

Abstract
Background:
It is estimated that postpartum depression (PPD) occurs in 10–15% of women in the year after childbirth. The highest number of women with PPD has limited access to psychosocial and pharmacological interventions. Long-distance counseling via mobile phone might be useful for the treatment of women with PPD, specifically in regions with low socioeconomical status and rural areas.
Objective:
Due to the high prevalence of PPD and its effects on health status of mothers and babies, we aimed to determine whether long-distance counseling via mobile phone text messaging is efficacious for the treatment of mothers at PPD risk.
Materials and Methods:
This pre-test and post-test clinical study was conducted in 2014 on 54 women referred to hospital affiliated to Hormozgan University of Medical Sciences in the south of Iran. Data were collected twice (baseline and follow-up) through telephone interviews for assessing PPD risk of participants via the Edinburgh Postnatal Depression Scale (EPDS). The participants were recontacted by phone within 14 days after their childbirth. Women at PPD risk (EPDS ≥12) were included in the study to receive daily text messages and others were excluded. Each mother received two daily text messages via mobile phones for 35 days. The data were analyzed using SPSS 16.
Results:
The average age of participants was 27.27 (range 17–35). Findings revealed that sending text messages to women with PPD would decline PPD. At pre-test, the average score for PPD was 14.44 (SD = 2.66) and it was declined to 11.94 (SD = 2.49) at the post-test phase. There was a significant difference between pre-test and post-test evaluations (P-value < 001).
Conclusions:
Long-distance counseling through sending text messages to patients with PPD can be an effective treatment along with other current treatments. This can improve mothers’ health literacy about maternal postpartum psychological disorders.
Keywords: Cell phone, childbirth, long-distance counseling, postpartum depression, pregnancy, text messaging
Introduction
Traditional interventions for postpartum depression (PPD), such as pharmacology and psychotherapy, are faced with several difficulties for new mothers including childcare, cost, and time. Therefore, it is essential to use new interventions for preventing or treating PPD.[1] PPD is an important mental health disorder, which occurs among 10–15% of mothers and begins any time after delivery and last up even more than 1 year. Treatment of PPD varies according to the severity and causes of the disease and is usually a combination of psychotherapy and pharmaceutical therapy.[2] Unfortunately, many new mothers are not aware of their illness and are unable or do not seek help for their treatment. Poor treatment may result in many considerable consequences for mothers, their partners, and their infants.[3] There are multiple barriers to appropriate treatment of mothers with PPD, including lack of time, not wanting to take medication, the stigma of PPD, lack of neonate's care, and cost,[4] which make it necessary to utilize alternative interventions such as the use of telephone and web-based interventions to provide patients with psychological interventions.[5,6] These tools ensure a rapidly modern approach for extending the accessibility to effective depression treatments for postpartum disorders.[3] Thus, those mothers who are reluctant to seek treatment for reasons such as geographical restrictions can willingly schedule to receive and follow their desired mode of therapy at home.[7]
A number of studies have investigated the effect of telephone and web-based interventions on mothers with PPD. For instance, Dennis indicated that telephone-based peer support in 4 weeks had a considerable impact on the control and relief of PPD of high-risk mothers. The majority of mothers were satisfied with this type of intervention.[8] Moreover, Lewis et al. used a telephone-based exercise intervention to encourage mothers to do exercises at least 5 days a week and 30 minutes per session for the prevention of PPD. This exercise intervention included telephone counseling and sending of motivational information to participants via e-mail which lasted for 6 months.[1] Furthermore, Pugh et al. indicated that internet-delivered cognitive behavior therapy (ICBT) was effective in reducing symptoms of PPD.[1]
Given the importance of appropriate prescription of information to mothers with PPD, specifically in low-income and developing countries, it is necessary to assess the utility of new and alternative methods in the treatment of this disorder. A number of studies have reported a higher rate of depression associated with childbirth in developing countries.[9] Thus, more attention should be paid to mental health status of mothers in such countries, specifically among socioeconomically deprived families. Although a number of studies have focused on telephone and web-based interventions, to our knowledge, text message interventions have not been used to support mothers with PPD. The purpose of this paper is, then, to illustrate this novel treatment approach for woman afflicted with PPD in a developing country, Iran.
Materials and Methods
We used a one-group, pre–post study design with data, collected at baseline and 35 days after the intervention. The study was conducted at Bandar Abbas, a city at the southern coast of Iran. Like other developing countries, the prevalence of PPD in Iran is higher than the average rate (25.3%).[10] We recruited women from the caesarean section delivery of a medical university affiliated hospital (level I with around 7,000–8,000 births/year) in Bandar Abbas city, Iran, in 2014. This is a maternity teaching hospital in which the majority of hospitalized women are whom with low or middle income families. The women with higher socioeconomic status in the city tend to give birth in private hospitals, as private hospitals provide higher quality services than public hospitals. The mothers are usually discharged within 24 hours after normal delivery and 48 hours after cesarean delivery.
Eligible participants were healthy women who had given birth for the first time; healthy and live singleton neonates born at 37–41 weeks of gestation, age of 17–37, owning a mobile phone, able to read and understand text messages, and women with partners who lived in Bandar Abbas city in Iran. Exclusion criteria included mothers with hospitalized infants in a neonatal intensive care unit, history of depression prior to or during pregnancy, having a serious medical condition, experiencing stressful life events during pregnancy, such as the death of a family member, previous miscarriage, obstetric complications, severe problems after childbirth such as infections and bleeding, consuming medications that might cause psychiatric disorders, and illiterate women. Women were also excluded if they used drugs and alcohol. Moreover, according to a systematic review in Iran, we excluded employed women and women with unplanned pregnancy.[10] The study sample size was calculated as 10, using the following formula and also the data of Gjerdingen et al. study (mean score of pre/post-interventions: 32.5 (SD = 8.2), 17.8 (SD = 9.9), respectively).[11] However, we recruited 54 participants. The significance level set at 5% risk of failure (=0.05).
In this phase, the project was throughly explained to women who were hospitalized for delivery and had the criteria to be included in the study. They were given the opportunity to ask their questions about the project. Those women who consented to participate in the study were registered by name, age, phone number, and address in Bandar Abbas for latter contacts. Data were collected twice (preintervention and postintervention) through telephone interviews. At 2 weeks after birth, the mothers were administered the Edinburgh Postnatal Depression Scale (EPDS), a widely used screening tool for detecting mothers with PPD. EPDS contains 10 items which, according to the Likert style, are scored from 0 (never) to 3 (yes, most of the time) and the scores range from 0 to 30. Mothers who obtain higher scores are more likely to have greater postpartum depressive symptoms.[4] The initial validation study of the Iranian version of the EPDS indicated that it was an acceptable, reliable, and valid measure of postnatal depression.[12] Thus, in the current study, we used the Persian (Iranian language) version of the EPDS. Women who scored 12 or more were considered to have PPD and were included in the intervention phase. Among the hospitalized women, those mothers who had the inclusion criteria were registered for later contacts. This phase was continued until the necessary study samples were included in the intervention phase. Women who scored more than 12 on the EPDS within the first 2 weeks after childbirth were recruited. Mothers received two daily text messages for 35 days. One week after the 35-day follow-up, the mothers were re-administered the EPDS [Table 1].
Table 1.
Age groups and the frequency of delivery types of women with postpartum depression who received mobile phone text messages support
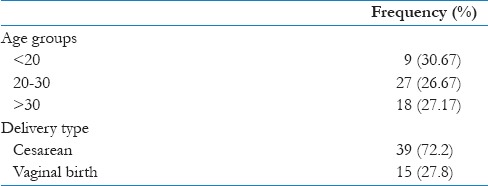
Women at PPD risk (EPDS ≥12) were included in the study to receive daily text messages. Each day two text messages were sent to mothers via a mobile phone for 35 days. Mobile phone text messages were sent to mothers between 10 and 11 am and between 7 and 8 pm. During the intervention phase, mothers could send us a message or call the health care providers in the research team (a nurse and a midwife), if they preferred to receive no more messages to be excluded from the study. The program aimed to provide new mothers with relevant information on PPD after the childbirth. This program motivated mothers with depressive symptoms to seek treatment. Text messages included information regarding topics such as general information about blue and PPD, techniques to cope with PPD symptoms, exercises to practice these techniques, relaxation techniques, interaction with other women with PPD, emotional changes in pregnancy, changes and challenges in partner relationship, interaction with infant, the importance of social support, etc.
The outcome measure in this study is depressive symptomatology which is measured by using the EDPS. The outcome of this study will potentially benefit a number of mothers with PPD. The study was approved by the ethics committee of Science and Research Branch, Islamic Azad University of Bandar Abbas, Hormozgan, Iran. Permission to conduct the study was also obtained from Hormozgan University of Medical Sciences, Bandar Abbas, Iran. All patients gave their consent.
Data were analyzed with SPSS 16 (Chicago, IL, USA). Descriptive analyses, including frequencies and means, were conducted on the demographic and pre/postintervention items. Nonparametric tests were used to perform statistical comparisons due to the non-normal data and the small sample sizes. The Wilcoxon signed-ranks test was used for pairwise pre/postcomparisons. The Mann–Whitney test was used to test the relationship between the pre/post interventions and type of delivery. Kruskal–Wallis test was used to test the relationship between the pre/postinterventions and level of education and also the relationship between pre/postinterventions and age groups.
Results
In a 3-week period, we interviewed the women who had hospitalized for childbirth to identify those who had the inclusion criteria. After childbirth at the hospital, we randomly selected the women and if a woman had the inclusion criteria, she was registered by a nurse in our team to be contacted 14 days later. This process continued consecutively after 103 women completed the baseline questionnaire, of which 63 scored above 12 in EDPS. However, seven women did not consent to participate in the study. Thus, 56 women completed the baseline questionnaire. One week after the 35-day intervention program ended, participants were requested to fill out the follow-up questionnaire. However, one woman did not answer our phone contacts (this woman was contacted three times in 2 days) and one woman was excluded from the study as she was not allowed by her husband to fill out the follow-up questionnaire. In overall, 54 women were included in the analysis. The average age of participants was 27.27 (range = 17–35) years. The 25-year-old women had the most frequency. Overall, 35 women (64.8%) had a degree below high school diploma or had a diploma degree, 15 women (27.8%) had a bachelor, and 4 had a master's degree (7.4%).
The EPDS scores of 42 participants decreased, whereas that of 8 participants increased in the follow-up phase and the scores of 4 participants did not change. At baseline, the majority of women scored 12 (23 [46.6%]), and in the follow-up phase, the majority of participants scored 13 (10 [18.5%]).
Results showed that the mean score of EDPS before pre-intervention was 14.44 (SD = 2.66) and the mean post-intervention score was 11.94 (SD = 2.49). Wilcoxon signed-ranks test revealed statistically significant differences between pre -and postintervention on EDPS. The mean overall decrease in scores on the EPDS pre -and post-intervention items was 2.5 points (P–value < 0.001). The Mann–Whitney test showed that there was no relationship between the pre -and postinterventions according to type of delivery (cesarean = 29.18 and vaginal birth = 23.13, P–value = 0.2). Furthermore, Kruskal–Wallis test indicated that the differences between pre -and post-interventions was not significant in regard with level of education (preintervention P–value = 0.76, post-intervention P–value = 0.81). Also, using Kruskal–Wallis test showed that the differences between pre- and postinterventions was not significant in regard to age groups (pre-intervention P–value = 0.78, post-intervention P–value = 0.73).
Moreover, we investigated the satisfaction level of participants with the support received. Mothers were asked to mention their satisfaction with the text messaging support experience. Results showed that the majority of women (26 [48.1%]) were moderately satisfied with text massages treatment delivery, followed by low satisfaction (21 [38.9%]), and high satisfaction (7 [13%]), respectively.
Discussion
To our knowledge, this article describes the first study that used mobile phone text messaging intervention for women with PPD. The primary aim of this study was to examine the efficacy of a text-messaging-based psychoeducational intervention for decreasing postnatal depressive symptoms and the treatment of PPD. Our participants were new mothers in a teaching hospital of a deprived region in Iran. Findings revealed that there was a significant difference between pre -and postintervention evaluations (preintervention SD = 2.66; postintervention SD = 2.49; (P –value < 0.001)). Edinburg postnatal scale was included to assess depressive symptoms. The satisfaction level was moderate as mentioned by 48.1% of participants.
As mentioned before, current interventional methods for supporting mothers with PPD are faced with many barriers such as lack of time for neonate's care and face-to-face psychotherapy, high cost of current treatments, and lack of access to treatments for those women in remote areas. For this reason, some studies examined the effectiveness of information and communication technologies such as telephone and web in supporting mothers with PPD. For example, Dennis studied the effect of peer support on PPD. This study concluded that telephone-based peer support has a positive effect on the decrease of depressive symptomatology among new mothers.[8] On the other hand, Mohammad-Alizadeh-Charandabi et al. could not find a significant relationship between the intervention and control groups regarding frequency of depression after a 2-month postnatal telephone support by a midwife (29.9% vs. 31.6%; Odds ratio 0.91, 95% CI 0.56–1.49),[13] whereas Kamalifard et al. showed that peer support via telephone was effective in the prevention of PPD.[14]
Moreover, some studies have used internet and web therapy with the practice of psychotherapy to overcome many of the barriers related to face-to-face psychotherapy for PPD. For example, Pugh et al. used a new therapeutic approach, that is ICBT, and indicated that at post-treatment, the interventions were effective in reducing PPD symptoms.[6] Our study is consistent with these studies. We indicated that text-delivered therapy via mobile phones decreased the PPD symptoms of mothers after post-intervention. However, there was not a significant difference between pre- and postinterventions according to type of delivery, level of education, and age groups. One reason could be that the sample size of our study was small. Our results can be important clinically as further studies may indicate that these types of treatment delivery might be effective for mothers with PPD.
It is maintained that the majority of mothers were satisfied with receiving telephone-based support for PPD.[15] However, contacting mothers with telephone is a laboring work that may lead to the lower degree of satisfaction with this form of supporting mothers with PPD. Other challenges include contacting mothers by mentors or supporters. Thus, these challenges should be taken into consideration when conducting a telephone support intervention study.[15] A treatment satisfaction among mothers with ICBT therapy and a strong therapeutic alliance is also reported. Delivering treatment via the internet is beneficial when a woman is performing her maternal duties such as breastfeeding.[6] In this study, we introduced a novel and promising method that is receiving treatment over mobile phone text messaging, which does not have the limitations of telephone contacts with mothers and the barriers of internet therapy such as low internet speed in deprived regions, rural, and remote areas. However, similar to telephone supports and web interventions, this innovative approach is also expected to overcome many of the barriers related to face-to-face psychotherapy for PPD. Mobile phones have the capacity of receiving text messages as well as accessing internet and online communication applications, such as WhatsApp, Viber, and Telegram. Nowadays, with the emergence of mobile internet in developing countries like Iran, as well as remote areas, sending text messages via mobile applications is more popular than other communication tools and probably is the easiest way of communication. Our study also showed that mothers were moderately satisfied with this type of treatment delivery. This is consistent with the majority of previous studies that used telephone and internet therapy for supporting mothers with PPD. These types of treatments ensure receiving necessary psychological treatments and educational information at home or wherever convenience for mothers or at the time that suits her. As mentioned by Pugh et al., (2014) this address challenges related to mobility and child caring.[6]
Strengths and Limitations
This study has some limitations, including its single-group, pre–post study design. Also, the weaknesses of the study include its selection bias that resulted in a homogenous sample that impairs the study generalizability and another bias was the use of a self-assessment tool (EDPS) for PPD diagnosis. Researchers lacked an automatic text messaging system to send messages to mothers. Such a system would improve the interaction between healthcare givers and patients. An automatic text messaging system gives mothers the chance to determine the time of receiving text messages, to send their feedbacks, and to ask their related questions. It is, therefore, proposed that the impact of psychoeducation via text messaging on patient outcomes should be followed up in future studies and the methodological limitations in this study should be improved.
Further research should also focus on studies investigating the effectiveness of text messaging interventions delivered in the antenatal period on the prevention of PPD. A larger study should be undertaken to evaluate the clinical and cost effectiveness of the text messaging intervention.
Conclusions
Using text messaging technology can improve access to and quality of interventions. There is a need to use new interventions such as text-messaging for supporting mothers with PPD. Test massaging improves the flexibility of treatment delivery and use of non-face-to-face contact. This may overcome many of the barriers to PPD treatment such as timely access to therapeutic counseling. Text messaging does not have the challenges related to telephone and internet therapy such as managing time to receive the treatment. Long-distance counseling via mobile phone text massaging declined the average score for PPD by 2.5 (P < 0.001). Therefore, this clinical study could fundamentally change how caregiver interventions are delivered. The implications of this study for policy and practice are that the mental health of mothers should be considered in postnatal care, specifically in low-income countries. Given the shortage of mental health manpower, the role of care will need to be met by new intervention methods such as text messaging.
Financial support and sponsorship
This study was supported by the Science and Research Branch, Islamic Azad University, Bandar Abbas, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to acknowledge the support of Science and Research Branch, Islamic Azad University of Bandar Abbas in Iran, and the Health Information Management Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran. We also appreciate Miss Naghdi who helped us in data collection, as well as the mothers who participated in the study.
References
- 1.Lewis BA, Gjerdingen DK, Avery MD, Guo H, Sirard JR, Bonikowske AR, et al. Examination of a telephone-based exercise intervention for the prevention of postpartum depression: Design, methodology, and baseline data from the healthy mom study. Contemp Clin Trials. 2012;33:1150–8. doi: 10.1016/j.cct.2012.07.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dennis CL, Dowswell T. Psychosocial and psychological interventions for preventing postpartum depression. Cochrane Database Syst Rev. 2013;28:CD001134. doi: 10.1002/14651858.CD001134.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Danaher BG, Milgrom J, Seeley JR, Stuart S, Schembri C, Tyler MS, et al. Web-based intervention for postpartum depression: Formative research and design of the MomMoodBooster program. JMIR Res Protoc. 2012;1:e18. doi: 10.2196/resprot.2329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Maloni JA, Przeworski A, Damato EG. Web recruitment and internet use and preferences reported by women with postpartum depression after pregnancy complications. Arch Psychiatr Nurs. 2013;27:90–5. doi: 10.1016/j.apnu.2012.12.001. [DOI] [PubMed] [Google Scholar]
- 5.Grigoriadis S, Ravitz P. An approach to interpersonal psychotherapy for postpartum depression: Focusing on interpersonal changes. Can Fam Physician. 2007;53:1469–75. [PMC free article] [PubMed] [Google Scholar]
- 6.Pugh NE, Hadjistavropoulos HD, Fuchs CM. Internet therapy for postpartum depression: A case illustration of emailed therapeutic assistance. Arch Womens Ment Health. 2014;17:327–37. doi: 10.1007/s00737-014-0439-2. [DOI] [PubMed] [Google Scholar]
- 7.Andrews G, Cuijpers P, Craske MG, McEvoy P, Titov N. Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: A meta-analysis. PLoS One. 2010;5:e13196. doi: 10.1371/journal.pone.0013196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dennis CL. The effect of peer support on postpartum depression: A pilot randomized controlled trial. Can J Psychiatry. 2003;48:115–24. doi: 10.1177/070674370304800209. [DOI] [PubMed] [Google Scholar]
- 9.Rahman A, Iqbal Z, Harrington R. Life events, social support and depression in childbirth: Perspectives from a rural community in the developing world. Psychol Med. 2003;33:1161–7. doi: 10.1017/s0033291703008286. [DOI] [PubMed] [Google Scholar]
- 10.Veisani Y, Delpisheh A, Sayehmiri K, Rezaeian S. Trends of postpartum depression in Iran: A systematic review and meta-analysis. Depress Res Treat 2013. 2013:291029. doi: 10.1155/2013/291029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gjerdingen DK, McGovern P, Pratt R, Johnson L, Crow S. Postpartum doula and peer telephone support for postpartum depression: A pilot randomized controlled trial. J Prim Care Community Health. 2013;4:36–43. doi: 10.1177/2150131912451598. [DOI] [PubMed] [Google Scholar]
- 12.Montazeri A, Torkan B, Omidvari S. The edinburgh postnatal depression scale (EPDS): Translation and validation study of the Iranian version. BMC Psychiatry. 2007;7:11. doi: 10.1186/1471-244X-7-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mohammad-Alizadeh-Charandabi S, Malakoti J, Sohrabi F, Shokranian N. The effect of telephone support on postpartum depression: A randomized controlled trial. J Caring Sci. 2013;2:147–55. doi: 10.5681/jcs.2013.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kamalifard M, Yavarikia P, Babapour Kheiroddin J, Salehi Pourmehr H, Iraji Iranagh R. The effect of peers support on postpartum depression: A single-blind randomized clinical trial. J Caring Sci. 2013;2:237–44. doi: 10.5681/jcs.2013.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dennis CL. Postpartum depression peer support: Maternal perceptions from a randomized controlled trial. Int J Nurs Stud. 2010;47:560–8. doi: 10.1016/j.ijnurstu.2009.10.015. [DOI] [PubMed] [Google Scholar]