

Abstract
Background:
Erosive osteoarthritis (EOA) is a commonly invoked diagnosis representing an important variant of hand osteoarthritis (OA). There is increasing literature on the prevalence, risk factors, etiology, and management of EOA.
Methods:
We systematically reviewed the literature to assess variability in the diagnostic definitions used to define EOA in these studies.
Results:
We reviewed 336 articles and found 62 articles citing diagnostic definitions for EOA. Radiographic appearance was the most commonly used criterion, but there was little agreement on the details or extent of the radiographic changes. Overall, 56 of the 62 studies included clinical features in the diagnostic definitions, yet these features varied considerably. Exclusion criteria were mentioned in 43 of the studies.
Conclusion:
Based on the widely disparate definitions of EOA, we urge caution in interpretation of this literature, and propose that further understanding of EOA will require consensus on its definition.
Keywords: Osteoarthritis, Erosive osteoarthritis, Inflammatory osteoarthritis
Introduction
The clinical syndrome known as erosive osteoarthritis (EOA) represents an important and clinically challenging type of hand osteoarthritis. The term erosive osteoarthritis (EOA) was first used in 1966 by Peter et al. [1]. Interestingly, many of this original cohort eventually developed rheumatoid arthritis. Synonyms at times used interchangeably in the literature include “inflammatory osteoarthritis” and “erosive osteoarthrosis.” Interest in this subset of OA has persisted and considerable literature on this topic exists. There is intriguing evidence that the epidemiology, clinical presentation, and even severity of symptoms differs from typical hand OA and yet management strategies are poorly defined and largely untested. Many unanswered questions have fostered a healthy debate about how EOA should be viewed by researchers and clinicians. In particular, controversy exists about whether it should be defined solely by radiographic findings or should include clinical criteria and, moreover, whether EOA should be considered a phase on a continuum of hand OA evolution.
In practice, EOA is often recognized by radiographic changes characterized by erosions and central cortical collapse. These may be accompanied by osteophytes, subchondral cyst formation, periarticular ossicles, and, less commonly, subluxations and ankyloses [2,3]. Clinical features attributed to EOA include an abrupt onset of severe hand pain with variable degrees of stiffness, erythema, joint swelling, esthetic concerns, and deformities [4,5]. Some authors suggest EOA patients may be younger than those with typical hand OA though a lack of an established EOA definition makes the epidemiology difficult to interpret [6].
Data from the Framingham Offspring and Community cohorts estimate the prevalence of EOA in the general population to be 3% among men and 10% among women though prevalence estimates are likely to vary significantly based on the specific population studied [7]. Other studies assessing progression of hand OA cite 40% of patients with classical osteoarthritis were “complicated by manifest erosive changes” [8]. Thus, EOA may comprise a significant number of patients with hand OA.
The diagnosis of EOA is currently challenging. Disease mimics include common inflammatory arthritides such as psoriatic arthritis and rheumatoid arthritis. Sjogren’s syndrome has been associated with a very destructive arthritis involving the PIP joints [9]. Crystal-induced arthropathies including gout, calcium pyrophosphate deposition disease, and basic calcium phosphate-induced periarthritis can also produce similar symptoms. It remains unclear how EOA relates to typical hand OA, it may be a subtype of hand OA rather than a unique disease entity.
In reviewing the EOA literature, we noted considerable variation in the disease definition. Inconsistent disease definition precludes a full understanding of many of the key aspects of EOA and complicates diagnostic strategies. In addition, interpretation of newly identified biomarkers, improved imaging technology including ultrasonography, and advanced genetic analyses requires a precise disease definition. Perhaps most importantly, the lack of diagnostic consensus on EOA seriously weakens the impact of clinical studies of therapies for this painful osteoarthritis.
We undertook a systematic review of the body of literature on EOA with an objective of assessing the variability of published definitions of EOA.
Patients and methods
Literature search
We performed an electronic literature search of PubMed and Ovid/Medline using search terms “erosive osteoarthritis” and “erosive OA” for articles published between 1962 and August 2015.
Inclusion and exclusion criteria
Studies were included for analysis if they met the following criteria: English language, human subjects, greater than or equal to 3 patients studied, a stated definition of EOA, and focus on hand OA. All identified review articles, case reports, letters to the editor, and opinion pieces were excluded.
Results
The Figure represents a flow sheet of the study selection process. Search term “erosive osteoarthritis” (search 1) identified 329 articles while use of “erosive OA” (search 2) identified 109 articles. Only 7 of the 109 articles found with search 2 were not found with search 1. Therefore, after reviewing 336 studies, 62 met our inclusion criteria and are represented in the Table.
Fig.
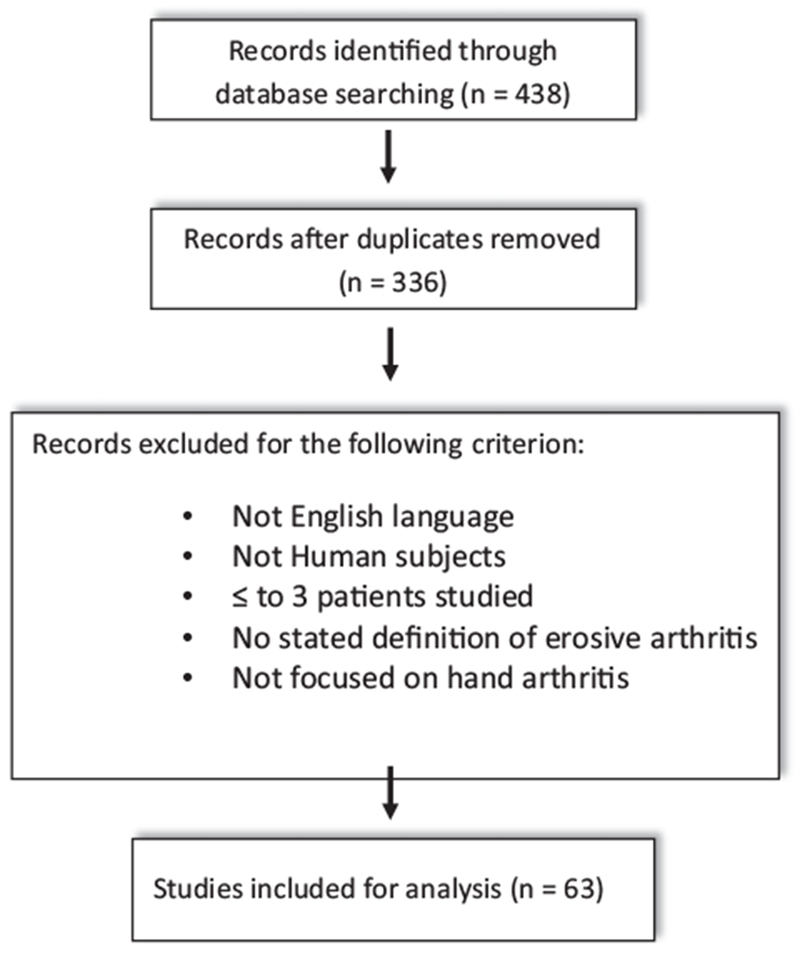
Flow diagram of study selection process.
Table.
Studies included in the systematic review
| Exclusion criteria |
||||||
|---|---|---|---|---|---|---|
| Clinical criteria | Radiologic criteria | No. of EOA patients | Labs | Patient characteristics | Family history of psoriasis | |
| 1 [17] | “… onset abrupt and painful” | Radiographic evidence of osteoarthritis | 170 | History of psoriasis | ||
| Nodal enlargement of small joints of hands | History or laboratory evidence of other rheumatic diseases | |||||
| 2 [18] | Osseous production or osteophytes of the PIP or DIP joints | 15 | ||||
| Erosions of the PIP and DIP joints | ||||||
| Absence of erosions at the inferior radioulnar or carpal articulations | ||||||
| 3 [19] | Symptomatic polyarticular IP hand OA affecting more than three rays of each hand— Heberden’s node formation | Subchondral erosions in three or more rays of each hand | 10 | Unrelated to obvious trauma | ||
| 4 [20] | Symptomatic polyarticular IP hand OA affecting more than three rays of each hand | Subchondral erosions in three or more rays of each hand | 10 | History of clinical, radiographic, or serological evidence of additional arthropathy | ||
| Heberden’s node formation | ||||||
| 5 [21] | “Presence of pain or stiffness in the fingers” | K/L grade III or IV OA in at least one joint with erosion of subchondral bone | 19 | |||
| 6 [22] | Bony erosions, collapse of subchondral plate or joint ankyloses of DIPs, PIPs, thumb IP joint, or MCPs | 33 | History of serologic or radiologic evidence of rheumatoid arthritis, psoriatic arthritis, SLE, or CPPD | |||
| 7 [23] | “…frank painful arthritis of PIP, DIP, and TMC joints.” | Joint-space narrowing and central joint erosions of PIP, DIP, and TMC joints | 24 | History of psoriasis, diabetes, spondyloarthritis, rheumatoid arthritis, gout, and tenosynovitis | Yes | |
| Juxta-articular osteoporosis | ||||||
| Marginal erosions “Laboratory abnormalities” | ||||||
| 8 [24] | “Inflammatory arthritis of PIP and DIP ....” | Evidence of OA and also bone erosions, collapse of subchondral plates, or joint ankylosis | 15 | History of other rheumatologic disorders known to cause articular changes | ||
| 9 [25] | ACR criteria for hand OA | Subchondral erosions and ankylosis of IP joints | 20 | History of rheumatoid arthritis, psoriatic arthritis, spondyloarthritis, and hyperparathyroidism | ||
| 10 [26] | “… acute, with pain, swelling, and tenderness of the joints.” | Presence of ≥3 subchondral erosions in DIPs, PIPs, 1st CMC, and trapezioscaphoid joints | 28 | RF+ | ||
| 11 [27] | “… phlogistic involvement of the DIP and PIP joints of each hand …” | “Typical” central erosions in IP joints | 56 | RF+ ANA+ |
History of psoriatic arthritis or psoriasis, RA, gout, pseudogout, Raynaud’s phenomenon, or undifferentiated spondyloarthropathies | |
| 12 [28] | ≥ 1 Central erosion in DIP and/or PIP | 24 | History of other erosive inflammatory and “dysmetabolic” conditions | |||
| 13 [29] | ACR criteria for hand OA | Central erosions | 21 | Post-menopausal Disease duration > 5 years | ||
| 14 [30] | “Inflammatory involvement of the DIP and/or PIP joints of each hand.” | “Typical EOA radiographic findings” | 56 | |||
| 15 [31] | ACR criteria for hand OA | ≥ 1 Joint erosions in thumb IP, DIPs, PIPs, and CMC-1 | 101 | |||
| 16 [32] | ACR criteria for hand OA | Radiographic central erosions and/or ankyloses in the IP joints of the hands in at least three digits | 26 | History of inflammatory arthritis, psoriasis, or CPPD. | ||
| Absence of erosions in the MCPs, carpal joints, or radio-carpal joint | ||||||
| 17 [33] | ACR criteria for hand OA | ≥ 1 Central erosion in DIP or PIP | 24 | History of other erosive inflammatory and “dysmetabolic” conditions | ||
| 18 [34] | ACR criteria for hand OA | Central erosions and/or ankylosis in IP joints in at least three digits | 30 | Personal history of psoriasis | Yes | |
| History of other rheumatic or skeletal degenerative diseases | ||||||
| 19 [35] | ACR criteria for hand OA | At least 2 erosions in IP joints | 84 | |||
| No erosions in MCPs | ||||||
| 20 [36] | “… typical EOA radiologic findings.” | 32 | History of psoriatic arthritis, rheumatoid arthritis, undifferentiated spondyloarthropathies, gout, and pseudogout | |||
| 21 [37] | ACR criteria for hand OA | ≥ 2 Erosions in DIP or PIP joints | 67 | RF+ | History of other known arthropathies | |
| No erosions in MCPs | ||||||
| 22 [38] | “Swelling, pain, and tenderness of DIP and PIP joints” | “Typical central erosions, subchondral plate collapse and bone ankyloses in combination with classical OA changes” | 22 | ESR > 20 mm/h CRP > 0.5 mg/dl |
Radiographic signs of rheumatoid arthritis, psoriatic arthritis, chondrocalcinosis, and gout | |
| Heberden’s and Bouchard’s nodes | RF+ ANA+ |
|||||
| 23 [39] | ACR criteria for hand OA | Central erosions, and/or ankylosis in the IP joints in at least 3 digits, associated with joint-space narrowing, subchondral sclerosis and/or osteophytes | 15 | History of psoriasis | Yes | |
| 24 [40] | ACR criteria for hand OA | ≥ 1 Articular surface erosion at the DIP and/or PIP | 12 | History of SLE, psoriasis | ||
| 25 [41] | ACR criteria for hand OA | K/L scoring | 30 | History of fracture, inflammatory disease (RA) or Paget’s disease. | ||
| 26 [42] | High pain level on VAS | “Important radiographic erosions” | 3 | RF+ CCP+ ESR > 10 mm/h |
||
| 27 [43] | ACR criteria for hand OA | Single erosion of PIP or DIP joint Kallman grading scale |
55 | |||
| 28 [44] | ACR criteria for hand OA | Erosions on articular surface | 22 | |||
| 29 [45] | ACR criteria for hand OA | Central articular erosions in at least 1 PIP or DIP joints | 10 | RF+ CCP+ ANA + ESR/CRP in normal range |
History of concomitant rheumatic disease | |
| 30 [46] | Erosive OA PIP and DIP joints (excludes thumb) | 18 | History of other rheumatologic conditions | |||
| 31 [47] | ACR criteria for hand OA | Erosions in the central joint area of the IP joints | 18 | RF+ | ||
| 32 [48] | ACR criteria for hand OA | “Typical erosive changes in two or more digits” | 197 | History of other inflammatory arthritides or psoriasis | Yes | |
| 33 [49] | ACR criteria for hand OA | Erosive features according to the V/V system in ≥ 2 IP joints | 12 | |||
| 34 [50] | ACR criteria for hand OA | Classic central erosions in at least 2 joints | 13 | RF+ | History of psoriasis, connective tissue disease, other inflammatory arthritides, inflammatory bowel diseases, gout, or chondrocalcinosis | Yes |
| 35 [51] | ACR criteria for hand OA | Presence of erosions in at least 1 joint | 31 | |||
| 36 [52] | ACR criteria for hand OA | Presence of central subchondral bone erosions in ≥ 2 IP joints of the hands | 94 | RF+ CCP+ |
History of other known arthropathies, radiographic chondrocalcinosis, or sacroillitis | Yes |
| 37 [53] | ACR criteria for hand OA | EULAR recommendations for EOA | 32 | History of infections, cancer, renal, and liver diseases, cryoglobulinemia, scleroderma, sjogren syndrome, autoimmune thyroiditis, psoriatic arthritis undifferentiated spondyloarthropathies, gout, and pseudogout. | ||
| 38 [54] | EULAR recommendations for the diagnosis of hand OA | 9 | ||||
| 39 [55] | ACR criteria for hand OA | ≥ 1 Erosive IP finger joint | 9 | |||
| 40 [56] | Self-reported hand pain | ≥ 1 IP joint with erosions according to the V/V system | 96 | |||
| 41] [57] | ACR criteria of hand OA | “Erosive pattern” K/L and Kallman scoring systems |
233 | History of clinical and laboratory features of chronic inflammatory rheumatic diseases (including microcrystal diseases) | Yes | |
| 42 [58] | ACR criteria of hand OA | Kallman grading scale | 31 | |||
| 43 [59] | ACR criteria for hand OA | ≥ 1 IP finger joint in erosive phase of V/V system | 60 | RF+ CCP+ |
History of chronic inflammatory rheumatic disease | |
| 44 [60] | ACR criteria for hand OA | Presence of erosive features in ≥ 2 IP joints according to V/V system | 167 | History of other rheumatic diseases or disorders that can impair the functionality of the hand | ||
| 45 [61] | Painful phase VAS score > 4/10 of two or more PIPs or DIPs | ≥ 2 PIP or DIP with sharp marginal defects, central crumbling erosions | 38 | History of rheumatologic diseases | ||
| 46 [62] | ACR criteria of hand OA | ≥ 2 IP joints with central erosions | 233 | RF+ | History of chronic inflammatory diseases including rheumatoid arthritis, inflammatory bowel disease, uveitis, connective tissue diseases, or psoriasis. History or evidence of microcrystalline arthritis. |
Yes |
| 47 [63] | ACR criteria for hand OA | ≥ 2 Joints with erosive features according to V/V system | 68 | |||
| 48 [64] | ≥ 1 DIP/PIP joint with K/L grade > 2 and erosion in same joint | 355 | ||||
| 49 [65] | ACR criteria for hand OA | ≥ 1 Central bone erosion in IP joints No erosions in MCP and/or thumb base joint |
57 | History of known arthropathies or psoriasis | Yes | |
| 50 [66] | Hand pain, aching, or stiffness > 1 day in last 1 month |
≥ 1 “E or R” phase DIP, PIP, or 1st IP joints according to V/V system |
80 | |||
| 51 [67] | Hand pain, aching, or stiffness > 1 day in last 1 month | Presence of erosions in IP joints according to V/V system | 52 | History of rheumatoid arthritis or psoriatic arthritis | ||
| 52 [68] | ACR criteria for hand OA | ≥ 1 Erosion in IP joint | 13 | |||
| 53 [69] | Self-reported symptoms Presence of HN and/or BN |
Central erosion in at least 2 IP joints | 146 | |||
| 54 [70] | ACR criteria for hand OA | ≥ 1 Erosive IP joint | 9 | History of rheumatoid arthritis, psoriatic arthritis, or gout | ||
| 55 [71] | ACR criteria for hand OA | > 1 “E or R” phase joint according to V/V | 28 | RF+ | History of other inflammatory joint disease or disorders such as carpel tunnel syndrome History of trauma or operation on the hands < 6 months ago |
|
| 56 [72] | Hand pain on a few days or more in previous month | ≥ 1 “E or R” phase IP joints according to V/V system | 80 | History of rheumatoid arthritis or psoriatic arthritis | ||
| 57 [73] | ACR criteria for hand OA | IP joint central erosions | 24 | |||
| 58 [74] | Hand pain ≥ 1 day in last 1 month | ≥ “E or R” phase in CMC, DIP, PIP, or 1st IP joints according to V/V system | History of systemic inflammatory rheumatic disease History of inflammatory changes on radiographs |
|||
| 59 [75] | ACR criteria for hand OA | ≥ 1 Erosion in DIP or PIP joint | 14 | History of any autoimmune disease including psoriasis | ||
| 60 [76] | ACR criteria for hand OA | ≥ 1 Joints with central erosions joints with grade ≥ 2 according to K/L | 131 | History of inflammatory joint diseases | ||
| 61 [77] | ACR criteria for hand OA | Central erosions in IP joints Erosions in MCP joints | 55 | History of trauma or other arthropathies including rheumatoid arthritis, psoriatic arthritis, gout, or chondrocalcinosis | ||
| 62 [78] | ACR criteria for hand OA | “Gull-wing” configuration at DIP and/or PIP joints | 17 | History of arthritis/arthralgia involving the hand, such as rheumatoid arthritis, peripheral spondyloarthritis, hemochromatosis, traumatic arthritis, crystalline arthritis, and fibromyalgia. | ||
ACR = American College of Rheumatology, EULAR = European League Against Rheumatism, EOA = erosive osteoarthritis, OA = osteoarthritis, K/L = Kellgren and Lawrence, V/V = Verbruggen and Veys, DIP = distal interphalangeal, PIP = proximal interphalangeal, MCP = metacarpalphalangeal, IP = interphalangeal, CMC = carpometacarpal, VAS = visual analog scale, HN = Heberden’s nodes, BN = Bouchard’s nodes, “E or R” = erosive or remodeled.
The sizes of the studies varied among the 62 studies included for analysis with patient numbers ranging from 3 to 355. Defining clinical definition as information obtainable by history or physical exam, 55 of the 62 studies used a definition that included some combination of both clinical and radiographic parameters. Overall, 37 studies used the 1990 ACR criteria for hand OA as a clinical criterion [10]. One study used the EULAR task force evidence-based recommendations for hand OA diagnosis published in 2008 [11]. Six studies used no clinical inclusion. In all, 18 of the 62 studies employed unique clinical criteria based on features such as the number of involved joints, pain levels on VAS, presence of visible or palpable nodes, duration and frequency of joint pain, swelling, and stiffness.
Radiological definitions were included in all studies except one and remain the major parameter for the definition of EOA. The single study not including a radiographic criterion was a magnetic resonance imaging study (54). In all, 17 of the 62 studies used a named OA grading or scoring system such as Kellgren and Lawrence [2], Verbruggen and Veys [12], or Kallman [3].The majority of studies (64%) outlining individual radiographic definitions for EOA often included common terms such as central articular erosions, subchondral erosions, ankyloses, or “gull wing” or “saw tooth” deformities. Five studies refer to “typical” EOA radiographic findings as a radiologic definition. Sixteen studies included images of radiographs depicting examples of EOA. Radiographic definitions included a threshold for the number of involved joints in 37 of the 62 studies identified. Of those 37 articles, 19 required ≥ 1 involved joint, 12 required ≥ 2 involved joints, and 6 required ≥ 3 involved joints. Four studies included the presence of MCP erosions as an exclusion criterion.
Overall, 40 of the 62 studies included an alternative diagnosis as an exclusion criterion. The presence of psoriasis, rheumatoid arthritis, a spondyloarthropathy, crystal arthropathy, a metabolic condition, and trauma are all sporadically mentioned as exclusion criteria. Twelve studies included the presence of a positive rheumatoid factor as an exclusion criterion. Four studies also included the presence of a positive ANA or elevated inflammatory markers as exclusion criteria. Interestingly, the presence of a family history of psoriasis was also infrequently mentioned as an exclusion criterion.
Discussion
It is not clear whether EOA is a subset of HOA to be placed on a spectrum of degenerative joint diseases or whether it represents a separate disease entity with a pathophysiology similar to arthropathies traditionally felt to represent inflammatory disease such as crystal arthritis, rheumatoid arthritis, or spondyloarthropathy. However, defining EOA remains critical in order to study the disease further with hopes of improved understanding of the pathogenesis and, ultimately improve accuracy of diagnosis and efficacy of treatment. The goal of this work was not to establish a set of diagnostic criteria but rather to carefully review the available literature and determine disparities and trends across studies regarding the definition of EOA.
This systematic review found remarkably little uniformity among studies regarding a definition of EOA. While the majority of studies (60%) used the 1990 ACR hand OA definition (which includes patient experiencing pain, aching, or stiffness along with hard tissue enlargement of 2 or more selected joints and fewer than 3 swollen MCP joints along with hard tissue enlargement of 2 or more DIP joints or deformity of 2 or more of 10 selected joints), some included no clinical definitions and 30% of studies included no exclusion criteria to limit inclusion of common EOA mimics. Nearly all studies used some form of a radiographic definition. However, radiographic definitions varied widely and the majority of authors used their own unique radiographic definitions of EOA. Approximately, 1/3 of studies required patients to only meet radiographic criteria at a single joint often without any consideration of prior joint trauma or other local processes. Masking even more lack of uniformity when it comes to defining EOA in the literature is the observation that several authorship groups are cited multiple times in the Table. For example, the Italian group of authors including Dr. Punzi is responsible for 7 out of the 62 publications.
There are many potential reasons for this lack of consistency in the EOA literature. Central to the problem, undoubtedly, is it is unknown whether EOA is a unique entity or whether it represents a true subtype of HOA. As a result, there are no established diagnostic or classification criteria for EOA accepted by musculoskeletal medicine groups or societies. Proposed diagnostic criteria have been outlined which includes a combination of clinical criteria, exclusion criteria, limited radiographic criteria, and normal (or near normal) markers of inflammation but these are not validated and do not seem widely used [13]. In addition, the pathogenesis of EOA remains unclear with an evolving literature regarding biomarkers and imaging advancements with potential to continuously redefine the disease. Finally, diagnostic criteria are particularly important for recruitment for therapeutic studies which are, in general, limited in HOA literature. Radiographic definitions for defining EOA are very important. However, there currently is not a clear consensus regarding a preferred method for an HOA grading scale and, moreover, correlation between pain, disability, and radiographic findings is known to be poor. Several scoring systems have been created in an effort to grade osteoarthritis severity. Among them, the initial Kellgren and Lawrence system has been criticized for an excessive dependence on the presence of osteophytes and a modified score has been created to combat this potential shortcoming [14]. Large image collections, including the OARSI atlases, are widely available and provide a standardized semi-quantitative methodology to assess for presence and severity of OA at many anatomical sites including the hand [15]. Another scoring system from Verbruggen and Veys based on a paradigm involving successive and radiographically recognizable phases of hand OA now includes an updated Ghent University Scoring System (GUSS) to adjust for pathological changes and phase overlap felt to be unique to EOA [16].
Future diagnostic definitions will need to consider demographics (including age and gender), description and duration of symptoms, longitudinal data regarding number of joints involved over time, and exam findings. In addition, major components of any future diagnostic definition of EOA should include well-defined radiographic findings as well as important “negatives” such as serology results and presence of co-morbidities such as psoriasis, inflammatory bowel disease, gout, and calcium pyrophosphate deposition disease. Most importantly, identifying efficacious treatments, that are rigorously tested, for patients suffering from EOA, will require an established disease definition.
Conclusion
In our review, we observed a lack of uniform diagnostic definitions in the EOA literature. In the future, it will be necessary to define EOA so as to establish clear classification and diagnostic criteria.
References
- [1].Peter JB, Pearson CM, Marmor L. Erosive osteoarthritis of the hands. Arthritis Rheum 1966;9:365–88. [DOI] [PubMed] [Google Scholar]
- [2].Kellgren JH, Lawrence JS. Radiological assessment of osteoarthrosis. Ann Rheum Dis 1957;16:494–502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Kallman DA, Wigley FM, Scott WW Jr, Hochberg MC, Tobin JD. New radiographic grading scales for osteoarthritis of the hand. Reliability for determining prevalence and progression. Arthritis Rheum 1989;32:1584–91. [DOI] [PubMed] [Google Scholar]
- [4].Punzi L, Frigato M, Frallonardo P, Ramonda R. Inflammatory osteoarthritis of the hand. Best Pract Res Clin Rheumatol 2010;24:301–12. [DOI] [PubMed] [Google Scholar]
- [5].Neuprez A, Bruyere O, Maheu E, Dardenne N, Burlet N, D’Hooghe P, et al. Aesthetic discomfort in hand osteoarthritis: results from the LIege Hand Osteoarthritis Cohort (LIHOC). Arthritis Res Ther 2015;17:346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Banks SE. Erosive osteoarthritis: a current review of a clinical challenge. Clin Rheumatol 2010;29:697–706. [DOI] [PubMed] [Google Scholar]
- [7].Haugen IK, Englund M, Aliabadi P, Niu J, Clancy M, Kvien TK, et al. Prevalence, incidence and progression of hand osteoarthritis in the general population: the Framingham Osteoarthritis Study. Ann Rheum Dis 2011;70:1581–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Verbruggen G, Veys EM. Numerical scoring systems for the progression of osteoarthritis of the finger joints. Rev Rhum Engl Ed 1995;62(6 Suppl. 1):27S–32S. [PubMed] [Google Scholar]
- [9].Shuckett R, Russell ML, Gladman DD. Atypical erosive osteoarthritis and Sjogren’s syndrome. Ann Rheum Dis 1986;45:281–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Altman R, Alarcon G, Appelrouth D, Bloch D, Borenstein D, Brandt K, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hand. Arthritis Rheum 1990;33:1601–10. [DOI] [PubMed] [Google Scholar]
- [11].Zhang W, Doherty M, Leeb BF, Alekseeva L, Arden NK, Bijlsma JW, et al. EULAR evidence-based recommendations for the diagnosis of hand osteoarthritis: report of a task force of ESCISIT. Ann Rheum Dis 2009;68:8–17. [DOI] [PubMed] [Google Scholar]
- [12].Verbruggen G, Veys EM. Numerical scoring systems for the anatomic evolution of osteoarthritis of the finger joints. Arthritis Rheum 1996;39:308–20. [DOI] [PubMed] [Google Scholar]
- [13].Anandarajah A Erosive osteoarthritis. Discov Med 2010;9:468–77. [PubMed] [Google Scholar]
- [14].Felson DT, Niu J, Guermazi A, Sack B, Aliabadi P. Defining radiographic incidence and progression of knee osteoarthritis: suggested modifications of the Kellgren and Lawrence scale. Ann Rheum Dis 2011;70:1884–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Altman RD, Gold GE. Atlas of individual radiographic features in osteoarthritis, revised. Osteoarthritis Cartilage 2007;15(Suppl. A): A1–56. [DOI] [PubMed] [Google Scholar]
- [16].Berbruggen G, Wittoek R, Vander Cruyssen B, Elewaut D. Ann Rheum Dis 2010;69:862–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Ehrlich GE. Inflammatory osteoarthritis. I. The clinical syndrome. J Chronic Dis 1972;25:317–28. [DOI] [PubMed] [Google Scholar]
- [18].Utsinger PD, Resnick D, Shapiro RF, Wiesner KB. Roentgenologic, immunologic, and therapeutic study of erosive (inflammatory) osteoarthritis. Arch Intern Med 1978;138:693–7. [PubMed] [Google Scholar]
- [19].Pattrick M, Manhire A, Ward AM, Doherty M. HLA-A, B antigens and alpha 1-antitrypsin phenotypes in nodal generalised osteoarthritis and erosive osteoarthritis. Ann Rheum Dis 1989;48:470–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Pattrick M, Aldridge S, Hamilton E, Manhire A, Doherty M. A controlled study of hand function in nodal and erosive osteoarthritis. Ann Rheum Dis 1989;48:978–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Duncan IJ, Hurst NP, Sebben R, Milazzo SC, Disney A. Premature development of erosive osteoarthritis of hands in patients with chronic renal failure. Ann Rheum Dis 1990;49:378–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Smith D, Braunstein EM, Brandt KD, Katz BP. A radiographic comparison of erosive osteoarthritis and idiopathic nodal osteoarthritis. J Rheumatol 1992;19:896–904. [PubMed] [Google Scholar]
- [23].Rovetta G, Monteforte P. Galactosaminoglycuronglycan sulfate in erosive osteoarthritis of the hands: early diagnosis, early treatment. Int J Tissue React 1996;18:43–6. [PubMed] [Google Scholar]
- [24].Punzi L, Bertazzolo N, Pianon M, Michelotto M, Todesco S. Soluble interleukin 2 receptors and treatment with hydroxychloroquine in erosive osteoarthritis. J Rheumatol 1996;23:1477–8. [PubMed] [Google Scholar]
- [25].Rovetta G, Battista S, Brignone A, Monteforte P. Quantitative ultrasound of the proximal phalanges: reproducibility in erosive and nodal osteoarthritis of the hands. Int J Tissue React 1999;21:121–7. [PubMed] [Google Scholar]
- [26].Olejarova M, Kupka K, Pavelka K, Gatterova J, Stolfa J. Comparison of clinical, laboratory, radiographic, and scintigraphic findings in erosive and nonerosive hand osteoarthritis. Results of a two-year study. Joint Bone Spine 2000;67:107–12. [PubMed] [Google Scholar]
- [27].Fioravanti A, Tofi C, Cerase A, Priolo F, Marcolongo R. Capillaroscopic findings in erosive and nodal osteoarthritis of the hands. Clin Rheumatol 2001;20:174–6. [DOI] [PubMed] [Google Scholar]
- [28].Rovetta G, Monteforte P, Molfetta G, Balestra V. Chondroitin sulfate in erosive osteoarthritis of the hands. Int J Tissue React 2002;24:29–32. [PubMed] [Google Scholar]
- [29].Rovetta G, Monteforte P, Grignolo MC, Brignone A, Buffrini L. Hematic levels of type I collagen C-telopeptide in erosive versus nonerosive osteoarthritis of the hands. Int J Tissue React 2003;25:25–8. [PubMed] [Google Scholar]
- [30].Falsetti P, Frediani B, Fioravanti A, Acciai C, Baldi F, Filippou G, et al. Sonographic study of calcaneal entheses in erosive osteoarthritis, nodal osteoarthritis, rheumatoid arthritis and psoriatic arthritis. Scand J Rheumatol 2003;32:229–34. [DOI] [PubMed] [Google Scholar]
- [31].Rovetta G, Monteforte P, Baratto L, Franchin F. Joint involvement patterns in nodal versus erosive osteoarthritis of the hands. Int J Tissue React 2004;26:39–42. [PubMed] [Google Scholar]
- [32].Stern AG, de Carvalho MR, Buck GA, Adler RA, Rao TP, Disler D, et al. Association of erosive hand osteoarthritis with a single nucleotide polymorphism on the gene encoding interleukin-1 beta. Osteoarthritis Cartilage 2003;11:394–402. [DOI] [PubMed] [Google Scholar]
- [33].Rovetta G, Monteforte P, Molfetta G, Balestra V. A two-year study of chondroitin sulfate in erosive osteoarthritis of the hands: behavior of erosions, osteophytes, pain and hand dysfunction. Drugs Exp Clin Res 2004;30:11–6. [PubMed] [Google Scholar]
- [34].Silvestri T, Pulsatelli L, Dolzani P, Punzi L, Meliconi R Analysis of cartilage biomarkers in erosive and non-erosive osteoarthritis of the hands. Osteoarthritis Cartilage 2004;12:843–5. [DOI] [PubMed] [Google Scholar]
- [35].Punzi L, Ramonda R, Sfriso P. Erosive osteoarthritis. Best Pract Res Clin Rheumatol 2004;18:739–58. [DOI] [PubMed] [Google Scholar]
- [36].Morozzi G, Bellisai F, Fioravanti A, Galeazzi M. Absence of anti-cyclic citrullinated peptide antibodies in erosive osteoarthritis: further serological evidence of the disease as a subset of osteoarthritis. Ann Rheum Dis 2005;64:1095–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Punzi L, Ramonda R, Oliviero F, Sfriso P, Mussap M, Plebani M, et al. Value of C reactive protein in the assessment of erosive osteoarthritis of the hand. Ann Rheum Dis 2005;64:955–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Iagnocco A, Filippucci E, Ossandon A, Ciapetti A, Salaffi F, Basili S, et al. High resolution ultrasonography in detection of bone erosions in patients with hand osteoarthritis. J Rheumatol 2005;32:2381–3. [PubMed] [Google Scholar]
- [39].Zoli A, Lizzio MM, Capuano A, Massafra U, Barini A, Ferraccioli G. Osteoporosis and bone metabolism in postmenopausal women with osteoarthritis of the hand. Menopause 2006;13:462–6. [DOI] [PubMed] [Google Scholar]
- [40].Magnano MD, Chakravarty EF, Broudy C, Chung L, Kelman A, Hillygus J, et al. A pilot study of tumor necrosis factor inhibition in erosive/inflammatory osteoarthritis of the hands. J Rheumatol 2007;34:1323–7. [PubMed] [Google Scholar]
- [41].Scarpellini M, Lurati A, Vignati G, Marrazza MG, Telese F, Re K, et al. Biomarkers, type II collagen, glucosamine and chondroitin sulfate in osteoarthritis follow-up: the “Magenta osteoarthritis study”. J Orthop Traumatol 2008;9:81–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Bacconnier L, Jorgensen C, Fabre S. Erosive osteoarthritis of the hand: clinical experience with anakinra. Ann Rheum Dis 2009;68:1078–9. [DOI] [PubMed] [Google Scholar]
- [43].Filkova M, Senolt L, Braun M, Hulejova H, Pavelkova A, Sleglova O, et al. Serum hyaluronic acid as a potential marker with a predictive value for further radiographic progression of hand osteoarthritis. Osteoarthritis Cartilage 2009;17:1615–9. [DOI] [PubMed] [Google Scholar]
- [44].Vlychou M, Koutroumpas A, Malizos K, Sakkas LI. Ultrasonographic evidence of inflammation is frequent in hands of patients with erosive osteoarthritis. Osteoarthritis Cartilage 2009;17:1283–7. [DOI] [PubMed] [Google Scholar]
- [45].Fioravanti A, Fabbroni M, Cerase A, Galeazzi M. Treatment of erosive osteoarthritis of the hands by intra-articular infliximab injections: a pilot study. Rheumatol Int 2009;29:961–5. [DOI] [PubMed] [Google Scholar]
- [46].Verbruggen G, Wittoek R, Vander Cruyssen B, Elewaut D. Morbid anatomy of ‘erosive osteoarthritis’ of the interphalangeal finger joints: an optimised scoring system to monitor disease progression in affected joints. Ann Rheum Dis 2010;69:862–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Koutroumpas AC, Alexiou IS, Vlychou M, Sakkas LI. Comparison between clinical and ultrasonographic assessment in patients with erosive osteoarthritis of the hands. Clin Rheumatol 2010;29:511–6. [DOI] [PubMed] [Google Scholar]
- [48].Vargiolu M, Silvestri T, Bonora E, Dolzani P, Pulsatelli L, Addimanda O, et al. Interleukin-4/interleukin-4 receptor gene polymorphisms in hand osteoarthritis. Osteoarthritis Cartilage 2010;18:810–6. [DOI] [PubMed] [Google Scholar]
- [49].Bijsterbosch J, Watt I, Meulenbelt I, Rosendaal FR, Huizinga TW, Kloppenburg M. Clinical burden of erosive hand osteoarthritis and its relationship to nodes. Ann Rheum Dis 2010;69:1784–8. [DOI] [PubMed] [Google Scholar]
- [50].Mancarella L, Magnani M, Addimanda O, Pignotti E, Galletti S, Meliconi R. Ultrasound-detected synovitis with power Doppler signal is associated with severe radiographic damage and reduced cartilage thickness in hand osteoarthritis. Osteoarthritis Cartilage 2010;18:1263–8. [DOI] [PubMed] [Google Scholar]
- [51].Wittoek R, Carron P, Verbruggen G. Structural and inflammatory sonographic findings in erosive and non-erosive osteoarthritis of the interphalangeal finger joints. Ann Rheum Dis 2010;69:2173–6. [DOI] [PubMed] [Google Scholar]
- [52].Ramonda R, Musacchio E, Campana C, Frigato M, Frallonardo P, Barbieri V, et al. Immunogenetic aspects of erosive osteoarthritis of the hand in patients from northern Italy. Scand J Rheumatol 2011;40:139–44. [DOI] [PubMed] [Google Scholar]
- [53].Guidelli GM, Morozzi G, Simpatico A, Fioravanti A. Rheumatoid factor isotypes in patients with erosive osteoarthritis of the hand. Int J Rheum Dis 2011;14:e49–50. [DOI] [PubMed] [Google Scholar]
- [54].Schraml C, Schwenzer NF, Martirosian P, Koetter I, Henes JC, Geiger K, et al. Assessment of synovitis in erosive osteoarthritis of the hand using DCE-MRI and comparison with that in its major mimic, the psoriatic arthritis. Acad Radiol 2011;18:804–9. [DOI] [PubMed] [Google Scholar]
- [55].Wittoek R, Jans L, Lambrecht V, Carron P, Verstraete K, Verbruggen G. Reliability and construct validity of ultrasonography of soft tissue and destructive changes in erosive osteoarthritis of the interphalangeal finger joints: a comparison with MRI. Ann Rheum Dis 2011;70:278–83. [DOI] [PubMed] [Google Scholar]
- [56].Kwok WY, Kloppenburg M, Rosendaal FR, van Meurs JB, Hofman A, Bierma-Zeinstra SM. Erosive hand osteoarthritis: its prevalence and clinical impact in the general population and symptomatic hand osteoarthritis. Ann Rheum Dis 2011;70:1238–42. [DOI] [PubMed] [Google Scholar]
- [57].Addimanda O, Mancarella L, Dolzani P, Ramonda R, Fioravanti A, Brusi V, et al. Clinical associations in patients with hand osteoarthritis. Scand J Rheumatol 2012;41:310–3. [DOI] [PubMed] [Google Scholar]
- [58].Braun M, Hulejova H, Gatterova J, Filkova M, Pavelkova A, Sleglova O, et al. Pentosidine, an advanced glycation end-product, may reflect clinical and morphological features of hand osteoarthritis. Open Rheumatol J 2012;6:64–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [59].Verbruggen G, Wittoek R, Vander Cruyssen B, Elewaut D Tumour necrosis factor blockade for the treatment of erosive osteoarthritis of the interphalangeal finger joints: a double blind, randomised trial on structure modification. Ann Rheum Dis 2012;71:891–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [60].Wittoek R, Cruyssen BV, Verbruggen G. Predictors of functional impairment and pain in erosive osteoarthritis of the interphalangeal joints: comparison with controlled inflammatory arthritis. Arthritis Rheum 2012;64:1430–6. [DOI] [PubMed] [Google Scholar]
- [61].Saviola G, Abdi-Ali L, Campostrini L, Sacco S, Baiardi P, Manfredi M, et al. Clodronate and hydroxychloroquine in erosive osteoarthritis: a 24-month open randomized pilot study. Mod Rheumatol 2012;22:256–63. [DOI] [PubMed] [Google Scholar]
- [62].Addimanda O, Mancarella L, Dolzani P, Punzi L, Fioravanti A, Pignotti E, et al. Clinical and radiographic distribution of structural damage in erosive and nonerosive hand osteoarthritis. Arthritis Care Res (Hoboken) 2012;64:1046–53. [DOI] [PubMed] [Google Scholar]
- [63].Hodkinson B, Maheu E, Michon M, Carrat F, Berenbaum F. Assessment and determinants of aesthetic discomfort in hand osteoarthritis. Ann Rheum Dis 2012;71:45–9. [DOI] [PubMed] [Google Scholar]
- [64].Haugen IK, Felson DT, Englund M, Wang K, Aliabadi P, Guermazi A, et al. The association between erosive hand osteoarthritis and subchondral bone attrition of the knee: the Framingham Osteoarthritis Study. Ann Rheum Dis 2012;71:1698–701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [65].Punzi L, Ramonda R, Deberg M, Frallonardo P, Campana C, Musacchio E, et al. Coll2-1, Coll2-1NO2 and myeloperoxidase serum levels in erosive and non-erosive osteoarthritis of the hands. Osteoarthritis Cartilage 2012;20:557–61. [DOI] [PubMed] [Google Scholar]
- [66].Kwok WY, Kloppenburg M, Marshall M, Nicholls E, Rosendaal FR, van der Windt DA, et al. Comparison of clinical burden between patients with erosive hand osteoarthritis and inflammatory arthritis in symptomatic community-dwelling adults: the Keele clinical assessment studies. Rheumatology (Oxford) 2013;52:2260–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [67].Marshall M, Peat G, Nicholls E, van der Windt D, Myers H, Dziedzic K. Subsets of symptomatic hand osteoarthritis in community-dwelling older adults in the United Kingdom: prevalence, inter-relationships, risk factor profiles and clinical characteristics at baseline and 3-years. Osteoarthritis Cartilage 2013;21:1674–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [68].Vlychou M, Koutroumpas A, Alexiou I, Fezoulidis I, Sakkas LI. High-resolution ultrasonography and 3.0 T magnetic resonance imaging in erosive and nodal hand osteoarthritis: high frequency of erosions in nodal osteoarthritis. Clin Rheumatol 2013;32:755–62. [DOI] [PubMed] [Google Scholar]
- [69].Pulsatelli L, Assirelli E, Dolzani P, Addimanda O, Mancarella L, Pavloska B, et al. Increased serum vascular cell adhesion molecule (VCAM)-1 levels in patients with erosive hand osteoarthritis. Rheumatology (Oxford) 2013;52:400–2. [DOI] [PubMed] [Google Scholar]
- [70].Jans L, De Coninck T, Wittoek R, Lambrecht V, Huysse W, Verbruggen G, et al. 3 T DCE-MRI assessment of synovitis of the interphalangeal joints in patients with erosive osteoarthritis for treatment response monitoring. Skeletal Radiol 2013;42:255–60. [DOI] [PubMed] [Google Scholar]
- [71].Kortekaas MC, Kwok WY, Reijnierse M, Huizinga TW, Kloppenburg M. In erosive hand osteoarthritis more inflammatory signs on ultrasound are found than in the rest of hand osteoarthritis. Ann Rheum Dis 2013;72:930–4. [DOI] [PubMed] [Google Scholar]
- [72].Marshall M, Nicholls E, Kwok WY, Peat G, Kloppenburg M, van der Windt D, et al. Erosive osteoarthritis: a more severe form of radiographic hand osteoarthritis rather than a distinct entity? Ann Rheum Dis 2015;74:136–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [73].Koutroumpas A, Giannoukas A, Zintzaras E, Exarchou E, Baliakos A, Makaritsis K, et al. Erosive hand osteoarthritis is associated with subclinical atherosclerosis and endothelial dysfunction. Int J Biomed Sci 2013;9:217–23. [PMC free article] [PubMed] [Google Scholar]
- [74].Kwok WY, Kloppenburg M, Marshall M, Nicholls E, Rosendaal FR, Peat G. The prevalence of erosive osteoarthritis in carpometacarpal joints and its clinical burden in symptomatic community-dwelling adults. Osteoarthritis Cartilage 2014;22:756–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [75].Shirinsky IV, Shirinsky VS Treatment of erosive osteoarthritis with peroxisome proliferator-activated receptor alpha agonist fenofibrate: a pilot study. Rheumatol Int 2014;34:613–6. [DOI] [PubMed] [Google Scholar]
- [76].Magnusson K, Hagen KB, Osteras N, Nordsletten L, Natvig B, Haugen IK. Diabetes is associated with increased hand pain in erosive hand osteoarthritis: data from a population-based study. Arthritis Care Res (Hoboken) 2015;67:187–95. [DOI] [PubMed] [Google Scholar]
- [77].Ramonda R, Sartori L, Ortolan A, Frallonardo P, Lorenzin M, Punzi L, et al. The controversial relationship between osteoarthritis and osteoporosis: an update on hand subtypes. Int J Rheum Dis 2015. [DOI] [PubMed] [Google Scholar]
- [78].Ma J, Talukdar R, Gainers-Hasugluw V. Pilot open observations on doxycycline treatment for erosive osteoarthritis of the hand. J Clin Rheumatol 2015;21:38–9. [DOI] [PubMed] [Google Scholar]