

Abstract
Aims and Objectives:
The parent's oral health knowledge has a great influence on their children, so the aim of the study was to estimate the parental knowledge about oral health care and its influence in maintaining the diet and hygiene practices on their children and also to access how the demographic variables will influence them in taking their child to dental visits.
Materials and Methods:
The self-administered pretested questionnaire was distributed among Saudi parents whose children are in the age group of 2–6 years vising primary health care centers (PHCCs) in Riyadh city. The PHCCs were divided into five zones (Central, East, West, South, and North). 240–250 samples were randomly selected from each zone to reach the prescribed sample size of 1200. The survey will be composed of self-administered pretested questionnaires seeking for age, gender, educational level, and their financial status followed by 26 questions related to parent knowledge about oral health (14), dietary (5), and hygiene (7) practices what they implement on their child. The data collected were analyzed using SPSS software SPSS 25.0 (SPSS, Inc., Chicago, IL, USA).
Results:
Demographic information showed that the average age of the parents who participated in the study is 32.2 years. The mothers were 942 (75.7%) and fathers were 303 (24.3%) among the participants. The mean knowledge score among the mothers (34.85) is slightly greater than fathers (34.76). Similar results with dietary and hygiene practices were not statistically significant (>0.05). The parents having more than one child have better knowledge, of which the parents with more than three children have better scores, which is statistically significant. 69.3% of the parents prefer taking to a dentist only when they have a problem. Moreover, these findings found to be statistically significant (P < 0.05).
Conclusion:
Parents should get access to oral health knowledge to put in practice on their children so as to influence them in gaining better oral health.
KEYWORDS: Dental visits, dietary practices, hygiene practices, oral health knowledge
INTRODUCTION
Children, though dependent on parents, have every right to enjoy high standard of health including the oral health.[1] The children develop their daily proficiency from their parents, thereby improving their day-by-day skills from them.[2] Children younger than 6 years generally put in much of their time with their parents and caregivers even though they go to preschool. These early years include “primary socialization,” from which their daily routines (dietary and hygiene practices) are achieved. These routines which acquired from their parents or care givers improve their general well-being, specifically the dietary and hygiene practices to develop the good oral health care habits. This acquiring knowledge by the child depends on the knowledge of the parents.[2,3,4] In the present world, most of the parents are getting educated because of various community programs conducted in their respective countries. Furthermore, in Saudi Arabia, The Dental Directorate, Ministry of Saudi Arabia, organized many public oral health programs such as “Community Oral Health Education” and “Oral Health Weeks” to educate the population particularly the parents so as to improve their daily routines.
Consistently visiting the dentist will allow us to prevent various forthcoming issues related to teeth making ourselves to move toward a positive oral health.[5,6] Unfortunately, rather than combination of prevention and dental visits, it has become the combination of pain and dental visits which in turn prevents us from going to a dentist because of painful visits. This can be avoided by adequate monitoring by the dentists and motivation of the parents to attain a painless regular visits.[6]
We hypothesize that dietary and hygiene practices are in direct relation to parental knowledge on oral health.
Our aim of the study was to assess the oral health knowledge and how they influence the oral health habits (dietary and hygiene practices) on their children and also how the demographic variables will influence them in taking their child to dental visits.
MATERIALS AND METHODS
Questionnaire method was selected as it may provide chance to cover large group of population. However, there are more chances that questions can be misinterpreted because of subjective variation. To overcome this, direct interview or face-to-face interview method was chosen to make the participants answer effectively.[7,8]
STUDY POPULATION AND SETTING
The study was conducted in primary health care centers (PHCCs) in Riyadh city among the Saudi nationals after approval from the IRB (IRB No: RC/IRB/2018/1067) Riyadh Elm University during July 2018. The services in PHCCs are totally free and around 99% of every Saudi national would register officially within the nearest allotted PHCCs. A simple random sampling was employed for selection of participants according to al-Doghaither et al.[9] where the PHCCs are divided into five zones (Central, East, West, South, and North). It was planned in such a way that the sample size of approximately 245–250 were selected by simple random sampling from each zone so as to reach the prescribed sample size of 1200 which was calculated according to using a level of precision formula (n = z2 pq/d2). To overcome certain rejections, our target was marginally increased to get more than the prescribed sample size and finally managed to achieve a sample size of 1245 which was ahead of the sample needed.
Inclusion criteria were Saudi parents whose children are in the age of 2–6 years and are mentally and physically stable to answer the questionnaire. Exclusion criteria were those participants not adhering to the above limits, which includes the parents who are not Saudi nationals and those not having a child between 2 and 6 years of age. Furthermore, the parents who are by anyway related to dentistry such as dentists or dental hygienists are excluded for this research.
STUDY INSTRUMENT
The survey will be composed of self-administered pre-tested questionnaires[2,10,11] seeking for age, gender, educational level, and their financial status followed by 26 questions related to parent knowledge about oral health,(14) dietary (5), and hygiene (7) practices what they implement on their child.
This pretested questionnaire for the easy understanding to the local population was translated to Arabic by Arabic native speaker who is able to speak both English and Arabic. Later, it was back-translated to English by another bilingual native Arabic speaker. This translated English questionnaire was compared with original English questionnaire. Through these continuous cycles, we could manage to get the original meaning in Arabic language. A pilot study was done out utilizing this bilingual instrument to ensure equivalence, clarity, and comprehension. This method of validation was similar to the one done by Kotha et al.[12] Consent was provided to all participants’ before answering the questionnaires.
Data collection
A brief description of the questionnaire was given to the participants to enable them to answer appropriately.
Data management
Basic demographic data of the parents who participated was asked to answer about their gender, educational and financial status, and number of children they have were collected.
PARENTAL KNOWLEDGE
The designed questionnaire included 14 questions to assess the knowledge of the parents regarding oral health. Three possible responses yes (counted as score 3), may be (counted as score 2), and no (counted as score 1) were used for these 14 questions. Hence, the possible total scores ranged from 14 to 42. Higher the score indicates better knowledge regarding the oral health among the participants.
DIETARY AND HYGIENE PRACTICES
The dietary and hygiene practices part of the questionnaire has five questions each. Three possible responses ranged from always (counted as score 3), sometimes (counted as score 2), to rarely (counted as score 1). Scores ranged between 5 and 15 for both dietary and hygiene practices. Higher the score indicates better dietary and hygiene practices followed by parents toward their children.
STATISTICAL ANALYSIS
After computing the cumulative score, the reliability of the questionnaire was examined using Cronbach's alpha and it was 0.82, 0.87, and 0.85 for knowledge, dietary, and hygiene practices, respectively, which was considered a good level of reliability. The data collected were analyzed using SPSS software SPSS 25.0 (SPSS, Inc., Chicago, IL, USA). Descriptive statistics were used to show the participants’ demographics, and independent sample t-test was used to analyze between the parents (mothers and fathers) with their knowledge, dietary, and hygiene practices. One-way ANOVA for the other demographic factors was to analyze the relationship with the parental practices followed by post hoc analysis to analyze the influence within the intragroup demographic mean variables. Chi-square analysis was done to assess how the child was taken to a dentist in relation to demographic variables. Pearson correlation was used to correlate among these parental knowledge and their practices to estimate the interrelationships within themselves.
RESULTS
Demographic information showed that the average age of the parents who participated in the study is 32.2 years. The mothers were 942 (75.7%) and fathers 303 (24.3%) among the participants.
Table 1 shows the relationship between the demographic factors with the means of oral health care factors (parental knowledge, dietary, and hygiene practices). The mean knowledge score among the mothers (34.85) is slightly greater than fathers (34.76), which was not statistically significant. The dietary and the hygiene practice scores follow the same where mothers are slightly more than the fathers without any statistically significance between them.
Table 1.
Relationship between the demographic factors with knowledge, dietary, and hygiene practices
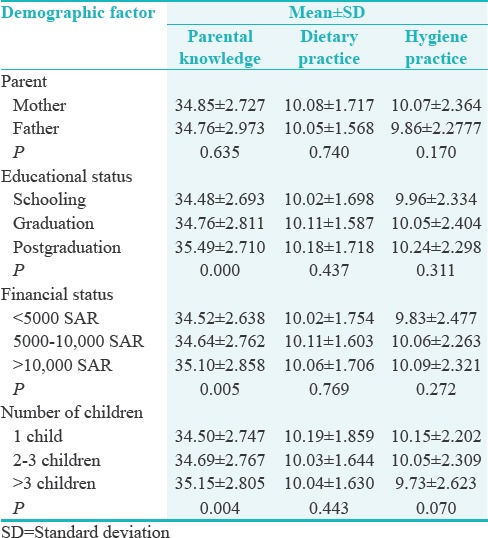
The education status in relation to the knowledge about oral health showed that the knowledge score is more in parents who have done higher studies and is highly significant statistically (<0.001). The dietary and hygiene practice scores though more in parents with good education are not significant statistically (P > 0.05).
Financial status showed that both the scores of parental knowledge and hygiene practices are more in participants having the greater earning with significant relation with knowledge score (P = 0.005) but not the hygiene practice score (P = 0.272). Participants earning between 5000 and 10,000 SAR are more keen on dietary practice and so the score, though not statistically significant in relation to groups with either extremes of their financial status.
The parents with more children have the highest knowledge score and are significant (P < 0.05) with converse scores for dietary and hygiene practice though not statistically significant.
Table 2 shows the post hoc analysis of the parental knowledge scores within the groups of demographic variables. After identifying the significance between the three groups, post hoc gives the significance within the groups separately like in the table given. For example, parental knowledge showed the significance between the education groups as in Table 1. Table 2 shows the significance in specific between parents who did graduation and postgraduation than that of parents with school education. Similarly, among the groups with financial status, the parents earning between 5000 and 10,000 SAR have significant relation though less oral health knowledge scores than with parents earning >10,000 SAR. The parents having more than one child have better knowledge, of which the parents with more than three children, and is statistically significant.
Table 2.
Post hoc analysis of the parental knowledge scores within the groups of demographic variables

Table 3 gives the preference of taking to a dentist in relation to demographic factors. 69.3% of the parents prefer taking to a dentist only when they have a problem. 27.5% unfortunately do not prefer going to a dentist. These findings found be significant (P < 0.05). More than half of the participants (69.2%) take their children only if they have a problem irrespective of their educational status and the results found to be significant. Similar results for other demographic factors, financial status (68.6%) and number of children (69%) though statistically not significant (>0.05).
Table 3.
Demographic factors in relation to preference of taking to a dentist
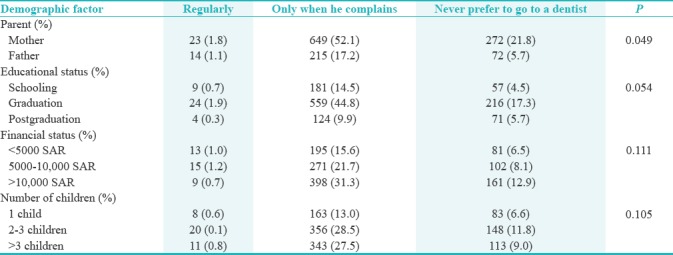
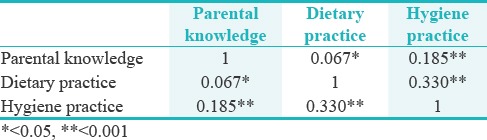
Table 4 gives the Pearson correlation among these three oral health score components, i.e., within parental knowledge, dietary, and hygiene practice scores. The parents with good knowledge follow better dietary practice on their children which is significant (P < 0.05) and highly significant with hygiene practice aspect (P < 0.001). The parents who follow good dietary practice for their children will also concentrate more on hygiene practice, which is statistically highly significant (P < 0.001).
Table 4.
Pearson correlation among three oral health score components
DISCUSSION
Oral health literacy is how much people have the ability to acquire, process, and comprehend fundamental oral health data and services expected to settle on achieving proper health resources.[13,14] Any decrease in the oral health knowledge among the parents will influence in maintaining diet and hygiene practices within their children.[15,16] There are various associated components with decreased knowledge and poor attitudes among the parents such as low socioeconomic status,[13,17,18,19] living in impoverished areas,[13,15,20] ethnicity or immigrant status,[13,15,21] lack of further education,[13,15,22] high caries status in the children,[13,22] and difficult past dental experience,[13,23] so this research was planned how much interest the Saudi parents have toward their children. The results obtained from the present survey clearly gives a view that the parental knowledge and their attitudes toward themselves about oral health have a greater influence on their children.[24,25,26,27,28,29] Within the parents, mothers definitely have a major role and more often they being the role model to their children. It is usually the mother who has more knowledge compared to fathers regarding their child's oral health and our results conclude the same but not statistically significant, unlike previous studies.[24,25,26,27]
The education status in relation to the knowledge about oral health is usually directly related where in which our study showed similar results and is statistically significant conveying that higher studies would influence the oral health knowledge.[27] There is one previous study done in Mexican mothers who are less in their education results in reduced knowledge and hence the parental practices.[30] Similar results are also from the previous studies.[15,22,26] It has been recommended that the parents with a general, enhanced level of education may be able to collect the information from the relevant source and can comprehend the knowledge completely.[26,31] One of the fundamental factors that may give some thoughts regarding parental knowledge about oral health is the frequency of dental visits that educated mothers do take their children regularly to a dentist.[20] A study by Al-Zahrani et al., 2014[32] only 22% of the parents agreed that the child was taken to a dentist only if they have dental problem but not regularly. Contradictory results in our study show that 54.7% mothers take their children but only when they complain in spite of being educated with statistically significant results. The results in the present study confirmed that educated parents with better financial status follow better parental practices as in other studies.[15,28,33,34,35,36,37] It was also found that many studies conducted in various countries have concluded that parents with low educational status with lower income levels were important indicators for the parental practices (dietary and hygiene) among their children.[3,38] In conclusion, the postulated theory for this could be that reduced education status reduces the financial status which resulted in limited access to the dentists on a regular basis.[39,40] Conflicting studies in the previous research show that parents irrespective of their educational or financial status do not prefer taking their child to the dentist due to multiple reasons which include expensive, ignorance, lack of access to dental care or even their past painful experience in the dental setting.[41,42] These are some of the reasons which developed the concept of “dental neglect” which was defined as “the failure by a parent or guardian to seek treatment for visually untreated caries, oral infections and pain; or failure of the parent or guardian to follow through with treatment once informed that the above condition(s) exists.”[41,43]
Although in Saudi Arabia in spite having wide range of health-care system to the locals such as providing free dental health care to the citizens in the Ministry of Health, there is no requirement for dentists to encourage the recall visits for the patients. This makes the patients being irregular visiting only when in pain leading to painful visits for children. Public health experts now suggest to encourage dentists to recall children regularly and also conduct camps regularly in schools to overcome fear among the dentists so that the regular visits can be improved.[6]
Parents having more than one child prefer taking to a dentist without negligence probably they faced the consequences with the first child suffering.[34] Antithetical results can be seen in our study by not visiting the dentist regularly because managing many children by only mother makes it irregular which can be overcome here in Saudi Arabia because most of the families hire maids to handle children.
The hygiene practices and the decisions of parents, especially the mothers, are specifically connected with those of their children. Dentists always acknowledge that endeavors went for enhancing parental oral health care practices could result in improving the oral health for their children. Anyway, various variables have been determined that would affect the mother's care affecting the child's oral health. Some of them include mother's education, age, occupation, present knowledge, and their attitude towards oral health.[44]
The parents with good oral health knowledge would have an eye on the diet given to their child and hence the hygiene practices which all of them are directly proportional among themselves.[13] Our results also gave similar results being directly proportional and also statistically significant.
Previous methodical reviews[45,46] and even in recent researches,[11,47,48] it was proved that upgrading the knowledge on oral health among the parents and caregivers would certainly enhance the oral hygiene practices in their children and this can be accomplished by conducting various oral health educational programs.
As hypothesized, the primary outcome which measured parental knowledge confirmed in our research that this would influence their children as they being the role models would transfer the values, norms, and demeanor that are accepted for their children. The secondary outcomes include the dietary and hygiene practices could be viably accomplished and are directly related to parental knowledge. This direct relationship between primary and secondary outcomes was demonstrated in our research [Table 4] that parental knowledge is the utmost important. Hence, the school settings ought to give chance for the parents as in school gatherings, community meetings, and oral health services to improve oral health knowledge among parents.
The conclusions of the present research may give a perspective of the link between parents’ attitudes and their children's oral health; however, there are a few constraints in light of the fact that the investigation is cross-sectional and the sample is not substantial, just by considering only parents visiting the PHCCs. There are additional issues identified in understanding this survey. For instance, in spite of the major participants having finished their secondary school, there are some who were uneducated or had only few years of study. Recollecting bias, in answering to the questionnaire, may likewise have been confinement.[28]
The findings in the present research have evolved to give rise to new questions where we need to answer in the forthcoming researches such as relating the parental knowledge and their practices with the child's oral health status to understand how parents are applying their knowledge into practice. Researches should change the perceptions of parents and caregivers about the oral health importance to aid in reducing the oral health problems in the future generation.
CONCLUSION
As it was evidenced by this and many other previous studies, educating the parents improved their child's oral health. It would be more fruitful to educate mother to-be individuals regarding oral health care and its maintenance so that the next generation is handled in a systematic way. This can be achieved by concentrating at the grassroots level by conducting various educational programs among the parents to achieve a major goal.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
Acknowledgments
The authors thank Dr. Avidapu Rajshekhar for helping us in statistics. We also thank all the parents who cooperated for our study.
REFERENCES
- 1.World Health Organization. Basic Documents. 39th ed. Geneva: World Health Organization; 1992. [Google Scholar]
- 2.ElKarmi R, Shore E, O’Connell A. Knowledge and behaviour of parents in relation to the oral and dental health of children aged 4-6 years. Eur Arch Paediatr Dent. 2015;16:199–204. doi: 10.1007/s40368-014-0155-7. [DOI] [PubMed] [Google Scholar]
- 3.Prabhu A, Rao AP, Reddy V, Ahamed SS, Muhammad S, Thayumanavan S, et al. Parental knowledge of pre-school child oral health. J Community Health. 2013;38:880–4. doi: 10.1007/s10900-013-9693-x. [DOI] [PubMed] [Google Scholar]
- 4.Naidu RS, Davis L. Parents’ views on factors influencing the dental health of Trinidadian pre-school children. Community Dent Health. 2008;25:44–9. [PubMed] [Google Scholar]
- 5.Badri P, Saltaji H, Flores-Mir C, Amin M. Factors affecting children's adherence to regular dental attendance: A systematic review. J Am Dent Assoc. 2014;145:817–28. doi: 10.14219/jada.2014.49. [DOI] [PubMed] [Google Scholar]
- 6.AlHumaid J, El Tantawi M, AlAgl A, Kayal S, Al Suwaiyan Z, Al-Ansari A. Dental visit patterns and oral health outcomes in Saudi children. Saudi J Med Med Sci. 2018;6:89–94. doi: 10.4103/sjmms.sjmms_103_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Grinyer P. Survey methods in social investigation. J Oper Res Soc. 1973;24:148. [Google Scholar]
- 8.Szolnoki G, Hoffmann D. Online, face-to-face and telephone surveys-comparing different sampling methods in wine consumer research. Wine Econ Policy. 2013;2:57–66. [Google Scholar]
- 9.al-Doghaither AH, Abdelrhman BM, Saeed AA, Magzoub ME. Factors influencing patient choice of hospitals in Riyadh, Saudi Arabia. J R Soc Promot Health. 2003;123:105–9. doi: 10.1177/146642400312300215. [DOI] [PubMed] [Google Scholar]
- 10.Wapniarska K, Buła K, Hilt A. Parent's pro-health awareness concerning oral health of their children in the light of survey research. Przegl Epidemiol. 2016;70:59. [PubMed] [Google Scholar]
- 11.Pan N, Cai L, Xu C, Guan H, Jin Y. Oral health knowledge, behaviors and parental practices among rural-urban migrant children in Guangzhou: A follow-up study. BMC Oral Health. 2017;17:97. doi: 10.1186/s12903-017-0385-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kotha SB, Chaudhary M, Terkawi S, Ahmed M, Ghabban SN, Fernandez RAA, et al. Correlation of perceived self-rated oral health status with various dental health and awareness factors. J Int Soc Prev Community Dent. 2017;7:S119–24. doi: 10.4103/jispcd.JISPCD_304_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mani SA, John J, Ping WY, Ismail N. Early childhood caries: Parents knowledge, attitude and practice towards its prevention in Malaysia. In: Mandeep V, editor. In Oral Health Care: Pediatric, Research, Epidemiology and Clinical Practices. Guildford, UK: In Tech; 2012. [Google Scholar]
- 14.Firmino RT, Ferreira FM, Paiva SM, Granville-Garcia AF, Fraiz FC, Martins CC, et al. Oral health literacy and associated oral conditions: A systematic review. J Am Dent Assoc. 2017;148:604–13. doi: 10.1016/j.adaj.2017.04.012. [DOI] [PubMed] [Google Scholar]
- 15.Williams NJ, Whittle JG, Gatrell AC. The relationship between socio-demographic characteristics and dental health knowledge and attitudes of parents with young children. Br Dent J. 2002;193:651–4. doi: 10.1038/sj.bdj.4801652. [DOI] [PubMed] [Google Scholar]
- 16.Chala S, Houzmali S, Abouqal R, Abdallaoui F. Knowledge, attitudes and self-reported practices toward children oral health among mother's attending maternal and child's units, Salé, Morocco. BMC Public Health. 2018;18:618. doi: 10.1186/s12889-018-5542-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.National Academies of Sciences, Engineering, and Medicine. Parenting Matters: Supporting Parents of Children Ages 0.8. Washington, DC: National Academies Press; 2016. [PubMed] [Google Scholar]
- 18.Dykes J, Watt RG, Nazroo J. Socio-economic and ethnic influences on infant feeding practices related to oral health. Community Dent Health. 2002;19:137–43. [PubMed] [Google Scholar]
- 19.Finlayson TL, Siefert K, Ismail AI, Sohn W. Maternal self-efficacy and 1-5-year-old children's brushing habits. Community Dent Oral Epidemiol. 2007;35:272–81. doi: 10.1111/j.1600-0528.2007.00313.x. [DOI] [PubMed] [Google Scholar]
- 20.Silver DH. A comparison of 3-year-olds’ caries experience in 1973, 1981 and 1989 in a Hertfordshire town, related to family behaviour and social class. Br Dent J. 1992;172:191–7. doi: 10.1038/sj.bdj.4807819. [DOI] [PubMed] [Google Scholar]
- 21.Skaret E, Espelid I, Skeie MS, Haugejorden O. Parental beliefs and attitudes towards child caries prevention: Assessing consistency and validity in a longitudinal design. BMC Oral Health. 2008;8:1. doi: 10.1186/1472-6831-8-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Szatko F, Wierzbicka M, Dybizbanska E, Struzycka I, Iwanicka-Frankowska E. Oral health of polish three-year-olds and mothers’ oral health-related knowledge. Community Dent Health. 2004;21:175–80. [PubMed] [Google Scholar]
- 23.Tickle M, Milsom KM, Humphris GM, Blinkhorn AS. Parental attitudes to the care of the carious primary dentition. Br Dent J. 2003;195:451–5. doi: 10.1038/sj.bdj.4810600. [DOI] [PubMed] [Google Scholar]
- 24.Chan SC, Tsai JS, King NM. Feeding and oral hygiene habits of preschool children in Hong Kong and their caregivers’ dental knowledge and attitudes. Int J Paediatr Dent. 2002;12:322–31. doi: 10.1046/j.1365-263x.2002.00389.x. [DOI] [PubMed] [Google Scholar]
- 25.Nagarajappa R, Kakatkar G, Sharda AJ, Asawa K, Ramesh G, Sandesh N, et al. Infant oral health: Knowledge, attitude and practices of parents in Udaipur, India. Dent Res J (Isfahan) 2013;10:659–65. [PMC free article] [PubMed] [Google Scholar]
- 26.Suresh BS, Ravishankar TL, Chaitra TR, Mohapatra AK, Gupta V. Mother's knowledge about pre-school child's oral health. J Indian Soc Pedod Prev Dent. 2010;28:282–7. doi: 10.4103/0970-4388.76159. [DOI] [PubMed] [Google Scholar]
- 27.Suma Sogi HP, Hugar SM, Nalawade TM, Sinha A, Hugar S, Mallikarjuna RM, et al. Knowledge, attitude, and practices of oral health care in prevention of early childhood caries among parents of children in Belagavi city: A Questionnaire study. J Family Med Prim Care. 2016;5:286–90. doi: 10.4103/2249-4863.192332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Garbin CA, Soares GB, Dócusse GF, Garbin AJ, Arcieri RM. Oral health education in school: Parents’ attitudes and prevalence of caries in children. Rev Odontol UNESP. 2015;44:285–91. [Google Scholar]
- 29.Abiola Adeniyi A, Eyitope Ogunbodede O, Sonny Jeboda O, Morenike Folayan O. Do maternal factors influence the dental health status of Nigerian pre-school children? Int J Paediatr Dent. 2009;19:448–54. doi: 10.1111/j.1365-263X.2009.01019.x. [DOI] [PubMed] [Google Scholar]
- 30.Hoeft KS, Barker JC, Shiboski S, Pantoja-Guzman E, Hiatt RA. Effectiveness evaluation of contra caries oral health education program for improving Spanish-speaking parents’ preventive oral health knowledge and behaviors for their young children. Community Dent Oral Epidemiol. 2016;44:564–76. doi: 10.1111/cdoe.12250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Khanduri N, Singhal N, Mitra M, Rohatgi S. Knowledge, attitude, and practices of parents toward their children and #39;s oral health: A questionnaire survey in Bhairahawa (Nepal) Int J Pedod Rehabil. 2018;3:59–61. [Google Scholar]
- 32.Al-Zahrani AM, Al-Mushayt AS, Otaibi MF, Wyne AH. Knowledge and attitude of Saudi mothers towards their preschool children's oral health. Pak J Med Sci. 2014;30:720–4. doi: 10.12669/pjms.304.5069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kumar G, Singh DK, Jalaluddin M, Dileep CL, Rout P, Mohanty R, et al. Oral health of pre-school aged children in Dhanbad district, Jharkhand, India – A peek into their mother's attitude. J Clin Diagn Res. 2013;7:2060–26. doi: 10.7860/JCDR/2013/6858.3405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Amin MS, Perez A, Nyachhyon P. Parental awareness and dental attendance of children among African immigrants. J Immigr Minor Health. 2015;17:132–8. doi: 10.1007/s10903-013-9912-7. [DOI] [PubMed] [Google Scholar]
- 35.Shaghaghian S, Savadi N, Amin M. Evaluation of parental awareness regarding their child's oral hygiene. Int J Dent Hyg. 2017;15:e149–55. doi: 10.1111/idh.12221. [DOI] [PubMed] [Google Scholar]
- 36.Nazari Z, Taherpour M. mothers’ awareness, regarding orodental health of their children at age of 1-6 years old in shirvan. J North Khorasan Univ Med Sci. 2013;5:979–86. [Google Scholar]
- 37.Naderifar M, Akbarsharifi T, Pairovi H, Haghani H. Mothers’ awareness, regarding orodental health of their children at age of 1-6 years old. Iran J Nurs. 2006;19:15–27. [Google Scholar]
- 38.Bozorgmehr E, Hajizamani A, Malek Mohammadi T. Oral health behavior of parents as a predictor of oral health status of their children. ISRN Dent 2013. 2013:741783. doi: 10.1155/2013/741783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Mishra A, Pandey RK, Chopra H, Arora V. Oral health awareness in school-going children and its significance to parent's education level. J Indian Soc Pedod Prev Dent. 2018;36:120–4. doi: 10.4103/JISPPD.JISPPD_1172_17. [DOI] [PubMed] [Google Scholar]
- 40.Van den Branden S, Van den Broucke S, Leroy R, Declerck D, Hoppenbrouwers K. Effects of time and socio-economic status on the determinants of oral health-related behaviours of parents of preschool children. Eur J Oral Sci. 2012;120:153–60. doi: 10.1111/j.1600-0722.2012.00951.x. [DOI] [PubMed] [Google Scholar]
- 41.Fisher-Owens SA, Lukefahr JL, Tate AR. American Academy of Pediatrics, Section on Oral Health, Committee on Child Abuse and Neglect, American Academy of Pediatric Dentistry, Council on Clinical Affairs, Council on Scientific Affairs, et al. Oral and dental aspects of child abuse and neglect. Pediatrics. 2017;140:pii: e20171487. [PubMed] [Google Scholar]
- 42.Merdad L, El-Housseiny AA. Do children's previous dental experience and fear affect their perceived oral health-related quality of life? BMC Oral Health. 2017;17:47. doi: 10.1186/s12903-017-0338-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.American Academy of Pediatric Dentistry Definition of Dental Neglect. [Last accessed on 2016 May 23]. Available from: http://www.aapd.org/policies/
- 44.Oredugba F, Agbaje M, Ayedun O, Onajole A. Assessment of mothers’ oral health knowledge: Towards oral health promotion for infants and children. Health. 2014;6:908–15. [Google Scholar]
- 45.Nakre PD, Harikiran AG. Effectiveness of oral health education programs: A systematic review. J Int Soc Prev Community Dent. 2013;3:103–15. doi: 10.4103/2231-0762.127810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Stein C, Santos NM, Hilgert JB, Hugo FN. Effectiveness of oral health education on oral hygiene and dental caries in schoolchildren: Systematic review and meta-analysis. Community Dent Oral Epidemiol. 2018;46:30–7. doi: 10.1111/cdoe.12325. [DOI] [PubMed] [Google Scholar]
- 47.Mahat G, Bowen F. Parental knowledge about urban preschool children's oral health risk. Pediatr Nurs. 2017;43:30–4. [PubMed] [Google Scholar]
- 48.Dinea SD, Domnariu CD. Evaluation of parental knowledge about oral health of a preschool children population. Acta Med Transilvanica. 2017;22:6–8. [Google Scholar]