

Abstract
Background
The naturally occurring male-to-female (M/F) ratio at birth is 1.05. Higher ratios found primarily in countries across Asia have been attributed to prenatal sex selection due to son preference. There is growing evidence that sex-selective practices continue following migration; however, little is known about these practices following migration to Australia.
Methods
In this population-based study we assessed M/F ratios at birth per mother’s country of birth for all registered births 1999–2015 in Victoria, Australia (n = 1 191 250). We also compared the M/F ratio among births to mothers born elsewhere to that of mothers born in Australia, stratified by time period and parity.
Results
Compared with the naturally occurring M/F ratio as well as to the M/F ratio among births to mothers born in Australia, there was an increased ratio of male births to mothers born in India, China and South-East Asia, particularly at higher parities and in more recent time periods (elevated M/F ratios ranged from 1·079 to 1·248, relative risks of male birth ranged from 1·012 to 1·084 with confidence intervals between 1·001 and 1·160 and P-values between 0·005 and 0·039). The most male-biased sex ratios were found among multiple births to Indian-born mothers, and parity of two or more births to Indian and Chinese-born mothers in 2011–15.
Conclusions
The male-biased sex ratios observed in this study indicate that prenatal sex selection may be continuing following migration to Australia from countries where these practices have been documented. The excess of males among multiple births raises the question as to what role assisted reproduction plays. Findings also suggest that systematic discrimination against females starts in the womb.
Keywords: Australia, relative risk, sex ratio, pregnancy, sex selection, sex preselection
Key Messages
This study adds to the limited but growing literature on male-biased sex ratios at birth and sex-selective practices in the context of migration to Western high-income countries.
Analyses revealed a higher than expected proportion of male births to mothers born in India, China and South East Asia. An unexpected finding was a substantially elevated proportion of male births among multiple-birth infants of Indian-born mothers.
The results have implications for social policies aimed at promoting gender equality and policies for assisted reproduction and prenatal diagnosis (sex identification and selection), as well as population-based surveillance methods aimed at identifying signs of gender discriminatory practices in pregnancy and childbirth.
Background
Between 1970 and 2010, sex selection and postnatal excess female mortality due to discrimination have resulted in an estimated 126 million women ‘missing’ worldwide. China and India have been identified as the major contributors to this deficit.1,2 High male-to-female (M/F) ratios at birth have been observed in a number of countries across Asia, but also other parts of the world, including in Southern Caucasus and parts of South East Europe.1
M/F ratios at birth higher than the biological ratio of 1.05 (biological range 1.04–1.063) is a simple yet strong indicator of systematic discrimination against females through prenatal sex selection.1–3 Prenatal sex selection most commonly occurs through termination of pregnancy following sex determination.1 It is also possible through pre-implantation genetic diagnosis by identifying the sex of the embryo for in vitro fertilization (IVF), or through sperm sorting.1 Ultrasound is the most widespread technology for fetal sex determination, and a rapid increase in sex ratio imbalances has been seen in some regions since the 1980s, when the use of ultrasound scans in pregnancy became widespread.1,3 Other prenatal sex determination methods include amniocentesis, chorionic villus sampling and, in the most recent years, a blood test from the pregnant woman early in pregnancy.1,4
M/F ratio imbalances generally increase with birth order in settings characterized by son preference, often with a sharp rise after first births (where M/F ratios often are at normal levels).1 With the M/F ratios observed in India and China, it has been estimated that 30% of sonless women in India resort to termination of female pregnancies after the second birth, and that 25% of sonless women in China resort to termination of female pregnancies after the first birth.3 In some settings, lower M/F ratios at birth have been observed in contexts of nutritional deprivation due to higher vulnerability of male fetuses.5 M/F ratios at birth have also been suggested to fluctuate due to stressors such as wars, surrounding temperature, economic crises and ecological disasters. However, the current evidence is thin and the effect on M/F ratios of these other factors is negligible in comparison with documented sex imbalances attributed to prenatal sex selection.3,6
Australia is a multicultural country with about the third of the population born overseas, with the largest groups originating from the UK, New Zealand, China, India, the Philippines and Vietnam. Since 2004, sex selection has been prohibited throughout Australia, with the exception of situations where there is a risk of transmission of a genetic condition, disease or abnormality that would severely limit the quality of life of the person who would be born.7 A number of states, including Victoria, also have legislative prohibitions on sex selection during assisted reproduction.8 Abortion is available on request in Victoria if the woman is not more than 24 weeks pregnant.9 There is evidence to suggest that sex-selective practices continue in some migrant communities in Western high-income countries irrespective of the majority cultural consensus to reject such practices.10–26 However, no previous research has been undertaken to explore the situation in Australia.
Our aim in this study was to describe M/F ratios at birth among infants born in Victoria of mothers born in different countries, and to assess potential differences in M/F ratios between mothers born in Australia and mothers born elsewhere. All analyses are stratified by time period and parity.
Methods
Study design
Data for this population-based study were derived from the Victorian Perinatal Data Collection (VPDC), which is a population-based surveillance system that collects information on maternal characteristics, obstetric conditions, procedures and outcomes of every birth in Victoria, Australia.
Procedures
We obtained data on all births at ≥20 weeks of gestation (live birth or stillbirth) or with birthweight ≥400 g (if gestation unknown) during the time period 1999–2015 (n = 1 191 250).
Variables
Dependent variable
Births were categorized as male or female. Each infant in multiple births had an individual case record, enabling analysis of multiple births regardless of whether they were of the same or mixed sex.
Independent variable
We classified all births based on the birth country of the mother and according to the World Health Organization (WHO) regions (Africa, Americas, South East Asia, European, Eastern Mediterranean and Western Pacific). Countries with >10 000 births over the study period were analysed separately by country (Australia, India, UK, Vietnam, China, New Zealand, Philippines and Sri Lanka) and remaining countries were collapsed into WHO world regions. A listing of countries per WHO region is presented in Supplementary File 1, available as Supplementary data at IJE online.
Time trends
To investigate possible time trends, data were trichotomized into the periods 1999-2004, 2005-10 and 2011–15.
Maternal and infant characteristics
Infant birthweight (grams), estimated gestation (weeks), birth plurality, parity (all previous pregnancies that resulted in a live birth or stillbirth of ≥20 weeks of gestation or at least ≥400 g in weight), maternal age (in years), and marital status (dichotomized as married/not married, where the second category included widowed, divorced, separated, de facto and not stated) were used to describe maternal and infant characteristics. Parity was also in used in analyses of M/F ratios and relative risks and categorized into 0, 1 and ≥2.
Missing values and accuracy of data
The dataset was largely complete, missing values were less than 0.001% for all variables used and cases with missing variables were consistently excluded from analyses. The following accuracy of birth data collected in 200327 and 201128 have been documented, respectively: infant sex, 99.7/99.3%; mother’s country of birth, 92.7/93.7%; parity, 98.6/97.4%; infant birth date, 99.8/not available (n.a.) %; infant birthweight, 98.9/95.8%; estimated gestation, 91.9/93.1%; plurality, 99.8/100%; maternal age, 99.7/97.8%; and marital status, 96.4/92.4%.
Statistical analyses
To establish M/F ratios at birth and their 95% confidence intervals (CIs), we used logistic regression (intercept-only model). Point estimates above or below 1.04–1.06, with a 95% CI excluding the natural ratio of 1.05, were considered as different from the natural ratio. To investigate differences between mothers born in Australia (reference category) and in other countries, relative risks (RRs) with 95% CIs for male births were estimated using generalized linear models (GLM) with a Poisson distribution, log link function and robust covariance matrix estimator. Maternal age was adjusted for in these analyses, as a number of previous studies have indicated a negative relationship between male birth and increasing maternal age.29,30 All data were analysed using SPSS version 24.
We undertook analyses separately for singleton and multiple births, and all births combined. However, because M/F ratios are most commonly reported as population sex ratios at birth, we decided to present the majority of findings based on all births combined, to facilitate comparison with the naturally occurring M/F ratio, as well as with previous publications and country-specific reports on population sex ratios at birth across the globe.
Ethical considerations
Ethics approval was obtained from La Trobe University (SHE CHESC), reference S15/232. Use of the VPDC data was approved by the Consultative Council on Obstetric and Paediatric Mortality and Morbidity (CCOPMM) in Victoria, Australia.
Results
Background characteristics of mothers giving birth in Victoria, Australia 1999–2015
There were 1 191 250 births reported in Victoria between 1999 and 2015, of which 852 016 (71.5%) were of Australian-born mothers. Table 1 outlines maternal, infant and birth-country characteristics of the study sample.
Table 1.
Maternal, infant and birth-country characteristics of mothers giving birth in Victoria, Australia 1999–2015
| Maternal characteristics |
Infant characteristics |
Birth country characteristicsa |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mother’s country of birth, (n) | % of births | Mother’s age (years), mean (SD) | Marital status, married (%) | Parity no. (%) |
Male sex (%) | Birth plurality, singleton (%) | Birthweight (grams), mean (SD) | Gestational age (weeks), mean (SD) | Fertility rate | Male-to-female ratio at birth | ||
| 0 | 1 | ≥2 | ||||||||||
| Australia (852 016) | 71.5 | 30.4 | 67.2 | 365 865 | 296 990 | 189 106 | 51.3 | 96.5 | 3383 (613.9) | 38.8 (2.2) | 1.77 | 1.06b |
| (5.4) | (42.9) | (34.9) | (22.2) | |||||||||
| India (36 426) | 3.1 | 29.5 | 97.8 | 21 662 | 12 418 | 2341 | 51.9 | 97.6 | 3143 (568.8) | 38.7 (2.2) | 2.45 | 1.12 |
| (3.9) | (59.5) | (34.1) | (6.4) | |||||||||
| UK (29 171) | 2.5 | 33.2 | 75.3 | 12 059 | 10 502 | 6609 | 51.3 | 96.2 | 3401 (603.8) | 38.9 (2.1) | 1.89 | 1.05 |
| (4.8) | (41.3) | (36.0) | (22.7) | |||||||||
| Vietnam (27 922) | 2.4 | 30.8 | 77.1 | 11 887 | 10 511 | 5522 | 51.3 | 98.1 | 3180 (503.0) | 38.7 (1.9) | 1.82 | 1.11 |
| (5.1) | (42.6) | (37.6) | (19.8) | |||||||||
| China (23 454) | 2.0 | 31.4 | 90.4 | 13 139 | 8657 | 1658 | 52.1 | 98.0 | 3312 (512.9) | 38.9 (1.9) | 1.60 | 1.15 |
| (4.7) | (56.0) | (36.9) | (7.1) | |||||||||
| New Zealand (23 013) | 1.9 | 30.2 | 54.0 | 9089 | 7196 | 6723 | 51.6 | 96.7 | 3424 (621.5) | 38.9 (2.2) | 2.03 | 1.05 |
| (5.9) | (39.5) | (31.3) | (29.2) | |||||||||
| Philippines (11 199) | 0.9 | 31.5 | 80.0 | 4660 | 3982 | 2556 | 50.7 | 97.7 | 3225 (568.4) | 38.4 (2.1) | 3.02 | 1.05 |
| (5.3) | (41.6) | (35.6) | (22.8) | |||||||||
| Sri Lanka (11 192) | 0.9 | 31.7 | 97.0 | 5278 | 4300 | 1614 | 51.2 | 97.2 | 3167 (576.4) | 38.5 (2.2) | 2.07 | 1.04 |
| (4.4) | (47.2) | (38.4) | (14.4) | |||||||||
| Rest of European Region (43 629) | 3.7 | 31.6 | 83.8 | 18 499 | 15 930 | 9196 | 51.4 | 96.7 | 3388 (87.8) | 38.9 (2.1) | - | - |
| (5.2) | (42.4) | (36.5) | (21.1) | |||||||||
| Eastern Mediterranean Region (38 677) | 3.3 | 29.0 | 91.7 | 11 512 | 10 606 | 16 554 | 51.4 | 97.2 | 3303 (578.7) | 38.9 (2.1) | - | - |
| (5.6) | (29.8) | (27.4) | (42.8) | |||||||||
| Rest of Western Pacific Region (36 092) | 3.1 | 31.6 | 84.2 | 16 070 | 12 040 | 7981 | 51.2 | 97.5 | 3260 (576.7) | 38.7 (2.1) | - | - |
| (5.0) | (44.5) | (33.4) | (22.1) | |||||||||
| African Region (18 967) | 1.6 | 31.1 | 79.6 | 6974 | 6063 | 5922 | 51.1 | 96.8 | 3320 (616.9) | 38.9 (2.3) | - | - |
| (5.2) | (36.8) | (32.0) | (31.2) | |||||||||
| Rest of South-East Asia Region (16 305) | 1.4 | 30.2 | 87.5 | 7934 | 5441 | 2925 | 52.0 | 97.9 | 3223 (555.2) | 38.7 (2.0) | - | - |
| (4.9) | (48.7) | (33.4) | (17.9) | |||||||||
| Region of the Americas (14 709) | 1.2 | 32.2 | 80.5 | 6687 | 5042 | 2978 | 51.1 | 97.0 | 3386 (584.4) | 38.9 (2.1) | - | - |
| (5.0) | (45.5) | (34.3) | (20.2) | |||||||||
SD, standard deviation.
Birth country characteristics obtained from the Central Intelligence Agency.36
Reported national average. The male-to-female ratio for all births in Victoria 1999-2015 was 1.054, as shown in this study.
Mothers born in the Eastern Mediterranean region were on average youngest, and mothers born in the UK were oldest (mean age 29.0 and 33.2 years, respectively). The vast majority of mothers from India (97.8%), China (90.4%) and Sri Lanka (97.0%) and the Eastern Mediterranean (91.7%) were married, compared with two-thirds of the Australian-born mothers (67.2%). Parity varied considerably between countries/regions; 42.8% (n = 16 554) of births to Eastern Mediterranean mothers were of parity 2 or higher, whereas the equivalent figure for Indian and Chinese-born mothers were 6.4% (n = 2341) and 7.1% (n = 1658), respectively, compared with 22.2% of Australian born mothers (n = 189 106) (Table 1). The number of births to Indian, Chinese and Eastern Mediterranean-born mothers increased the most during the period 1999-2015, with a more than 10-fold increase in births to Indian-born mothers from 1999 to 2015 (Figure 1).
Figure 1.

A, B. Number of births per year per country (A) and region (B) of birth of mothers giving birth in Victoria, Australia 1999–2015.
Male-to-female ratios at birth by mother’s country or region of birth 1999-2015
For the period 1999-2015, the M/F ratio among births to Australian-born mothers was 1.053 (95% CI 1.048-1.057). At the same time, the M/F ratios among births to Indian and Chinese-born mothers were elevated above the natural ratio, with RRs of male birth higher compared with births to Australian-born mothers (Table 2).
Table 2.
Male-to-female ratios at birth and relative risk for male birth in Victoria 1999–2015 by mother’s birthplace, stratified by birth plurality
| Mother’s country of birth | n males/n females | M/F ratio | RRa(95% CI) | Sig. |
|---|---|---|---|---|
| Singleton and multiple births | ||||
| All births | 611 078/579 548 | 1.054 (1.051–1.058) | – | |
| Australia | 436 724/414 874 | 1.053 (1.048–1.057) | Ref. | |
| India | 18 887/17 508 | 1.079 (1.057–1.101) | 1.012 (1.001–1.022) | 0.025 |
| UK | 14 962/14 199 | 1.054 (1.030–1.078) | 1.001 (0.990–1.013) | 0.801 |
| Vietnam | 14 311/13 599 | 1.052 (1.028–1.077) | 1.000 (0.988–1.012) | 0.999 |
| China | 12 225/11 217 | 1.090 (1.062–1.118) | 1.017 (1.005–1.030) | 0.007 |
| New Zealand | 11 883/11 123 | 1.068 (1.041–1.096) | 1.007 (0.994–1.020) | 0.273 |
| Philippines | 5678/5518 | 1.029 (0.992–1.068) | 0.989 (0.971–1.008) | 0.247 |
| Sri Lanka | 5728/5462 | 1.049 (1.011–1.088) | 0.998 (0.980–1.017) | 0.864 |
| Rest of European Region | 22 397/21 219 | 1.056 (1.036–1.076) | 1.002 (0.992–1.011) | 0.726 |
| Eastern Mediterranean Region | 19 847/18 803 | 1.056 (1.035–1.077) | 1.001 (0.991–1.011) | 0.888 |
| Rest of Western Pacific Region | 18 456/17 614 | 1.048 (1.026–1.070) | 0.998 (0.988–1.009) | 0.741 |
| African Region | 9693/9261 | 1.047 (1.017–1.077) | 0.997 (0.983–1.011) | 0.688 |
| Rest of South East Asia Region | 8465/7825 | 1.082 (1.049–1.116) | 1.013 (0.998–1.028) | 0.086 |
| Region of the Americas | 7516/7190 | 1.045 (1.012–1.080) | 0.997 (0.982–1.013) | 0.751 |
| Singleton births | ||||
| Australia | 421 386/400 092 | 1.053 (1.049–1.058) | Ref. | |
| India | 18 408/17 111 | 1.076 (1.054–1.098) | 1.010 (1.000–1.020) | 0.055 |
| UK | 14 391/13 674 | 1.052 (1.028–1.077) | 1.001 (0.989–1.012) | 0.923 |
| Vietnam | 14 052/13 315 | 1.055 (1.031–1.081) | 1.001 (0.989–1.012) | 0.851 |
| China | 11 992/10 986 | 1.092 (1.064–1.120) | 1.018 (1.005–1.031) | 0.006 |
| New Zealand | 11 521/10 733 | 1.073 (1.046–1.102) | 1.009 (0.996–1.022) | 0.164 |
| Philippines | 5554/5388 | 1.031 (0.993–1.070) | 0.990 (0.972–1.008) | 0.280 |
| Sri Lanka | 5563/5315 | 1.047 (1.008–1.087) | 0.997 (0.979–1.016) | 0.765 |
| Rest of European Region | 21 680/20 493 | 1.058 (1.038–1.078) | 1.003 (0.993–1.012) | 0.605 |
| Eastern Mediterranean Region | 19 278/18 291 | 1.054 (1.033–1.076) | 1.000 (0.990–1.010) | 0.962 |
| Rest of Western Pacific Region | 17 990/17 191 | 1.046 (1.025–1.069) | 0.997 (0.987–1.008) | 0.622 |
| African Region | 9375/8975 | 1.045 (1.015–1.075) | 0.996 (0.982–1.010) | 0.572 |
| Rest of South East Asia Region | 8296/7657 | 1.083 (1.050–1.118) | 1.014 (0.998–1.029) | 0.078 |
| Region of the Americas | 7286/6975 | 1.045 (1.011–1.079) | 0.997 (0.981–1.013) | 0.697 |
| Multiple births | ||||
| Australia | 15 332/14 782 | 1.037 (1.014–1.061) | Ref. | |
| India | 478/397 | 1.204 (1.054–1.375) | 1.072 (1.008–1.140) | 0.026 |
| UK | 571/525 | 1.088 (0.966–1.224) | 1.024 (0.967–1.086) | 0.415 |
| Vietnam | 259/284 | 0.912 (0.771–1.079) | 0.937 (0.857–1.024) | 0.150 |
| China | 233/231 | 1.009 (0.841–1.210) | 0.987 (0.900–1.081) | 0.771 |
| New Zealand | 362/390 | 0.928 (0.805–1.071) | 0.945 (0.877–1.019) | 0.143 |
| Philippines | 124/130 | 0.954 (0.746–1.219) | 0.959 (0.845–1.088) | 0.514 |
| Sri Lanka | 165/147 | 1.122 (0.899–1.401) | 1.040 (0.936–1.155) | 0.471 |
| Rest of European Region | 715/726 | 0.985 (0.888–1.092) | 0.975 (0.925–1.028) | 0.354 |
| Eastern Mediterranean Region | 569/512 | 1.111 (0.986–1.252) | 1.033 (0.975–1.095) | 0.266 |
| Rest of Western Pacific Region | 466/423 | 1.102 (0.966–1.257) | 1.030 (0.967–1.098) | 0.360 |
| African Region | 318/286 | 1.112 (0.948–1.304) | 1.034 (0.958–1.117) | 0.386 |
| Rest of South East Asia Region | 169/168 | 1.006 (0.813–1.245) | 0.985 (0.885–1.096) | 0.783 |
| Region of the Americas | 230/215 | 1.070 (0.888–1.288) | 1.016 (0.928–1.113) | 0.727 |
Bold: M/F ratio point estimate above or below 1.04–1.06 with a 95% CI excluding the natural ratio of 1.05, or RR with P = <0.05.
Sig., significance; M/F ratio, male-to-female ratio. RR, relative risk.
Adjusted for maternal age.
In analyses of singleton and multiple births separately, M/F ratios remained higher than expected among singleton births to Indian- and Chinese-born mothers, although differences between groups were statistically significant only for births to Chinese-born mothers (Table 2). Among multiple births, M/F ratios were considerably higher than expected for births to Indian-born mothers (M/F ratio 1.204, 95% CI 1.054-1.375), with the RR of male birth being higher compared with Australian-born mothers (RR 1.072, 95% CI 1.008-1.140, P = 0.026) as also illustrated in Figure 2. The M/F ratio for the total sample of multiple births (n = 39 485) was 1.040 (95% CI 1.020-1.061), slightly lower than for singleton and multiple births combined.
Figure 2.
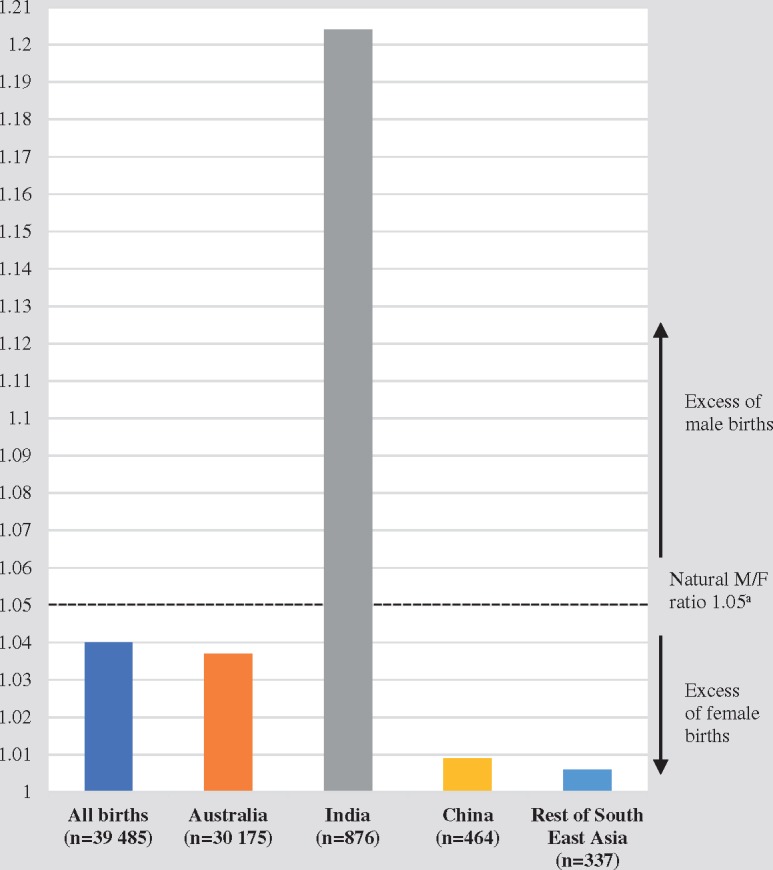
Male-to-female ratios, multiple births 1999–2015, aNatural ratio for singleton and multiple births combined. See Table 2 for M/F ratios with CIs.
Male-to-female ratios at birth by mother’s country or region of birth, stratified by parity
The M/F ratios decreased stepwise as parity increased in the total sample and among births to Australian-born mothers. On the contrary, we found a stepwise increase in M/F ratios as parity increased among births to Indian, Chinese and South East Asian-born mothers (Table 3; illustrated in Supplementary File 2, available as Supplementary data at IJE online). This pattern was unique to these countries/regions, although differences between groups could only be established for Indian- and Chinese-born mothers at parity 1 (i.e. one previous birth). The M/F ratio of births to African-born mothers was lower than expected at parity ≥2, and the RR for male birth elevated among New Zealand mothers at parity ≥2 (Table 3).
Table 3.
Male-to-female ratios by mother’s country or region of birth, and the influence of mother’s birthplace on risk of male birth, stratified by parity
| Mother’s country of birth | Parity | n males/n females | M/F ratio | RRa (95% CI) | Sig. |
|---|---|---|---|---|---|
| All births | 0 | 264 897/250 268 | 1.058 (1.053–1.064) | ||
| 1 | 211 260/200 499 | 1.054 (1.047–1.060) | |||
| ≥2 | 134 856/128 727 | 1.048 (1.040–1.056) | |||
| Australia | 0 | 187 995/177 688 | 1.058 (1.051–1.065) | Ref.b | |
| 1 | 152 061/144 796 | 1.050 (1.043–1.058) | Ref. | ||
| ≥2 | 96 639/92 364 | 1.046 (1.037–1.056) | Ref. | ||
| India | 0 | 11 128/10 509 | 1.059 (1.031–1.088) | 1.000 (0.987–1.014) | 0.977 |
| 1 | 6517/5895 | 1.106 (1.067–1.145) | 1.025 (1.008–1.043) | 0.005 | |
| ≥2 | 1239/1102 | 1.124 (1.037–1.220) | 1.036 (0.997–1.077) | 0.071 | |
| UK | 0 | 6221/5834 | 1.066 (1.029–1.105) | 1.005 (0.987–1.023) | 0.574 |
| 1 | 5359/5138 | 1.043 (1.004–1.084) | 0.997 (0.978–1.016) | 0.732 | |
| ≥2 | 3382/3226 | 1.048 (0.999–1.100) | 1.002 (0.978–1.026) | 0.877 | |
| Vietnam | 0 | 6064/5815 | 1.043 (1.006–1.081) | 0.993 (0.975–1.011) | 0.441 |
| 1 | 5413/5098 | 1.062 (1.022–1.103) | 1.005 (0.987–1.024) | 0.582 | |
| ≥2 | 2833/2685 | 1.055 (1.001–1.112) | 1.005 (0.979–1.031) | 0.722 | |
| China | 0 | 6796/6334 | 1.073 (1.037–1.110) | 1.007 (0.990–1.024) | 0.405 |
| 1 | 4545/4109 | 1.106 (1.060–1.154) | 1.025 (1.004–1.046) | 0.017 | |
| ≥2 | 884/774 | 1.142 (1.037–1.258) | 1.044 (0.998–1.092) | 0.062 | |
| New Zealand | 0 | 4725/4360 | 1.084 (1.040–1.130) | 1.012 (0.992–1.032) | 0.243 |
| 1 | 3633/3562 | 1.020 (0.974–1.068) | 0.985 (0.963–1.009) | 0.215 | |
| ≥2 | 4725/4360 | 1.084 (1.040–1.129) | 1.025 (1.001–1.049) | 0.041 | |
| Philippines | 0 | 2355/2304 | 1.022 (0.965–1.083) | 0.984 (0.956–1.012) | 0.255 |
| 1 | 2062/1918 | 1.075 (1.010–1.144) | 1.011 (0.981–1.042) | 0.462 | |
| ≥2 | 1260/1296 | 0.972 (0.900–1.050) | 0.965 (0.927–1.004) | 0.077 | |
| Sri Lanka | 0 | 2748/2529 | 1.087 (1.029–1.147) | 1.013 (0.987–1.040) | 0.323 |
| 1 | 2181/2118 | 1.030 (0.970–1.093) | 0.990 (0.961–1.020) | 0.512 | |
| ≥2 | 799/815 | 0.980 (0.889–1.081) | 0.969 (0.922–1.018) | 0.213 | |
| Rest of European Region | 0 | 9504/8990 | 1.057 (1.027–1.088) | 1.000 (0.986–1.015) | 0.970 |
| 1 | 8161/7766 | 1.051 (1.019–1.084) | 1.000 (0.985–1.016) | 0.985 | |
| ≥2 | 4729/4462 | 1.060 (1.017–1.104) | 1.007 (0.987–1.028) | 0.505 | |
| Eastern Mediterranean Region | 0 | 5896/5609 | 1.051 (1.013–1.090) | 0.996 (0.978–1.014) | 0.637 |
| 1 | 5489/5112 | 1.074 (1.034–1.115) | 1.011 (0.992–1.030) | 0.263 | |
| ≥2 | 8459/8080 | 1.047 (1.015–1.079) | 1.000 (0.985–1.015) | 0.977 | |
| Rest of Western Pacific Region | 0 | 8254/7806 | 1.057 (1.025–1.091) | 1.000 (0.985–1.016) | 0.969 |
| 1 | 6148/5883 | 1.045 (1.008–1.083) | 0.998 (0.980–1.016) | 0.809 | |
| ≥2 | 4054/3924 | 1.033 (0.989–1.079) | 0.944 (0.973–1.016) | 0.611 | |
| African Region | 0 | 3632/3338 | 1.088 (1.038–1.140) | 1.014 (0.991–1.037) | 0.237 |
| 1 | 3113/2945 | 1.057 (1.005–1.112) | 1.003 (0.978–1.028) | 0.833 | |
| ≥2 | 2943/2975 | 0.989 (0.940–1.041) | 0.973 (0.948–0.998) | 0.036 | |
| Rest of South East Asia Region | 0 | 4103/3822 | 1.074 (1.027–1.122) | 1.007 (0.985–1.029) | 0.539 |
| 1 | 2829/2609 | 1.084 (1.028–1.144) | 1.016 (0.990–1.042) | 0.240 | |
| ≥2 | 1531/1391 | 1.101 (1.024–1.184) | 1.025 (0.990–1.061) | 0.169 | |
| Region of the Americas | 0 | 3416/3268 | 1.045 (0.996–1.097) | 0.995 (0.972–1.019) | 0.681 |
| 1 | 2586/2456 | 1.053 (0.996–1.113) | 1.001 (0.974–1.029) | 0.942 | |
| ≥2 | 1514/1464 | 1.034 (0.962–1.111) | 0.996 (0.961–1.032) | 0.811 |
Bold: M/F ratio point estimate above or below 1.04–1.06 with a 95% CI excluding the natural ratio of 1.05, or RR with P = <0.05.
Adjusted for maternal age.
Individual Australian-born parity group used as reference for the corresponding parity group from each of the other countries/regions.
Male-to-female ratios at birth by mother’s country or region of birth, stratified by time period and parity
Over the three time periods 1999–2004, 2005–10 and 2011–15, the M/F ratio slightly increased within the natural range for infants of Australian-born mothers (1.049, 1.053 and 1.057, respectively) (Table 4). The M/F ratios were higher than expected for infants of Indian, Chinese and South East Asian-born mothers in 2005-10, with RRs of male birth higher than among infants of Australian-born mothers (Table 4). No abnormal M/F ratios or RRs were found for remaining countries/regions.
Table 4.
Male-to-female ratios by mother’s birthplace and relative risk for male birth, stratified by time period and parity
| Mother’s country of birth | Time period | Parity | n males/n females | M/F ratio | RRa (95% CI) | Sig. |
|---|---|---|---|---|---|---|
| Australia | 1999–2004 | All | 147 040/140 189 | 1·049 (1·041–1·057) | Ref.b | |
| 0 | 62 620/59 635 | 1·050 (1·038–1·062) | Ref. | |||
| 1 | 50 960/48 820 | 1·044 (1·031–1·057) | Ref. | |||
| ≥2 | 33 459/31 734 | 1·054 (1·038–1·071) | Ref. | |||
| 2005–10 | All | 159 217/151 215 | 1·053 (1·046–1·060) | Ref. | ||
| 0 | 68 410/64 370 | 1·063 (1·051–1·074) | Ref. | |||
| 1 | 55 211/52 600 | 1·050 (1·037–1·062) | Ref. | |||
| ≥2 | 35 580/34 229 | 1·039 (1·024–1·055) | Ref. | |||
| 2011–15 | All | 130 467/123 470 | 1·057 (1·048–1·065) | Ref. | ||
| 0 | 56 965/53 683 | 1·061 (1·049–1·074) | Ref. | |||
| 1 | 45 890/43 376 | 1·058 (1·044–1·072) | Ref. | |||
| ≥2 | 27 600/26 401 | 1·045 (1·028–1·063) | Ref. | |||
| India | 1999–2004 | All | 1701/1646 | 1·033 (0·966–1·106) | 0·993 (0·960–1·027) | 0·673 |
| 0 | 779/779 | 1·000 (0·905–1·104) | 0·976 (0·929–1·026) | 0·346 | ||
| 1 | 715/657 | 1·088 (0·979–1·210) | 1·020 (0·969–1·073) | 0·450 | ||
| ≥2 | 207/210 | 0·986 (0·814–1·194) | 0·969 (0·879–1·068) | 0·522 | ||
| 2005–10 | All | 5984/5451 | 1·098 (1·058–1·139) | 1·019 (1·001–1·037) | 0·039 | |
| 0 | 3841/3451 | 1·113 (1·063–1·165) | 1·021 (0·999–1·045) | 0·064 | ||
| 1 | 1753/1636 | 1·072 (1·002–1·146) | 1·010 (0·977–1·044) | 0·558 | ||
| ≥2 | 389/364 | 1·069 (0·926–1·233) | 1·016 (0·947–1·089) | 0·663 | ||
| 2011–15 | All | 11 202/10 411 | 1·076 (1·048–1·105) | 1·009 (0·995–1·022) | 0·207 | |
| 0 | 6508/6279 | 1·036 (1·001–1·073) | 0·988 (0·971–1·006) | 0·201 | ||
| 1 | 4049/3602 | 1·124 (1·075–1·176) | 1·029 (1·007–1·052) | 0·010 | ||
| ≥2 | 643/528 | 1·218 (1·085–1·366) | 1·074 (1·019–1·132) | 0·008 | ||
| China | 1999–2004 | All | 2428/2221 | 1·093 (1·032–1·158) | 1·020 (0·993–1·049) | 0·153 |
| 0 | 1085/985 | 1·102 (1·011–1·201) | 1·024 (0·983–1·068) | 0·260 | ||
| 1 | 1065/980 | 1·087 (0·996–1·185) | 1·018 (0·976–1·062) | 0·412 | ||
| ≥2 | 278/256 | 1·086 (0·917–1·287) | 1·017 (0·937–1·104) | 0·689 | ||
| 2005–10 | All | 3388/3051 | 1·110 (1·057–1·166) | 1·027 (1·003–1·051) | 0·029 | |
| 0 | 1972/1788 | 1·103 (1·035–1·176) | 1·018 (0·988–1·050) | 0·245 | ||
| 1 | 1193/1052 | 1·134 (1·044–1·232) | 1·038 (0·998–1·080) | 0·061 | ||
| ≥2 | 223/221 | 1·057 (0·876–1·275) | 1·011 (0·923–1·109) | 0·810 | ||
| 2011–15 | All | 6409/5945 | 1·078 (1·041–1·117) | 1·010 (0·922–1·027) | 0·286 | |
| 0 | 3739/3561 | 1·050 (1·003–1·099) | 0·995 (0·972–1·018) | 0·657 | ||
| 1 | 2287/2077 | 1·101 (1·038–1·168) | 1·019 (0·990–1·049) | 0·196 | ||
| ≥2 | 383/307 | 1·248 (1·074–1·449) | 1·084 (1·014–1·160) | 0·018 | ||
| Rest of South East | 1999–2004 | All | 1448/1353 | 1·070 (0·994–1·153) | 1·010 (0·974–1·047) | 0·595 |
| Asia region | 0 | 749/659 | 1·137 (1·024–1·262) | 1·038 (0·989–1·091) | 0·134 | |
| 1 | 445/431 | 1·032 (0·904–1·179) | 0·995 (0·932–1·062) | 0·870 | ||
| ≥2 | 254/263 | 0·966 (0·813–1·147) | 0·958 (0·877–1·046) | 0·335 | ||
| 2005–10 | All | 2919/2600 | 1·123 (1·065–1·183) | 1·031 (1·005–1·057) | 0·018 | |
| 0 | 1404/1292 | 1·087 (1·008–1·172) | 1·010 (0·974–1·048) | 0·576 | ||
| 1 | 990/840 | 1·179 (1·075–1·292) | 1·056 (1·012–1·102) | 0·012 | ||
| ≥2 | 525/467 | 1·124 (0·993–1·273) | 1·038 (0·979–1·102) | 0·213 | ||
| 2011–15 | All | 4098/3872 | 1·058 (1·013–1·106) | 1·000 (0·979–1·022) | 0·969 | |
| 0 | 1950/1871 | 1·042 (0·978–1·110) | 0·991 (0·960–1·022) | 0·560 | ||
| 1 | 1394/1338 | 1·042 (0·967–1·123) | 0·992 (0·956–1·030) | 0·692 | ||
| ≥2 | 752/661 | 1·138 (1·025–1·263) | 1·041 (0·991–1·094) | 0·109 |
Bold: M/F ratio point estimate above or below 1.04–1.06 with a 95% CI excluding the natural ratio of 1.05, or RR with P = <0·05.
Adjusted for maternal age.
Individual Australian-born year and parity group used as reference (Ref.) for the corresponding year and parity group from each of the other countries/regions.
When stratified for both time period and parity, the M/F ratios were also higher than expected in the most recent time period 2010-15 for Indian and Chinese births, most notably at parity ≥2 (India: M/F ratio 1.218; China: M/F ratio 1.248). Furthermore, the pattern of stepwise increasing M/F ratios with increasing parity was very similar for Indian and Chinese births in this most recent time period (Table 4 and Figure 3).
Figure 3.

Male-to-female ratios at birth by mother’s country or region of birth, stratified by time period and parity.
Discussion
This is the first study in Australia to show a systematic excess of male births to mothers born in India, China and the South East Asia region. The study is also unique in the world to show excess male births among multiple-birth infants in a population sample. The most notable findings were the stepwise increasing M/F ratios with increasing parity, and the high M/F ratios of parity ≥2 infants of Indian and Chinese-born mothers in the time period 2011-15 and of multiple births to Indian-born mothers. The results are consistent with previous evidence from other Western high-income countries, including Canada, Greece, Italy, Norway, the UK and the USA, where elevated M/F ratios have been observed following migration among infants of Indian,10–24,26 Chinese,10–14,19,26 and South East Asian-born mothers,16 particularly at higher-order births.
The findings are also consistent with a 2015 report by Special Broadcasting Service (SBS) radio based on national data from the Australian Bureau of Statistics (ABS), which indicated higher than normal M/F ratios at birth among infants of Chinese-born and Indian-born mothers between 2003 and 2013 (M/F ratios of 1.095 and 1.082, respectively).31 To our knowledge, the report has not been scientifically evaluated or published, and does not take into account the influence of parity or birth order.
Some of the previous studies from other Western high-income countries have addressed the influence of: the sex of previous siblings; the relationship between terminations and son birth; mixed nativity couples; and duration of residence in the new country, on M/F ratios and sex selection. In a study from the USA, it was shown that Indian mothers were significantly more likely to give birth to a boy if the previous births were girls, and more likely to terminate a pregnancy before the second or third birth if the previous births were girls.19 Studies from Italy11 and Canada21 show a relationship between previous terminations of pregnancy and a son birth among Chinese parents11 and Indian mothers.21 One Canadian study identified elevated M/F ratios at higher-order births also among couples with mixed nativity, including where the father was Indian-born and the mother Canadian-born.22 In another study, high M/F ratios were observed to persist independently of duration of residence in Canada among Indian immigrants.23
A novel finding of this study was the substantially elevated M/F ratio among multiple-birth infants of Indian-born mothers. M/F ratios are generally lower in multiple births compared with singleton births,13 as also indicated in this study. Multiple births are also more common after medically assisted compared with natural conception.32 The finding thus raises the question whether assisted reproduction and sex selection through IVF33 may have contributed to our findings. Sex selection via assisted reproduction for non-medical reasons is currently not allowed in Australia.7 However, Australian couples who want access to these services may choose to travel to international clinics. This issue, including that overseas clinics may not have the same standard of care as Australian clinics, was one of many factors raised by the National Health and Medical Research Council (NHMRC) in the discussion of sex selection for non-medical purposes in the 2017 review of ‘Ethical guidelines on the use of assisted reproductive technology in clinical practice and research’.7 The findings of this study can provide an important contribution to this continuing debate.
In the most recent years, a new method for prenatal diagnosis has been introduced in Australia, the Non-invasive Prenatal Testing (NIPT), which has facilitated identification of fetal sex with high accuracy at an early gestation.4 It has been discussed that NIPT has the potential to influence the rate of pregnancy terminations, as it can be used for expectant parents to act upon the results because of preference for one sex, for family balancing or for the purpose of influencing the sex in the birth order of children.4 Even though NIPT is still costly (approximately 450 AUD) and not publicly funded in Australia, an increasing demand has been observed.34 It is anticipated that this test will become more widely used as the price drops, because of its advantages in identifying genetic abnormalities and fetal sex earlier in pregnancy.4 Its implementation has also been shown to reduce the number of invasive diagnostic tests and also fetal losses related to these procedures.35 It is advisable to closely monitor its potential effect on birth sex ratios in the population, in parallel with its increasing uptake.
Interestingly, although Indian-, Chinese- and Vietnamese-born mothers share a birth country context where M/F ratios are significantly elevated at national levels,36 our findings indicate that the practice of sex selection may not continue with migration from Vietnam (on a scale large enough to distort sex ratios in this subgroup). One possible explanation for this finding may be differences between groups in relation to how similar or dissimilar the migrant population is to the general population of the birth country, including factors such as education, socioeconomic status, religion and desired family size. Another explanation may be that there are differences in the pace and level of assimilation between immigrant groups in Australia. Further research into underlying motives for sex selection after migration seems imperative, to disentangle why sex selection may continue within some ethnic communities but not others.
A surprising finding was the low proportion of higher-parity births among Indian-born mothers in this study. India has a relatively high fertility rate in comparison with the other country categories in this study sample (see Central Intelligence Agency, Table 136), and the results indicate a significant drop in fertility with migration. In the context of son preference, fertility decline has been shown to increase the tendency to turn to prenatal sex selection to increase the chance of a male birth,1 as the stopping rule (i.e. to continue to have children until a son is born) may not be a feasible option for couples who desire a small family. This may also explain why M/F ratios generally increase with parity in this context.1 The figures in Table 4 (also illustrated in Figure 3) show that M/F ratios were significantly elevated above the natural ratio for first births (parity 0) of Indian-born mothers in 2005-10, and higher for the first than subsequent births. This can possibly be explained by the fact that 64% of births to Indian-born mothers were of parity 0 in this time period (compared with 59% in the subsequent period) and, if couples wish to have only one child, they may act to influence the sex of the first birth. The substantially male-biased sex ratios seen at parity ≥2 for births of Indian and Chinese mothers in 2011-15 (1.22 and 1.25, respectively), have less of an effect on the overall M/F ratio, as the number of births is much smaller at these higher parities. This shows, however, the importance of taking parity into account in the investigation of potential sex-selective practices in populations. According to our calculations, the high M/F ratios at higher-parity births to Chinese and Indian mothers in 2011-15 indicate that for every 10th and 12th female born, respectively of parity two or higher, one female was de-selected either through termination of pregnancy or assisted reproductive treatment (calculations based on comparison with the M/F ratios of Australian-born mothers in the same parity category).
A few existing studies on sex ratios in Western high-income countries are based on population data covering the periods before and after the 1980s, which coincides with the introduction of fetal sex determination through ultrasound and the possibility of sex selection via assisted reproduction. These studies from the UK, USA and Norway provide evidence that sex selection rather than environmental or biological factors is behind the significantly elevated M/F ratios at birth in some immigrant populations, as the studies consistently show elevated M/F ratios in periods after the 1980s only.13,18–20,24
Although the World Health Organization has suggested a range of measures important for prevention of prenatal sex selection,37 there is a gap in the literature regarding interventions to address the phenomenon within migrant communities in Western high-income countries. It is imperative that these measures also address the social and cultural factors leading to son-preference and the social, economic and symbolic positions of females,3 including the values parents put on their sons and daughters.
Strengths and limitations
This study is the first of its kind in Australia, with important policy implications. The routinely collected population-based data have been shown to be largely accurate and complete in rigorously conducted validation studies,27,28 which eliminates the risk of response bias. We were unable to obtain data before 1999, however; because immigration from countries with high M/F ratios was low in the early periods of this study, the contribution of further data from earlier years would likely be limited. Other limitations include that we were not able to assess the influence of time since immigration, the number and sex of previous siblings, partner’s country of birth, second or subsequent generation migration, or other socioeconomic factors including education. It is important to note also that we are unable to draw conclusions about the individual contribution of assisted reproduction versus pregnancy termination to our findings.
Further research
The perinatal data collections across Australia collect data on a range of variables related to pregnancy and childbirth, in some states (including Victoria) also including total number of previous induced abortions and total number of previous spontaneous abortions, and if ART assisted the current pregnancy. Exploration of these variables could potentially provide further indications of whether the identified male-biased sex ratios are the result of sex-selective abortions or ART. Through data linkage with previous births, it would be possible also to analyse sex ratios based on the sex composition of siblings. This analysis is suggested to provide the most robust evidence of selective choices.1
Conclusions
This study provides evidence that prenatal sex selection may be taking place following migration to Australia. It is important that health policy makers support and strenghten population-based surveillance systems that allow for monitoring of birth outcomes, birth sex ratios (also by parity), and other relevant indicators for gender discriminatory practices in pregnancy and childbirth, to reinforce social policies to tackle gender discrimination in all its forms, including son preference, and to evaluate the adherence and effectiveness of such policies.
Funding
This work was supported by La Trobe University, Australia, and Umeå University, Sweden.
Supplementary Material
Acknowledgements
We are grateful to CCOPMM for providing access to the de-identified data used for this project and for the assistance of the staff at the Consultative Councils Unit, Safer Care Victoria, and to Stav Hillel, Senior Learning Adviser, La Trobe University Library, for assistance with the literature review. The conclusions, findings, opinions and views or recommendations expressed in this paper are strictly those of the authors. They do not necessarily reflect those of CCOPMM.
Author Contributions
K.E., A.A., R.P. and M-A.D. designed the study and K.E. and M-A.D. retrieved data. K.E. performed the literature search. K.E. and A.A. performed statistical analyses and K.E. drafted the manuscript including tables and figures. M-A.D., R.P. and A.A. provided important input on data interpretation, contributed to writing the manuscript and provided input on all drafts.
Conflict of interest: In addition to her university role, M-A.D. also works part-time at the Consultative Councils Unit at Safer Care Victoria. We declare no other potential competing interests.
References
- 1. Guilmoto CZ. The masculinization of births. Overview and current knowledge. Population 2015;70:183–244. [Google Scholar]
- 2. Bongaarts J, Guilmoto CZ.. How many more missing women? Excess female mortality and prenatal sex selection, 1970–2050. Pop Dev Rev 2015;41:241–69. [Google Scholar]
- 3. United Nations Population Fund. Sex Imbalances at Birth: Current Trends, Consequences and Policy Implications. Bangkok: UNFPA Asia and the Pacific Regional Office, 2012. [Google Scholar]
- 4. Chapman AR, Benn PA.. Noninvasive prenatal testing for early sex identification: a few benefits and many concerns. Perspect Biol Med 2013;56:530–47. [DOI] [PubMed] [Google Scholar]
- 5. Song S. Does famine influence sex ratio at birth? Evidence from the 1959–1961 Great Leap Forward Famine in China. Proc Biol Sci 2012;279:2883–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Helle S, Helama S, Lertola K.. Evolutionary ecology of human birth sex ratio under the compound influence of climate change, famine, economic crises and wars. J Anim Ecol 2009;78:1226–33. [DOI] [PubMed] [Google Scholar]
- 7. National Health and Medical Research Council. Ethical Guidelines on the Use of Assisted Reproductive Technology in Clinical Practice and Research. Canberra: National Health and Medical Research Council, 2017. [Google Scholar]
- 8. Parliament of Victoria. Assisted Reproductive Treatment Act 2008 (VIC). No. 76 of 2008. Melbourne, VIC: Parliament of Victoria, 2008.
- 9. Parliament of Victoria. Abortion Law Reform Act 2008 (VIC). No 58 of 2008. Melbourne, VIC: Parliament of Victoria, 2008.
- 10. Almond D, Sun Y.. Son-biased sex ratios in 2010 US Census and 2011-2013 US natality data. Soc Sci Med 2017;176:21–24. [DOI] [PubMed] [Google Scholar]
- 11. Ambrosetti EOL, Ciniza C, Marina A.. Sex imbalances at birth in migratory context: Evidence from Italy. Genus 2015;71:29–51. [Google Scholar]
- 12. Lhila A, Simon KI.. Prenatal health investment decisions: does the child's sex matter? Demography 2008;45:885–905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Egan JF, Campbell WA, Chapman A, Shamshirsaz AA, Gurram P, Benn PA.. Distortions of sex ratios at birth in the United States; evidence for prenatal gender selection. Prenat Diagn 2011;31:560–65. [DOI] [PubMed] [Google Scholar]
- 14. Almond D, Edlund L.. Son-biased sex ratios in the 2000 United States Census. Proc Natl Acad Sci USA 2008;105:5681–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Ray JG, Henry DA, Urquia ML.. Sex ratios among Canadian liveborn infants of mothers from different countries. CMAJ 2012;184:E492–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Almond D, Edlund L, Milligan K.. Son preference and the persistence of culture: evidence from South and East Asian immigrants to Canada. Pop Dev Rev 2013;39:75–95. [Google Scholar]
- 17. Auger N, Daniel M, Moore S.. Sex ratio patterns according to Asian ethnicity in Quebec, 1981–2004. Eur J Epidemiol 2009;24:17–24. [DOI] [PubMed] [Google Scholar]
- 18. Dubuc S, Coleman D.. An increase in the sex ratio of births to India-born mothers in England and Wales: evidence for sex-selective abortion. Popul Dev Rev 2007;33:383–400. [Google Scholar]
- 19. Abrevaya J. Are there missing girls in the United States? Evidence from birth data. Am Econ J Appl Econ 2009;1:1–34. [Google Scholar]
- 20. Singh N, Pripp AH, Brekke T, Stray-Pedersen B.. Different sex ratios of children born to Indian and Pakistani immigrants in Norway. BMC Pregnancy Childbirth 2010;10:40.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Urquia ML, Moineddin R, Jha P. et al. Sex ratios at birth after induced abortion. CMAJ 2016;188:E181–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Urquia ML, Ray JG, Wanigaratne S, Moineddin R, O'Campo PJ.. Variations in male-female infant ratios among births to Canadian- and Indian-born mothers, 1990-2011: a population-based register study. CMAJ Open 2016;4:E116–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Brar A, Wanigaratne S, Pulver A, Ray JG, Urquia ML.. Sex ratios at birth among Indian immigrant subgroups according to time spent in Canada. J Obstet Gynaecol Can 2017;39:459–64 e2. [DOI] [PubMed] [Google Scholar]
- 24. Tonnessen M, Aalandslid V, Skjerpen T.. Changing trend? Sex ratios of children born to Indian immigrants in Norway revisited. BMC Pregnancy Childbirth 2013;13:170.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Grech V. Further evidence of male offspring preference for certain subgroups in the United States (2007–2015). Early Hum Dev 2017;110:9–12. [DOI] [PubMed] [Google Scholar]
- 26. Gavalas V, Rontos K, Nagopoulos N.. Sex ratio at birth in twenty-first century Greece: the role of ethnic and social groups. J Biosoc Sci 2015;47:363–75. [DOI] [PubMed] [Google Scholar]
- 27. Davey MA, Sloan ML, Palma S, Riley M, King J.. Methodological processes in validating and analysing the quality of population-based data: a case study using the Victorian Perinatal Data Collection. Health Inf Manag 2013;42:12–19. [DOI] [PubMed] [Google Scholar]
- 28. Flood MM, McDonald SJ, Pollock WE, Davey MA.. Data accuracy in the Victorian Perinatal Data Collection: results of a validation study of 2011 data. Health Inf Manag 2017;46:113–26. [DOI] [PubMed] [Google Scholar]
- 29. Orvos H, Kozinszky Z, Bartfai G.. Natural variation in the human sex ratio. Hum Reprod 2001;16:803.. [DOI] [PubMed] [Google Scholar]
- 30. Mathews TJ, Hamilton BE.. Trend analysis of the sex ratio at birth in the United States. Natl Vital Stat Rep 2005;53:1–17. [PubMed] [Google Scholar]
- 31. SBS Radio. The News “It’s a Girl”, Still Unwelcome in Some Cultures in Australia. 19 Aug 2015. https://www.sbs.com.au/radio/storystream/news-its-girl-still-unwelcome-some-cultures-australia (19 May 2017, date last accessed).
- 32. Kulkarni AD, Jamieson DJ, Jones HW. et al. Fertility treatments and multiple births in the United States. N Engl J Med 2013;369:2218–25. [DOI] [PubMed] [Google Scholar]
- 33. Sills ES, Palermo GD.. Preimplantation genetic diagnosis for elective sex selection, the IVF market economy, and the child—another long day's journey into night? J Assist Reprod Genet 2002;19:433–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. McLennan A, Palma-Dias R, da Silva Costa F, Meagher S, Nisbet DL, Scott F.. Noninvasive prenatal testing in routine clinical practice—an audit of NIPT and combined first-trimester screening in an unselected Australian population. Aust N Z J Obstet Gynaecol 2016;56:22–28. [DOI] [PubMed] [Google Scholar]
- 35. O'Leary P, Maxwell S, Murch A, Hendrie D.. Prenatal screening for Down syndrome in Australia: costs and benefits of current and novel screening strategies. Aust N Z J Obstet Gynaecol 2013;53:425–33. [DOI] [PubMed] [Google Scholar]
- 36. Central Intelligence Agency. The World Factbook (Field Listings ′Sex Ratio′ and ′Total Fertility Rate′) 2017. https://www.cia.gov/library/publications/resources/the-world-factbook/fields/2018.html - 203 (19 May 2017, date last accessed).
- 37. World Health Organization. Preventing Gender-biased Sex Selection. An Interagency Statement OHCHR, UNFPA, UNICEF, UN Women and WHO Geneva: WHO, 2011.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.