

Short abstract
Objective
This study was performed to determine whether exposure to personal music players (PMPs) in the immediate morning prior to hearing testing confounds the association between mobile phone use and hearing thresholds of adolescents.
Design
In this cohort study of cognitive function in year 7 students (median age 13 years, range 11–14), information regarding the weekly use of mobile phones and the use of PMPs was assessed by a questionnaire. Pure-tone audiometry was used to establish hearing thresholds for all participants.
Results
Among a cohort of 317 adolescents (60.9% females), 130 were unexposed to PMP use while 33 were exposed to PMP use in the morning prior to hearing testing. No statistically significant difference in hearing threshold shifts was found between adolescents who were and were not exposed to PMP use prior to hearing testing. Likewise, the difference in the use of mobile phones according to the PMP use status was not statistically significant.
Conclusion
Exposure to PMPs prior to hearing testing did not introduce confounding in the present study of mobile phone use and hearing loss among adolescents.
Keywords: Audiometry, adolescents, mobile telephones, personal music players, confounder, threshold shift
Abbreviations
- MoRPhEUS
Mobile Radiofrequency Phone Exposed Users Study
- PMP
personal music player
- PTS
permanent threshold shift
- TTS
temporary threshold shift
Introduction
The use of personal music players (PMPs) such as MP3, iPods, smart phones, and similar devices has dramatically increased worldwide during the last decade. According to the Scientific Committee on Emerging and Newly Identified Health Risks, PMPs are becoming increasingly popular particularly among children and teenagers.1 Adolescents often listen to high-volume (sound pressure) music at home, on public transport, inside motor vehicles, and while jogging, strolling, or relaxing.2,3
The media has recently raised the issue of possible permanent hearing loss, also known as a permanent threshold shift (PTS), secondary to the use of these devices. Much of our knowledge regarding PTS has been derived from occupational studies performed in the 1950s and 1960s, and only recently has more concern arisen regarding the combination of workplace and recreational noise.4 Measuring PTS by pure-tone audiometry requires the absence of any influence from temporary threshold shifts (TTSs) and the use of serial audiometry. Studies have shown that PMP exposure is associated with the development of noise-induced hearing loss and tinnitus in adolescents.5–7 Audiometric tests have demonstrated significantly worse hearing thresholds in adolescents and young adults who use PMPs.8 Besides noise from PMPs, there has also been concern about mobile phone use and hearing loss following reports that demonstrated significant changes in hearing thresholds, suggesting caution in the use of mobile phones to prevent auditory damage in children.9,10
Hutter et al.11 suggested that hearing impairment induced by PMPs may be a confounder in the association between mobile phone use and hearing loss. However, this was not further investigated in other studies. Additional investigations are therefore required to clarify the association among mobile phone use, PMP exposure, and hearing loss in adolescents.
The present investigation was undertaken within a large study investigating exposure to mobile phones and cognitive function in teenagers. Our aim was to determine whether exposure to PMPs in the morning immediately prior to hearing testing confounds the association between mobile phone use and the hearing threshold levels of adolescents.
Methods
The MoRPhEUS (Mobile Radiofrequency Phone Exposed Users Study) was a cohort study that investigated cognitive function, hearing loss, and blood pressure in year 7 students in 20 secondary schools across the metropolitan area of Melbourne, Australia. The methodological details of the study have been previously described.12 In brief, schools from the three sectors in the Victorian education system (independent, state, and Catholic schools) were randomly approached regarding participation in the study. Students aged 11 to 13 years were recruited from one of the year 7 level classes in each school. Ethical approval for the MoRPhEUS study was granted by the Monash University Human Research Ethics Committee, and written informed consent was obtained from all participants and their parents.
All eligible students completed two questionnaires: a one-page hearing health questionnaire and additional questions relating to PMP use in the main questionnaire. The students were first asked if they used a PMP for more than 2 hours per day; they were then asked if they had used a PMP on the morning prior to the audiometric testing. We also assessed whether they had been exposed to loud noise in the past 72 hours of the date of the interview. Further questions regarding listening times prior to the day of the interview were asked in a general questionnaire. The day before the hearing test, the study supervisors informed all students not to use their PMPs on the morning prior to the scheduled interview and audiometric testing. On the morning of the hearing test, each participant completed the hearing health questionnaire, including a question asking whether they had “listened to an iPod/MP3 player/Discman today.” The subjects were then categorized into two groups: the exposed group comprised students who had used PMPs within 3 hours of the hearing testing, and the unexposed group comprised those who had not used PMPs in the specified period.
Adolescents who did not provide information regarding PMP use and those with pre-existing ear problems such as grommet insertion, previous surgery, or ear disease were excluded from further analysis (Figure 1). We restricted our final analysis to only those students who also reported use of mobile phones.
Figure 1.
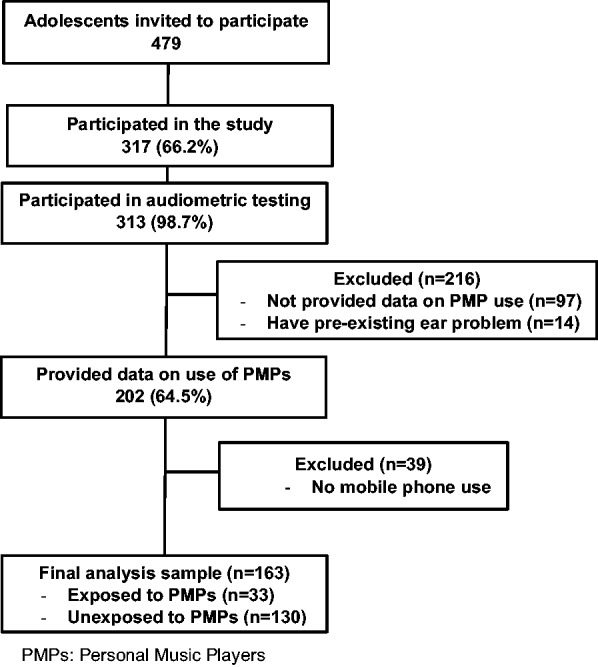
Study participant flow.
Pure-tone audiometry was undertaken using a Madsen Electronics MM304 audiometer (Otometrics, Taastrup, Denmark), calibrated and used in accordance with the pure-tone audiometric testing algorithm of the Australian Standard AS IEC 60645.1 and the ISO 8253–1: 2010.13,14 Measurements of air-conduction hearing threshold levels for each ear were undertaken in an audiological booth or a quiet room conforming to the background levels as specified in the Australian Standard AS/NZS 1269.4 2005,15 for the appropriate audiometric ear cups (TDH39). Before starting the testing, the test administrators checked the ambient sound pressure levels inside the testing rooms using a sound level meter. This was also done at the end of testing and confirmed to be within normal limits. The frequencies tested were 0.25 kHz, 0.50 kHz, 1 kHz, 1.5 kHz, 2 kHz, 3 kHz, 4 kHz, 6 kHz, and 8 kHz. The pure-tone averages were calculated by averaging the thresholds per ear obtained at each test frequency and were further classified into either low frequency (0.5, 1, and 2 kHz) or high frequency (3, 4, and 6 kHz) for each ear.16,17 The results were then aggregated for the PMP exposed and unexposed groups. An otological examination was performed to check the ear canal for wax and the tympanic membrane for possible inflammation or perforation using the Welch Allyn otoscope (Model 25020; Welch Allyn, Skaneateles Falls, NY, USA).
The hearing threshold was compared between the exposed and unexposed groups using t-tests on each individual metric (i.e., low frequency right ear, high frequency right ear, low frequency left ear, and high frequency left ear). As previously described,12 exposure to mobile phones was assessed using the total reported number of voice calls made and received per week. This included the log10 transformation of total calls made and received by adolescents; i.e., the log(total calls). When the respondent specified a range of calls per week, the arithmetic average was chosen. Unlike the total number of calls made and received, the log(total calls) was normally distributed. An offset of 1 was added to include valid zeroes, and the distribution was truncated at 70 to exclude extreme outliers and obtain a more representative statistic. Text messaging (SMS) was not expected to have any effect upon hearing, so this was omitted from the current analysis.
Adjusting for clustering within schools, the use of regression methods with robust estimation of variance did not lead to any appreciable difference from the results that were unadjusted for clustering; therefore, only the latter results are reported for simplicity. We did not adjust for clustering in our analysis of exposure to mobile phones because a previous analysis did not find any clustering effects.12 All statistical analyses were undertaken using Stata version 13.0 (StataCorp, College Station, TX, USA). All tests were two-sided, and P < 0.05 was considered statistically significant.
Results
A total of 479 students were approached, 313 of whom underwent audiometric testing. Of these 313 students, 202 (64.5%) provided data on PMP use in the MoRPhEUS study. The ages of the 202 adolescents enrolled ranged from 11 to 13 years, and 60.9% were girls. Of the 163 (80.7%) who responded to the mobile phone use question, 33 (20.2%) were exposed while 130 (79.8%) were unexposed to the use of PMPs in the morning prior to hearing testing.
The results of mobile phone use (average number of calls per week for those using mobile phones to make and receive calls) by PMP use on the morning prior to hearing testing are summarized in Table 1. There was no significant difference between the PMP exposed and unexposed groups in relation to their calls using mobile phones (mean difference of log(total calls), −0.16; 95% confidence interval, −0.35 to 0.03).
Table 1.
Self-reported use of mobile phones (total calls per week) by adolescents unexposed and exposed to PMPs prior to audiometric testing.
| n | Mean log(total calls)* | SD log(total calls) | |
|---|---|---|---|
| Unexposed to PMPs prior to hearing test | 130 | 0.96 (95% CI, 0.90–1.02) | 0.36 |
| Exposed to PMPs prior to hearing test | 33 | 1.12 (95% CI, 0.94–1.30) | 0.50 |
PMPs, personal music players; CI, confidence interval; SD, standard deviation
*Mean difference in log(total calls) = −0.16 (95% CI, −0.35 to 0.03) using the separate variable formula.
The use of PMPs for more than 2 hours per day was reported by 14 (38%) adolescents in the exposed group and 28 (17%) in the unexposed group (odds ratio, 2.98; 95% confidence interval, 1.37–6.50). However, there was no significant difference between the PMP exposed and unexposed groups in relation to their exposure to loud music in the last 72 hours before the date of the interview (χ2 = 2.09). No significant difference was observed between boys and girls in relation to their mobile phone use (χ2 = 0.087) or exposure to PMPs prior to the hearing test (χ2 = 0.039).
Table 2 presents the audiological results of adolescents by their PMP exposure status. We did not restrict the audiological results to only those reporting mobile phone use; therefore, the numbers analyzed in Table 2 are greater than those in Table 1 (n = 37 exposed and n = 165 unexposed). Likewise, there was no significant difference in the hearing thresholds for each frequency by the PMP exposure status of adolescents for each ear (Figure 2). Adolescents exposed to PMPs in the morning prior to audiometric testing did not have significantly different threshold shifts compared with the unexposed group in any of the four metrics (low frequency right, high frequency right, low frequency left, and high frequency left).
Table 2.
Hearing thresholds (dB HL) for the left and right ears of participants unexposed and exposed to PMPs prior to audiometric testing.
| LF_Right (dB) | HF_Right (dB) | HF_Left (dB) | LF_Left (dB) | |
|---|---|---|---|---|
| Unexposed to PMPs (n = 165) | 7.47 ±4.42(6.79–8.14) | 9.33 ±5.55(8.48–10.18) | 8.93 ±6.19(7.98–9.88) | 8.60 ±5.45(7.76–9.44) |
| Exposed to PMPs(n = 37) | 7.74 ±4.83(6.13–9.35) | 9.50 ±6.41(7.36–11.64) | 9.50 ±5.74(7.59–11.41) | 9.14 ±5.31(7.37–10.91) |
| Mean difference* | −0.28(−1.89 to 1.33) | −0.17(−2.22 to 1.88) | −0.57(−2.77 to 1.62) | −0.55(−2.49 to 1.40) |
| Total | 7.52 ± 4.49 | 9.36 ± 5.70 | 9.03 ± 6.10 | 8.70 ± 5.41 |
Except for the mean difference, data are presented as mean ± standard deviation and 95% confidence interval.
PMPs, personal music players; LF, low frequency (0.5, 1, and 2 kHz); HF, high frequency (3, 4, and 6 kHz).
*Pairwise comparisons (unexposed vs. exposed) in each metric (e.g., LF_Right).
Figure 2.

Hearing thresholds for right and left ears by personal music player exposure prior to audiometry in adolescents (broken line, exposed, n = 37; solid line, unexposed, n = 165).
Discussion
This study investigated whether exposure to PMPs in the morning immediately prior to hearing testing confounds the association between mobile phone use and hearing threshold levels of adolescents. The findings showed no significant difference between the hearing threshold levels of the PMP exposed and unexposed groups. The hearing thresholds ranged from 7 to 9 dB among students in the two groups; this is considered well within the normal range. This finding is also consistent with previously published reports that defined normal hearing as any pure tone average of <15 dB in both ears for adolescents.17,18 The disproportionate use of PMPs for more than 2 hours per day by the exposed group was not surprising because these were the students who inadvertently used their players on the morning of the audiometric testing.
Previous reports have also affirmed that adolescents and young adults often play their MP3 players at maximum volume.2,19 However, reports regarding the likelihood of TTS with significant individual variability in auditory function tests following digital music player use have produced conflicting results.20,21 A more recent study of 17-year-old Swedish students also showed worse measured hearing thresholds for those who listened to digital music players at louder volumes.22 Our results suggest that normal use of PMPs prior to audiometric testing is unlikely to induce significant hearing loss incurred by the use of these devices that may introduce confounding in the association between mobile phone use and hearing threshold levels of adolescents. Previous studies have demonstrated that music exposure results in a reliable but small TTS that quickly recovers.20,23
Furthermore, there was no difference in mobile phone use between the two groups. Because confounders must be associated with both the exposure and the outcome, the current findings suggest a lack of evidence for significant confounding due to the use of PMPs in the MoRPhEUS study. Our results do not support the suggestion by Hutter et al.11 that use of PMPs may introduce confounding in mobile phone studies.
The strengths of this study lie in its design and power. The design of this study involved a quasi-random selection of exposed and unexposed students because the exposed students were those who forgot to avoid using their PMPs on the morning of the audiometric testing. This characteristic should have been independent of the subjects’ hearing status. This study also had sufficient power to determine statistical differences in the mean hearing threshold of ≤3 dB. Pure-tone audiometry performed by a trained and experienced operator will at best be accurate to about 2 dB across most frequencies.18 A shift in the hearing threshold of ≥3 dB would have given cause for concern because previous studies have reported only small (2- to 3-dB) differences in pure-tone audiometric thresholds in users of PMPs compared with nonusers.7,23,24 Our results indicate that the differences between the exposed and unexposed groups were much smaller than this minimum clinically important shift.8
The limitations of this study can be summarized in four main areas. First, our study design was cross-sectional; therefore, we could only test for the hearing threshold that simultaneously contained both TTS and PTS components. This is a limitation that has been discussed in detail previously.25 In any event, serial testing to determine the use of TTS as a surrogate for PTS is questionable. Furthermore, previous studies do not provide conclusive information about the lasting effects of leisure noise on hearing thresholds.26
The absence of a statistically significant difference between the PMP exposed and unexposed groups in the hearing test results infers that the level or duration of exposure to noise from PMPs is unlikely to cause significant shift in the hearing threshold levels of adolescents.
The second limitation is that we relied upon the self-reported hearing history provided by the subjects; the students in the exposed group were self-selected because they had forgotten to avoid using their devices on the morning of the hearing testing. This may have introduced non-differential misclassification that cannot be quantified. Our third limitation involves the use of only pure-tone audiometry. We did not perform bone conduction testing or other standard audiological tests that might have indicated some other difference in the acoustic profiles of the two groups. Finally, the fourth limitation is that the exposure to mobile phone use was assessed using the total reported number of voice calls made and received per week; however, mobile phones are used for multiple purposes these days.
In conclusion, we found no evidence for confounding by exposure to PMPs in this study of the hearing threshold and mobile phone use. However, we recommend caution in future mobile phone studies that investigate outcomes such as hearing loss and tinnitus because our results may not be generalizable to adult populations. Because the use of PMPs is growing not only in adolescents but also in young adults,5,8,27 future research will require greater focus on longer periods of exposure to mobile phones and PMPs to improve on the current findings. Serial audiometry after the establishment of baseline thresholds may also provide more robust results.
Acknowledgements
The authors would like to thank all the participants of this study.
Declaration of conflicting interests
MA holds small parcels of shares in Telstra and SingTel, both of which operate mobile telephone networks in Australia. CD and DM hold small parcels of Telstra shares. GB, BZ, and II have no competing interests.
Funding
The MoRPhEUS study was funded by the National Health and Medical Research Council of Australia (NHMRC) and was conducted in collaboration with the Australian Centre for Radiofrequency Bioeffects Research (ACRBR). GB and DM are funded by the NHMRC.
References
- 1.Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR), Potential health risks of exposure to noise from personal music players and mobile phones including a music playing function, http://ec.europa.eu/health/archive/ph_risk/committees/04_scenihr/docs/scenihr_o_018.pdf (2008).
- 2.Vogel I, Brug J, Hosli EJ, et al. MP3 players and hearing loss: adolescents' perceptions of loud music and hearing conservation. J Pediatr 2008; 152: 400–404. [DOI] [PubMed] [Google Scholar]
- 3.Sulaiman AH, Husain R, Seluakumaran K. Hearing Risk among Young Personal Listening Device Users: Effects at High-Frequency and Extended High-Frequency Audiogram Thresholds. J Int Adv Otol 2015; 11: 104–109. [DOI] [PubMed] [Google Scholar]
- 4.Williams W, Burgess M. The combination of workplace and recreational noise exposure. Acoustics Australia 2007; 35: 91–96. [Google Scholar]
- 5.Twardella D, Raab U, Perez-Alvarez C, et al. Usage of personal music players in adolescents and its association with noise-induced hearing loss: A cross-sectional analysis of Ohrkan cohort study data. Int J Audiol 2017; 56: 38–45. [DOI] [PubMed] [Google Scholar]
- 6.le Clercq CM, van Ingen G, Ruytjens L, et al. Music-induced Hearing Loss in Children, Adolescents, and Young Adults: A Systematic Review and Meta-analysis. Otol Neurotol 2016; 37: 1208–1216. [DOI] [PubMed] [Google Scholar]
- 7.Kim MG, Hong SM, Shim HJ, et al. Hearing threshold of Korean adolescents associated with the use of personal music players. Yonsei Med J 2009; 50: 771–776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jiang W, Zhao F, Guderley N, et al. Daily music exposure dose and hearing problems using personal listening devices in adolescents and young adults: A systematic review. Int J Audiol 2016; 55: 197–205. [DOI] [PubMed] [Google Scholar]
- 9.Samkange-Zeeb F, Blettner M. Emerging aspects of mobile phone use. Emerg Health Threats J 2009; 2: e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Medeiros LN, Sanchez TG. Tinnitus and cell phones: the role of electromagnetic radiofrequency radiation. Braz J Otorhinolaryngol 2016; 82: 97–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hutter HP, Moshammer H, Wallner P, et al. Tinnitus and mobile phone use. Occup Environ Med 2010; 67: 804–808. [DOI] [PubMed] [Google Scholar]
- 12.Abramson MJ, Benke GP, Dimitriadis C, et al. Mobile telephone use is associated with changes in cognitive function in young adolescents. Bioelectromagnetics 2009; 30: 678–686. [DOI] [PubMed] [Google Scholar]
- 13.Standards Australia Electroacoustics-Audiological equipment- Pure-tone audiometer. Part 1: Pure-tone audiometers (IEC 60645–1:2001, MOD), 2002.
- 14.ISO. 8253-1: 2010. Acoustics: Audiometric test methods, Part 1: Pure-tone air- and bone-conduction audiometry. Geneva: International Organization for Standardization, 2000. [Google Scholar]
- 15.Australian/New Zealand Standard. Occupational noise management. Part 4: Auditory assessment, 2014.
- 16.Niskar AS, Kieszak SM, Holmes A, et al. Prevalence of hearing loss among children 6 to 19 years of age: the Third National Health and Nutrition Examination Survey. JAMA 1998; 279: 1071–1075. [DOI] [PubMed] [Google Scholar]
- 17.Wake M, Tobin S, Cone-Wesson B, et al. Slight/mild sensorineural hearing loss in children. Pediatrics 2006; 118: 1842–1851. [DOI] [PubMed] [Google Scholar]
- 18.Marcoux AM, Feder K, Keith SE, et al. Audiometric thresholds among a Canadian sample of 10 to 17 year old students. J Acoust Soc Am 2012; 131: 2787–2798. Available at: https://www.ncbi.nlm.nih.gov/pubmed/22501057. [DOI] [PubMed] [Google Scholar]
- 19.Torre P., 3rd Young adults' use and output level settings of personal music systems. Ear Hear 2008; 29: 791–799. [DOI] [PubMed] [Google Scholar]
- 20.Le Prell CG, Dell S, Hensley B, et al. Digital music exposure reliably induces temporary threshold shift in normal-hearing human subjects. Ear Hear. 2012; 33: e44–e58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Spankovich C, Griffiths SK, Lobarinas E, et al. Temporary threshold shift after impulse-noise during video game play: laboratory data. Int J Audiol 2014; 53(Suppl 2): S53–S65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Widen SE, Basjo S, Moller C, et al. Headphone listening habits and hearing thresholds in swedish adolescents. Noise Health 2017; 19: 125–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Le Prell CG, Spankovich C, Lobarinas E, et al. Extended high-frequency thresholds in college students: effects of music player use and other recreational noise. J Am Acad Audiol 2013; 24: 725–739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Meyer-Bisch C. Epidemiological evaluation of hearing damage related to strongly amplified music (personal cassette players, discotheques, rock concerts)–high-definition audiometric survey on 1364 subjects. Audiology 1996; 35: 121–142. [DOI] [PubMed] [Google Scholar]
- 25.Roger P. Hamernik, Donald Henderson, Salvi R. New perspectives on noise-induced hearing loss. New York: Raven Press, 1982. [Google Scholar]
- 26.Carter L, Williams W, Black D, et al. The leisure-noise dilemma: hearing loss or hearsay? What does the literature tell us? Ear Hear 2014; 35: 491–505. [DOI] [PubMed] [Google Scholar]
- 27.Rabinowitz PM. Hearing loss and personal music players. BMJ 2010; 340: c1261. [DOI] [PubMed] [Google Scholar]