

Abstract
Purpose:
To grade the severity of limbal stem cell deficiency (LSCD) based on the extent of clinical presentation and central cornea basal epithelial cell density (BCD).
Methods:
This is a retrospective observational case-control study of forty-eight eyes of 35 patients with LSCD and 9 eyes of 7 normal subjects were included. Confocal images of the central cornea were acquired. A clinical scoring system was created based on the extent of limbal and corneal surface involvement. LSCD was graded as mild, moderate, and severe stages based on the clinical scores. The degree of BCD reduction was given a score of 0 to 3.
Results:
Compared with BCD in control eyes, BCD decreased by 23.0%, 40.4%, and 69.5% in the mild, moderate and severe stages of LSCD classified by the clinical scoring system, respectively. The degree of BCD reduction was positively correlated with larger limbal and corneal surface involvement, and when the central visual axis was affected (all p≤0.0005). The mean CDVA LogMAR was 0.0±0.0 in control eyes, 0.2±0.5 in mild LSCD, 0.6±0.4 in moderate LSCD, and 1.6±1.1 in severe LSCD (p<0.0001). There was a significant correlation between a higher clinical score and CDVA LogMAR (rho = 0.82; p<0.0001) and a greater decrease of BCD (rho = −0.78; p<0.0001).
Conclusion:
A clinical scoring system was developed to assess the extent of clinical presentation of LSCD. A classification system to grade the severity of LSCD can be established by combining the BCD score with the clinical score.
Keywords: Limbal Stem Cell Deficiency, limbal stem cell, classification system, in vivo confocal microscopy, diagnosis
INTRODUCTION
Corneal epithelial limbal stem cells maintain the integrity of the corneal surface, and they are located at basal layer of the limbal epithelium.1–3 Limbal stem cell deficiency (LSCD) is often present in many common ocular pathologic conditions such as multiple surgeries, drug toxicity, chronic inflammation, Stevens-Johnson syndrome, and chemical injury.
The diagnosis of LSCD is currently based mainly on history and clinical presentation. Clinical manifestations of LSCD vary in severity and extent of involvement. Classic clinical signs include stippling fluorescein staining, epithelial opacity or persistent late fluorescein staining in a vortex pattern, recurrent epithelial defects, and neovascularization of the corneal surface.4–6 However, these clinical signs can be subtle in LSCD and are not pathognomonic. In addition, these signs are seen in others conditions that do not have LSCD as a component. Moreover, at the time of presentation in patients with partial LSCD, very early and subtle changes can be missed by clinical examination alone.
Laboratory tests are helpful in confirming the diagnosis of LSCD. For many years, impression cytology has been the standard diagnostic test for LSCD,7 but the false-negative rate is high, mostly because the goblet cell deficiency seen in LSCD is also seen in many other co-existing conditions and sampling errors. Cytokeratins have been proposed as markers of conjunctival epithelial cells in the diagnosis of LSCD; however, the sensitivity of detection methods needs to be confirmed in larger clinical studies. Moreover, these tests are not quantitative of the degree of the LSCD.8,9
In vivo laser scanning confocal microscopy has been used to evaluate and quantify the microstructural changes of the corneal and limbal epithelium in eyes with different degrees of LSCD that was graded on the basis of clinical presentation.10–14 Significant microstructural changes associated with early LSCD and corneal basal epithelial cell density (BCD) and sub-basal nerve density were identified as potential parameters for the diagnosis and severity assessment of LSCD. Recently, our group has demonstrated that epithelium thickness, central cornea BCD, limbus BCD, and sub-basal nerve density are significantly decreased in eyes with LSCD and that the degree of reduction correlates with the severity of LSCD.15–17
To date, a scoring system to classify LSCD has not been established, in part because of a lack of a specific and quantitative diagnostic method for LSCD. In light of the new findings of quantifiable parameters for the characterization of LSCD severity, we investigated a possible correlation between the clinical grading and the central corneal BCD, and whether a system to grade the severity of LSCD based on clinical presentation and central cornea BCD was feasible.
MATERIALS AND METHODS
We conducted a retrospective, observational, cross-sectional, comparative study in a single center, which was approved by the Institutional Review Board at the University of California, Los Angeles (UCLA Institutional Review Board #10–001601). The described research adhered to the tenets of the Declaration of Helsinki, and the work is HIPAA-compliant. Appropriate consent was obtained before the initiation of the study.
The medical records of patients with the diagnosis of LSCD based on clinical presentation who were seen from 2010 to 2015 were reviewed. Impression cytology was performed in 25 subjects who gave permission for the test. Proper consent was obtained prior to the study. Each patient underwent a comprehensive eye examination, slit-lamp microscopy and photography, and in vivo laser scanning confocal microscopy. Impression cytology was performed for 13 patients who were willing to undergo the test to confirm the diagnosis of LSCD. Corrected distance visual acuity (CDVA) and images previously acquired by confocal imaging were reviewed. Nine eyes of 7 normal subjects without ocular disease as indicated by slit-lamp examination and without a history of ocular disease or ocular surgery were selected as the control group.
Confocal microscopy analysis:
Z-scan images were taken by the Heidelberg Retina Tomograph III Rostock Corneal Module Confocal Microscope (Heidelberg Engineering GmBH, Dossenheim, Germany). A minimum of 3 volume scans of the central cornea were collected. The volume scans with minimal motion artifacts were selected for analysis. The 3 image frames of the central cornea basal cell layer that best showed cellular morphology were selected. A defined area in the image was selected for cell count in the area without compression artifact if present. Each image frame was 400 × 400 μm. Two independent, masked observers then proceeded to measure central cornea BCD in all 3 images according to the protocol established by the manufacturer as previously reported.14 If there was a significant difference in BCD measured by the 2 observers, a third masked independent observer performed a third measurement, and only the 2 closest central cornea BCD measurements were used for the analysis.
Clinical scoring system and LSCD severity classification:
Two independent observers evaluated the clinical manifestations of LSCD ie, stippling or late fluorescein staining, fluorescein staining or epithelial opacity in a vortex pattern, epithelial defects, and vascularization of the cornea. A clinical scoring system to grade LSCD presentation was created on the basis of 3 criteria (Figure 1).
Figure 1:

Representative diagram of the limbal stem cell deficiency clinical grading system. Limbus involvement in clock hours (top panel), cornea surface area (middle panel) and visual axis involvement (bottom panel) criteria are shown. Slit lamp photo of an eye with a total score of 6 points, classified as the moderate stage of limbal stem cell deficiency (far right panel).
1). Limbus:
A score of 1 to 4 points was based on the extent of limbal involvement as follows: 1 point for limbal involvement extending from 1 to 3 clock hours, 2 points for limbal involvement extending from 4 to 6 clock hours, 3 points for limbal involvement from 7 to 9 clock hours, and 4 points for limbal involvement from 10 to 12 clock hours.
2). Cornea surface:
The cornea surface was divided into 4 areas that were perpendicular to the axis of greatest corneal involvement. A score of 1 to 4 was assigned to eyes with the corresponding number of areas that were affected.
3). Visual axis:
The visual axis area was defined as a central cornea area within 4-mm diameter. A score of 2 was assigned if the central visual axis was involved and 0 if it was not involved.
The total score was the sum of all points from the above 3 clinical criteria, (range of total scores, 2 to 10 points). The minimal score was 2, because a clinical diagnosis of LSCD requires the involvement of at least 1 clock hour of limbus and 1 cornea surface.
Based on the final score, the stages of LSCD was classified as mild (2 to 4 points), moderate (5 to 7 points), and severe (8 to 10 points) based on the clinical grading.
A reverse analysis based on the degree of BCD reduction to classify the degree of LSCD. The range in area between 0 to 8576 cells/mm2 was divided into 3 subgroups: mild BCD reduction (5501–8576 cells/mm2, n=22), moderate BCD reduction (2501–5500 cells/mm2, n=15), and severe BCD reduction (0–2500 cells/mm2, n=7). A score of 1, 2, and 3 was assigned to mild, moderate, and severe BCD reduction, respectively. A total revised final score was generated by adding the clinical grading and BCD grading.
Statistical analysis
Statistical analysis was performed with SAS software version 9.4 (SAS, Inc., Cary, NC). A p-value ≤ 0.05 was considered statistically significant. The differences in the mean values of continuous variables with a skewed distribution (e.g., age, BCD, CDVA in LogMAR) between patient subgroups were compared by the Kruskal-Wallis test, and the differences in the percentages of categorical variables between patient subgroups were compared by the Fisher exact test. Spearman correlation coefficient was used to investigate the potential correlation among the final clinical total score, BCVA and BCD.
RESULTS
Forty-eight eyes of 35 patients diagnosed with LSCD and 9 eyes of 7 normal patients were included in the study. According to the clinical score system that we applied to classify severity, LSCD was classified as mild in 18 eyes (38%), as moderate in 17 eyes (35%), and as severe in 13 eyes (27%).
Table 1 summarizes the patients’ demographic features. The median ages were 55.5 years (range, 24–94 years) for the patients with LSCD and 48.5 years (range, 27–88 years) for normal subjects in the control group. The mean age with standard deviation was listed in Table 1. There was no significant difference in age (p = 0.11) or gender (p = 0.49) between the control and LSCD groups. The leading etiologies of LSCD were contact lens wear (n=15; 31.3%), multiple ocular surgeries (n=13; 27.1%), drug toxicity (n=5; 10.4%), Stevens-Johnson syndrome (n=4; 8.3%), and chronic eye inflammation (n=4; 8.3%). The average final clinical score was 2.7±0.8 points (range, 2–4 points) for mild LSCD, 6.2±0.8 points (range, 5–7 points) for moderate LSCD, and 9.5±0.8 points (range, 8–10 points) for severe LSCD. Eyes with central clinical involvement had a higher mean clinical score (5.8±1.9) than did those without central involvement (3.2±1.2, p<0.0001), even when 2 points for central involvement were not added.
Table 1.
Demographic of Patients with Limbal Stem Cell Deficiency and Normal Controls.
| LSCD | Mild | Moderate | Severe | Control | P | |
|---|---|---|---|---|---|---|
| No. eyes (%) | 48 | 18 (38) | 17 (35) | 13 (27) | 9 | |
| Age (year), mean ± SD | 60.1 ± 19.7 | 49.1 ± 15.9 | 64.5 ± 21.3 | 69.6 ± 16.0 | 48.8 ± 20.1 | 0.11* |
| Gender | 0.49* | |||||
| Male, n (%) | 25 (52.1%) | 9 (50.0%) | 10 (58.8%) | 6 (46.2%) | 6 (66.7%) | |
| Female, n (%) | 23 (47.9%) | 9 (50.0%) | 7 (41.2%) | 7 (53.8%) | 3 (33.3%) | |
| Etiologies of limbal stem cell deficiency, n (%) | ||||||
| Contact lens | 15 (31.3%) | 9 (50.0%) | 5 (29.4%) | 1 (7.7%) | ||
| Multiple surgeries | 13 (27.1%) | 4 (22.2%) | 4 (23.5%) | 5 (38.5%) | ||
| Drug toxicity | 5 (10.4%) | 0 | 3 (17.6%) | 2 (15.4%) | ||
| Stevens-Johnson syndrome | 4 (8.3%) | 2 (11.1%) | 1 (5.9%) | 1 (7.7%) | ||
| Chronic inflammation | 4 (8.3%) | 1 (5.6%) | 2 (11.8%) | 1 (7.7%) | ||
| Mucous membrane pemphigoid | 3 (6.3%) | 1 (5.6%) | 1 (5.9%) | 1 (7.7%) | ||
| Chemical injury | 3 (6.3%) | 1 (5.6%) | 0 | 2 (15.4%) | ||
| Idiopathic | 1 (2.1%) | 0 | 1 (5.9%) | 0 |
Comparing LSCD to Controls
The mean central cornea BCD was 9252 ± 445 cells/mm2 (range, 8576–9948 cells/mm2) in the control group and 5387 ± 2798 cells/mm2 (range, 0–9472 cells/mm2) in the LSCD group (p < 0.0001). A number of zero was given when no cells were detected on the confocal image. When the mean BCD of the LSCD group (all with different clinical scores) was compared with that of the control group, there was a trend toward a decrease in BCD in the central cornea in eyes with higher clinical scores. When the BCD values of the LSCD severity subgroups were compared with the BCD of the control group, the central cornea BCD was reduced by 23.0% in the mild stage subgroup (7121 ± 1553 cells/mm2), 40.4% in the moderate stage subgroup (5512 ± 2171 cells/mm2), and 69.5% in the severe stage group (2821 ± 3050 cells/mm2) (p < 0.0001) (Table 2, Figure 2, left). Using the Spearman correlation coefficient, a higher total clinical score was found to significantly correlate with a decrease of central corneal BCD (rho = −0.78, p < 0.0001)
Table 2.
Central Cornea Basal Cell Density and Visual Acuity in Patients with Limbal Stem Cell Deficiency and Controls.
| LSCD | Mild | Moderate | Severe | Control | P* | |
|---|---|---|---|---|---|---|
| No. eyes (%) | 48 | 18 (38) | 17 (35) | 13 (27) | 9 | |
| Total score, mean ± SD | 5.8 ± 2.9 | 2.7 ± 0.8 | 6.2 ± 0.8 | 9.5 ± 0.8 | 0 ± 0 | <0.0001 |
| CDVA LogMAR, mean ± SD | 0.7 ± 0.9 N=43 |
0.2 ± 0.5 N=17 |
0.6 ± 0.4 N=14 |
1.6 ± 1.1 N=12 |
0.0 ±0.0 | <0.0001 |
| BCD (cells/mm2), mean ± SD | 5387 ± 2798 | 7121 ± 1553 | 5512 ± 2171 | 2821 ± 3050 | 9252 ± 445 | <0.0001 |
| BCD reduction (%) | 41.8 | 23.0 | 40.4 | 69.5 | ref. |
Kruskal-Wallis test; ref.: reference
Figure 2:
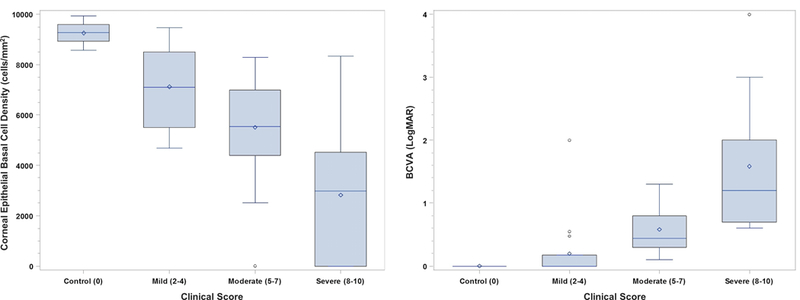
Box and whisker plot of the central cornea basal cell density (cells/mm2, left panel) and corrected distant visual acuity in LogMAR (right panel) in the control group and in patients with mild, moderate, and severe limbal stem cell deficiency. The central cornea basal cell density and corrected distant visual acuity in all patients with limbal stem cell deficiency was significantly less than that in the controls. Asterisk denotes P < 0.0001.
The central cornea BCD significantly decreased with more clock hours of limbal involvement. The mean BCD was 7111 ± 1492 cells/mm2 when 1 to 3 clock hours (n=17) of limbus were involved, 5554 ± 2275 cells/mm2 when 4 to 6 clock hours (n=16) were involved, 5835 ± 2057 cells/mm2 when 7 to 9 clock hours (n=6) were involved, and 1532 ± 2441 cells/mm2 when 10 to 12 clock hours (n=9) of limbus were involved (p < 0.0001).
The BCD also significantly decreased with more cornea surface areas affected. The mean BCD was 7488 ± 1589 cells/mm2 when 1 area (n=9) of cornea surface was involved, 6588 ± 1542 cells/mm2 when 2 areas (n=17) were involved, 4834 ± 2361 cells/mm2 when 3 areas (n=10) were involved, and 2567 ± 2967 cells/mm2 when 4 areas (n=12) were involved (p < 0.0001). Additionally, BCD was significantly less in eyes with visual axis involvement (4121 ± 2913 cells/mm2, n=27) than in eyes without involvement in the visual axis (7013 ± 1559 cells/mm2, n=21; p = 0.0005).
The superior limbus was the most commonly affected region (85.4% of eyes [41/48]), the inferior limbus was the next most commonly affected area (50% of eyes [24/48]), and the temporal and nasal limbus were least affected (48% of eyes [23/48]). When the limbal location that was affected was compared with the same region but unaffected in eyes with sectoral LSCD, we found a greater decrease of central cornea BCD if the affected quadrants were the inferior (affected inferior, 3974 ± 2670 cells/mm2, n=24; vs. unaffected, 6799 ± 2170 cells/mm2, n=24), the nasal (affected nasal, 4085 ± 2977 cells/mm2, n=23; vs. unaffected, 6583 ± 2023 cells/mm2, n=25), and the temporal quadrants (affected temporal, 4191 ± 2953 cells/mm2, n=23; vs. unaffected, 6486 ± 2170 cells/mm2, n=25) (p ≤ 0.005 for all comparisons). There was no difference between BCD in eyes that superior quadrant was involved (5396 ± 2977 cells/mm2, n=41) versus eyes with clinically normal superior quadrant (5330 ± 1492 cells/mm2, n=7; p=0.51).
The mean CDVA in LogMAR was 0.0 ± 0.0 in the control group and 0.7 ± 0.9 in the LSCD group. Visual acuity decreased with the severity of the disease to 0.2 ± 0.5 in the mild, 0.6 ± 0.4 in the moderate and 1.6 ± 1.1 in the severe stage group (p < 0.0001, Figure 2, right). Similar to that observed with BCD reduction, visual acuity significantly decreased with more clock hours of limbus involved, more areas of cornea surface affected and if the visual axis was involved (p < 0.0001 for all comparisons). Spearman correlation coefficient suggested that a higher total score significantly correlates with a decrease in visual acuity (rho = 0.82, p < 0.0001).
Receiver operating characteristic curve analysis of BCD in control subjects and those with LSCD revealed the lower cutoff value for BCD that signifies possible LSC dysfunction was 8576 cells/mm2, and the resulting sensitivity and specificity were 91.7% and 100%, respectively (Suppl Figure). Because BCD is a quantitative and more objective parameter of LSCD grading, we performed a reverse analysis based on the degree of BCD reduction to classify the degree of LSCD. The range in area between 0 to 8576 cells/mm2 was divided into 3 subgroups: mild BCD reduction (5501–8576 cells/mm2, n=22), moderate BCD reduction (2501–5500 cells/mm2, n=15), and severe BCD reduction (0–2500 cells/mm2, n=7). As shown in Table 3, 22% of eyes (4/18) that had a clinical score ≤4 (mild stage based on clinical grading) had a BCD that was within the normal range. Among 13 eyes that were classified having as severe LSCD by clinical examination (clinical score of 8–10), only 6 eyes had severe BCD reduction, and 3 eyes had mild BCD reduction.
Table 3.
Central Corneal Basal Cell Density and Clinical Scoring
| Clinical Grading | Normal (>8576 cells/mm2) |
Mild BCD Reduction (5501–8576 cells/mm2) |
Moderate BCD Reduction (2501–5500 cells/mm2) |
Severe BCD Reduction (≤ 2500 cells/mm2) |
Total |
|---|---|---|---|---|---|
| Control | 9 (100%) | 0 | 0 | 0 | 9 |
| Mild (2–4 points) | 4 (22%) | 9 (50%) | 5 (28%) | 0 | 18 |
| Moderate (5–7 points) | 0 | 10 (59%) | 6 (35%) | 1 (6%) | 17 |
| Severe (8–10 points) | 0 | 3 (23%) | 4 (31%) | 6 (46%) | 13 |
To increase the accuracy of the clinical scoring system to quantify the severity of LSCD, a score of 1, 2, and 3 was assigned to mild, moderate, and severe BCD reduction, respectively. If BCD was in the normal range, then a score of 0 was given. Representative confocal images of each confocal grade are shown in Figure 3. A new classification system in which the total scores were generated by the addition of the clinical scores and BCD scores was established. A total score of 2 to 5 indicated the mild stage of LSCD, a score of 6 to 9 indicated the moderate stage, and a score of 10 to 13 indicated the severe stage. With this new classification system, mild LSCD in one eye was reclassified as moderate LSCD, moderate LSCD in another eye was reclassified as severe LSCD, and severe LSCD in a third eye was reclassified as moderate LSCD.
Figure 3.

Representative confocal images of corneal basal epithelial cells in normal and limbal stem cell deficiency (LSCD). Basal epithelial cells are compact and have clear cell-cell junction in normal eye (top left panel). The size of the epithelial cells is slightly larger in LSCD with confocal grade 1 (top right panel) and cells became metaplastic in grade 2 (bottom left panel). In grade 3, cells with normal corneal epithelial cell morphology are not detected (bottom right panel).
DISCUSSION
Accurate diagnosis of LSCD can be very challenging because the clinical findings are often present in other corneal diseases. Other diseases could be mistaken as LSCD or the severity of LSCD could be misclassified based on clinical exam alone.18,19 It is important to ascertain the diagnosis of LSCD and its extent before considering treatment options if possible. Accurate staging of LSCD is important in monitoring disease progression and treatment outcomes.
Previous studies showed that a significant reduction in BCD was detected early in LSCD.14,15 Thus, BCD reduction in the central cornea is likely an early finding that suggests dysfunction of LSCs and could be used to assess the function of LSCs. In early sectoral LSCD, a similar degree of limbal BCD reduction was found in clinically affected and unaffected limbal region and a global thinning of the epithelium occurred in both the central cornea and limbus.15,16 These findings suggest that LSCs are affected globally in eyes with sectoral clinical presentation. These studies classified the degree of LSCD mainly on the basis of the fluorescein staining pattern (stippling versus late staining), the presence of corneal vascularization, and a prior history of recurrent corneal erosion. The extent of ocular surface involvement was not evaluated.
In the current study, we further refined the clinical grading system by including the extent of limbal and corneal involvement (Figure 1). Using this refined clinical scoring system, we reclassified LSCD as mild, moderate, and severe. The correlation of central corneal BCD, visual acuity, and LSCD severity graded by our new clinical grading system was investigated. We used central cornea BCD to validate the new clinical scoring system because BCD can be quantified more objectively with the same standard, and BCD measurements probably represent overall LSC function. Using this new clinical grading system, we found BCD was significantly decreased in eyes with more severe stages of LSCD. There is a significant correlation between the total clinical score and the degree of BCD reduction.
Our clinical scoring system appeared to be in agreement with BCD grading in a majority of the eyes. In eyes classified as having mild or moderate LSCD by the clinical scoring system, none in the mild category and only 1 eye (6%) in the moderate category had a level of BCD that was classified as severe LSCD (<2500 cells/mm2). Only 4 eyes classified as having mild LSCD and none in the moderate or severe stages as determined by the clinical scoring system had a BCD above the normal level (8576 cells/mm2).
We selected central visual axis involvement as one of the three clinical criteria in the clinical scoring system because we hypothesized that a larger area of central cornea involvement probably is correlated with a more severe level of LSC dysfunction/deficiency. This hypothesis was supported by our finding of a positive correlation between the total clinical score and the CDVA reduction. It is not surprising that CDVA was significantly decreased in the more advanced stage of disease because the likelihood of central cornea involvement is greater during severe disease. However, in eyes with other comorbidities, LSCD might not be the only cause of reduced vision. Therefore, visual acuity was not included in our clinical scoring system.
A slight decrease in limbal BCD in older age patients has been reported.20 More importantly, a decrease in central cornea BCD of 9% to 15% has been observed in patients with diabetic retinopathy and of 17% to 27% in patients with keratoconus.21–25 In our study, the average reduction in central cornea BCD is far greater in patients with LSCD (41.8%) than in patients with these other conditions. In addition, epithelial cell morphologic changes in keratoconus and diabetic retinopathy have not been reported. Therefore, we believe that this larger reduction of central cornea BCD in the current study is likely due to a generalized LSC dysfunction/deficiency. However, in the mild stage of LSCD, the average BCD reduction is 23%. Therefore, BCD reduction alone should not be used as the only diagnostic criterion for the mild stage of LSCD. In patients with mild LSCD, other parameters such as cell morphology, epithelial thickness, and subbasal nerve density are likely necessary to aid in the assessment of LSCD.
The leading etiologies of LSCD in the current study were contact lens wearing (31%) and multiple ocular surface surgeries (27%). The clinical presentation of corneal involvement in these two conditions can differ from the presentation by other conditions such as chemical burns or autoimmune diseases. In LSCD caused by contact lens wear and multiple ocular surgeries, superior limbus involvement is more frequent: in the present series it was affected in 85% of eyes, whereas about 50% of other limbal locations were affected. However, the fact that central cornea BCD was similar in eyes with affected and unaffected superior limbus suggests that, despite the different diagnoses among patients, a decrease in BCD is a phenomenon common to all eyes that have LSCD and is not limited to a specific condition that leads to LSCD. Also, the clinical scoring system proposed in this study consists of clinical examination of limbal and corneal areas; therefore, we believe that this clinical scoring method could be applied to LSCD due to conditions in addition to those we examined.
There are limitations of the study. The current proposed clinical scoring system is an initial attempt to assess the extent of clinical presentation. Although a good correlation between the clinical scoring system and more objective parameters, ie, the central cornea BCD and CDVA, was found, the clinical scoring system was not precise in all eyes. Three eyes that had a clinical grade of severe LSCD had only a mild reduction of central corneal BCD, a finding that suggests that LSC function was not severely compromised in these eyes. Therefore, clinical presentation of LSCD alone is not sufficient to quantify the degree of LSCD. A new classification system that combines the clinical scores and BCD reduction scores may more accurately quantify the severity of LSCD or LSC function. Other quantifiable parameters such as limbal BCD, subbasal nerve density, and epithelial thickness would be necessary to establish more accurate staging of LSCD.11,12,14–17 In future investigations, the classification system could be further refined by including these quantifiable parameters. A larger prospective study would be necessary to further validate the classification system.
In conclusion, there is a strong correlation between the clinical scoring system and two objective parameters, ie, central corneal BCD and CDVA. Clinical presentation alone has limitations of quantifying the degree of LSCD. A classification system can be established by combining central corneal BCD and clinical presentation to stage LSCD.
Supplementary Material
Acknowledgments
Funding disclosure: This study was supported by California Institute for Regenerative Medicine (CLIN1–08686) and in part by an unrestricted grant from Research to Prevent Blindness. SXD received grant support from the National Eye Institute (5P30EY000331 and 1R01EY021797). The funding organizations had no role in the design or conduct of this research.
Footnotes
Conflict of Interests: SXD is a consultant for Chiesi Farmaceutici S.p.A.; none of the authors have financial interests in the material discussed in the manuscript.
REFERENCES
- 1.Schermer A, Galvin S, Sun TT. Differentiation-related expression of a major 64K corneal keratin in vivo and in culture suggests limbal location of corneal epithelial stem cells. J Cell Biol. 1986;103:49–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lavker RM, Tseng SC, Sun TT. Corneal epithelial stem cells at the limbus: looking at some old problems from a new angle. Exp Eye Res.2004;78:433–446. [DOI] [PubMed] [Google Scholar]
- 3. Tseng SC. Concept and application of limbal stem cells. Eye (Lond).1989;3 ( Pt 2):141–157. [DOI] [PubMed] [Google Scholar]
- 4.Dua HS, Azuara-Blanco A. Limbal stem cells of the corneal epithelium. Surv Ophthalmol.2000;44:415–425. [DOI] [PubMed] [Google Scholar]
- 5.Dua HS, Gomes JA, Singh A. Corneal epithelial wound healing. Br J Ophthalmol.1994;78:401–408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Le Q, Xu J, Deng SX. The diagnosis of limbal stem cell deficiency. Ocul Surf.2018;16:58–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Puangsricharern V, Tseng SC. Cytologic evidence of corneal diseases with limbal stem cell deficiency. Ophthalmology.1995;102:1476–1485. [DOI] [PubMed] [Google Scholar]
- 8.Poli M, Burillon C, Auxenfans C, et al. Immunocytochemical Diagnosis of Limbal Stem Cell Deficiency: Comparative Analysis of Current Corneal and Conjunctival Biomarkers. Cornea.2015;34:817–823. [DOI] [PubMed] [Google Scholar]
- 9.Ramirez-Miranda A, Nakatsu MN, Zarei-Ghanavati S, et al. Keratin 13 is a more specific marker of conjunctival epithelium than keratin 19. Mol Vis.2011;17:1652–1661. [PMC free article] [PubMed] [Google Scholar]
- 10.Chidambaranathan GP, Mathews S, Panigrahi AK, et al. In vivo Confocal Microscopic Analysis of Limbal Stroma in Patients With Limbal Stem Cell Deficiency. Cornea.2015;34:1478–1486. [DOI] [PubMed] [Google Scholar]
- 11.Miri A, Alomar T, Nubile M, et al. In vivo confocal microscopic findings in patients with limbal stem cell deficiency. Br J Ophthalmol.2012;96:523–529. [DOI] [PubMed] [Google Scholar]
- 12.Nubile M, Lanzini M, Miri A, et al. In vivo confocal microscopy in diagnosis of limbal stem cell deficiency. Am J Ophthalmol.2013;155:220–232. [DOI] [PubMed] [Google Scholar]
- 13.Vera LS, Gueudry J, Delcampe A, et al. In vivo confocal microscopic evaluation of corneal changes in chronic Stevens-Johnson syndrome and toxic epidermal necrolysis. Cornea.2009;28:401–407. [DOI] [PubMed] [Google Scholar]
- 14.Deng SX, Sejpal KD, Tang Q, et al. Characterization of limbal stem cell deficiency by in vivo laser scanning confocal microscopy: a microstructural approach. Arch Ophthalmol.2012;130:440–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chan EH, Chen L, Rao JY, et al. Limbal Basal Cell Density Decreases in Limbal Stem Cell Deficiency. Am J Ophthalmol.2015;160:678–684 e674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chan EH, Chen L, Yu F, et al. Epithelial Thinning in Limbal Stem Cell Deficiency. Am J Ophthalmol.2015;160:669–677 e664. [DOI] [PubMed] [Google Scholar]
- 17.Chuephanich P, Supiyaphun C, Aravena C, et al. Characterization of the Corneal Subbasal Nerve Plexus in Limbal Stem Cell Deficiency. Cornea.2017;36:347–352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Le Q, Samson CM, Deng SX. A Case of Corneal Neovascularization Misdiagnosed as Total Limbal Stem Cell Deficiency. Cornea.2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chan E, Le Q, Codriansky A, et al. Existence of Normal Limbal Epithelium in Eyes With Clinical Signs of Total Limbal Stem Cell Deficiency. Cornea.2016;35:1483–1487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Patel DV, Sherwin T, McGhee CN. Laser scanning in vivo confocal microscopy of the normal human corneoscleral limbus. Invest Ophthalmol Vis Sci.2006;47:2823–2827. [DOI] [PubMed] [Google Scholar]
- 21.Bitirgen G, Ozkagnici A, Bozkurt B, et al. In vivo corneal confocal microscopic analysis in patients with keratoconus. Int J Ophthalmol.2015;8:534–539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mocan MC, Yilmaz PT, Irkec M, et al. In vivo confocal microscopy for the evaluation of corneal microstructure in keratoconus. Curr Eye Res.2008;33:933–939. [DOI] [PubMed] [Google Scholar]
- 23.Cai D, Zhu M, Petroll WM, et al. The impact of type 1 diabetes mellitus on corneal epithelial nerve morphology and the corneal epithelium. Am J Pathol.2014;184:2662–2670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chang PY, Carrel H, Huang JS, et al. Decreased density of corneal basal epithelium and subbasal corneal nerve bundle changes in patients with diabetic retinopathy. Am J Ophthalmol.2006;142:488–490. [DOI] [PubMed] [Google Scholar]
- 25.Quadrado MJ, Popper M, Morgado AM, et al. Diabetes and corneal cell densities in humans by in vivo confocal microscopy. Cornea.2006;25:761–768. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.