

Abstract
Background:
Road traffic injuries (RTIs) are a complex phenomenon caused by nonlinear combination and interaction of man, vehicles, road, and environment.
Aim:
This study aims to find out the outcome and severity of RTI in a district of West Bengal, India.
Settings and Design:
A cross-sectional study was conducted among inpatients of Departments of Surgery and Orthopedics of Bankura Sammilani Medical College and Hospital, West Bengal, India.
Materials and Methods:
The study was conducted for 1 year interviewing 295 RTI selected through scheduled sampling. Information pertaining to demographic and correlates of RTI was collected by face to face and over telephone using semi-structured questionnaire. Nine-item Simplified Injury Severity Scale (SISS) was used to assess injury severity. Internal consistency of SISS scale was showed by Cronbach's alpha and association with the correlates was done by Mann–Whitney U-test.
Statistical Analysis Used:
With SPSS version 22.0, binary logistic regression, and Mann–Whitney U-test.
Results and Conclusion:
Fatal outcome in terms of death and permanent disability was 34.24% and they had higher marginally significant (P = 0.06), SISS score (45.17 ± 12.59). Participants with absence of protective devices, presence of comorbidities, drunkenness, with accidents over national highways, in-between 6 am and 6 pm, mechanized two-wheelers, and nonreceipt of first aid were found to have significantly high scores compared to their counterpart. SISS, as a proxy measure of severity assessment, could throw a light on it and awareness generation and legislative stringency might be need of the hour for the country.
Keywords: Accidents, cross-sectional study, logistic regression, Mann–Whitney U
INTRODUCTION
Road traffic injury (RTI) can be defined as, “An event that occurs on a way or street open to public traffic; resulting in one or more persons being injured or killed, where at least one moving vehicle is involved.”[1]
During 2014, a total of 450,898 cases of “road accidents” were reported which rendered 477,731 persons injured and 141,526 deaths. Deaths due to RTI in India have increased by 2.9% during 2014 (141,526) over 2013 (137,423). A total of 51 cases of road accidents took place every 1 h during 2014, wherein 16 persons were killed.[2]
Considering RTIs as a major health burden on the global community, the United Nations General Assembly proclaimed 2011–2020 as the Decade of Action for Road Safety with the overall goal to stabilize and then halve the level of road traffic fatalities around the world.[3]
Road safety is a multisectoral and multidimensional issue. Dr. William Haddon developed an analytical tool by considering road transport as an ill-designed “man-machine” interface requiring a comprehensive systemic approach defining a crash event in three phases of the time sequence: precrash, crash, and postcrash – as well as the epidemiological triad of human, vehicle, and environment that can interact during each phase of a crash. The resulting nine-cell Haddon matrix models a dynamic system, with each cell of the matrix allowing opportunities for intervention to reduce road crash injury.[4]
Very few studies have been found to address the determinants of severity of accidents, especially in West Bengal where total number of RTI cases was 120,585 with death rate being 9.1% from January to December 2014.[5]
In Bankura district, the traffic accidents are getting increased with all its severity day by day. Still, this area is mostly unexplored, especially in this part of the country.
This study was embarked upon to find out various human-, environmental-, and treatment-related factors determining outcome and severity of RTI of the study participants.
MATERIALS AND METHODS
Study design and settings
An institution-based, descriptive, cross-sectional study was conducted from July 1, 2015 to June 30, 2016 in the Inpatient Departments of Surgery and Orthopedics of Bankura Sammilani Medical College and Hospital (BSMC), Bankura, West Bengal.
Study population and sampling
The study population was comprised of the RTI victims admitted in the inpatients, of them who were unconscious or in disoriented state without any accompanying person available at the time of interview were purposively excluded from the participation. As per literature, the prevalence rate of death from road traffic accident (RTA) was found to be 46%.[5] The sample size was calculated as (Zα)2× p × (100-p)/L2= (1.96)2 × 46 × 54/6 × 6 = 265. (Where Zα = standard normal deviate at 95% confidence, P = prevalence, 100-p = complement to prevalence, L = allowable error around prevalence). Assuming 10% nonresponse rate, the sample size was revised to be (265 + 10% of 265) 292 which was rounded off to final sample size of 295. As data collection was done twice in a week including Sundays, the days were paired as Monday–Thursday, Tuesday–Friday, Wednesday–Saturday, and Thursday–Sunday so that all days of a week were covered for data collection. At the start, the pair of the days for the first day of data collection was selected by simple random sampling, and then sequentially other days were chosen.
Study tools
Data were collected using predesigned, pretested, semi-structured questionnaire (in local vernacular) and Simplified Injury Severity Scale (SISS)[6] for developing countries with nine items (age, body part injured, depth of injury, level and duration of consciousness, amount of bleeding, duration of hospitalization, type and result of treatment) with the total score varying from 14 to 75 and tallied with hospital records, especially for clinical findings. Content validity was tested with 13 subject matter experts and content validity ratio >0.54 was considered as per the number of subject matter experts. None of the items failed to achieve the minimum value. Language validation was done by two forward and two backward translations in parallel by two language experts, so that the meaning and contents of the items remained unaltered as well as sentences were grammatically correct. Pretesting of the questionnaire was conducted in Bishnupur District Hospital around 36.7 km from Bankura (through NH14) on 30 RTA inpatients for a period of 1 month (April 2015).
Operational definitions
Protective devices
Satisfactory: a) For motorized two-wheelers: having appropriate crash helmets. b) For four and more wheelers and rear seat occupants: having seat-belts.
Driving status
Driver: Professional drivers and nondrivers who were behind the steering but amateur driver.
Road condition
Satisfactory: Road was ply worthy and nonsatisfactory; depilated roads.
Type of car
Two-wheelers: motorized and non-motorized vehicles with two wheels.
Others: vehicles with more than two wheels.
Drunkenness
Present: The participant was under influence of alcohol and absent in otherwise.
Time between road traffic injury and treatment received
Less than 1 h: Within “golden hour” and ≥1 h: Beyond that time.
Distraction
Out of talking or texting over mobile phones – present or absent.
Data collection
Data collection was done by principal investigator as her designated assignment for partial fulfillment of the requirement for the degree of MD (community medicine) under supervision of corresponding author. The eligible patients admitted within previous 24 h of scheduled day of data collection were interviewed and information about sociodemographics, presence of various risk factors such as drunken driving, usage or nonusage of protective devices, distracted driving, environmental factors, and care seeking that is place of primary treatment received, time gap between accident and treatment received, and pattern of injury were collected. The patients were clinically observed for pattern of injuries. Relevant hospital records were reviewed for corroboration of findings as obtained during face to face and telephonic interview.
Data regarding further proceeding and duration of hospital stay and final outcome were collected through telephonic interview conducted after 1 month. Severity of injury of RTI victims was assessed by SISS.
Ethics
The study was conducted after obtaining ethical clearance from the Institutional Ethics Committee of BSMC and written permission from the HODs of Department of Surgery and Orthopedics.
Informed consent was obtained from the study participants as written or by LTI, as applicable and ascent from minors followed by guardian's consent was obtained.
Data analysis
Data analysis was done by the investigators themselves with the help of software SPSS version 22.0 (IBM, New York, USA) free version after entering the data in Microsoft Excel spreadsheet. Data were described by mean, median, standard deviation (SD), and proportion. Internal consistency of SISS was done by Cronbach's alpha. Association of SISS with correlates was done by nonparametric tests, that is, Mann–Whitney U-test. Binary logistic regression with adjusted odds ratio (AOR) and its 95% confidence interval (CI) was used to test for association of different correlates with outcome.
RESULTS
The study revealed that 70.51% of the study participants were male. The average age of the male and female patients was 36.02 ± 15.75 (mean ± SD) and 36.21 ± 18.08 years, respectively. More than two-thirds, 68.13% were from urban areas, 76.30% were Hindu, and 23.70% were Muslim and other religion by birth and belief. Proportion of patients belonged to SC and ST was 59%, 56% had lower educational level, 56.3% were from socioeconomic status (SES) IV and V (according to BG Prasad SES scale, modified in April 2016), and 60.4% were married.
Proportion of accident was more in the winter season (47.5%), toward the end and beginning of the week (51.86%) and between 6 am and 12 noon (40.68%).
Among the victims behind the steering, 32.86% were professional driver. Those who were in mechanized two-wheelers and four-wheelers, 87.18% had no protective device while accident. About 45.20% of the victims were drunk while 12.2% told that, they were distracted by talking or texting over mobile or were busy with playing video games just before the occurrence. Substantially, the higher number of accidents was witnessed by nonmetal roads (34.58%), with lack of ply worthiness (52.88%). Majority of the victims were the riders of two-wheelers (40%). The current study might give the assumption of driver fatigue being the contributing cause as among the forty professional drivers, majority of whom were long-distance truck drivers, 29, that is, 63.04% were driving continuously for ≥8 h before the occurrence and 65.71% told that they were not in position to take rest for at least 8 h before starting for the journey came fatal. Majority (65.69%) received extremity injuries causing walking inability (41.36%) and 67.32% could manage to reach medical college hospital within 1 h which is considered “golden hour” for RTIs in terms of chance of survival.
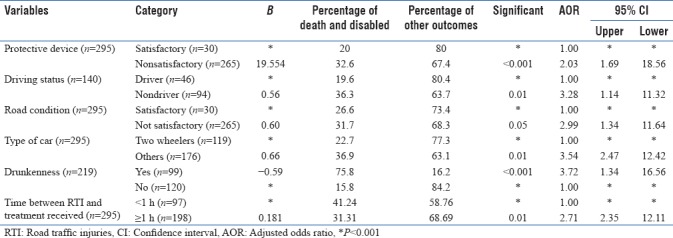
Slightly more than one-third (34.24%) faced fatal outcome, that is, death and disability. Binary logistic regression revealed significant statistical association (P < 0.05) between death, disability, and driving status (AOR = 1.01; 95% CI: 1.14–11.32); nonusage of protective devices (AOR = 1.66; 95% CI: 1.69–18.56); road condition (AOR = 1.01; 95% CI: 1.34–11.64); type of vehicle (AOR = 1.12; 95% CI: 2.47–12.42); drunkenness of victims (AOR = 1.02; 95% CI: 1.34–16.56); and time interval from occurrence of accident to receipt of primary treatment (AOR = 1.32; 95% CI: 2.35–12.11) [Table 1].
Table 1.
Binary logistic regression showing relationship between outcome of road traffic injuries and correlates
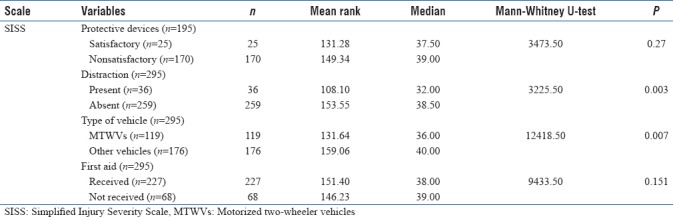
In Mann–Whitney U-test, for relationship between SISS score and human factors, the mean rank was higher for absence of protective devices (149.34), drunkenness (110.15), and absence of distraction (153.55). Therefore, these groups had greater number of high scores within them. It was significantly higher for the distraction scores only (P < 0.05). Regarding environmental factors, higher mean rank was there for accidents between 6 pm and 6 am (154.70), for vehicles other than mechanized two-wheelers (159.06), and accidents over national highways (150.09). Therefore, these groups had greater number of high scores within them. SISS level was only significant for type of vehicles (P < 0.05). SISS score and infirmity and treatment-related relation by Mann–Whitney U-test revealed higher mean rank for receipt of first aid (151.91) and receipt of primary treatment at medical college and hospital (151.40). Therefore, these groups had greater number of high scores within them [Table 2].
Table 2.
Distribution of road traffic injuries patients according to relationship between Simplified Injury Severity Scale and correlates
DISCUSSION
Sociodemographics
Age and gender inclination of the current study could be because males predominantly work outdoors being more commonly exposed to traffic and partly be due to their reckless behavior. This was similar to the findings made by Singh et al.[7] Among the study population, more than two-thirds were Hindu and proportion of SC and ST was more than half of the total study population. Similar results were found in studies conducted by Mehta[8] in Delhi and Choudhary et al. from Sevagram.[9] In this study, majority were from urban background which is in contrast to a study done by Singh et al. where found majority of the victims were from rural areas.[10]
Environmental factors of road traffic injury
The seasonal occurrence of the present study was in accordance with the observation made by Singh et al.[11] This might be caused by poor adaptability to light in the foggy environment as well as more numbers of local festivals observed during this time when people take more opportunity of getting drunkenness, ignoring traffic laws more which are compounded with more people gathering on roads, and making traffic maintenance more difficult. Similar findings were obtained by Bhuyan and Ahmed.[12] and Pathak et al.[13] Timing of majority of accidents in the current study had similarity to Mishra et al.[14] Among the 140 drivers who faced accident, nearly one-third were professional in the present study.
Precipitating factors for road traffic injury
Usage of protective devices was considered relevant only in cases of occupants of motorized two-wheeler vehicles (MTWV) and four-wheelers in the form of appropriate helmets and seat belt, respectively. As revealed in this study, overall usage of protective devices was quite low. Tripathy reported only 13.2% of two-wheeler vehicle passengers (drivers and pillion riders) were on helmets, of which 44.4% were ISI certified and so being full coverage helmets and only 7.5% of four-wheeler vehicle passengers (drivers and copassengers) were using seat belts at the time of accidents.[15] Singh et al.[16] and Pathak et al. got the similar findings.[17]
History of drunkenness in the present study was higher than observation by Bhuyan and corresponding findings were reported by Patil et al.,[18] Swaddiwudhipong et al.,[19] and Jha et al.[20] Nearly 46.37% of alcohol consumption was documented among drivers in a study by Mishra et al.[14] History of any kind of distraction in the current study was comparable to Shah 9.33%,[21] but Singh et al. found higher mobile phone usage among survivors of road crashes in North India.[16]
In the present study, timing of accidents was closely supported by Shah from Ahmadabad[21] and Pathak et al.,[13] whereas Singh et al. observed majority of the accidents between 12 pm and 8 pm.[10]
In the current study, more than two-third of drivers gave the history of inadequate rest before driving and among professional drivers, driving for continuous ≥ 8 h was rampant. Bayan et al. cited fatigue as a contributory factor for accident toward the fag end of journey.[22]
Pattern of injuries and road traffic accident
Pattern of injuries being over hands and legs in the present study was in concordance with Pathak et al.[13]
The “golden hour” philosophy and road traffic injuries
Role of “golden hour” presuming survival, behind Dr. R. Adams Cowley[23] in the current study had similar finding to Ansari et al.[24] and Lahiri et al.[25]
Outcome of road traffic injury
Findings on fatal outcome in terms of either death or permanent disability was comparable to Bhuyan and Ahmed[12] and Dandona and Mishra.[26]
Determining and influencing factors for severity of road traffic injury
This study revealed influence of alcohol, nonusage of protective devices, and history of any kind of distraction to be significantly associated with grave outcomes of accidents. Pathak et al. found higher odds for sustaining head injuries by the people who did not wear headgear.[13] Mishra et al. showed the presence of personal problems, alcohol consumption, usage of mobile phones, chronic diseases, and psychological conflicts were found to be significantly associated with fatality.[14]
Most fatal accidents took place in nonmetal and in-between 12 midnight and 6 am which might be contributed by sleepiness of the drivers besides loose traffic regulations at late night hours. Maximum grave outcome was observed in accidents in nonmechanized two-wheeler accidents. Singh et al. found significant association of fatality and daytime accidents.[10]
SISS score was significantly higher in the presence of distraction, two-wheelers, and injuries with associated danger signs. Shah found 21% of patients had low Glasgow Coma Scale at presentation.[21] Following Trauma Index Score (TIS), Jha et al. found majority with moderate-to-severe TIS,[20] whereas Kiran et al. showed 30.4% had moderate (TIS 8–18) and 11.2% severe (TIS > 18) injuries.[27]
Strength of the study
The study was conducted following schedule sampling; so that, the pattern and determinants of the RTI could be well depicted, especially in perspective to the representativeness of throughout the time frame.
Future directions of the study
Besides characterization of trauma, measuring the impact of intervention on RTI cases through well-designed public health and clinical research methods such as trauma registries and surveillance programs, this work is expected to open up new horizon in “Accidentology.” Intervention study with extensive awareness campaign might show rays of hope in future.
CONCLUSION
Nonusage of protective devices, steering in hands of nonprofessional drivers, poor road conditions, more wheeled vehicles, drunkenness, distraction, receipt of first aid, and lapsing ≥1 h on reaching health-care facility were found as major determinants of grave outcomes, be it measured directly or with the help of proxy measure as SISS.
Stringent enforcement of legislations requiring the use of helmets by users of MTWVs and seat belt by four-wheeler riders, prohibition of talking or texting while driving, no drinking while on steering and overall awareness generation towards current and potential road users might be helpful, to reduce the enlarging prevalence and addressing post-crush severity.
Limitations
For the present study, the data were collected from in-patients and hence who did not seek admission, might be brought dead or discharged after preliminary management were missed. As outcome was assessed by telephonic interview one month after initial data collection, there was chance of over and under-fabrication of actual information.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to express their gratitude toward all the nursing staff of the Department of General Surgery and Orthopedics, who helped a lot even during their busy hours while collecting data.
REFERENCES
- 1.Suri S, Parr M. The hidden epidemic-war on roads. Indian J Crit Care Med. 2004;8:69–72. [Google Scholar]
- 2.National Crime Record Bureau. New Delhi, India: Ministry of Home Affairs, Government of India; 2014. Ministry of Home Affairs, Government of India. Accidental Deaths and Suicides in India. [Google Scholar]
- 3.World Health Organization. Geneva: World Health Organization; 2011. Saving Millions of Lives-Decade of Action for Road Safety 2011-2020. [Google Scholar]
- 4.Haddon W., Jr The changing approach to the epidemiology, prevention, and amelioration of trauma: The transition to approaches etiologically rather than descriptively based. Am J Public Health Nations Health. 1968;58:1431–8. doi: 10.2105/ajph.58.8.1431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Directorate of Health Sciences. West Bengal: Government of West Bengal; [Last accessed on 2017 Aug 02]. Health on the March 2014-2015. State Bureau of Health Intelligence. Available from: http://www.wbhealth.gov.in . [Google Scholar]
- 6.Verma PK. Simplified injury severity scale for developing countries (SISS) Inj Prev. 2012;18:A1–246. [Google Scholar]
- 7.Singh A, Bhardwaj A, Pathak R, Ahluwalia SK. An epidemiological study of road traffic accident cases at a tertiary care hospital in rural Haryana. Indian J Community Health. 2011;23:53–6. [Google Scholar]
- 8.Mehta SP. An epidemiological study of road traffic accident cases admitted in Safdarjang hospital, New Delhi. Indian J Med Res. 1968;56:456–66. [PubMed] [Google Scholar]
- 9.Choudhary BL, Deepak S, Tirpude BH, Sharma RK, Veena M. Profile of road traffic accidents cases in Kasturba hospital of MGIMS, Sevagram, Wardha, Maharashtra, India. Med Legal Update. 2005;5:1–12. [Google Scholar]
- 10.Singh D, Singh SP, Kunran M, Goel S. Epidemiology of road traffic accidents in children in Chandigarh zone of North West India. Egypt J Forensic Sci. 2015;3:54–9. [Google Scholar]
- 11.Singh R, Singh HK, Gupta SC, Kumar Y. Pattern, severity and circumtances of injuries sustained in road traffic accidents: A tertiary care hospital-based study. Indian J Community Med. 2014;39:30–4. doi: 10.4103/0970-0218.126353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bhuyan PJ, Ahmed F. Road traffic accident: An emerging public health problem in Assam. Indian J Community Med. 2013;38:100–4. doi: 10.4103/0970-0218.112441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pathak SM, Jindal AK, Verma AK, Mahen A. An epidemiological study of road traffic accident cases admitted in a tertiary care hospital. Med J Armed Forces India. 2014;70:32–5. doi: 10.1016/j.mjafi.2013.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mishra B, Sinha Mishra ND, Sukhla S, Sinha A. Epidemiological study of road traffic accident cases from Western Nepal. Indian J Community Med. 2010;35:115–21. doi: 10.4103/0970-0218.62568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tripathi M, Tewari MK, Mukherjee KK, Mathuriya SN. Profile of patients with head injury among vehicular accidents: An experience from a tertiary care centre of India. Neurol India. 2014;62:610–7. doi: 10.4103/0028-3886.149382. [DOI] [PubMed] [Google Scholar]
- 16.Singh RK, Gupta K, Kumar A, Singh GK, Singh A, Kumar S. Elucidation of risk factors in survivors of road traffic accidents in North India. Trauma Orthop Hard Tissue. 2013;2:1–6. [Google Scholar]
- 17.Pathak A, Desania NL, Verma R. Profile of road traffic accidents and head injury in Jaipur (Rajasthan) J Indian Acad Forensic Med. 2008;30:6–9. [Google Scholar]
- 18.Patil SS, Kakade R, Durgawale P, Kakade S. Pattern of road traffic injuries: A study from Western Maharashtra. Indian J Community Med. 2008;33:56–7. doi: 10.4103/0970-0218.39248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Swaddiwudhipong W, Nguntra P, Mahasakpan P, Koonchote S, Tantriratna G. Epidemiologic characteristics of drivers, vehicles, pedestrians and road environments involved in road traffic injuries in rural Thailand. Southeast Asian J Trop Med Public Health. 1994;25:37–44. [PubMed] [Google Scholar]
- 20.Jha N, Srivastava DK, Roy G, Jagdish S. Epidemiological study of road traffic accident cases: A study from South India. Indian J Community Med. 2004;29:20–4. [Google Scholar]
- 21.Shah A, Jarwani B. Study of patients of road traffic accidents arriving in emergency department (ED) of V.S hospital at Ahmadabad city, single centre pilot study. NHL J Med Sci. 2014;3:23–6. [Google Scholar]
- 22.Bayan P, Bhawalkar JS, Jadhav SL, Banerjee A. Profile of non-fatal injuries due to road traffic accidents from a industrial town in India. Int J Crit Illn Inj Sci. 2013;3:8–11. doi: 10.4103/2229-5151.109409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Thomas V, Sridhar L. Epidemiologic profile of road traffic accident cases admitted in a tertiary care hospital – A retrospective study in Hyderabad, Andhra Pradesh. Int J Med Pharm Sci. 2013;3:30–6. [Google Scholar]
- 24.Ansari S, Akhdar F, Mandoorah M, Moutaery K. Causes and effects of road traffic accidents in Saudi Arabia. Public Health. 2000;114:37–9. doi: 10.1038/sj.ph.1900610. [DOI] [PubMed] [Google Scholar]
- 25.Lahiri SK, Mandal P, Mandi P, Mitra SP, Chatterjee T. A study on cases contracting road traffic accidents in rural area and attending the Tarakeswar rural hospital, West Bengal. Indian J Prev Soc Med. 2005;36:94–101. [Google Scholar]
- 26.Dandona R, Mishra A. Deaths due to road traffic crashed in Hyderabad city in India: Need for strengthening surveillance. Natl Med J India. 2004;17:74–9. [PubMed] [Google Scholar]
- 27.Kiran ER, Saralaya KM, Vijaya K. A prospective study on road traffic accidents. J Punjab Acad Forensic Med Toxicol. 2004;4:12–6. [Google Scholar]