

Abstract
ABSTRACT: Purpose: We high lightened the changes in Visual Evoked Potentials (VEP) and Brainstem Auditory Evoked Potentials (BAEP) in Multiple Sclerosis (MS). The recordings of evoked potentials were repeated at an interval of 2 months for a total of 12 months. Results: Prolonged latencies of the VEP waves (mostly P100) gas confirmed the multifocal character of MS lesions. The positive effect of corticostheroids in MS flare and the changing course of the disease following administration of interferon. The BAEP recordings have not shown reproducible modifications. Conclusions: Succesive VEP monitoring brings on valuable information by highlighting infraclinical lesions and monitoring the evolution of the disease.
Keywords: multiple sclerosis, visual evoked potentials, P100 wave
Introduction
MULTIPLE SCLEROSIS (MS) is a disease of the central nervous system with unknown causes. It is characterized by the successive apparition of diseminatind demyelinating lesions randomly in the central nervous system and has an uncharacteristical symptomatology, evolving in flairs, with sympoms that can dissapear or persist. [1, 2].
The cause of the disease is unknown, the most accepted hypothesis is a viral infections which occurs in adolescency genetically predisposed subjects, and then develops an auto-immune process linked with deficiencies of the T-supressor cells.
From epidemiological point of view MS is a disease that affects both genders, but has an increased prevalence in the female population, and affects predominantly young adults (7 out of 10 cases appear between 20-40 years).
Caucasian population has the highest prevalence of MS, while dark-skinnde population has ½ of the risk of Caucasian population, while the Asian population has very low prevalence of MS.
There is a 25% concordance in monozygotic twins.
The appartenence to the genetic haplotype HLA-DR2 significantly increase the risk of developing MS[2].
MS is characterized by the presence of demyelinating lesions (plaques) in the nervous system with the following characteristics:
-distinct boundaries
-randomly disseminated in the white matter of the peripheric nervous system after the emergence from the brainstem
-variable number of lesions
-different age of coexisting lesions
Clinical signs appear following the localization of the lesions, the most affected are the optic nerve, pyramidal patways, sensitive pathways, oculomotor muscles and the cerebellum
Several phenotypes (commonly named types), or patterns of progression, have been described:
relapsing-remitting (RRMS-the most frequent)
secondary progressive (SPMS)
primary progressive (PPMS)
progressive relapsing(PRMS)
Base diagnosis remains objectifying dissemination in time and space character inflammatory lesions .
Magnetic resonance imaging (MRI) brings decisive information about the nature and localization of the lesions, while cerebro-spinal liquid alterations are suggestive but not patognomonic.
Recording the evoked potentials especially visual evoked potentials can highlight a significant delay of latency of some well-defined waves, the value of visual evoked potentials(VEP) is higher for patients with clinical signs of MS but with no alterations on the MRI scan.
The study of evoked potentials: visual, auditive and somesthesic can be very useful in MS by highlighting an infraclinical lesion. Visual evoked potentials can be more sensible than MRI for finding lesions of the optical nerve.
In pacients with spastic diplegia, the elongation of VEP latency is present in 75% of the patients, with the signification of optical nerve damage, confirming the multifocal character of the lesions[3,4].
Dynamic recording of VEP can monitor the evolution of MS and help evaluate the effect of corticotherapy in flairs.
Material and methods
This study was part of a research start-up grant that targeted evocked potentials in diagnostic and management of same neurological diseases.
The proposed method usese evoked potentials in the diagnostic and management of MS by:
-selecting a group of patients with MS diagnosed in a neurology clinics.
-making a database for the study which includes significant clinical informations,
paraclinical(MRI) and therapeutical informations.
-recording VEP and Brainstem Auditory Evoked Potentials( BAEP) in dynamics from the patients with MS
-study of evoked potentials in patients with MS with corticotherapy in comparison with the patients without corticotherapy[4].
Patient population
The study enrolled 15 patient (12 woman) with a history of documented diagnosis of MS with a mean age of 46 years for woman and 40 years for man.
The prevalent symptomatology was with motor deficit pyramidal syndrome.
7 patients have recurrent-remisive form of MS, 2 patients have primary-progressive form and 6 with secondary-progressive form. 1 presents repartition of MS clinical forms.
Figure 1.
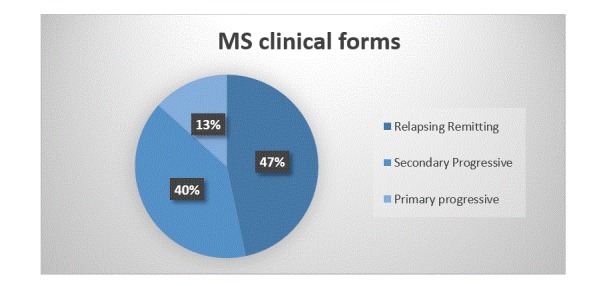
Repartition of MS clinical forms
10 patients out of 15 received treatment with corticotherapy in flares. Out of the 5 patients without corticotherapy 3 patient followed treatment with interferon.
The evoked potentials recordings were compared with those obtained from a group without neurological impairments.
The informed consent was obtained from each pacient at the screening visit.
Patient assessment:
Recording of the evoked potentials was made using a Nihon Kohden Neuropack EMG/EP Measuring System.
Visual Evoked Potentials:
-Stimulating left eye – gathering from Occipital left electrode and Occipital right electrode
-Stimulating right eye – gathering from Occipital left electrode and Occipital right electrode
Stimulation type: pattern reversal(checkboard pattern) – 200 stimuli
In monocular full-field stimulation the two occipital lobes are participating in the answer and the potentials represents the algebraic sum of generated wave activity.
Technical data:
Pattern: full-field
Dimensions: 64 cases
Display: checkboard pattern
Time on screen 100 ms
Display mode: reverse
The latencies of the waves N75, P100 and N145 are measured. The P100 wave is found constantly in normal individuals, the variability in latency is small between different individuals but amplitude variations are common.
Individual variability is small and the difference in interocular latency between the left eye and right eye does not exceed 8 miliseconds.
VEP are particularly useful in the assessment of lesions in a confirmed MS pacient and for sustaining the diagnosis criterias in incert MS diagnostics[4,5].
Chiappa affirms that if VEP are abnormal in a patient without visual impairment, they signify an infraclinical form of disease and are representantive for nerve damage in MS[5,6].
Mangiere states that in multifactorial analysis VEP are more abnormal in patients that have optical neuritis in antecedents and inflammatory signs in LCR if examined more than 6 months after the first symptoms or if the pacient has had more than 3 flares[5].
Longitudinal studies had shown that abnormalities in VEP can diminish after the clinical signs disappear, but very rarely the abnormalities disappear completely.
In the MS patients without optical nerve damage, VEP have the tendency to deteriorate, in parallel with the disese progression outside the visual pathways.
The most frequent observed anomaly is the increase in latency of the P100 wave, with the conservation of amplitude, the increase in latency can be unilateral or bilateral but most often is assymetric[7,8].
In conclusion, like all complementary examinations, VEP must be interpreted carefully, in connection with the clinical context.
Brainstem Auditory Evoked Potentials:
Stimulation method: click with 70 dB, mono-auricular stimulation, averaging 1000 evoked answers, in contralateral ear we are using masking noise.
Technical data:
Waveform: click
Output Phase: Altern
Click duration: 0.1 msec.o V-Stimulating left eye – gathering from Occipital left electrode and Occipital right electrode
Tone Frequency: 1 KHz
Results:BAEP is presented as a succession of 6 peaks numbered from I to VI and with a latency below 10 miliseconds. We are evaluating the presence or absence of the waves, the morphology of answers, the latency of the components and measure the interval between waves [9,10].
Follow-up:
All patients were followed for a year after enlisting in the study, VEP and BAEP were recorded in dynamic at an interval of roughly 2 months, in relation with the clinical evolution and treatment.
Statistical analysis were performed by using the statistic functions Anova and t-Test.
Results
VEP obtained by stimulating the left eye and right eye of each patient were stored and analyzed with a specifically designed software.
The waves N75, P100 and N145 were identified and they're latencies were measured.
BAEP obtained by stimulating the left and right ear of each patient were stored and analyzed with a specifically designed software.
The waves I, II, III, IV and V were identified and they're latencies were measured, also we measured the latencies between I-III, III-V and I-V waves.
The results of VEP and BAEP recordings were stored in the database with the records of the patients.
Analysis of VEP:
The VEP of patients with MS were compared with a group of patients without neurological impairment and of similar age. The mean latencies and standard deviations were calculated for the waves composing the VEP:
78.56 ms medium latency and 2.80 standard deviation for N75
109.31 ms medium latency and 5.19 standard deviation for P100
148.3 ms medium latency and 5.19 standard deviation for N145
From the dynamic VEP recordings of MS patients the following values of latencies were calculated:
81.16 ms medium latency and 7.12 standard deviation for N75
118.01 ms medium latency and 20.77 standard deviation for P100
180.279 ms medium latency and 18.26 standard deviation for N145
We note that the latencies of the VEP waves have significant increased latencies than in the group of normal patients[4,8,9]. High values of standard deviation show an increased variability of latencies because of recurrent remisions of the disease.Fig.2 presents VEP latencies in MS and normal subjects.
Figure 2.
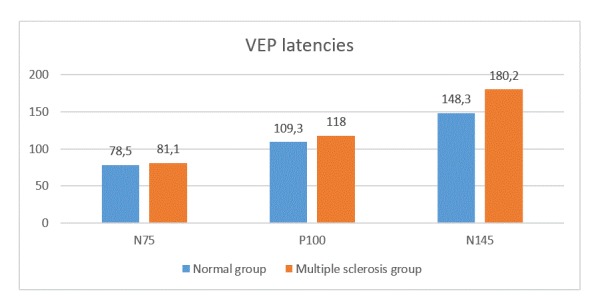
VEP latencies in MS and normal
Analysis of BAEP:
The BAEP of patients with MS were compared with a group of patients without neurological impairments and of similar age.
The following medium values of the wave latencies have been calculated:
I 1,71 ms
II 2.85 ms
III 3.97 ms
IV 5.18 ms
V 5.75 ms
Intervals between waves:
I-V 4.03 ms
I-III 2.23 ms
III-V 1.77 ms
The values of standard deviations are corresponding with those found in other major published studies. From the dynamic recordings of BAEP from MS patients similar values with those of the normal patients were calculated.
The interval between the I-III waves has a medium value in the MS patient group of 2.24 ms, while in the comparison group is 2.23 ms. The interval III-V is 1.77 ms in the MS group and also 1.77 ms in the normal group.
Discussions
VEP: Analyzing the recordings in each form of MS is done, we follow the value of the latency of P100 wave which has the most significant statistical importance.
With the Anova function, the medium values of the P100 wave were tested in patients with MS, comparing them with healthy subjects. A significant statistic difference between the medium values of the 2 groups is calculated: p=0.012
The dynamic VEP recordings have brought important information about the natural evolution of the disease, the clinical form of MS and the effect of the therapy.
In the recurrent-relapsing form the recording of VEP shows:
Without Corticotherapy:
-Moderate increases in P100 latency (maximum 110 ms) in one of the recordings (patient T.M., 38 years) which is spontaneously remitting.
In the case of the pacient U.F. we observe in the dynamic VEP recordings the increase of P100 latency 2 times which is decreasing, but not to the normal values specific of that age.
The patient D.M. has recurrent-relapsing Ms diagnose for 15 years and also has diabetes and presents P100 latencies above 130 ms bilateral, with tendencies to increase.
With Corticotherapy:
-Pacient F.C. presents an evolutive flair (with increased P100 latency) which is remitting under corticotherapy, followed recently by another flair (duration of 6 weeks) that does not improve presently, with an increase of P100 at 121.2 ms.
Patient T.M. (50 years) presents latencies of the P100 wave above 120 ms bilaterally, following an evolutive flair but does return to normal values after corticotherapy.
Patients treated with interferon:
2 patients had followed interferon therapy for 2 and a half years prior introduction in the study.
Patient M.M. (34 years) presents little variations of the P100 latency with a tendency to decreasing latency in the last 3 months.
Patient C.C. (31 years) presents a singular episode with a dramatic increase in the latency of the P100 wave (135 ms) with a 15.3 difference between the left and right eyes, followed by the returning to normal values in the next recordings.
In the secondary-progressive form of MS:
In this cathegory we find old cases of MS with high increases in latencies of the N75, P100 and N145 waves, pacient Z.L. exhibits high increases in the latencies of the N75, P100 and N145 waves, with bilateral symmetry.Patients I.D., N.I., E.M. have increased latencies of P100 with assimetry between the left and right eyes, the corticotherapy has a limited effect, motor deficiencies are present and pronounced. Pacient B.M., without corticotherapy shows a slow but irreversible increase in the latencies of P100.
Patient S.M., with interferon treatment has a temporary increase of the P100 latencies, followed-up by a recovery to normal values.
In the primary-progressive form of MS:
VEP recordings indicate that:
-Pacient B.N. has a temporary positive effect of corticotherapy, followed by a tendency to aggravation of MS, confirmed by the VEP aspect.
-Pacient B.B., with corticotherapy in antecedents does not show in the records significant changes in VEP.
BAEP latencies in MS are similar with those of the normal group. A series of alterations are present in MS patients, like the absence of some waves, alteration of the morphology of the waves, or increased latencies, but all are inconstant, inconsistent and cannot be systematised.
Conclusion
Dynamic VEP recordings have confirmed the importance of the visual evoked potentials in the diagnostic and management of MS.
The reference values of the test group without neurological impairment are similar with those of the major studies.
The latencies of VEP Waves are significantly altered in MS, the changes have confirmed the multifocal character of MS lesions. Analysis of VEP brings arguments in support of the MS diagnostic.
VEP monitoring by successive recordings brings important information of the evolution of MS, allowing a more efficient treatment.
Monitoring the VEP in dynamic can can find an alteration that emphasizes te risk og recurrence of the disease.
The biggest delays of the P100 latency accompanied or not by interocular assimetry were present in patients with a long history of MS and with the secondary-progressive form.
Succesive recordings of VEP have confirmed the positive effect of corticotherapy in flair and the positive evolution after treatment with interferon.
A new element in VEP monitoring is the dissapearence of VEP anomalies in some cases of recently diagnosed MS patients, with a complete recovery of wave latencies after treatment (corticotherapy or interferon).
The dynamic BAEP recordings does not show systematic reproductible changes in the MS patients which have participate in the study.
Acknowledgments
This study was funded by POS CCE-A2-O2.3.1-2012, Contract 575/12.09.2013.
References
- 1.Bajenaru O, Popescu CD, Tiu C, Marinescu D, Iana Gh. Guidelines for diagnosis and treatment for multiple sclerosis. Romanian Journal of Neurology(Ro J Neurol.)-EMCB[Internet] 2006;5(2):106–110. [Google Scholar]
- 2.Pierrot-Deseilligny C, Lubetzki C. In The neurologists of the group Piti�-Salp�tri�re: Neuro-pathology [Internet] 2000. Multiple Sclerosis and main differential diagnoses; pp. 71–83. [Google Scholar]
- 3.Evans AB. Medscape Reference[Internet] 2012. Clinical Utility of Evoked Potentials. pp. 1–10. [Google Scholar]
- 4.Calugaru L. PhD Thesis: �Clinical electroneurophysiology study in demyelinating diseases�. 1998. [Google Scholar]
- 5.Pidoux B. In Course OF Clinical Neurophysologie- [Internet] 2010. Visual evoked potentials; pp. 1–15. [Google Scholar]
- 6.Grecescu M. The incidence of visual subclinical manifestations in multiple sclerosis. Romanian Journal of Neurology(Ro J Neurol.) 2013;12(4):185–188. [Google Scholar]
- 7.Walsh P, Kane N, Butler S. The clinical role of evoked potentials. J Neurol Neurosurg Psychiatry. 2005;76:16–22. doi: 10.1136/jnnp.2005.068130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rigaudiere FV. In Eye and physiology of vision,I-Journals [Internet] 2013. Cortical Visual Evoked Potentials (VEP) pp. 17–27. [Google Scholar]
- 9.Mihancea P. Oradea,13 [Google Scholar]
- 10.Moore EJ. Bases of Auditory Brain-Stem Evoked Responses. New York: Grune & Stratton; 1983. pp. 132–186. [Google Scholar]