

Summary
In the neonatal period, the surgical mortality of palliation is extremely high for asplenia syndrome complicated by single ventricle combined with total anomalous pulmonary venous connection (TAPVC). Recently, stent implantation for the pulmonary venous drainage route soon after birth has been used instead of surgery to prevent pulmonary venous occlusion and to maintain stable hemodynamics in the neonatal period or in early infancy. Here, we successfully implanted stents in the ductus venosus (DV) in 2 neonates with asplenia syndrome complicated by infracardiac type TAPVC. The first patient was a 3-day-old male neonate with severe cyanosis. Immediately after TAPVC was diagnosed, we implanted a stent in the DV. The second patient was a 0-day-old female neonate. She was diagnosed as TAPVC by fetal echocardiogram. After the scheduled delivery, a stent was successfully implanted. We believe that stent implantation in the DV in the neonatal period is effective and less invasive than surgery in patients with infracardiac type TAPVC.
Keywords: Ductus venosus, Stent implantation, Asplenia syndrome, Total anomalous pulmonary venous connection, Catheter intervention
Introduction
The fate of infants with functional single ventricle such as in asplenia syndrome complicated by total anomalous pulmonary venous connection (TAPVC) is catastrophic compared to that of infants without TAPVC [1]. The current surgical mortality of isolated TAPVC is less than 10% and most patients successfully survive, while the outcome is unfavorable for patients with associated complex cardiac malformations [2]. It has been reported that an early age at initial operation, the need of palliative surgery with cardiopulmonary bypass, and an obstructed TAPVC are risk factors for mortality in these patients [1], [2]. Even though the surgical outcome has recently been improving in these patients [1], [3], [4], mortality is still high among patients with heterotaxy treated in the modern surgical era [5], and this situation continues to remain extremely challenging [6]. Patients with obstructed TAPVC, especially of the infracardiac type, usually present with critical illness. This requires alternative and aggressive management strategies, for instance, a stent implantation to maintain the pulmonary venous drainage and stable hemodynamics in the neonatal period or early infancy [2], [7].
We successfully implanted stents in the ductus venosus (DV) in 2 neonates with asplenia syndrome complicated by infracardiac type TAPVC [8]. Our novel strategy, stent implantation in the DV, may be a better alternative to early surgery for the treatment of infracardiac type TAPVC in asplenia syndrome.
Case reports
Patient 1
A 3-day-old male neonate, who was born at 39 weeks of gestation with a birth weight of 3000 g, was referred to our hospital with complaints of severe cyanosis. At admission, the SpO2 was 55%. Physical examination and echocardiogram revealed that the patient had asplenia syndrome, situs ambiguous, D-loop, D-transposition (A, D, D), single right ventricle, common atrium, pulmonary atresia, common atrioventricular canal defect, patent ductus arteriosus, infracardiac type TAPVC, right aortic arch, and bilateral superior vena cava. His cyanosis gradually improved by the administration of lipo-prostaglandin E1; however, the pulmonary congestion progressed with closing DV (Fig. 1). At 3 days of admission, cardiac catheterization and stent implantation in the DV was performed as follows. First, the umbilical vein was secured using a 6F sheath. A 6F multipurpose catheter was inserted into the portal vein through the umbilical vein. Portal venogram was used to find the exact route of the DV. Through the DV, a guide wire (0.014 in.) was carefully inserted into the common atrium. Since the DV had already started to close, it was difficult to pass the guide wire through the DV. Keeping the guide wire in the common atrium, a stent mounted on the balloon catheter was introduced over the guide wire and the stent was located in the DV. We successfully implanted the stents (GFX Micro-stents, 1 piece of diameter 3 mm and length 24 mm, and 2 pieces of diameter 3 mm and length 18 mm) in the DV from the atrium to the portal vein (Fig. 2). We confirmed that the flow through the DV was adequate by both angiogram and echocardiogram. Biphasic flow pattern was detected in the stent by a Doppler echocardiogram. Chest X-ray revealed that pulmonary congestion had disappeared. After the procedure, heparin (100 U/(kg day), intravenously) and aspirin (5 mg/(kg day), orally) were administered. Pulmonary venous return was not obstructive and the clinical course after the stent implantation was good. At the age of 8 days, Blalock-Taussig shunt was created successfully and lipo-prostaglandin E1 could be discontinued. One month after the stent implantation, SpO2 gradually decreased owing to restenosis of the DV. We performed redilation of the stent with a 5 mm balloon catheter. As the umbilical vein had already closed at that time, we retrogradely approached the DV from the right jugular vein through the common atrium. The SpO2 improved from 65% to 82%. At the age of 4 months, TAPVC repair was performed.
Figure 1.
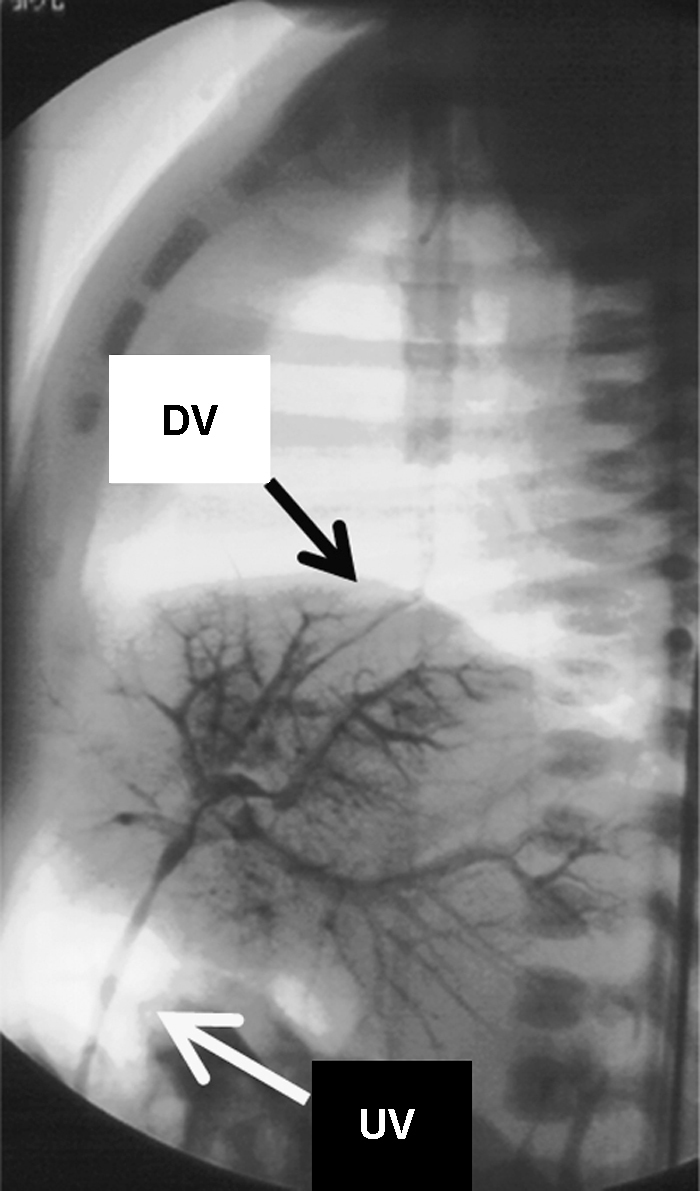
Portal venogram (patient 1). Portal venogram through the umbilical vein shows the course of the ductus venosus (DV). The DV had already started to close. UV, umbilical vein.
Figure 2.
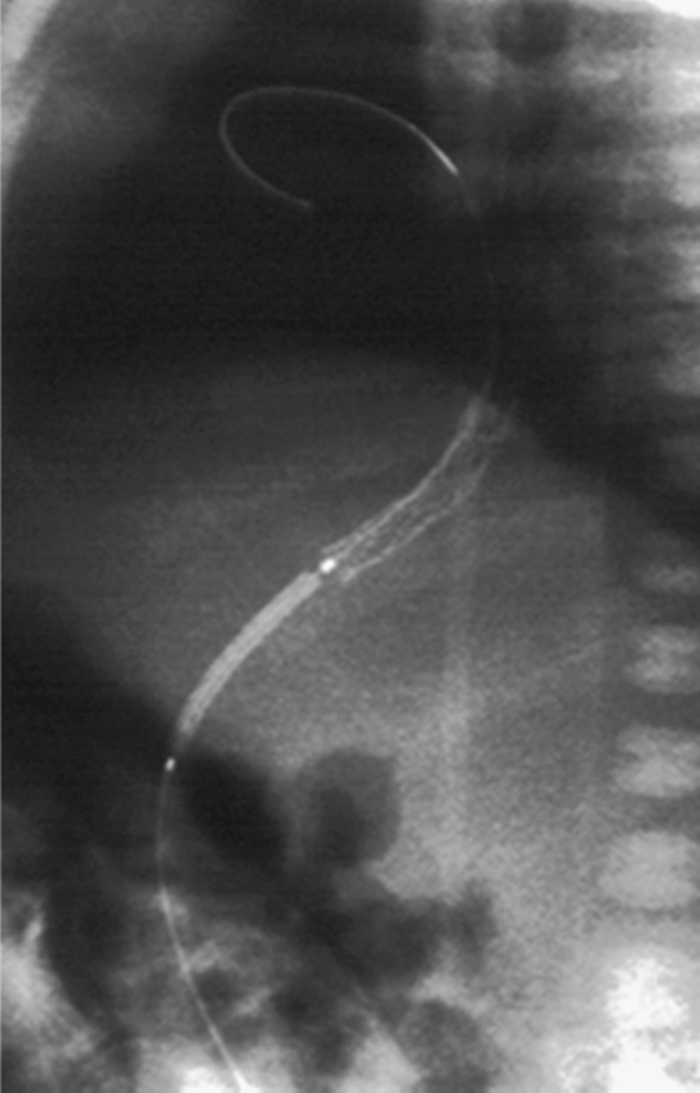
Stent implantation (patient 1). We successfully implanted the stents (GFX Micro-stents, 1 piece of diameter 3 mm and length 24 mm, and 2 pieces of diameter 3 mm and length 18 mm) retrogradely in the ductus venosus from the atrium to the portal vein.
Patient 2
A female neonate was born at 38 weeks of gestation with a birth weight of 2580 g by scheduled Cesarean section. The patient was diagnosed with asplenia syndrome (A, D, D), single right ventricle, common atrium, pulmonary atresia, common atrioventricular canal, patent ductus arteriosus, infracardiac type TAPVC, and bilateral superior vena cava according to the fetal echocardiogram. We successfully performed a stent implantation in the DV after birth. As described for Patient 1, we implanted the stents (Palmaz stent 2408 of diameter 8 mm and length 24 mm) in the DV. A stent with a larger diameter was selected since the first case demonstrated the importance of using a larger stent to maintain an optimal flow for a long period. A sufficient flow through the DV was maintained and redilation of the stent was not required (Fig. 3). At the age of 3 months, TAPVC repair, right ventricle-pulmonary artery shunt, and pulmonary artery angioplasty were performed.
Figure 3.
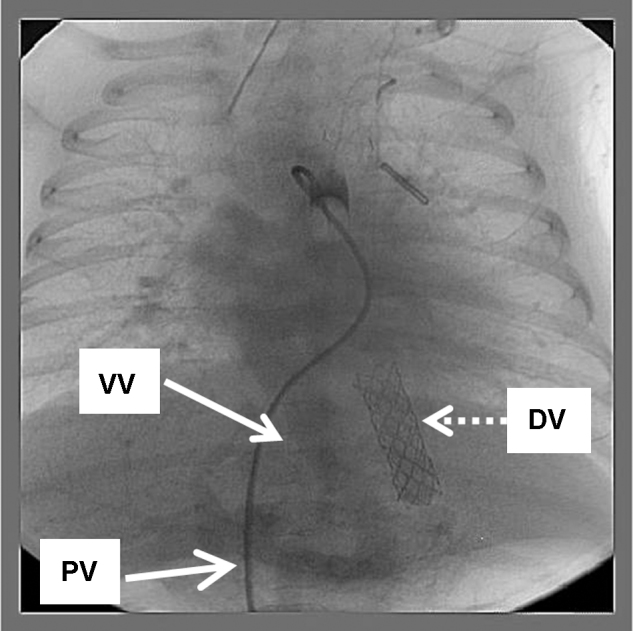
The late phase of the balloon-occlusion descending aortogram showing the pulmonary venous return root (patient 2). The projected contrast media enters bilateral lung via pulmonary arteries through the patent ductus arteriosus and then flows back into the pulmonary veins, the VV and finally the DV where the stent (Palmaz stent 2408 of diameter 8 mm and length 24 mm) was implanted. The sufficient pulmonary venous return flows inside the stent. VV, vertical vein; DV, ductus venosus; PV, portal vein.
Discussion
This is the first report of successful stent implantation in the DV in 2 newborns with asplenia syndrome with infracardiac type TAPVC in order to prevent pulmonary venous occlusion and maintain an adequate flow from the pulmonary vein into the atrium.
In asplenia syndrome complicated by infracardiac type TAPVC, pulmonary congestion progresses rapidly after the closure of the DV. The mortality rate of the palliative surgery is extremely high for TAPVC in the neonatal period. As a result, the prognosis of asplenia syndrome with infracardiac type TAPVC remains poor [1], [3], [4]. Therefore, an alternative method is required in order to treat TAPVC in the neonatal period. Catheter intervention is one of the most important treatments in complex heart diseases [7], [9]. Our novel strategy, stent implantation in the DV, is effective and less invasive than early surgery.
Since the DV closes quickly after birth, stent implantation in the DV becomes very difficult as the infant grows older. Consequently, this condition has to be diagnosed immediately and our procedure should be performed as soon as possible before the closure of the DV. For better results, intrauterine diagnosis by fetal echocardiogram should be performed, followed by pre-mediated delivery and subsequent stent implantation.
In the first patient, the restenosis of the DV caused by intimal proliferation occurred 1 month after the procedure, and redilation of the stent up to 5 mm in size was eventually required. In our experience, the appropriate size of the stent was at least 8 mm for these neonates; the best size of the stent for longer patency should be investigated in the future.
Most importantly, stent implantation in the DV soon after birth could delay the requirement for surgery with cardiopulmonary bypass in the neonatal period. Myocardial ischemia following cardiopulmonary bypass may cause deleterious cardiac dysfunction in neonates after surgery. These adverse effects may lead to high mortality after cardiac surgery in these patients. Our strategy is less invasive and is intended to improve the prognosis of patients with asplenia syndrome with infracardiac type TAPVC.
In conclusion, stent implantation in the DV soon after birth is an effective and less invasive therapy for neonates with complex congenital heart disease, particularly with infracardiac type TAPVC.
References
- 1.Lodge A.J., Rychik J., Nicolson S.C., Ittenbach R.F., Spray T.L., Gaynor J.W. Improving outcomes in functional single ventricle and total anomalous pulmonary venous connection. Ann Thorac Surg. 2004;78:1688–1695. doi: 10.1016/j.athoracsur.2004.04.057. [DOI] [PubMed] [Google Scholar]
- 2.Emmel M., Sreeram N. Total anomalous pulmonary vein connection: diagnosis, management, and outcome. Curr Treat Options Cardiovasc Med. 2004;6:423–429. doi: 10.1007/s11936-004-0026-3. [DOI] [PubMed] [Google Scholar]
- 3.Morales D.L., Braud B.E., Booth J.H., Graves D.E., Heinle J.S., McKenzie E.D., Fraser C.D., Jr. Heterotaxy patients with total anomalous pulmonary venous return: improving surgical results. Ann Thorac Surg. 2006;82:1621–1627. doi: 10.1016/j.athoracsur.2006.05.053. [DOI] [PubMed] [Google Scholar]
- 4.Nakata T., Fujimoto Y., Hirose K., Sakamoto K. Right atrial isomerism with infracardiac total anomalous pulmonary venous connection complicated by hiatal hernia. Eur J Cardiothorac Surg. 2008;34:460–462. doi: 10.1016/j.ejcts.2008.04.025. [DOI] [PubMed] [Google Scholar]
- 5.Foerster S.R., Gauvreau K., McElhinney D.B., Geva T. Importance of totally anomalous pulmonary venous connection and postoperative pulmonary vein stenosis in outcomes of heterotaxy syndrome. Pediatr Cardiol. 2008;29:536–544. doi: 10.1007/s00246-007-9128-5. [DOI] [PubMed] [Google Scholar]
- 6.Kanter K.R. Surgical repair of total anomalous pulmonary venous connection. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2006;9:40–44. doi: 10.1053/j.pcsu.2006.02.015. [DOI] [PubMed] [Google Scholar]
- 7.Kyser J.P., Bengur A.R., Siwik E.S. Preoperative palliation of newborn obstructed total anomalous pulmonary venous connection by endovascular stent placement. Catheter Cardiovasc Interv. 2006;67:473–476. doi: 10.1002/ccd.20478. [DOI] [PubMed] [Google Scholar]
- 8.Higaki T., Yamamoto E., Nakano T., Takata H., Ota M., Nagatani K., Murakami Y., Takeuchi E., Matsuda O., Terada K., Goto S., Miyazaki M., Kida K. Stent implantation for ductus venosus of Asplenia syndrome with infracardiac type of total anomalous pulmonary venous connection. Cardiol Young. 2001;11(suppl. 1):254. [Google Scholar]
- 9.Kobayashi T., Tomita H., Yokozawa M., Takamuro M., Hatakeyama K., Kim S.-H., Ono Y., Sakamoto K. Genesis stent implantation without using a long sheath in two children. J Cardiol. 2008;52:296–299. doi: 10.1016/j.jjcc.2008.06.002. [DOI] [PubMed] [Google Scholar]