angle and pulmonary function in patients with idiopathic scoliosis. J Phys Ther Sci. 2017;6:113–9. [Google Scholar]
- 24.Alayat MS, Abdel-Kafy EM, Abdelaal AM. H-reflex changes in adolescents with idiopathic scoliosis: A randomized clinical trial. J Phys Ther Sci. 2017;29:1658–63. doi: 10.1589/jpts.29.1658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kim G, HwangBo PN. Effects of schroth and Pilates exercises on the cobb angle and weight distribution of patients with scoliosis. J Phys Ther Sci. 2016;28:1012–5. doi: 10.1589/jpts.28.1012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Schreiber S, Parent EC, Khodayari Moez E, Hedden DM, Hill DL, Moreau M, et al. Schroth physiotherapeutic scoliosis-specific exercises added to the standard of care lead to better cobb angle outcomes in adolescents with idiopathic scoliosis-an assessor and statistician blinded randomized controlled trial. PLoS One. 2016;11:e0168746. doi: 10.1371/journal.pone.0168746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.HwangBo PN. Psychological and physical effects of schroth and Pilates exercise on female high school students with idiopathic scoliosis. J Korean Phys. 2016;28:364–8. [Google Scholar]
- 28.Gür G, Ayhan C, Yakut Y. The effectiveness of core stabilization exercise in adolescent idiopathic scoliosis: A randomized controlled trial. Prosthet Orthot Int. 2017;41:303–10. doi: 10.1177/0309364616664151. [DOI] [PubMed] [Google Scholar]
- 29.Kuru T, Yeldan İ, Dereli EE, Özdinçler AR, Dikici F, Çolak İ, et al. The efficacy of three-dimensional schroth exercises in adolescent idiopathic scoliosis: A randomised controlled clinical trial. Clin Rehabil. 2016;30:181–90. doi: 10.1177/0269215515575745. [DOI] [PubMed] [Google Scholar]
- 30.Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S. Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trial. Eur Spine J. 2014;23:1204–14. doi: 10.1007/s00586-014-3241-y. [DOI] [PubMed] [Google Scholar]
- 31.Veizaj RN. Physiotherapy in adolescents with idiopathic scoliosis. Randomized clinical trial (RCT) Int J Sci Res. 2013;5:980–82. [Google Scholar]
- 32.Cheon M, Park J, Lee Y, Lee J. Effect of chiropractic and lumbar exercise program on lumbar muscle strength and Cobb's angle in patients with scoliosis for u-Healthcare. EURASIP J Wirel Commun Netw. 2013;2013:132. [Google Scholar]
- 33.Diab AA. The role of forward head correction in management of adolescent idiopathic scoliotic patients: A randomized controlled trial. Clin Rehabil. 2012;26:1123–32. doi: 10.1177/0269215512447085. [DOI] [PubMed] [Google Scholar]
- 34.Zakaria A, Hafez A, Buragadda S, Melam GR. Stretching versus mechanical traction of the spine in treatment of idiopathic scoliosis. J Phys Ther Sci. 2012;24:1127–31. [Google Scholar]
- 35.Mandal RK, Raish M, Jawed A, Wahid M, Dar SA, Lohani M, et al. Meta-analysis reveals no correlation of caveolin-1 G14713A (G>A) gene polymorphism with increased cancer risk in Taiwanese population. Int J Health Sci (Qassim) 2018;12:3–9. [PMC free article] [PubMed] [Google Scholar]
- 36.Zaina F, Negrini S, Atanasio S. TRACE (Trunk aesthetic clinical evaluation), a routine clinical tool to evaluate aesthetics in scoliosis patients: Development from the aesthetic index (AI) and repeatability. Scoliosis. 2009;4:3. doi: 10.1186/1748-7161-4-3. [DOI] [PMC free article] [PubMed] [Google Scholar]