

Abstract
Aims and Objectives:
This research is intended to observe the influence of menopause on saliva and dental health. Salivary flow rate, pH of stimulated whole saliva, oral hygiene status, dental caries status, and periodontal status were evaluated in frequently menstruating and postmenopausal womankind.
Materials and Methods:
A cross-sectional study was conducted on forty healthy postmenopausal women (case group) and forty regularly menstruating healthy women (control group), who were selected from the Outpatient Department of Dr. Syamala Reddy Dental College and Hospital, Bengaluru. None of them had any systemic disease and not under any medication. Participants were asked to chew on an elastic band of standardized size. The flow rate was measured as ml/min. Salivary pH was measured using pH strips. Oral Hygiene Index-simplified (OHI-S), Decayed Missing and Filled Teeth (DMFT index), Community Periodontal Index (CPI), and Loss of Attachment (LOA) were assessed clinically. The results were analyzed with the Chi-square test and Student's t-test (P < 0.05).
Results:
Salivary pH and flow rate in the case cluster were considerably lesser when related to the control group (P < 0.001). OHI-S, DMFT, CPI, and LOA were found to be greater in postmenopausal women when related to the control group (P < 0.001).
Conclusion:
Here exists a noticeable diminution in the salivary pH and flow rate in postmenopausal womanhood which in turn leads to increased OHI-S, DMFT, CPI, and LOA. The study has presented that the significance of preventive dentistry upsurges with aging in females.
KEYWORDS: Decayed Missing and Filled Teeth, postmenopause, salivary flow rate
INTRODUCTION
It has been observed that life expectancy of women has increased significantly during the last decade, and most women spend one third of their lives after menopause1.[1] Menopause (as defined by the World Health Organization) is the eternal termination of menstruation due to loss of ovarian follicular activity. For many decades, women's health has been a universal concern. The emphasis of females’ well-being researchers and health policy planners has also moved toward postmenopausal women, and latest developments propose an upsurge in their number and life expectancy.[2,3,4] For centuries, instabilities of temperament and behavior have been accompanying with reproductive endocrine system variation in womankind. Long-standing concerns of variations in ovarian hormonal intensities include morbidities interrelated with age such as vascular diseases, osteoporosis, complications linked to memorization, urinary incontinence, and skin aging.[5]
The etiology of osteoporosis is very complicated; however, it is apparent that hormonal fluctuations after menopause upsurge the level of bone resorption, leading to an advanced risk of osteoporosis.[6] The brain is furthermore a goal on behalf of estrogen besides additional gonadal steroids. Subsets of neurons own intranuclear receptors for estrogen. Furthermore, it is also observed that complications such as Alzheimer's disease uttered earlier in females than in males. This may be accompanying with estrogen loss that occurs with menopause.[7] Several studies display that womenfolk who veteran initial menopause have an improved risk of heart diseases.[8,9] Urogenital complications are experienced by one-third of womenfolk since the age of 50 years and onward. Aging of skin has also been reported to be influenced by the decrease of female hormones after menopause.[5] Female sex hormones also regulate carbohydrate metabolism and adipose tissue distribution, and metabolic change leads to obesity.[10]
Oral uneasiness with dry mouth, changed perception, as well as burning sensation are the commonly reported chief complaints encountered in dental clinics. Most oral sensory complaints are caused by systemic diseases or are side effects of different medications. However, this does not hold true for a considerable number of patients seeking oral care. Previous studies have shown that many of these patients are menopausal women. The probable etiology of oral discomfort in menopausal women has been related to alterations in the quantity and/or quality of saliva.[11] Women at menopausal period may repeatedly develop many oral mucosal disorders. Burning mouth syndrome is considered as a common oral problem in these patients. Xerostomia is also a frequent finding among postmenopausal women. Other less common menopause-associated symptoms include bad or altered taste, viscous saliva, and mucosal disorders such as lichen planus, benign mucosal pemphigoid, and Sjogren's syndrome.[6]
The topic, the effect of menopause on salivary secretion was studied only by a few studies.[12] The study conducted by Bhat on the evaluation of the effect of menopause on saliva and dental health presented a decrease in salivary flow rate in postmenopausal females. In this study to examine the outcome of menopause on saliva and dental health, salivary flow rate, pH of stimulated whole saliva, and oral and hygiene status were determined in regularly menstruating and postmenopausal womankind who were not on medications.[1]
MATERIALS AND METHODS
The current study was carried out to examine the result of menopause on saliva and dental health. The research was done on healthy postmenopausal womenfolk’ patients chosen from among the patients who visited the outpatient division of the Department of Oral Medicine and Radiology, Dr. Syamala Reddy Dental College and Hospital, Bengaluru, for 10 months. The ethical approval was obtained from the institute with letter no. Reg No. SRDC 471/12 and the informed consent was taken from all the participants. The total sample consisted of eighty women (postmenopause and regular menstruation), based on convenient sampling. The study cluster comprised of forty healthy postmenopausal females with age range[1] from 41 to 60 years and the control group consisted of forty regularly menstruating healthy womenfolk with the age series from 21 to 31 years. The sample size was calculated by Student's t-test (two tailed, independent) which has been applied to find the significance of study parameters on a continuous scale between two groups (intergroup analysis) on metric parameters. Chi-square/Fisher's exact test was applied to find the significance of study parameters on a categorical scale among two or more groups.[9]
Inclusion criteria were women with usual chewing capacity, with no proof of dry mouth or any salivary gland disorders. Exclusion criteria were patients who were diabetic, hypertensive, on any medications, pan chewers, and completely edentulous.[1]
STUDY TOOL
It was allocated into two parts. Part one comprised of a structured conversation which documented demographic data, monthly menstruation, and several oral symptoms for each participant in this study. Part two was salivary collection and recording of clinical data.
SALIVA COLLECTION
Saliva was collected between 9 am and noon. The womankind was told not to consume, drink, or brush their teeth for at least 1 h before saliva collection. Salivary trials from the control cluster were composed in the first 3 days of menstruation. Contestants munched on an elastic band of standardized size. The saliva secreted through the first 1 min was swallowed, and saliva secreted during the next 5 min was spat into a graduated test tube. The flow rate was measured as ml/min. pH strips were used to determine the salivary pH.[1] Clinical assessment was done by Oral Hygiene Index Simplified (OHI-S), Decayed, Missing and Filled teeth (DMFT index), Community periodontal index (CPI), and Loss of attachment (LOA).
STATISTICAL ANALYSIS
Statistics found from questionnaires and clinical investigations were analyzed by the the SPSS software version 19.0 (IBM, Bangalore, India). Descriptive and inferential statistical analyses were conducted in the current study. Results on continuous measurements were presented on mean standard deviation (minimum–maximum), and results on categorical measurements were presented in number (%). The significance was assessed at 5% level of significance. Student's t-test (two tailed, independent) was applied to find the significance of study parameters on the continuous scale between two groups (intergroup analysis) on metric parameters. Chi-square/Fisher's exact test was applied to find the significance of study parameters on the categorical scale between two or more groups.
RESULTS
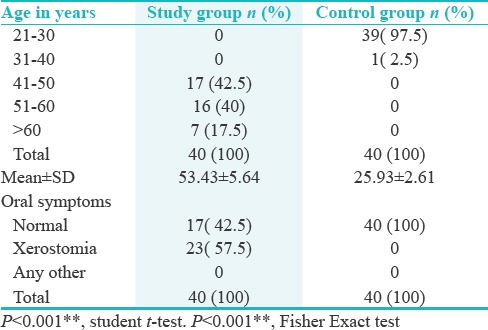
The mean age of the study group was 53.43 ± 5.64 years. The mean age of the control group was 25.93 ± 2.61 years. Out of the total forty women in the study group, majority (32 [80.0%]) were unemployed and out of the total forty women in the control group, majority, (22 [55.0%]) were unemployed. Majority of the study and control groups had high school education. Out of the total forty women in the study group, 17 (42.5%) were having normal oral symptoms and 23 (57.5%) were having xerostomia [Table 1].
Table 1.
Distribution of study group and control group according to age and oral symptoms
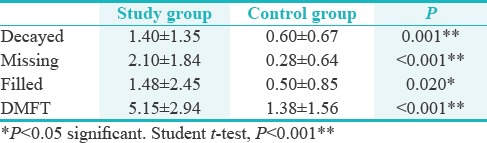
Out of the total forty women in the study group, 22 (55.0%) were having normal salivary flow rate and 18 (45.0%) were having hyposalivation. Out of the total forty women in the control group, all were having normal salivary flow rate. Out of the total forty women in the study group, twenty (50.0%) were having normal salivary pH and twenty (50.0%) were having acidic pH. Out of the total forty women in the control group, all were having normal salivary pH [Table 2]. Majority of the study group had poor OHI-S score (33 [82.5%]), and in the control group, majority had good OHI-S score (33 [82.5%]). Mean DMFT score in the study group and the control group was found to be 5.15 ± 2.94 and 1.38 ± 1.56, respectively, which was statistically significant with P < 0.001**. Mean CPI and LOA scores were also statistically significant with P < 0.001** [Tables 3–5].
Table 2.
Distribution of study group and control group according to salivary PH and Flow rate
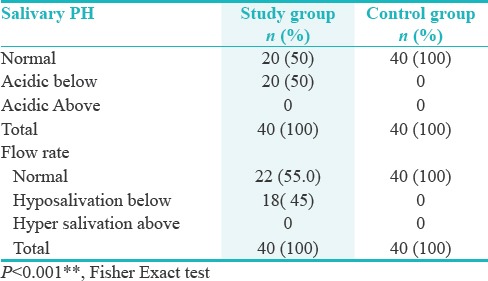
Table 3.
Distribution of study group and control group according to OHI-S
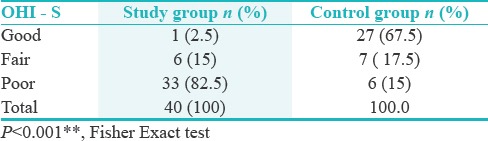
Table 5.
Comparison of study group and control group according Mean CPI and LOA

Table 4.
Comparison of study group and control group according Mean decayed, missing, filled and DMFT
DISCUSSION
In womankind approaching climacterium, various biological variations take place, most of which are due to reduced ovarian estrogen production.[5] Womanhood experience an upsurge in oral symptoms that may result from endocrine disturbances (reduced estrogen), calcium and vitamin deficiency, and several psychological issues throughout menopausal years. The most substantial oral symptom found in the menopausal women is oral dryness.[1] Saliva plays an important role in defensive oral tissues and avoiding external constituents from entering the body. When the salivary flow rate is reduced, predisposition to various oral diseases is enhanced. The measurement of the salivary flow rate is therefore of great importance.[2] Higher occurrence of dental caries, oral mucositis, dysphagia, oral infections, and altered taste has been recounted in those with reduced salivary flow.[3] Our study also show a notable diminution in the salivary flow rate, which might be attributed to the great values of OHI-S, DMFT, CPI, and LOA indices. Prior research on the effect of menopause on salivary flow rate has reported diverse results. Certain studies have stated no variation in salivary flow rate in the later period of menopause, although further studies have revealed reduced flow rates in postmenopausal womankind. Laine and Virtanen studied the oral status of menopausal and nonmenopausal females according to the World Health Organization criteria and reported lesser DMFT values in nonmenopausal women.[1] Dural have stated lower DMFT values in menstruating women.[4] Kullander, Sonesson, Laine, and Virtanen conveyed minor secretion rates in menopausal womankind than in menstruating women. Ship et al. and Ben Aryeh et al., however, reported that the salivary flow rate did not suggestively alter during menopause. Studies have recognized variations in numerous salivary constituents, such as mucin, IgA, phosphates, alterations in salivary pH, and electrical resistance.[2,7] An imperative function of salivary defense systems, predominantly built on proteins, is to switch bacterial colonization of the mouth. Long-standing instabilities such as aging as well as autoimmune diseases and medical treatment might be estimated to change salivary protein concentrations. It has been witnessed that the concentrations of salivary antimicrobial elements do not drop with age in unmedicated elderly people. Blum et al. suggested that estrogen replacement therapy drops serum immunoglobulins in postmenopausal women while snowballing serum E2 values. On the other hand, Widerstro¨m and Bratthall found a noticeable increase in the IgA level in the saliva of pregnant women. Barrington et al. proposed that S-IgA, which is the main IgA of mucosal surfaces, may diminish in postmenopausal women as a result of estrogen deficiency. This once again could mark as recurrent infection and cause undiagnosed postmenopausal flow of blood in the endometrium. It has been revealed that there are disparities in the mucosal immunological systems among the sexes, attributable to steroid sex hormones. Immune responses are stronger in women than in men. These expectations would lead to the model that falling concentrations or shortage of estrogen might affect the oral environment. Hyposalivation-interrelated subjective oral dryness or xerostomia is one more common appearance in postmenopausal females. The patients usually report a reduction in salivary flow, even though the fact that in only onethird of all cases hyposialia is present.[4,7,13,14] A destructive correlation was witnessed among the severity of dry mouth sensation and the salivary concentration of 17beta-estradiol in a case–control study conducted on 38 postmenopausal women. Adequate water consumption must be advised for these patients, along with sugar-free candies or munching gum to encourage salivation. Sialogogues such as pilocarpine may be indicated in some cases. Almost 45% of the authors have indicated that womenfolk who started with hormone therapy (HT) have reported that their quality of life has improved along with the decrease in oral discomfort. They have further proposed “increased saliva secretion” as the main reason behind such positive finding. These results also show that the composition of saliva in post- and premenopausal women seems to be estrogen dependent. Additionally, HT seemed to not affect the amount of the total salivary bacteria in either peri or postmenopausal women.[3]
In the study carried out by Ship et al. in the US on 43 healthy pre and postmenopausal females, it was reported that there were no changes in the quantity of saliva; hence suggesting that among healthy women, salivary gland function is not significantly influenced by menopause or HT. A study comparing stimulated and unstimulated salivary progesterone in menopausal women with oral dryness feeling showed that women with dry mouth had decreased unstimulated saliva flow and salivary progesterone compared with those without dry mouth. Thus, salivary progesterone level appears to be associated with oral dryness feeling in menopause.[3,9] In postmenopausal women, estrogen deficiency leads to monocytes and macrophages producing greater pro-inflammatory cytokines.[11] It has been shown that elderly people have significantly increased salivary calcium compared with younger people.[12,15] Our study showed a significant reduction of salivary pH. The changes may result from hormonal alterations taking place in menopausal women, altered sympathetic output related to stress, or from alterations in interactions between the cranial nerves serving taste and pain sensation.[2]
CONCLUSION
There is a marked decrease in the salivary pH and flow rate in postmenopausal women which in turn leads to increased OHI-S, DMFT, CPI, and LOA. The study has shown that the importance of preventive dentistry increases with aging in females. The studies should provide an exhaustive account of women's views, health-care practices, and their expectations about the roles of social institutions to tackle normal menopausal transition and healthy postmenopausal life. Such studies will help to devise culturally appropriate public health programs for menopausal and postmenopausal women to ensure healthy postreproductive life for them.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Bhat S. A study on evaluation of the effect of menopause on saliva and dental health. J Adv Dent Res. 2010;1:33–5. [Google Scholar]
- 2.Mishra SK. Menopausal transition and postmenopausal health problems: A review on its bio-cultural perspectives. Health. 2011;3:233–7. [Google Scholar]
- 3.Mojabi KB, Esfahani M, Hashemi HJ. Evaluation of Unstimulated Salivary Flow Rate and Oral Symptoms in Menopausal Women. J Dent Tehran Univ Med Sci. 2007;4:103–6. [Google Scholar]
- 4.Sema DURAL DDS. Evaluation of the Effect of Menopause on Saliva and Dental Health Cilt: 30, Sayý: 3, Sayfa; 15-18. 2006 [Google Scholar]
- 5.Anil S, Alsqah MN, Rajendran R. Burning mouth syndrome: Diagnostic appraisal and management strategies. Saudi Dent J. 2007;19:128–38. [Google Scholar]
- 6.Alani SH. The influence of menopause on unstimulated salivary flow and subjective oral dryness inrelation to other oral symptoms and salivary gland hypofunction. J Baghdad Coll Dent. 2012;24:78–80. [Google Scholar]
- 7.Leimola-Virtanen R, Helenius H, Laine M. Hormone replacement therapy and some salivary antimicrobial factors in post- and perimenopausal women. Maturitas. 1997;27:145–51. doi: 10.1016/s0378-5122(97)00024-8. [DOI] [PubMed] [Google Scholar]
- 8.Buencamino MC, Palomo L, Thacker HL. How menopause affects oral health, and what we can do about it. Cleve Clin J Med. 2009;76:467–75. doi: 10.3949/ccjm.76a.08095. [DOI] [PubMed] [Google Scholar]
- 9.Dutt P, Chaudhary S, Kumar P. Oral health and menopause: A comprehensive review on current knowledge and associated dental management. Ann Med Health Sci Res. 2013;3:320–3. doi: 10.4103/2141-9248.117926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tarkkila L, Furuholm J, Tiitinen A, Meurman JH. Oral health in perimenopausal and early postmenopausal women from baseline to 2 years of follow-up with reference to hormone replacement therapy. Clin Oral Investig. 2008;12:271–7. doi: 10.1007/s00784-008-0190-z. [DOI] [PubMed] [Google Scholar]
- 11.Rockenbach MI, Marinho SA, Veeck EB, Lindemann L, Shinkai RS. Salivary flow rate, pH, and concentrations of calcium, phosphate, and sIgA in Brazilian pregnant and non-pregnant women. Head Face Med. 2006;2:44. doi: 10.1186/1746-160X-2-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Singh R, Pallagatti S, Sheikh S, Singh B, Arora G, Aggarwal A, et al. Correlation of serum oestrogen with salivary calcium in post-menopausal women with and without oral dryness feeling. Gerodontology. 2012;29:125–9. doi: 10.1111/j.1741-2358.2011.00580.x. [DOI] [PubMed] [Google Scholar]
- 13.Bruckmann C. “Oral menopause” – Do you know this phenomenon? Womens Health Sci J. 2018;2:106. [Google Scholar]
- 14.Bhat SP. Assessment of periodontal status of postmenopausal women attending dental clinics. Int J Recent Sci Res. 2017;8:16089–94. [Google Scholar]
- 15.Palomo L, Williams K, Thacker H. Periodontal healing and osteoporosis in postmenopausal women. Ann Gerontol Geriatr Res. 2016;3:1043. [Google Scholar]