

Abstract
Increased tibial slope can be a cause of recurrent instability after anterior cruciate ligament reconstruction. This article presents a technique for an anterior closing-wedge osteotomy for slope correction. The indications for this procedure are patients with recurrent instability after anterior cruciate ligament reconstruction with a neutral leg axis or slightly varus deformity and a posterior slope of more than 12°. The exposure of the anterior aspect of the tibia is best made through an anterior approach approximately 1 to 2 cm medial to the tibial tuberosity. Hohmann retractors are placed from the medial and lateral sides behind the proximal tibia. The osteotomy lines are marked with 2 converging Kirschner wires with the use of an image intensifier. The entry point of the first Kirschner wire is just below the most inferior fibers of the patellar tendon. The hinge of the osteotomy should be just below the tibial insertion of the posterior cruciate ligament. The osteotomy is performed with an oscillating saw. The posterior cortex of the tibia should be left intact. After removal of the anterior base wedge, the osteotomy is closed by manual pressure. Osteosynthesis is performed with a lag screw from the tibial tuberosity to the distal tibia and an angular stable plate fixator.
Bony deformities as a cause of recurrent instability after anterior cruciate ligament (ACL) reconstruction have received increased attention in recent years.1, 2, 3, 4, 5, 6, 7, 8, 9 Various studies have shown that the inclination of the tibial plateau in the sagittal plane (slope) affects the stability of the knee joint.1, 10, 11 Owing to the posteriorly sloping articular surface, the tibia glides anteriorly under load (Fig 1). In the uninjured knee this anterior translation is prevented by the ACL. The higher the slope, the higher the in situ forces in the ACL. This means that an ACL graft will be increasingly loaded with an increased posterior slope.
Fig 1.
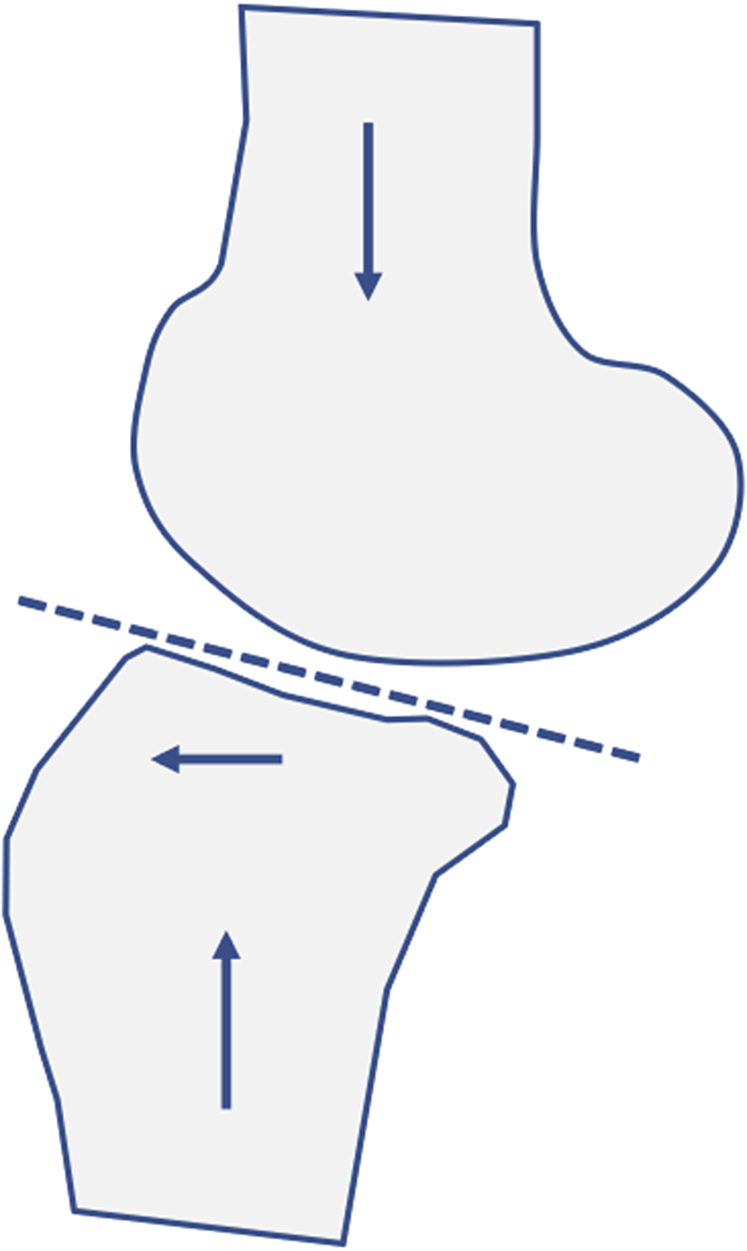
Effect of tibial slope on dynamic stability of knee joint. The left-facing arrow conveys the anterior translation of the tibia, and the up and down arrows convey the axial load.
Biomechanical studies have confirmed this concept.1, 6, 12 Agneskirchner et al.1 performed flexion osteotomies on knee joint preparations and biomechanically measured anterior translation. Their study showed that an increase in the posterior slope led to increased anterior translation of the tibia. Moreover, Giffin et al.6 investigated the effect of slope elevation on knee kinematics and "in situ" forces in the cruciate ligaments on human knee joint specimens. In their study, an elevated tibial slope under load similarly resulted in anterior displacement of the tibia relative to the femur. With increasing slope, increasing in situ forces in the ACL have been observed. Shelburne et al.12 have simulated the effect of a slope increase in a computer model. Their study showed that a slope increase led to increased anterior shear forces and increased anterior translation in activities of daily living (standing, squatting, and walking). In all these studies, it was concluded that increased tibial slope should be considered in patients with anterior instability. In veterinary medicine, osteotomies to reduce posterior tibial slope have long been used to treat anterior knee instability in dogs.13
In many cases, deformities in the sagittal plane are combined with deformities in the frontal plane (double varus and increased tibial slope). For double-varus deformity, a medial opening-wedge osteotomy is recommended for correction.8, 10, 14, 15, 16 With this technique, slope correction is larger in the medial compartment whereas the lateral slope is difficult to address. Christensen et al.17 have shown by magnetic resonance imaging that, in particular, an increased lateral tibial slope is associated with an increased risk of ACL graft failure. To address the lateral tibial slope. Dejour et al.3 and Sonnery-Cottet et al.18 described an anterior closing-wedge osteotomy at the level of the tibial tuberosity. A potential disadvantage of this technique is that the tibial tuberosity has to undergo osteotomy.
This article presents a technique for slope correction in which the anterior wedge is removed below the tibial tuberosity without the need to detach the tibial tuberosity.
Surgical Technique
Indications and Contraindications
Proper patient selection is very important for the success of this surgical procedure. The indications for this procedure are patients with recurrent instability after ACL reconstruction with a neutral leg axis or slightly varus deformity and a posterior slope of more than 12°. Because there is now clear evidence of a relation between tibial slope and rerupture, a slope-correcting osteotomy also may be indicated in some patients with a primary ACL injury and a posterior tibial slope of more than 15°.
Contraindications for this procedure include hyperextension of the knee (>10°), a varus deformity greater than 5°, and grade IV bicompartmental osteoarthritis according to Kellgren and Lawrence. Relative contraindications are a high body mass index (>30) and intensive smoking (>20 cigarettes per day).
Preoperative Planning
The aim of this operation is to reduce the increased tibial slope by removing an osseous wedge from the tibia distally to the tibial tuberosity (Fig 2, Video 1). To determine the tibial slope, various methods of measurement have been used in the literature.19, 20, 21, 22 Most authors have used lateral radiographs for slope determination.19, 20, 21, 22 On the lateral radiograph, the proximal anatomic tibial axis and a tangent to the medial tibial plateau are the most common reference lines. For these reference lines, the mean value of the posterior slope on the lateral radiograph is 7°, with a range between 0° and 10°.22 A posterior slope greater than 12° is considered increased in the literature.4, 13, 15, 21
Fig 2.

Anterior opening-wedge osteotomy. The osteotomy starts directly under the insertion of the patellar tendon. The hinge of the osteotomy is located just under the tibial insertion of the posterior cruciate ligament.
The amount of slope correction is planned on the lateral radiographic image (Fig 3). The postoperative slope should be less than 10°. When planning the slope correction, the preoperative extension of the knee joint must be taken into account. A genu recurvatum should be avoided. As a rule, the posterior slope is corrected by 6° to 8°.
Fig 3.
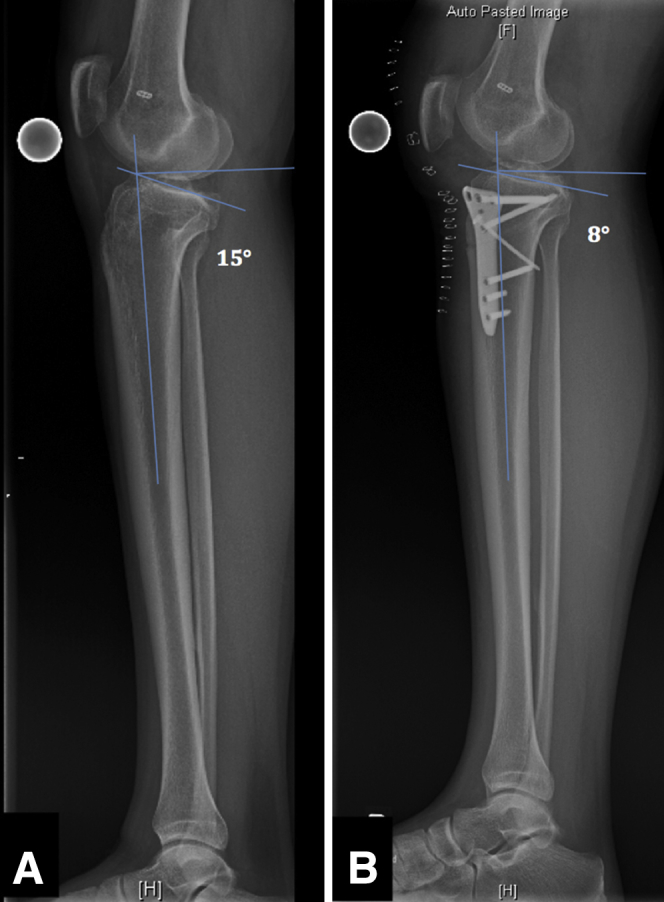
(A) Preoperative radiograph of a patient with recurrent anterior instability after anterior cruciate ligament reconstruction and with a posterior slope of 15°. The proximal anatomic tibial axis and a tangent to the medial tibial plateau are the reference lines for measurement. (B) Postoperative radiograph after anterior closing-wedge osteotomy.
Patient Setup
The patient is positioned supine on a radiolucent table. The procedure can be performed with general and spinal anesthesia. Perioperative antibiotic prophylaxis is performed with a third-generation cephalosporin. For surgery, the lower extremity is placed in a mobile leg holder. For the osteotomy, the knee should be flexed at about 45° (Fig 4). This position serves to protect the vessels and nerves in the popliteal fossa during osteotomy. For the osteosynthesis, the knee should be extended because the extension maintains the correction.
Fig 4.

The lower extremity is placed in a mobile leg holder at about 45° of flexion for the osteotomy. The black line marks the anterior approach approximately 1 to 2 cm medial to the tibial tuberosity. (ACL, anterior cruciate ligament.)
Diagnostic Arthroscopy
Arthroscopy of the knee joint should be performed before the osteotomy. Arthroscopy is used for evaluation of cartilage and meniscal injuries, as well as treatment of intra-articular damage. The slope correction can be combined with other surgical procedures such as primary or revision ACL reconstruction or bone tunnel filling with autologous or allogeneic cancellous bone. Other arthroscopic procedures (e.g., notchplasty or meniscal and cartilage surgery) are often required.
Exposure
The exposure of the anterior aspect of the tibia is best made through an anterior approach approximately 1 to 2 cm medial to the tibial tuberosity (Fig 4). However, in many revision cases, previous incisions exist and could be used for the approach or should be included in the approach. Then, the lateral extensor muscles have to be detached from the proximal tibia (Fig 5). Medially, a rasp is used to separate the superficial portion of the medial collateral ligament from the tibial bone. Hohmann retractors are placed from the medial and lateral sides behind the proximal tibia (Fig 6). After exposure of the tibial tuberosity, the osteotomy lines are marked with 2 converging 2.0-mm Kirschner wires (K-wires) with the help of an image intensifier (Fig 7). The K-wires are drilled obliquely in the proximal tibia. The entry point of the first K-wire is just below the most inferior fibers of the patellar tendon. The hinge of the osteotomy should be just below the tibial insertion of the posterior cruciate ligament. The surgeon should endeavor to leave the posterior cortex intact. An intact posterior cortex limits the risk of pseudarthrosis and protects the popliteal neurovascular structures. The height of the anteriorly based wedge depends on the preoperative planning; it is usually between 6 and 8 mm (Fig 8).
Fig 5.

Exposure of tibial tuberosity through medial incision. A Hohmann retractor protects the tibial head. With a rasp, the lateral extensor muscles have to be detached.
Fig 6.

Two Hohmann retractors protect the tibial head. With a rasp, the superficial portion of the medial collateral ligament is carefully separated. Then, the first Kirschner wire (K-wire) is drilled obliquely in the proximal tibia. The entry point of the first K-wire is just below the most inferior fibers of the patellar tendon.
Fig 7.
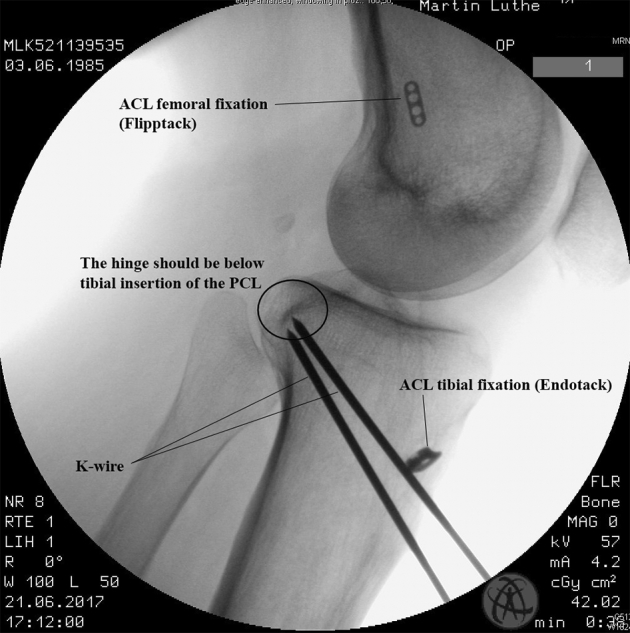
Fluoroscopic image with 2 obliquely ascending Kirschner wires that mark osteotomy. In this case, the Flipptack and Endotack (Karl Storz) were used for anterior cruciate ligament (ACL) fixation. (PCL, posterior cruciate ligament.)
Fig 8.

With a surgical ruler, the preoperative wedge height can be measured between the 2 Kirschner wires (K-wires).
Osteotomy and Implant Placement
Once the K-wires are in the correct position, the osteotomy is performed with an oscillating saw (TRS-Modular Drive; Synthes, West Chester, PA). During the osteotomy, the saw must be cooled with fluid (sodium chloride) to avoid heat damage to the tibial bone (Fig 9). The posterior cortex of the tibia serves as a hinge for the osteotomy. To avoid damage to the posterior cortex, a surgical ruler should be used to measure the length of the inserted K-wires (Fig 10). We recommend marking the length of the osteotomy on the oscillating saw (Fig 11). The K-wires and a narrow saw blade guide the oscillating saw (Fig 12). In patients with a slightly varus deformity, the osteotomy can also be 2-dimensional with an anterior- and lateral-based wedge (Fig 13).
Fig 9.

To avoid heat damage to the tibial bone during the osteotomy, the saw must be cooled with fluid (sodium chloride [NaCl]).
Fig 10.

To avoid damage to the posterior cortex, a Kirschner wire (K-wire) measuring device should be used to measure the length of the inserted K-wires.
Fig 11.

The length of the osteotomy is marked on the saw (arrow) to prevent damage to the posterior hinge and to protect the neurovascular structures. (K-wire, Kirschner wire.)
Fig 12.

The 2 Kirschner wires (K-wires) guide the osteotomy. In addition, a narrow saw blade can be used to guide the osteotomy.
Fig 13.

The anterior-based wedge is removed (asterisk). (K-wire, Kirschner wire.)
After removal of the anterior-based wedge, the osteotomy is closed by careful manual pressure (Fig 14). The osteotomy is closed when the 2 guide K-wires are parallel. Care must be taken to ensure that the lower extremity is not in unphysiological hyperextension after osteotomy. With the image intensifier, the amount of correction should be controlled. If the amount of correction is correct, osteosynthesis is performed with a lag screw from the tibial tuberosity to the distal tibia (Figs 14 and 15). This is followed by medial osteosynthesis with an angular stable plate fixator (e.g., Loqteq high tibial osteotomy plate; AAP Implants, Berlin, Germany). The angular stable plate can be slid under the skin to avoid a large incision (Fig 16). The plate is temporarily fixed with K-wires approximately 1 cm distal to the proximal tibia joint line. With an image intensifier, the plate position is controlled (Fig 17). Then, 4.5-mm locking screws are inserted. Typically, the proximal segment is stabilized with 4 locking screws and the distal segment is stabilized with 3 locking screws (Fig 18).
Fig 14.

After removal of the anterior-based wedge, the osteotomy is closed by careful manual pressure. (K-wire, Kirschner wire.)
Fig 15.
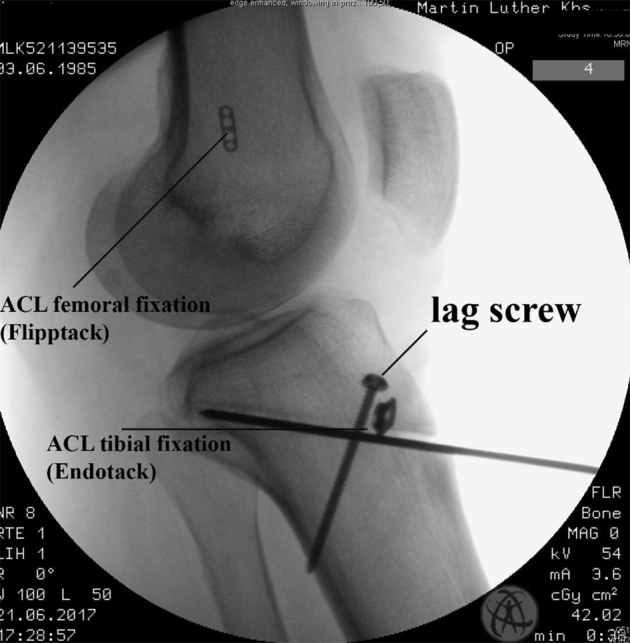
Fluoroscopic image with inserted lag screw from tibial tuberosity to distal tibia.
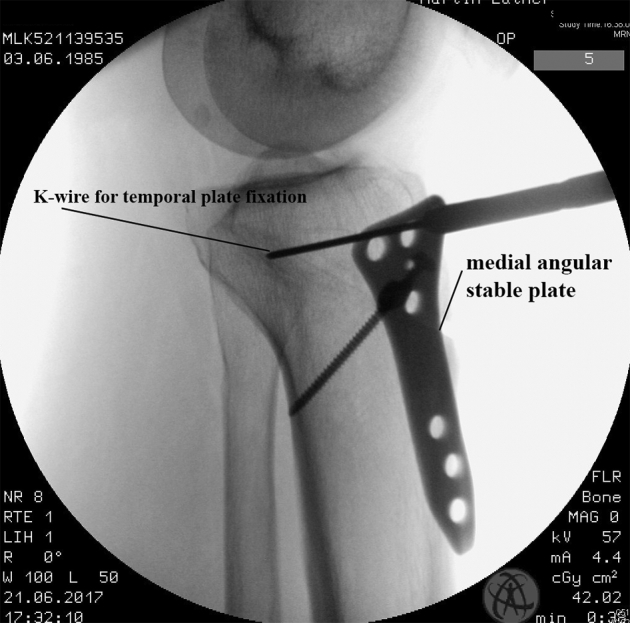
Fig 16.

The osteosynthesis is completed with a medial angular stable plate fixator (Loqteq high tibial osteotomy plate). The angular stable plate can be slid under the skin to avoid a large incision. (K-wire, Kirschner wire.)
Fig 17.
The medial plate is temporally fixed with Kirschner wires (K-wires) approximately 1 cm distal to the proximal tibial joint and checked with the image intensifier.
Fig 18.

Final lateral intraoperative radiograph with image intensifier. The closed osteotomy gap is clearly visible.
A Redon drain is normally not needed. After skin closure, a compressive dressing is applied.
Rehabilitation
The patient is mobilized with partial weight bearing with 10 kg for 2 weeks. Range of motion is not restricted. The stitches are removed postoperatively after 12 days. If the patient has plate-associated pain or discomfort, removal of the internal plate fixator can be performed.
Discussion
In this article, we present a technique for subtuberosity closing-wedge osteotomy for the correction of increased tibial slope. The effectiveness of this technique has been proven in clinical practice in recent years.
For patients with recurrent instability and a double-varus situation, a medial opening-wedge high tibial osteotomy is the gold standard to reduce the number of subjective instability events.8, 14, 15, 23 With a medial opening-wedge osteotomy, the tibial slope of the medial tibial plateau can be addressed if increased.8, 15 The potential of the medial opening-wedge osteotomy to correct an increased tibial slope of the lateral plateau, however, is limited.
Recent studies have shown that the lateral slope plays a defining role in recurrent instability after ACL reconstruction.17, 24 For this reason, it is especially important to address the lateral slope during revision surgery. Compared with the medial opening-wedge technique, this is best achieved with the subtuberosity closing-wedge osteotomy. Moreover, not all patients with an increased tibial slope have an associated varus deformity. In these cases an anterior closing-wedge osteotomy may be indicated.
For the anterior closing-wedge osteotomy, only 2 retrospective case series can be found in the literature. In both case series, an anterior closing-wedge osteotomy was described in which the tibial tuberosity must be detached.3, 18
Dejour et al.3 reported 9 patients who had undergone a second rupture of an ACL reconstruction. All patients had a posterior slope greater than 12°. These patients underwent an anterior closing-wedge osteotomy in combination with ACL reconstruction (quadriceps tendon in 8 and semitendinosus tendon in 1). The slope decreased from 13.2° ± 2.6° to 4.4° ± 2.3°. The mean Lysholm score was 73.8 ± 5.8, and the subjective International Knee Documentation Committee score was 71.6 ± 6.1. Dejour et al. concluded that the satisfactory results of this study suggest that the slope correction protects the reconstructed ACL from failure.
Sonnery-Cottet et al.18 examined 5 patients after a slope-reducing anterior closing-wedge osteotomy in combination with an ACL reconstruction after a period of 32 months. The mean posterior tibial slope decreased from 13.6° preoperatively to 9.2° postoperatively. The mean Lysholm score was 46.2 preoperatively and increased to 87.8 postoperatively. The mean subjective International Knee Documentation Committee score was 39.5 before surgery and 79.1 at the last follow-up. The mean Tegner activity score reached the same level as before the last ACL injury (7.4 and 7.2). Anterior laxity measured with the KT-1000 arthrometer (MEDmetric, San Diego, CA) decreased from 10.4 to 2.8 mm. Sonnery-Cottet et al. concluded that a combined ACL rerevision with proximal anterior closing-wedge osteotomy can restore the stability and function of the knee joint and prevent rerupture.
In both studies, the indication for an anterior closing-wedge osteotomy is a revision situation with a tibial slope greater than 12° and a neutral or slightly varus leg axis.3, 18 A possible disadvantage of these techniques is that the tibial tuberosity has to be detached for the anterior closing-wedge osteotomy. With the subtuberosity osteotomy described in this article, this additional surgical step can be avoided.
As with any other proximal tibial osteotomy, the anterior closing-wedge osteotomy is associated with various pitfalls. These pitfalls and the solutions for prevention are listed in Table 1. In summary, the anterior closing-wedge osteotomy described in this article is a safe method to reduce the tibial slope in patients with anterior instability.
Table 1.
Most Common Pitfalls of Closing-Wedge Osteotomy and Measures for Prevention
| Pitfall | Preventive Measure |
|---|---|
| Pseudarthrosis and healing complications |
|
| Injury to popliteal vessels and nerves |
|
| Undercorrection or overcorrection |
|
Footnotes
The authors report the following potential conflict of interest or source of funding: W.P. receives support from AAP Implants, Otto Bock Health Care, Karl Storz. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
Technique for anterior closing-wedge osteotomy for slope correction. The patient is positioned supine on a radiolucent table, and the lower extremity is placed in a mobile leg holder. An anterior approach is used approximately 1 to 2 cm medial to the tibial tuberosity. The lateral extensor muscles have to be detached from the proximal tibia. The superficial portion of the medial collateral ligament is separated from the tibial bone. After exposure of the tibial tuberosity, the osteotomy lines are marked with 2 converging 2.0-mm Kirschner wires. The entry point of the first Kirschner wire is just below the most inferior fibers of the patellar tendon. The hinge of the osteotomy should be just below the tibial insertion of the posterior cruciate ligament. The height of the anteriorly based wedge depends on the preoperative planning; it is usually between 6 and 8 mm. The osteotomy is performed with an oscillating saw. After removal of the anterior-based wedge, the osteotomy is closed by careful manual pressure. If the amount of correction is correct, osteosynthesis is performed with a lag screw from the tibial tuberosity to the distal tibia. This is followed by medial osteosynthesis with an angular stable plate fixator. Typically, the proximal segment is stabilized with 4 locking screws and the distal segment is stabilized with 3 locking screws.
References
- 1.Agneskirchner J.D., Hurschler C., Stukenborg-Colsman C., Imhoff A.B., Lobenhoffer P. Effect of high tibial flexion osteotomy on cartilage pressure and joint kinematics: A biomechanical study in human cadaveric knees. Winner of the AGA-DonJoy Award 2004. Arch Orthop Trauma Surg. 2004;124:575–584. doi: 10.1007/s00402-004-0728-8. [DOI] [PubMed] [Google Scholar]
- 2.Arun G.R., Kumaraswamy V., Rajan D. Long-term follow up of single-stage anterior cruciate ligament reconstruction and high tibial osteotomy and its relation with posterior tibial slope. Arch Orthop Trauma Surg. 2016;136:505–511. doi: 10.1007/s00402-015-2385-5. [DOI] [PubMed] [Google Scholar]
- 3.Dejour D., Saffarini M., Demey G., Baverel L. Tibial slope correction combined with second revision ACL produces good knee stability and prevents graft rupture. Knee Surg Sports Traumatol Arthrosc. 2015;23:2846–2852. doi: 10.1007/s00167-015-3758-6. [DOI] [PubMed] [Google Scholar]
- 4.Diermeier T., Imhoff A.B., Beitzel K. Flexion and extension osteotomy of the knee. Oper Orthop Traumatol. 2017;29:330–338. doi: 10.1007/s00064-017-0499-3. [in German] [DOI] [PubMed] [Google Scholar]
- 5.Feucht M.J., Mauro C.S., Brucker P.U., Imhoff A.B., Hinterwimmer S. The role of the tibial slope in sustaining and treating anterior cruciate ligament injuries. Knee Surg Sports Traumatol Arthrosc. 2013;21:134–145. doi: 10.1007/s00167-012-1941-6. [DOI] [PubMed] [Google Scholar]
- 6.Giffin J.R., Stabile K.J., Zantop T., Vogrin T.M., Woo S.L., Harner C.D. Importance of tibial slope for stability of the posterior cruciate ligament deficient knee. Am J Sports Med. 2007;35:1443–1449. doi: 10.1177/0363546507304665. [DOI] [PubMed] [Google Scholar]
- 7.Todd M.S., Lalliss S., Garcia E., DeBerardino T.M., Cameron K.L. The relationship between posterior tibial slope and anterior cruciate ligament injuries. Am J Sports Med. 2010;38:63–67. doi: 10.1177/0363546509343198. [DOI] [PubMed] [Google Scholar]
- 8.Tischer T., Paul J., Pape D. The impact of osseous malalignment and realignment procedures in knee ligament surgery: A systematic review of the clinical evidence. Orthop J Sports Med. 2017;5 doi: 10.1177/2325967117697287. 2325967117697287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lee C.C., Youm Y.S., Cho S.D. Does posterior tibial slope affect graft rupture following ACL reconstruction? Arthroscopy. 2018;34:2152–2155. doi: 10.1016/j.arthro.2018.01.058. [DOI] [PubMed] [Google Scholar]
- 10.Noyes F.R., Barber S.D., Simon R. High tibial osteotomy and ligament reconstruction in varus angulated, anterior cruciate ligament-deficient knees. A two- to seven-year follow-up study. Am J Sports Med. 1993;21:2–12. doi: 10.1177/036354659302100102. [DOI] [PubMed] [Google Scholar]
- 11.Black M.S., d'Entremont A.G., McCormack R.G., Hansen G., Carr D., Wilson D.R. The effect of wedge and tibial slope angles on knee contact pressure and kinematics following medial opening-wedge high tibial osteotomy. Clin Biomech. 2018;51:17–25. doi: 10.1016/j.clinbiomech.2017.10.021. [DOI] [PubMed] [Google Scholar]
- 12.Shelburne K.B., Kim H.J., Sterett W.I., Pandy M.G. Effect of posterior tibial slope on knee biomechanics during functional activity. J Orthop Res. 2011;29:223–231. doi: 10.1002/jor.21242. [DOI] [PubMed] [Google Scholar]
- 13.Kim S.E., Pozzi A., Kowaleski M.P., Lewis D.D. Tibial osteotomies for cranial cruciate ligament insufficiency in dogs. Vet Surg. 2008;37:111–125. doi: 10.1111/j.1532-950X.2007.00361.x. [DOI] [PubMed] [Google Scholar]
- 14.Dejour H., Neyret P., Boileau P., Donell S.T. Anterior cruciate reconstruction combined with valgus tibial osteotomy. Clin Orthop Relat Res. 1994;(299):220–228. [PubMed] [Google Scholar]
- 15.Feucht M.J., Tischer T. Osteotomies around the knee for ligament insufficiency. Orthopade. 2017;46:601–609. doi: 10.1007/s00132-017-3439-x. [in German] [DOI] [PubMed] [Google Scholar]
- 16.Noyes F.R., Barber-Westin S.D., Hewett T.E. High tibial osteotomy and ligament reconstruction for varus angulated anterior cruciate ligament-deficient knees. Am J Sports Med. 2000;28:282–296. doi: 10.1177/03635465000280030201. [DOI] [PubMed] [Google Scholar]
- 17.Christensen J.J., Krych A.J., Engasser W.M., Vanhees M.K., Collins M.S., Dahm D.L. Lateral tibial posterior slope is increased in patients with early graft failure after anterior cruciate ligament reconstruction. Am J Sports Med. 2015;43:2510–2514. doi: 10.1177/0363546515597664. [DOI] [PubMed] [Google Scholar]
- 18.Sonnery-Cottet B., Mogos S., Thaunat M. Proximal tibial anterior closing wedge osteotomy in repeat revision of anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42:1873–1880. doi: 10.1177/0363546514534938. [DOI] [PubMed] [Google Scholar]
- 19.Brazier J., Migaud H., Gougeon F., Cotten A., Fontaine C., Duquennoy A. Evaluation of methods for radiographic measurement of the tibial slope. A study of 83 healthy knees. Rev Chir Orthop Reparatrice Appar Mot. 1996;82:195–200. [in French] [PubMed] [Google Scholar]
- 20.Faschingbauer M., Sgroi M., Juchems M., Reichel H., Kappe T. Can the tibial slope be measured on lateral knee radiographs? Knee Surg Sports Traumatol Arthrosc. 2014;22:3163–3167. doi: 10.1007/s00167-014-2864-1. [DOI] [PubMed] [Google Scholar]
- 21.Utzschneider S., Goettinger M., Weber P. Development and validation of a new method for the radiologic measurement of the tibial slope. Knee Surg Sports Traumatol Arthrosc. 2011;19:1643–1648. doi: 10.1007/s00167-011-1414-3. [DOI] [PubMed] [Google Scholar]
- 22.Waldt S., Eiber M., Wörtler K. Thieme; Stuttgart: 2011. Messverfahren und Klassifikationen in der muskuloskelettalen Radiologie. [Google Scholar]
- 23.Trojani C., Elhor H., Carles M., Boileau P. Anterior cruciate ligament reconstruction combined with valgus high tibial osteotomy allows return to sports. Orthop Traumatol Surg Res. 2014;100:209–212. doi: 10.1016/j.otsr.2013.11.012. [DOI] [PubMed] [Google Scholar]
- 24.van Eck C., Azar A., Yaseen Z., Irrgang J., Fu F., Musahl V. Increased lateral tibial plateau slope predisposes male college football players to ACL injury. Arthroscopy. 2016;32(suppl):e7–e8. doi: 10.2106/JBJS.15.01163. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Technique for anterior closing-wedge osteotomy for slope correction. The patient is positioned supine on a radiolucent table, and the lower extremity is placed in a mobile leg holder. An anterior approach is used approximately 1 to 2 cm medial to the tibial tuberosity. The lateral extensor muscles have to be detached from the proximal tibia. The superficial portion of the medial collateral ligament is separated from the tibial bone. After exposure of the tibial tuberosity, the osteotomy lines are marked with 2 converging 2.0-mm Kirschner wires. The entry point of the first Kirschner wire is just below the most inferior fibers of the patellar tendon. The hinge of the osteotomy should be just below the tibial insertion of the posterior cruciate ligament. The height of the anteriorly based wedge depends on the preoperative planning; it is usually between 6 and 8 mm. The osteotomy is performed with an oscillating saw. After removal of the anterior-based wedge, the osteotomy is closed by careful manual pressure. If the amount of correction is correct, osteosynthesis is performed with a lag screw from the tibial tuberosity to the distal tibia. This is followed by medial osteosynthesis with an angular stable plate fixator. Typically, the proximal segment is stabilized with 4 locking screws and the distal segment is stabilized with 3 locking screws.