

Abstract
Background:
Food poisoning (FP) commonly occurs because of consuming contaminated food, which can be fatal. Many people are not aware of the dangers of FP. Thus, the purpose of this study is to analyze the knowledge, attitude, and practice (KAP) of FP among dietetic students (DS) and food handlers (FH) in a public university in Malaysia.
Materials and Methods:
A cross-sectional study was designed, and a self-administered questionnaire was distributed to 106 respondents. The survey comprised four sections including sociodemographic, knowledge, attitude, and practice.
Results:
Total percentage scores for KAP for FH were 86.06%, 32.40%, and 19.91%, respectively, whereas the KAP scores for DS were 89.36%, 34.26%, and 19.94%, respectively. This study revealed that the respondents had good knowledge but poor attitude and practice toward FP. Total mean percentage of KAP scores for DS was higher than FH. Besides, no significant difference was observed in KAP toward FP across different genders, age, education, and income levels among FH. However, for DS, significant difference (p = 0.008) was observed in knowledge toward FP between genders. Significant association (p = 0.048) was also reported in practice toward FP with age among DS. This study also found a significant association between knowledge and attitude (p = 0.032) and knowledge and practice (p = 0.017) toward FP among FH.
Conclusion:
Nevertheless, among DS, no significant association was observed between knowledge, attitude and practice toward FP. The findings may help them to plan effective methods to promote better understanding about FP and improving their knowledge and awareness.
KEYWORDS: Knowledge and practice, food poisoning, dietetic students, food handlers
INTRODUCTION
Food poisoning (FP) refers to a group of illnesses that result from the ingestion of contaminated food that contains infectious organisms.[1] FP is defined as “illnesses caused by bacteria or other toxins in food, typically with vomiting and diarrhea.”[2] It was estimated that 76 million illnesses because of foodborne diseases resulted in 325,000 hospitalizations and 5,000 deaths each year in the USA.[3] Similarly, 1.3 million cases of foodborne illnesses, 21,000 hospitalizations, and 500 deaths were reported in England and Wales yearly.[4] The incidence of foodborne diseases was reported as 47.79 per 100,000 population in Malaysia in 2009, but had 32% increase in 2010, which is after only one year lapse.[5] Three deaths had been reported in Malaysia after consuming food served at a wedding ceremony in 2013.[6] Multiple causes are reported that lead to FP of which the most important is incorrect food safety practices. Most cases of FP were due to poor hygiene practices and usually occur in the school canteens, hostel kitchens, restaurants, and stall markets.[7]
This study was explicitly conducted among food handlers (FH) and dietetic students (DS) in a public university in Malaysia. The main reason for choosing these two groups was that DS were supposed to be more aware toward FP as they learnt about food safety and nutritional facts, whereas FH should also be mindful regarding this issue. This study also aims to find out the association between sociodemographic data with knowledge, attitude, and practice (KAP) toward FP among DS and FH.
MATERIALS AND METHODS
Study area: This study was carried out in a public university in Malaysia.
Sampling population: This survey involved DS from Year I to IV and FH from the cafeterias in the university campus.
Study design: A cross-sectional study was designed and carried out, which involved the distribution of self-administered questionnaire to DS and FH in the university campus.
Study period: Data were collected from February 17, 2016, to February 26, 2016.
Sampling method
The study respondents were selected by quota sampling where convenient sampling was carried in the groups of DS and FH.
Inclusion criteria
Volunteered to participate in this study
Understood either English or Malay as the questionnaires provided were in these two languages
Aged 18 years or above
Sample size: The sample size (n) was 106, calculated using the single proportion formula [n = (Zα/2/Δ)2 p (1 – p)] using Zα/2 = 1.96 for 95% confidence interval, p = 0.50 as proportion in population,[8] and precision, Δ = 0.10, with the addition of 10% nonresponse rate.
Data collection
The survey was conducted by distributing the self-administered questionnaire to the respondents. Before that, detail briefing was given to them so that they understood the purpose of this study. The data were collected among DS and FH in the public university. The questionnaire contained four sections, section A, B, C, and D, which were sociodemographic, knowledge, attitude, and practice toward FP, respectively. Each section consisted of 15 questions. Section A was designed to determine the sociodemographic information of the respondents, which included age, level of education, sex, and income. Section B contained two parts, the answer choices for part 1 were “yes,” “no,” and “I do not know,” whereas for part 2, they were “true,” “false,” and “not sure.” For section C, “strongly agree” to “strongly disagree” (Likert scale) were the answer choices for attitude, whereas for section D, “never” to “always” were the answer choices. In this questionnaire, the respondents needed to tick the appropriate answer choices. All items were modified from previous studies.[7,8] The questionnaire was validated through two approaches, which were content validity and face validity. The content validity of the questionnaire was validated by experts in this field, whereas face validity was conducted through a pilot study.
Scoring system
The scoring system for KAP toward FP is shown in Table 1, whereas the grading of the total scores for the levels of KAP is shown in Table 2.
Table 1.
Scoring system for knowledge, attitude, and practice
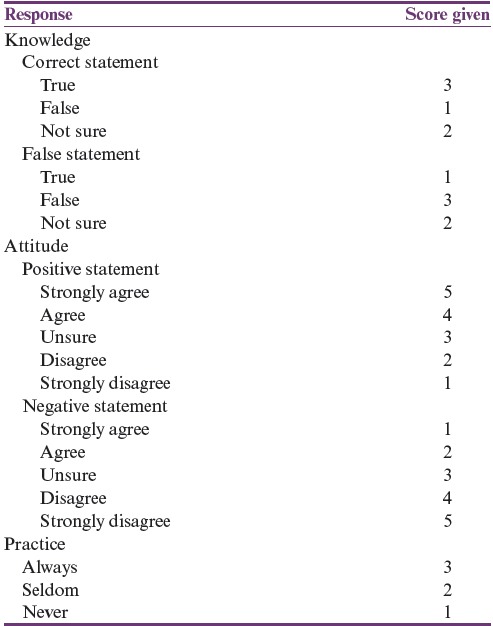
Table 2.
Grading of the total scores for the level of knowledge, attitude, and practice toward food poisoning

Data analysis
Data collected from the questionnaires were analyzed using the SPSS (Statistical Package for Social Scieces) 21, IBM, Armonk, NY, United States of America. Comparison of mean total scores of KAP between two independent groups was analyzed using independent t-test, whereas analysis of variance (ANOVA) was used for the comparison between more than two independent groups after checking for the relevant assumptions of the tests. Association between numerical variables was analyzed using Pearson correlation where the assumptions were satisfied, or otherwise Spearman correlation test was used.
Ethical approval
The study approval was obtained from the university’s postgraduate and research committee (Memo No. IIUM/310/G/13/4/4–179, February 1, 2016). Each respondent’s personal information was confidential, and study participation was voluntary. The study population was informed about the objectives and processes of the study where the data gathered would be anonymized, including for publication. Written consent was then obtained before the questionnaires were distributed.
RESULTS
Sociodemographic characteristic of the respondents
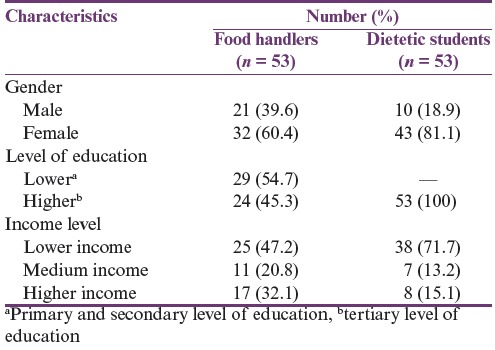
In this KAP study, 106 respondents participated involving FH (n = 53) and DS (n = 53). The sociodemographic characteristics include age, gender, occupation, and level of education and income. Female respondents were more than male respondents for both the groups [Table 3]. The respondents’ age involved in this study was 18–51 years, and the mean age was 27.14 (standard deviation [SD] = 7.21) years. The details of sociodemographic data are shown in Table 3.
Table 3.
Sociodemographic data of the respondents (n = 106)
Scores for knowledge, attitude, and practice toward food poisoning
The total percentage scores for KAP for FH were 86.06%, 32.40%, and 19.91%, respectively, whereas the KAP scores for DS were 89.36%, 34.26%, and 19.94%, respectively. According to the classifications in Table 2, the respondents had good knowledge but poor attitude and practice toward FP. Generally, the total KAP percentage score for FH was lower than that for DS.
Knowledge toward food poisoning
Most of the respondents (FH = 98.1%, DS = 100%) had heard about FP. Again, most of the respondents (89.6%) knew that FP can lead to death. In addition, 77.4% (41) and 90.6% (48) of FH and DS, respectively, knew the causes of FP. The correct answers for the causes of FP are Salmonella, Staphylococcus aureus, and Listeria spp. In this part, 52.8% of FH and 98.1% of DS identified Salmonella as the cause of FP. Both groups showed positive answers in identifying raw egg (FH = 52.8%, DS = 94.3%), raw milk (FH = 62.3%, DS = 77.4%), and sushi (FH = 30.2%, DS = 62.3%) as the causes of FP. Unfortunately, more than one-third of FH opined that sushi could not cause FP. A total of 58.5% and 98.1% of FH and DS, respectively, answered correctly as Escherichia coli to be associated with FP with raw and undercooked meat. The respondents also identified Campylobacter (FH = 50.9%, DS = 47.2%) as the cause of FP with raw or undercooked poultry. For the next statement, respondents needed to choose the correct symptoms of FP, which were vomiting, diarrhea, and abdominal cramp. All DS and more than 90% of FH answered correctly regarding the symptoms of vomiting and diarrhea for FP, whereas, regarding abdominal cramp, only 88.7% of FH and 79.2% of DS answered correctly. Approximately half of the respondents knew that the slices of honeydew, baked potato, leftover turkey, and chocolate cake kept overnight on the counter and eaten as it is can cause FP. The last question regarding the suitable temperature (74°C) of heating of leftover food was answered precisely by 37.7% and 50.9% of FH and DS, respectively.
Attitude toward food poisoning
Among the respondents, 52.8% FH and 79.3% DS “disagree” to drink raw milk rather than pasteurized milk. In addition, only 30.2% FH and 11.3% DS “disagree” that it is safe to eat fresh raw milk and cheese. On the other hand, 86.8% FH and 92.5% DS “agree” with the statement that they prefer cutting their nails regularly because long nails could contaminate food. Approximately 77.4% of both groups “agree” that wearing gloves is important during the preparation of food. Next, 51% FH and 83% DS respondents “disagree” that half-cooked meat is safe to be eaten. Only 15.1% (8) but 90.5% (48) of FH and DS, respectively, “disagree” that drinking milk from a dented can is safe. Meanwhile, 84.9% (45) and 90.6% (48) of FH and DS, respectively, “disagree” to eating in unclean cafeteria. On next question, 45.3% (24) and 71.7% (38) of FH and DS “agree” that all of us can be a source of FP. Finally, 34% (18) and 66% (35) of FH and DS “disagree” that wiping off the cutting board with a clean paper towel is enough to prevent the spreading of foodborne pathogens.
Practice toward prevention of food poisoning
Among the respondents, 67.9% (36) and 81.1% (43) of FH and DS, respectively, always checked the expiry date before buying foods, whereas 67.9% (36) and 79.2% (42) of FH and DS, respectively, always washed the cutting board before use. On the other hand, 86.8% (46) and 52.8% (28) of FH and DS, respectively, always washed their hands with water and soap after using the toilet. Subsequently, 24.5% (13) and 15.1% (8) of FH and DS, respectively, never kept cooked meat or chicken for more than 4 h at room temperature. Again, 60.4% (32) and 5.7% (3) of FH and DS, respectively, never allow their fingernails to grow long. Finally, 88.7% (47) and 90.6% (48) of FH and DS, respectively, always practiced washing fresh vegetables or fruits before eating.
Association of sociodemographic characteristics with knowledge, attitude, and practice toward food poisoning
Comparing knowledge, attitude, and practice toward food poisoning between food handlers and dietetic students
Figure 1 shows the comparison of mean total scores of KAP toward FP among FH and DS in the study. DS showed significantly higher mean total percentage score in knowledge (p = 0.004) and attitude (p = 0.010) as compared to FH, but the difference was not significant for practice scores.
Figure 1.
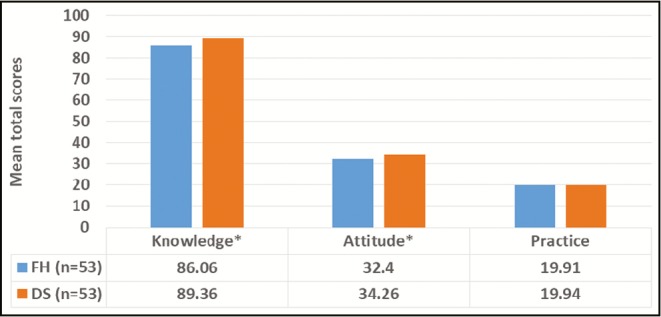
Comparing mean total scores of knowledge, attitude, and practice toward food poisoning between food handlers (FH) and dietetic students (DS). *Significant difference using independent t-test (p-values of knowledge = 0.004 and attitude = 0.010)
Factors associated with knowledge, attitude, and practice toward food poisoning among food handlers and dietetic students
As shown in Table 4, no significant association was observed between the total scores of KAP toward FP with age among FH and DS, except for between practice and age among DS (r = −0.276; p = 0.048). The result indicates negative, fair, or little correlation between the variables, meaning the total scores of practice toward FP was lower with older age of DS. On the other hand, comparisons of KAP total scores between different genders, levels of education, and income among FH and DS are shown in Figures 2–4, respectively, with no significant difference found except for the comparison of knowledge between male and female among DS (p = 0.008) with male DS showing higher scores as compared to female DS.
Table 4.
Correlation between total scores of knowledge, attitude, and practice toward food poisoning with age among food handlers and dietetic students

Figure 2.
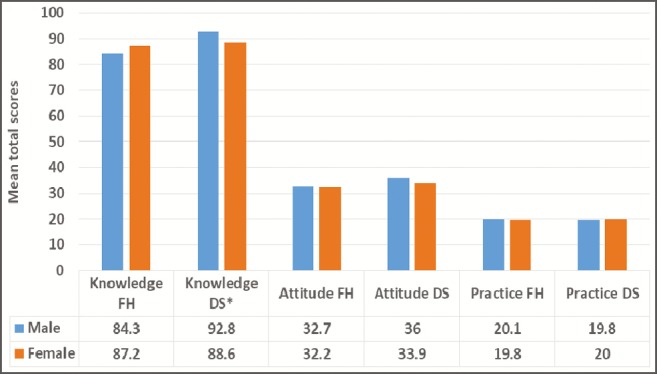
Comparing mean total scores of knowledge, attitude, and practice toward food poisoning between different genders among food handlers (FH), n (male) = 21; n (female) =32 and dietetic students (DS), n (male) = 10; n (female) = 43. *Significant difference using independent t-test (p = 0.008)
Figure 4.
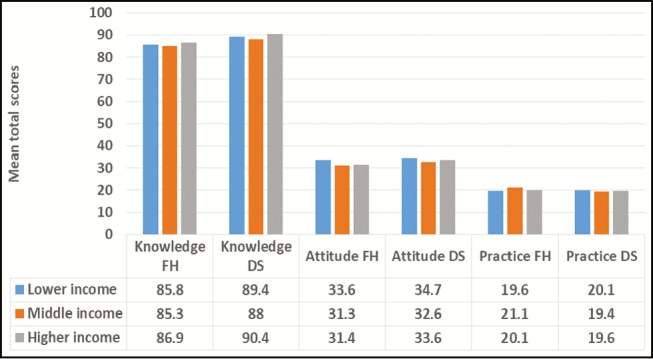
Comparing mean total scores of knowledge, attitude, and practice toward food poisoning between different levels of education among food handlers (FH), n (male) = 21; n (female) = 32. Analysis of variance (ANOVA) test carried out found no significant difference for any of the variables
Figure 3.
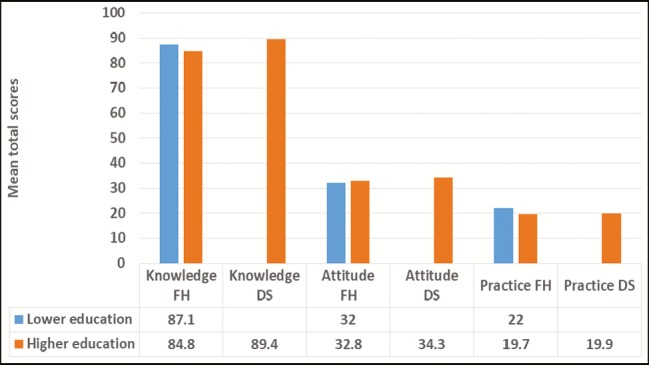
Comparing mean total scores of knowledge, attitude, and practice toward food poisoning between different levels of education among food handlers (FH), n (male) = 21; n (female) = 32. Comparison cannot be made between levels of education among dietetic students (DS), n = 53, because all of them came from the same level of higher education. Independent t-test performed found no significant difference for any of the variables
Correlation between knowledge, attitude, and practice toward food poisoning
A significant association (r = −0.296, p = 0.032) was observed between knowledge and attitude toward FP among FH, also between knowledge and practice (r = 0.326, p = 0.017) [Table 5]. However, no significant association was observed between attitude and practice among FH, neither was any significant association detected between knowledge, attitude, and practice among DS [Table 5].
Table 5.
Association between total scores of knowledge, attitude, and practice toward food poisoning using Pearson correlation test among food handlers and dietetic students

DISCUSSION
According to the World Health Organization, 700,000 Asians die each year because of FP.[10] Hence, it is essential to possess good KAP toward the illness. The respondents in this study had good knowledge but poor attitude and practice toward FP. The total mean KAP score for DS was higher than that for FH.
Sociodemographic characteristics of respondents
A total number of 106 respondents were involved in this study, which consisted of 53 DS and 53 FH. In this study, female respondents outnumbered male respondents. The possible explanation could be that female respondents were more interested toward the dietetic field and worked in the kitchen as FH. The mean age was 27.14 (SD = 7.21) years. In terms of income, most of DS fall in low-income category. Students’ scholarship amount was considered in that category.
Knowledge toward food poisoning
The mean percentage knowledge score for DS is higher than that for FH. This correlates with correct answers given by most of DS regarding knowledge about FP. Among the three components, knowledge had the highest percentage score. DS had higher knowledge regarding FP as compared to FH. Both groups were aware that FP could lead to death. Majority of DS knew the cause of FP but more than half of FH were not sure. One study revealed that health science discipline scored higher in food safety knowledge.[11] DS scored higher because they studied about food safety education.[12] In addition, both groups answered sushi could cause FP. It has been reported that sushi can promote FP and hepatitis B.[13] Thus, ensuring the cleanliness and food safety in common dining places in students’ hostels, in cafe and restaurants should be considered as an important public health action.[14]
The most common pathogens involved in FP are Staphylococcus aureus, Escherichia coli, Salmonella, Listeria spp., Campylobacter, and Clostridium perfringens.[15] DS had better knowledge regarding this as compared to FH as more than 50% of DS answered correctly. However, more than 18% of both categories of respondents were unsure regarding Legionella, which is consistent to an earlier study.[16] Legionella is a microorganism, which is actually often responsible for severe pneumonia.[17] Nevertheless, many of the respondents managed to answer correctly regarding the symptoms of FP, and this is consistent with an earlier finding.[15] Leftover food should be heated to 74°C to prevent FP. DS scored higher on this matter as 50.9% of them answered correctly, whereas in FH, only 37.7% answered correctly. Moreover, according to the Malaysian Ministry of Health, leftover food should be reheated at least at 74°C to prevent FP.[5] On the other hand, a previous study reported that FH had a high score in knowledge regarding food temperature control.[18] This study findings were similar to an earlier study in Turkey where FH had a low score in food temperature control.[19]
Attitude toward food poisoning
Although the mean percentage attitude scores of DS were higher than FH, the scores indicated that the respondents of both categories had poor attitude toward FP. This finding is similar to a previous study where the mean percentage of attitude scores were poor.[8] However, both groups “disagree” to drink raw milk rather than pasteurized milk, though this result is not supported by another previous study, which mentioned that the farmer believed that the raw milk is healthier than pasteurized milk.[20]
It has been reported that most of FH gave the correct statement that the consumption of raw milk and cheese could increase the risk of FP.[21] Nevertheless, more than half of DS in this study opined that eating raw milk and cheese is safe. This result is similar to another study, which similarly reported that eating raw milk and cheese is safe.[8] Furthermore, the majority of FH showed a negative attitude toward hygienic statement as compared to DS. This finding was supported by earlier research findings, which reported that more than 50% of FH showed negative attitude in terms of hygiene.[22] This study also found that FH showed a negative attitude toward the prevention of FP as majority “agree” that washing hand with water only to prevent FP as opposed to washing hand with water and soap. It has been advocated that proper hand washing is essential especially among retail FH to ensure a good standard of food safety and to avoid FP.[23,24,25] Besides, most DS opined that drinking from a dented can is harmful, whereas only a minor portion of FH agreed with the earlier notion. This denotes that FH has a negative attitude in preventing FP. This is one of the important facts that FH need to know as they prepare food and drinks for the customer. Drinking from a dented container can lead to a considerable dangerous health hazard.[26]
Practice toward prevention of food poisoning
It can be considered from the mean percentage practice score that both groups had a poor practice of food hygiene. However, an earlier study revealed that FH showed a positive attitude, which was different from this study.[18] A few other studies also revealed that FH had a high mean score in hygiene practice and achieved an acceptable level.[27,28] However, an overseas study found that FH showed poor practice of strict food hygiene strategies toward prevention of FP.[29] On the other hand, it has been reported that food exposed at room temperature for 4 h or more are not safe to be eaten.[30]
Association between sociodemographic factors with knowledge, attitude, and practice toward food poisoning
In terms of knowledge toward FP, DS scored significantly higher than FH. This could be because DS had a higher education level as compared to FH. This statement is supported by earlier research findings mentioning that those who have high education level tend to have a high mean score in knowledge.[17] This study also found a significant difference in terms of knowledge toward FP between male and female respondents among DS. The finding denotes that male respondents have higher knowledge level regarding FP as compared to female respondents. This result was different and opposite to another study, which revealed that female students have a high mean score in terms of knowledge.[11] Furthermore, this study also revealed a significant difference of total attitude toward FP between FH and DS, besides a significant association between the total scores of practice and age among DS. A study found no significant relationship between gender and practice toward FP among FH, which is similar to the findings in this study.[22]
Correlation between knowledge, attitude, and practice toward food poisoning
The results obtained showed a negative correlation between knowledge and attitude among FH. FH in this study showed high scores in knowledge but tend to have negative attitude toward FP. However, a previous study reported a positive correlation between knowledge and attitude among FH.[31] It has been mentioned that knowledge helps to improve attitude.[32]
Also, negative correlation was observed between knowledge and practice among DS and attitude and practice among both respondent groups, but the correlation was not statistically significant. These findings were similar to a previous research report, which found negative correlation between attitude and practice among FH.[31] Another study revealed that having good knowledge and attitude will lead to good practice measures among FH.[22] However, the results of this study revealed that having good knowledge and attitude does not lead to good practice as reported in a Turkish study.[19]
Also, a significant association was observed between knowledge and practice toward FP among FH. The r value showed little positive correlation, which means that knowledge leads to positive practice. Nevertheless, another research revealed a negative correlation between knowledge and practice among FH.[31] However, in this study, a negative correlation was observed between total knowledge and practice among DS, though it was not statistically significant. Finally, no significant association was reported between practice and attitude of FP for both groups. This is a cross-sectional study with its inherent limitation. Moreover, it is a single-center research with limited study because of financial and time constraints.
CONCLUSION
In conclusion, this study shows that FH and DS had good knowledge but poor attitude and practice, though the total mean percentage score of KAP for DS was higher than that for FH. Besides, no significant difference was observed in KAP toward FP across different genders, age, education, and income levels among FH. However, DS possess significant differences in knowledge toward FP between genders. Also, a significant association was observed between practices toward FP with age among DS. This study also found a significant association between knowledge and attitude and knowledge and practice regarding FP among FH. Nevertheless, among DS, no significant association was observed between knowledge, attitude, and practice toward FP.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Al-Mazrou YY. Food poisoning in Saudi Arabia. Potential for prevention? Saudi Med J. 2004;25:11–4. [PubMed] [Google Scholar]
- 2.Hormny AS. Oxford advance learner's dictionary of current English. 7th ed. New York: Oxford University Press; 2007. [Google Scholar]
- 3.Mead PS, Slutsker L, Dietz V, McCaig LF, Bresee JS, Shapiro C, et al. Food-related illness and death in the United States. Emerg Infect Dis. 1999;5:607–25. doi: 10.3201/eid0505.990502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Adak GK, Long SM, O’Brien SJ. Trends in indigenous foodborne disease and deaths, England and Wales: 1992 to 2000. Gut. 2002;51:832–41. doi: 10.1136/gut.51.6.832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ministry of Health. Annual Reports. Planning division health informatics center, Ministry of Health, Malaysia. 2014. [Last accessed on 2015 Nov 12]. Available from: http://www.health.gov.bt/publications/annualreports/
- 6.Ramli S, Rattanachot O, Sahir SFM, Osman AR. Tiga Maut Keracunan Makanan, Utusan Malaysia. 2013. [Last accessed on 2018 Oct 9]. Available from: http://www.utusan.com.my/utusan/Jenayah/20131001/je_01/Tiga-maut-keracunanmakanan .
- 7.Norazmir MN, Norazlanshah H, Naqieyah N, Anuar MIK. Understanding and use of food package nutrition label among educated young adults. Food Control. 2012;11:934–40. [Google Scholar]
- 8.Sharif L, Al-Malki T. Knowledge, attitude and practice of Taif University students on food poisoning. Food Control. 2010;21:55–60. [Google Scholar]
- 9.Tikuye A. South Africa: University of South Africa; 2013. [Last accessed on 2018 Oct 9]. Knowledge, attitude, and practices of health care providers towards isoniazide preventive therapy (IPT) provision in Addis Ababa, Ethiopia [dissertation] Available from: http://uir.unisa.ac.za/bitstream/handle/10500/11916/dissertation_tikuye_am.pdf;sequence=1 . [Google Scholar]
- 10.World Health Organization. Food safety: resolution of the executive board of the WHO, 105th Session, EB105. R16 28, Agenda item 3.1. 2000. [Last accessed on 2018 July 16]. Available from: http://apps.who.int/gb/archive/pdf_files/EB105/eer16.pdf .
- 11.Unklesbay N, Sneed J, Toma R. College students’ attitudes, practices, and knowledge of food safety. J Food Prot. 1998;61:1175–80. doi: 10.4315/0362-028x-61.9.1175. [DOI] [PubMed] [Google Scholar]
- 12.Scheule B. A comparison of the food safety knowledge and attitudes of hospitality and dietetic students. J Hosp Tour Educ. 2002;14:42–50. [Google Scholar]
- 13.Ng W-M. Popularization and localization of sushi in Singapore: an ethnographic survey. New Zealand J Asian Stud. 2001;3:7–19. [Google Scholar]
- 14.Kwon J, Roberts KR, Sauer K, Cole KB, Shanklin CW. Food safety risks in restaurants and school foodservice establishments: health inspection reports. [Last accessed on 2018 July 15];Food Prot Trends. 2014 34:25–35. Available from: http://www.foodprotection.org/files/food-protection-trends/Jan-Feb-14-kwon.pdf . [Google Scholar]
- 15.Sharifa Ezat WP, Netty D, Sangaran G. Paper review of factors, surveillance and burden of foodborne disease outbreak in Malaysia. Malay J Public Health Med. 2013;13:98–105. [Google Scholar]
- 16.Mitchell RE, Fraser AM, Bearon LB. Preventing food-borne illness in food service establishments: broadening the framework for intervention and research on safe food handling behaviors. Int J Environ Health Res. 2007;17:9–24. doi: 10.1080/09603120601124371. [DOI] [PubMed] [Google Scholar]
- 17.Rathore MH. Legionella infection. Drugs and diseases. Pediatrics: general medicine. 2018. [Last accessed on 2018 July 15]. Available from: https://emedicine.medscape.com/article/965492-overview .
- 18.Sharif L, Obaidat MM, Al-Dalalah MR. Food hygiene knowledge, attitudes and practices of the food handlers in the military hospitals. Food Nutr Sci. 2013;4:245–51. [Google Scholar]
- 19.Bas M, Ersun AS, Kıvanç G. The evaluation of food hygiene knowledge, attitudes, and practices of food handlers’ in food businesses in Turkey. Food Control. 2006;17:317–22. [Google Scholar]
- 20.Hegarty H, O’Sullivan MB, Buckley J, Foley-Nolan C. Continued raw milk consumption on farms: why? Commun Dis Public Health. 2002;5:151–6. [PubMed] [Google Scholar]
- 21.Osaili TM, Obeidat BA, Jamous DOA, Bawadi HA. Food safety knowledge and practices among college female students in north of Jordan. Food Control. 2011;22:269–76. [Google Scholar]
- 22.Abdul-Mutalib NA, Syafiaz AN, Sakai K, Shirai Y. An overview of foodborne illness and food safety in Malaysia. Int Food Res J. 2015;22:896–901. [Google Scholar]
- 23.qFood Standards Australia New Zealand. A guide to the food safety standards. Chapter 3. Australia New Zealand Food Standards Code. 3rd ed. 2016. [Last accessed on 2018 July 15]. Available from: http://www.foodstandards.gov.au/publications/Documents/Safe%20Food%20Australia/FSANZ%20Safe%20Food%20Australia_WEB.pdf .
- 24.Mathur P. Hand hygiene: back to the basics of infection control. Indian J Med Res. 2011;134:611–20. doi: 10.4103/0971-5916.90985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Darko S, Mills-Robertson FC, Wireko-Manu FD. Evaluation of some hotel kitchen staff on their knowledge on food safety and kitchen hygiene in the Kumasi Metropolis. Int Food Res J. 2015;22:2664–9. [Google Scholar]
- 26.Byrd-Bredbenner C, Abbot JM, Quick V. Food safety knowledge and beliefs of middle school children: implications for food safety educators. J Food Sci Educ. 2010;9:19–30. [Google Scholar]
- 27.Saad M, See TP, Adil MAM. Hygiene practices of food handlers at Malaysian government institutions training centers. Proc Soc Behav Sci. 2013;85:118–27. [Google Scholar]
- 28.Rodríguez M, Valero A, Posada-Izquierdo GD, Carrasco E, Zurera G. Evaluation of food handler practices and microbiological status of ready-to-eat foods in long-term care facilities in the Andalusia region of Spain. J Food Prot. 2011;74:1504–12. doi: 10.4315/0362-028X.JFP-10-468. [DOI] [PubMed] [Google Scholar]
- 29.Akabanda F, Hlortsi EH, Owusu-Kwarteng J. Food safety knowledge, attitudes and practices of institutional food-handlers in Ghana. BMC Public Health. 2017;17:40. doi: 10.1186/s12889-016-3986-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.United States Department of Agriculture. Food Safety and Inspection Service. Food Safety Information. How temperatures affect food. 2011. [Last accessed on 2018 July 15]. Available from: https://www.fsis.usda.gov/shared/PDF/How_Temperatures_Affect_Food.pdf .
- 31.Ansari-Lari M, Soodbakhsh S, Lakzadeh L. Knowledge, attitudes and practices of workers on food hygienic practices in meat processing plants in Fars, Iran. Food Control. 2010;21:260–3. [Google Scholar]
- 32.Acikel CH, Ogur R, Yaren H, Gocgeldi E, Ucar M, Kir T. The hygiene training of food handlers at a teaching hospital. Food Control. 2008;19:186–90. [Google Scholar]