

Abstract
The International Atomic Energy Agency (IAEA) through the International Action Plan on Radiation Protection of Patients and the International Commission on Radiological Protection have for some time carried out important efforts to assure that in the medical applications of the ionising radiations, the optimisation of radiological protection of patients is fundamental, to such a point that the IAEA includes it directly as a requirement for these practices (in its International Basic Safety Standards for Protection against Ionising Radiation and for the Safety of Radiation Sources (BSS)-GSR Part 1, 2011). For this reason, among the objectives of Regional Project RLA/9/057 and Regional Project RLA/9/067, the intention was to establish the dose references in conventional radiology for Latin America, for the purposes of determining whether these doses comply with the requirements of the BSS and to tend to improve practices, in order to minimise the dose received by the patients.
INTRODUCTION
The International Atomic Energy Agency (IAEA) and the International Commission on Radiological Protection have for some time carried out important efforts to assure that in the medical applications of the ionising radiations, the optimisation of radiological protection of patients is fundamental, to such a point that the IAEA includes it directly as a requirement for these practices [in its International Basic Safety Standards for Protection against Ionising Radiation and for the Safety of Radiation Sources (BSS)].
Work is normally performed with dosage guiding levels, which can then be used for institutions to compare with the dosages received by their patients, in order to review their working protocols and to optimise their practices to assure the effective protection on the patients involved.
For this reason, among the objectives of Regional Project RLA/9/57 and Regional Project RLA/9/67, the intention was to establish the dose references in conventional radiology for Latin America, for the purposes of determining whether these doses comply with the requirements of the BSS(1) and to improve practices, in order to minimise the dose received by the patients.
This work is a continuation of the one carried out in project ARCAL LXXV ‘Pilot Exercise for the Determination of Guidance Levels in General Radiography and Mammography in Latin America’, coordinated by the IAEA and PAHO.
The decision was taken to perform a sampling that would involve all of the countries and be divided into two phases:
In the first phase, basic information on the characteristics of the radiology centres, the type of equipment and the functioning characteristics with respect to personnel and technical controls was obtained. Data on the exposure parameters for each selected technique and for the observance of image quality criteria were also gathered.
In the first phase, a total of 34 health centres participated from the following countries. These data are presented in Table 1.
Table 1.
Countries and corresponding health centres that participated in phase 1.
| Country | Institutions |
|---|---|
| Argentina | 5 |
| Brazil | 7 |
| Costa Rica | 4 |
| Cuba | 2 |
| El Salvador | 1 |
| Guatemala | 3 |
| Honduras | 4 |
| Mexico | 1 |
| Nicaragua | 1 |
| Dominican Republic | 1 |
| Uruguay | 2 |
| Venezuela | 3 |
During the second phase, dose measurements were taken on conventional thoracic, spine and antero posterior (AP) X rays. In total, 628 thoracic dose determinations and 350 spine dose determinations in X rays were taken. A total of 27 health centres from different countries participated in this phase. The centres for each country are presented in Table 2.
Table 2.
Countries and corresponding health centres that participated in phase 2.
| Country | Institutions |
|---|---|
| Argentina | 5 |
| Brazil | 5 |
| Costa Rica | 5 |
| Cuba | 2 |
| El Salvador | 1 |
| Guatemala | 3 |
| Mexico | 1 |
| Nicaragua | 1 |
| Peru | 1 |
| Venezuela | 3 |
METHODOLOGY
First phase
This phase lasted from March 2008 to December 2009.
The data collection for the first phase with regard to information on each health centre and technical controls was performed through tables like the ones shown in Appendix 1, which were completed by a person designated specially to this work in each centre.
The surveyed institutions were classified according to the following types: private, public, small, medium, large, total amount of X-ray rooms and amount of equipment in the facility.
With respect to professional staff, information on the amount of medical radiologists, residents, technicians (with and without a radiology course) is obtained, and information is gathered with respect to the technician's years of experience, whether there are any medical physicists, whether quality control is made and whether a programme of equipment maintenance exists.
An assessment of the radiologic equipment, the environmental conditions of the rooms, the available resources of radiologic protection for the operator and the patient and the processing systems (analogical or digital) is made.
Each institution was also requested to send the protocols employed for the thoracic and spinal techniques. Finally, a request was made in this phase that the quality of the images obtained be evaluated by specialised professionals. An initial sample of 20 patients was requested, although this amount was not achieved by all participating institutions.
Finally, for the first phase, information on the image quality criteria for thoracic and spine X rays in their AP and lateral projections was required, following the recommendations of the European guidelines on quality criteria for diagnostic radiographic images.(2)
The image quality criteria for all three studies are summarised in the charts that appear in Appendix 2 and were completed in each health centre for the series of studies performed.
The information on the exposure parameters was obtained by requesting each centre to prepare tables in the X-ray rooms, for each practice performed. In this manner, the information was collected according to the patient's age and sex, their physical characteristics summed up in weight and thickness and also the exposure parameters: kVp, mA s, distance focus to X-ray film and distance focus to patient.
Second phase
This phase lasted from March 2010 to December 2011
For the second phase, and beginning with the performance measurements of the X-ray tubes, the skin-entrance air kerma values were calculated for each technique for a series of patients with anthropometric parameters (height, weight and thickness) within standard values.
For this purpose, calculation tables were used, which allow us to obtain the X-ray tube's performance values, from which the kerma values for each procedure and patient are then calculated. As a total, kerma values were obtained for 978 procedures.
Data for entrance surface air kerma in μGy for the studies considered in this data collection within Regional Project RLA/9/57-67 were obtained from the calculation table mentioned in the Methodology section, based on the performance of the X-ray tubes.
The procedure used for the kerma determinations was similar to the one used in the work carried out by Project ARCAL LXXV, which was announced in the publication ‘Pilot Exercise for the Determination of Guidance Levels in General Radiography and Mammography in Latin America’, which is transcribed in the following section.
Selection of the patients and radiological studies
Samples were taken of a minimum of 10 patients per each participating X-ray room, with the required observance for image quality, and two types of radiological tests were selected: one for thorax in its posteroanterior projection and one for the spine in its anteroposterior and lateral projections. The definition of adult patients for the purposes of this study is men and women between a height of 1.65 and 1.75 m and a weight between 65 and 75 kg.
Determination of entrance surface air kerma of the patient was performed following the Technical Report 457 from IAEA(3).Excel sheets were prepared for data collection and automatic calculation of entrance surface air kerma. This chart compiled data on age, sex, height and weight of patient. Also kVp, mA s, distance focus to X-ray film, distance focus to patient exposure parameters, size of X-ray film and entry dosage were requested.
RESULTS
Not all of the countries that participated in the first phase did so in the second phase.
First phase
Table 3 summarises the results for the health centres surveyed, with respect to size, personnel and quality control and equipment maintenance:
Table 3.
The results on the health centres surveyed, with respect to size, personnel and quality control and equipment maintenance.
| Country | # | Priv. | Publ. | Large | Med. | Small | Number of radiologists | Technicians with course | Medical physicist | Quality control | Maintenance |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Argentina | 5 | 3 | 2 | 3 | 2 | 35 | 183 | 0 | 3 | 5 | |
| Brazil | 7 | 2 | 5 | 3 | 4 | 42 | 255 | 1 | 2 | 5 | |
| Costa Rica | 4 | 1 | 3 | 3 | 1 | 21 | 83 | 0 | 0 | 3 | |
| El Salvador | 2 | 2 | 1 | 1 | 6 | 33 | 0 | 2 | 2 | ||
| Guatemala | 3 | 1 | 2 | 3 | 15 | 78 | 0 | 1 | 2 | ||
| Honduras | 4 | 1 | 3 | 4 | 16 | 82 | 0 | 1 | 2 | ||
| Nicaragua | 2 | 2 | 1 | 1 | 7 | 13 | 0 | 2 | 2 | ||
| Dom. Rep. | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | |||
| Uruguay | 2 | 2 | 1 | 1 | 6 | 14 | 0 | 0 | 1 | ||
| Venezuela | 4 | 1 | 3 | 3 | 1 | 31 | 102 | 0 | 0 | 1 | |
| 34 | 12 | 22 | 22 | 11 | 2 | 180 | 844 | 1 | 12 | 24 |
According to Table 3, it can be observed that 65 % of the surveyed centres are public, and a similar percentage shows that there are centres with high workloads.
Only one of them has a Medical Physicist working in diagnostic radiology, and only 35 % of the centres perform some type of quality control.
As a general norm, it can be observed that the technicians who work at the surveyed centres have approved some type of radiology course.
Table Table 4 shows the average values of the exposure parameters that emerged from the survey.
Table 4.
The average values of the exposure parameters that emerged from the survey.
| kVp | mA s | |
|---|---|---|
| Thorax | 97 | 16 |
| AP Spinal | 86 | 27 |
| AL Spinal | 86 | 60 |
AP, antero posterior.
With respect to the degree of performance of the image quality criteria(2), as observed in Figure 1 for the case of the thorax, it is true that although the performance percentage is >80 % for all criteria, two, seven and eight are <85 %.
Figure 1.

Performance percentage of the image quality criteria items for thoracic X ray (see Appendix 1).
In the case of the spine in its anteroposterior projection, criteria one, five and seven have the lowest performance (Figure 2), and for the lateral projection, the least satisfying criterion is two (Figure 3).
Figure 2.

Performance percentage of the image quality criteria for spine X ray in anteroposterior projection.
Figure 3.

Performance percentage of the image quality criteria for spine X ray in lateral projection.
In general, it can be affirmed that in conventional radiology, positioning is vital for a good image quality.
Second phase
The reference dose corresponding to the respective procedures was estimated as the 75th percentile of the data population.
In Table 5 the calculated values are presented, expressed in all cases as mGy, and the guidance levels of the basic norms.
Table 5.
The calculated values , expressed in all cases as mGy, and the guidance levels of the basic norms.
| Amount of centres | Average dose (mGy) | Reference level (mGy) | Guidance level BSS (mGy) | |
|---|---|---|---|---|
| Thorax | 50 | 0.19 | 0.28 | 0.15–0.30 |
| AP spinal | 28 | 4.12 | 4.76 | 5.0–10.0 |
| AL spinal | 25 | 9.47 | 10.49 | 15.0–30.0 |
| Period up to 2009 DRL (mGy) | 2009–2011 DRL (mGy) | |||
| Thorax | 0.38 | 0.28 | ||
| AP spinal | 5.91 | 4.76 | ||
| AL spinal | 12.31 | 10.49 | ||
In Figure 4a–c the values obtained by country, for thorax, AP spinal and AL spinal, respectively, can be observed.
Figure 4.
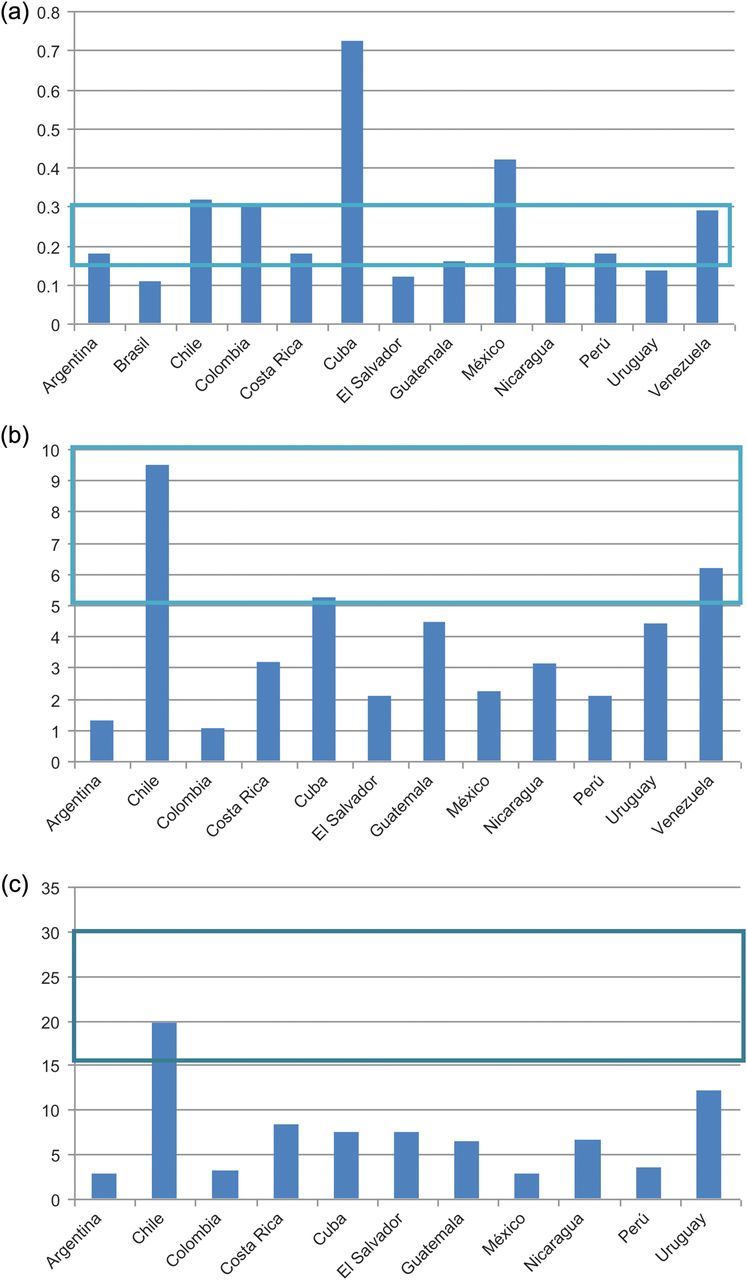
Average values per country of entrance surface air kerma compared with the recommended dosage in the BSS, in mGy for (a) thorax, (b) antero posterior spinal and (c) AL spinal.
CONCLUSIONS
When this survey was being made, digital technology was not widespread, and for this reason, only results of analogical equipment are presented.
The analysis carried out on the exposure parameters of the three types of radiological studies revealed a large statistical dispersion, which suggests that a wide variety of criteria were employed by the radiological technicians, while working with the same equipment and even for centres of the same country, the large variation in the technical factors generate a dispersion in the 75th percentile. This is indicative that efforts should be made to optimise radiographic techniques.
The same is suggested with respect to the anthropometric characteristics of the patients.
Analysing the dose reference values for Latin America obtained in this work, a decrease can be observed with respect to those obtained in the sample of Project ARCAL 75 (see Table 5), which suggests that these types of actions tend towards decrease in the doses received by the patients. Although during the authors’ study period, a dosage decrease was noticed in the referenced centres, it must not be forgotten that in their work some institutions that employ fast screens were included, while the BSS reference values are considered for slow screens.
Appendix 1: Table used for the information survey of the centres.
| Type of institution |
| Private |
| Public |
| Small |
| Medium |
| Large |
| Total amount of X-ray rooms |
| Total amount of equipment in the institution |
| Fixed conventional X ray |
| Portable conventional X ray |
| Mammography |
| Tomography |
| Fluoroscopy |
| Processer |
| Number of professionals in the institution |
| Medical radiologists |
| Medical residents |
| Technicians with radiology course |
| Technicians without radiology course |
| Amount of technicians with experience in radiology? |
| How many with experience <2 y |
| How many with experience of 2–5 y |
| How many with experience of 5–10 y |
| How many with experience >10 y |
| Does the facility have a medical physicist? |
| Is there a quality control programme implemented? |
| Is it performed by the medical physicist? |
| Is it performed by the technician? |
| Is it performed by an external engineer? |
| Is IAEA protocol used? |
| Is ACR protocol used? |
| Is Spanish protocol used? |
| Other? |
| Assessment of radiological equipment |
| Equipment brand |
| Equipment model |
| Tube brand |
| Tube model |
| Year of manufacture |
| Installation date |
| Range of kV |
| Range of mA s |
| Is the equipment analogical? |
| Is the equipment digital? |
| Automatic exposure control? |
| Focal spot marked on housing? |
| Is the total filtration value indicated? |
| Is there an audible or luminous indication on the command console to reveal radiation emission? |
| Is it possible to see and maintain contact with the patient? |
| Is the luminous indication of the radiation field functioning? |
| Equipment maintenance |
| Is there a preventive maintenance programme? |
| Is it internal? |
| Supplied by the manufacturer or representative? |
| Supplied by an external company? |
| Is there a contract? |
| Maintenance frequency: biannual? |
| Maintenance frequency: annually? |
| Maintenance frequency: every 2 y? |
| Other? |
| Environmental conditions of the room |
| Is there air conditioning in the mammography equipment room? |
| Is the air conditioning functioning? |
| Does the room have reinforcement? |
| Are the doors reinforced? |
| Is there a luminous indicator on the door? |
| Is there a radioprotection sign on the door? |
| Protection measures for the operator and the patient |
| Is there a fixed barrier or window lead shielding? |
| What material is the barrier made of? |
| Are there protection aprons in the room? |
| How many? |
| Do technicians use a personal dosemeter? |
| Is it a film dosemeter? |
| Is it TLD? |
| Other dosemeters? |
| Assessment of processing systems |
| Do you use an X-ray film to obtain image? |
| Do you use CR to obtain image? |
| Do you use DR to obtain image? |
| In the case of Digital Radiology: |
| Model of CR cassettes? |
| Brand of CR cassettes? |
| Model of DR detector? |
| Brand of DR detector? |
| Can the images be extracted? |
| In ‘for processing’ format? |
| In ‘for processing’ format? |
| Brand of the workstation monitor? |
| Model of the workstation monitor? |
| Is the workstation monitor CRT type? |
| Is the workstation monitor LCD type? |
| Matrix size of workstation monitor? |
| Does the software of the monitor belong to the workstation? |
| In the case of radiographic film |
| Brand? |
| Model? |
| Type of screen? |
| Is the process of the film manual? |
| Is the process of the film automatic? |
| Brand of processer? |
| Model of processer? |
| Developer temperature? |
| Total processing time? |
| Is the variation between the value of measured time and the one indicated on the equipment acceptable? (Tolerance: <±3 % with respect to the value indicated by the manufacturer) |
| If you have a thermometer measure the temperature of the developer |
| Is the variation between the measured value and the one indicated on the equipment acceptable? (Tolerance: ±0.5 with respect to the value indicated by the manufacturer) |
| Is there evidence of stains or scratches in the films after the process? |
| Darkroom inspection |
| Is there a ventilation system? |
| Is it functioning? |
| Is the floor non-slip, waterproof and anticorrosive? |
| Is the room clean? |
| Can you perceive a strong odour of liquid developer? |
| Is there an extractor fan? |
| Is the white light switch located in places where it cannot be activated involuntarily? |
| Is the safety light at a distance of more than 120 cm from the surface? |
| Is the power of the safety light lower or equal to 15 W? |
| Are there signs of infiltration or dampness on the walls? |
| Are the boxes of film in vertical position and organised? |
| Are there entries of light in the darkroom? |
| Are the films organised by their expiry date? |
| Amount of negatoscopes |
| Can you observe stains at a first glance? |
| Are there luminosity differences in the negatoscope? |
| Is there a magnifying glass? |
| Can you vary the intensity of the negatoscope? |
| Can you disguise the image of the X ray? |
| Can you vary the intensity of the observation room? |
| If you have a photometer, measure the luminance of the negatoscope |
| Is the measured value acceptable? (tolerance: luminance: 1500 cd m−2) |
| Uniformity of the negatoscope |
| Is the measured value acceptable? (Tolerance: Uniformity: <15 %) |
| Illumination of the viewing room |
| Is the measured value acceptable? (tolerance: illumination: <100 lux) |
APPENDIX 2: IMAGE QUALITY CRITERIA FOR THORACIC AND SPINE X RAYS IN THEIR AP AND LATERAL PROJECTIONS, FOLLOWING THE RECOMMENDATIONS OF THE EUROPEAN GUIDELINES ON QUALITY CRITERIA FOR DIAGNOSTIC RADIOGRAPHIC IMAGES.
| Quality criteria-thorax |
| 1. Image performed in deep inspiration, evaluated from (6 anterior and 10 posterior) ribs above the diaphragm and holding breath |
| 2. Symmetrical reproduction of the thorax shown by the central position of the spinous process between the medial clavicular heads |
| 3. Medial aspect of the scapula outside of the lung parenchyma |
| 4. Complete reproduction of the thoracic cage above the diaphragm |
| 5. Clear visualisation of the vascular pattern in all the lung, particularly the peripheral vessels |
| 6. Clear visualisation of: |
| (a) trachea and principal bronchial tubes |
| (b) borders of the heart and aorta |
| (c) diaphragm and costophrenic angles |
| 7. Visualisation of the retrocardiac lung and mediastinum |
| 8. Visualisation of the spine through the heart shadow |
| Quality criteria: AP spinal view |
| 1. Clear visualisation of the surface of the superior and inferior vertebral endplates, as a single line, in the central part of the X-ray beam |
| 2. Clear visualisation of the pedicles |
| 3. Visualisation of the intervertebral spaces |
| 4. Visualisation of the spinous and transverse processes |
| 5. Clear visualisation of the cortex and the trabecular structures |
| 6. Visualisation of adjacent soft tissue, particularly of the psoas muscle |
| 7. Visualisation of the sacroiliac articulation |
| Quality criteria: lateral spinal view |
| 1. Precise visualisation of the surface of the superior and inferior vertebral endplates, as a single line, with visualisation of the intervertebral space |
| 2. Total superposition of the posterior borders of the vertebrae |
| 3. Visualisation of the pedicles and of foramina |
| 4. Visualisation of the spinous processes |
| 5. Precise visualisation of the cortex and the trabecular structures |
References
- 1.IAEA. International Atomic Energy Agency; 2011. IAEA safety standards: radiation protection and safety of radiation sources. International Basic Safety Standards. [Google Scholar]
- 2.European Commission. Office for Official Publications of the European Communities; 1996. European guidelines on quality criteria for diagnostic radiographic images. Directorate-General XII: Science, Research and Development. [Google Scholar]
- 3.IAEA. International Atomic Energy Agency; 2007. Technical Reports Series No. 457. [Google Scholar]