

Abstract
Background. Staphylococcus aureus bacteremia (SaB) carries considerable morbidity and mortality. We examined the predictive value of serum concentrations of interleukin (IL)–10, proinflammatory cytokines, and terminal complement on patient survival and SaB duration.
Methods. Clinical information on consecutive patients with SaB at a tertiary medical center were collected prospectively. Patient serum samples obtained at the day of clinical presentation were assayed for tumor necrosis factor–α, IL-1β, IL-10, and complement membrane attack complex C5b-9 concentrations using enzyme-linked immunoassay. Logistic regression identified predictors of mortality and duration of bacteremia.
Results. In 59 patients with SaB, 14% died and 17% had prolonged bacteremia (>4 days). Elevated IL-10 serum concentrations (>7.8 pg/mL) identified all 8 patients who died, whereas there were no deaths in patients with normal IL-10 (P = .016). The lack of an IL-1β response (≤0.45 pg/mL) defined all patients with SaB >4 days. In multivariate analysis, patient age (odds ratio [OR], 1.16; P = .022), duration of bacteremia (OR, 1.16; P = .031), and serum IL-10 (OR, 1.05; P = .014) were identified as independent predictors of patient mortality.
Conclusions. SaB mortality was confined strictly to patients with elevated IL-10 concentrations. We recommend that future clinical trials of SaB stratify patients according to IL-10 and IL-1β serum concentrations in order to better evaluate the impact of therapeutic interventions on patient outcome.
Patients with Staphylococcus aureus bacteremia (SaB) experience a wide spectrum of disease severity, bacteremia duration, and clinical outcomes. This heterogeneity suggests case-by-case variation in the host inflammatory response and cytokine signaling. Examining the broader literature regarding patients with fever, an increased ratio of the anti-inflammatory cytokine interleukin (IL)–10 to the proinflammatory cytokine tumor necrosis factor–α (TNF-α) was predictive of increased mortality [1]. The relative contributions of host genetics and pathogen virulence factors to this balance are poorly understood, but recent evidence suggests that circulating bacterial peptidoglycan may play an important role in increasing IL-10 concentrations [2]. Peptidoglycan-driven IL-10 can attenuate T-helper (Th) 1/Th17 adaptive immunity against S. aureus, thus indicating a potential detrimental effect of this cytokine upon patients with SaB [3].
The clinical relevance of complement has not been thoroughly defined in patients with SaB. The fact that S. aureus has evolved elaborate schemes of complement evasion [4] suggests a pivotal role in pathogenesis of infection. Recent data from animal models correlate complement activation and protection from S. aureus bacteremia and associated septic complications [5, 6]. S. aureus peptidoglycan may mediate leukopenia and thrombocytopenia through activation of the host complement system [7].
Several threads of published evidence point to an attenuated host inflammatory response accompanying reduced vancomycin susceptibility in S. aureus, particularly in vancomycin-intermediate S. aureus (VISA), with potential clinical consequences. For example, changes in cell surface structures in heterogeneous VISA and VISA strains were associated with significantly reduced nuclear factor κ–B activation in macrophages, resulting in reduced TNF-α and IL-1β expression [8]. A clinical study demonstrated an inverse relationship between vancomycin minimum inhibitory concentration (MIC) and the incidence of septic shock [9]. Subsequent clinical data revealed that the increased mortality associated with VISA is not dependent on alterations in antibiotic therapy, suggesting that the higher vancomycin MIC may be a marker of pathogenicity, perhaps via an immune-evasive phenotype, rather than inferior antibiotic potency [10].
The goal of this study was to examine the clinical relevance of host immune response, including select proinflammatory and anti-inflammatory cytokines and terminal complement in patients with SaB at presentation and prior to the institution of antibiotic therapy. These immunologic data were then examined collectively with clinical and pathogen characteristics in univariate and multivariate logistic regression analyses to determine their impact on duration of bacteremia and mortality prior to discharge.
METHODS
Patient and Isolate Identification and Collection
Consecutive patients with blood cultures growing methicillin-susceptible (MSSA) or methicillin-resistant S. aureus (MRSA) from April 2009 through March 2010 at the University of Wisconsin Hospital (a 493-bed academic medical center in Madison, WI) were identified and analyzed for this study. Patients were included if at least 2 positive blood cultures were identified, or 1 positive culture was congruent with a clinical diagnosis of SaB. The institutional review board reviewed and approved the study prior to patient inclusion and sample collection.
Patient demographics, clinical infection and inflammation markers, and infection source were collected upon initial presentation. Clinical markers of infection and inflammation relative to SaB included vital signs (temperature, blood pressure, pulse, respiratory rate) and blood work (peripheral blood white blood cell count, erythrocyte sedimentation rate, and C-reactive protein). The bacteremia source was classified into 3 groups based on confirmed or suspected foci: (1) noncatheter primary endovascular, encompassing endocarditis and unknown or presumed endovascular sources; (2) secondary to another primary nonendovascular focus of infection (eg, lung, soft tissue, bone/joint); or (3) catheter source. Patient serum samples were obtained at the initial onset of presentation of SaB and stored at –80°C until analysis. This was possible because routine clinical blood samples obtained from patients at the time of their hospital admission are routinely stored at 4°C for 5 days. Once a case of SaB was identified, a study investigator gathered the stored blood taken upon admission, collected and froze the serum until time for analysis.
Initial S. aureus blood culture isolates were obtained from the clinical microbiology laboratory upon identification of a positive specimen.
S. aureus Genotypic and Phenotypic Assays
All laboratory analyses were performed by investigators blinded to outcome data. Antibiotic susceptibility testing was performed for vancomycin, daptomycin, linezolid, and telavancin by broth microdilution according to Clinical and Laboratory Standards Institute guidelines [11] and/or Etest according to the manufacturer (bioMerieux, Marcy l'Etoile, France). S. aureus clonal spa typing analysis was done following the method of Koreen et al [12]. The spa type identification was performed using the Ridom StaphType (version 2.1.1) software (Ridom GmbH, Wurzburg, Germany). The spa clonal complex was determined using BURP (based upon repeat patterns) algorithm [13]. Repeat-duplication and -excision in addition to substitution and base-insertion and -deletion events were taken into account when the relatedness of different spa types was calculated.
Quantification of Serum Cytokine and Terminal Complement Concentrations
Serum cytokine concentrations were determined by high-sensitivity, quantitative sandwich enzyme-linked immunoassay (ELISA) according to manufacturer's instructions (R&D Systems, Minneapolis, MN) for TNF-α (normal range in healthy subjects: 0.55–2.8 pg/mL), IL-1β (0.125–0.45 pg/mL), and IL-10 (0.78–7.8 pg/mL). Complement C5b serum concentrations were determined by membrane attack complex C5b-9 ELISA having a minimum detection of 0.46 ng/mL, with healthy subjects having undetectable concentrations (BD Biosciences Pharmigen, San Diego, CA). Samples were allowed to thaw at room temperature only once before testing to prevent protein degradation. All assays were performed in duplicate and measured for absorbance at 490 nm within 30 minutes of final preparation.
Clinical Outcomes
The primary clinical outcomes were in-hospital mortality prior to discharge and duration of bacteremia while receiving appropriate antistaphylococcal antibiotic therapy. Duration of bacteremia was categorized into 2 subsets: prolonged and short-term bacteremia based on Classification and Regression Tree (CART) methodology to determine the optimal threshold (days duration) for predicting mortality. Total duration of bacteremia included cases of persistent bacteremia (consecutive days of positive blood cultures) and microbiologic relapse (ie, recurrence of a positive blood culture after the first negative culture) while receiving antibiotic treatment. All subjects were prospectively observed during the course of therapy, and all clinical information was collected prior to isolate characterization and cytokine serum concentration measurements.
Statistical Methods
Immunological marker concentrations between groups were compared with a 2-sample t test or nonparametric Wilcoxon rank sum test if the markers did not meet criteria for Gaussian distribution. The percent of patients with normal and abnormal cytokine concentrations for the primary clinical outcomes (mortality and duration of bacteremia) were compared using Fisher exact test. Univariate analysis followed by multivariate logistic regression analysis was conducted to evaluate the associations between each of the immunological markers (as continuous variables) and the primary clinical outcomes. Odds ratios (ORs) and the corresponding 95% confidence intervals (CIs) were reported. The original nonparsimonious multivariate model included all markers, which were identified as at least marginally significant (P < .10) predictors in the univariate mortality analysis as well as other clinically important characteristics (eg, age, gender, duration of bacteremia). Predictive variables were then selected via forward stepwise selection with a P value cutoff of <.10. A previously deleted variable was allowed to reenter the final model if its P value was <.10. The likelihood ratio test was used to compare models. CART methodology [14] and receiver operating characteristic (ROC) analysis were performed to identify threshold values for selected (significant) predictors in order to classify patients into mortality groups. All P values were 2-sided and significance was defined as P < .05.
RESULTS
Clinical and Microbiological Characteristics
Fifty-nine consecutive adult patients (age: mean 58.9 years, median 58 years, range 21–92 years; 64% male) with S. aureus bacteremia (duration: median 2 days; mean 5.3 ± 11.7 days, range 1–65 days) were identified and included in the analysis. The most frequent source of bacteremia was from a secondary source (63%), most notably from pneumonia or deep-seated abscesses, followed by primary endovascular (25%) and catheter sources (12%).
MRSA was the causative pathogen in 21 cases (36%). Vancomycin MICs by Etest ranged from 0.38 to 2 mg/L, with only 20% yielding MICs >1 mg/L (1.5 mg/L—10 isolates; 2 mg/L—1 isolate). The vancomycin MIC50 was higher with Etest compared to broth dilution (1 mg/L vs 0.5 mg/L, respectively). The genotypic analysis revealed considerable heterogeneity, with 30 spa types among 59 isolates: spa type t002 was the most common (n = 11) followed by t008 (n = 9) and t012 (n = 4). The remaining spa types were represented by less than 4 isolates (Supplemental Figure 1).
Overall, the mortality rate in patients with S. aureus bacteremia was 14%, consistent with prior studies. The comparison of patient and organism characteristics between patients who survived versus those who died is presented in Table 1. Primary endovascular noncatheter infection was significantly associated with patient death (P = .030). The mean severity of illness index (Acute Physiology and Chronic Health Evaluation II score) was higher, but not significantly different in those who died compared to survival. The most common comorbidity in this population was diabetes (36%) followed by respiratory failure (19%) and renal failure/hemodialysis (5%).
Table 1.
Comparison of Patient and Organism Characteristics Stratified According to Survival Outcome
| Patient Characteristic | Survived (n = 51) | Died (n = 8) | P Value |
|---|---|---|---|
| Age, years (mean ± SD) | 57 ± 16 | 68 ± 18 | .226a |
| Gender: female, no. (%) | 17 (33%) | 4 (50%) | .360b |
| APACHE II scorec | 9.2 ± 5.2 | 13.8 ± 7.6 | .178a |
| Source | |||
| Primary: endovasculard | 10 (20%) | 5 (62%) | .030b |
| Secondarye | 34 (67%) | 3 (38%) | .135b |
| Catheter-associated | 7 (14%) | 0 (0%) | .578b |
| Duration of bacteremia, days | 3.3 ± 3.5 | 17.9 ± 28.8 | .567a |
| Immunologic response on admission (serum concentrations) | |||
| TNF-α (pg/mL) | 4.5 ± 4.7 | 15.2 ± 15.4 | .011a |
| IL-1β (pg/mL) | 9.9 ± 13.7 | 10.0 ± 7.5 | .511a |
| IL-10 (pg/mL) | 18.8 ± 3.6 | 84.1 ± 97.1 | .001a |
| IL10 : TNF-α | 4.6 ± 5.2 | 9.3 ± 13.4 | .228a |
| Complement C5b-9 (ng/mL) | 7933 ± 4800 | 6804 ± 6849 | .292a |
| MRSA | 19 (37%) | 2 (25%) | .700b |
| Vancomycin MIC, Etest | |||
| ≤1 mg/L | 42 (82%) | 6 (75%) | .322b |
| >1 mg/L | 9 (18%) | 2 (25%) |
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; IL, interleukin; MIC, minimum inhibitory concentration; MRSA, methicillin-resistant S. aureus; TNF, tumor necrosis factor.
a Wilcoxon test or t test; or bPearson test.
c APACHE II scores available on 49 of 59 patients on the first day of bacteremia (43/51 survived and 6/8 died).
d Includes endovascular, endocarditis, or unknown presumed to be endovascular.
e Includes any site secondary to another primary nonendovascular focus of infection.
Association of Cytokine Concentrations at Clinical Presentation to Patient Mortality
Cytokine concentrations on the first day of bacteremia in all patients were often higher than the upper limit of normal in healthy individuals for terminal complement C5b-9 (100% of patients), IL-1β (92%), IL-10 (59%), and TNF-α (52%). Significantly higher mean serum concentrations of TNF-α (15.2 ± 15.4 pg/mL vs 4.5 ± 4.7 pg/mL; P = .011) and IL-10 (84.1 ± 97.1 pg/mL vs 18.8 ± 3.6 pg/mL; P = .001) were noted among patients who died versus those that survived, while there were no differences in mean IL-1β or C5b-9 concentrations between patients who died versus survived.
We compared the percent of patients presenting on the first day of bacteremia with elevated cytokine concentrations to survival outcome (Table 2). Of note, all 8 patients who died had IL-10 concentrations above the normal range (>7.8 pg/mL), while no deaths occurred in those patients with normal IL-10 concentrations (P = .016). These same patients had elevated IL-1β concentrations (>0.45 pg/mL), but elevated concentrations also occurred in 90% of patients who survived and therefore this marker was not a significant outcome predictor. Interestingly, only 5 patients with SaB had normal IL-1β concentrations, all of which survived.
Table 2.
Mortality and Survival of Patients With S. aureus Bacteremia Stratified by Normal or Elevated Cytokine Concentrations
| Cytokine Concentration | Outcome |
P Valuea | |
|---|---|---|---|
| Death (n = 8) | Survival (n = 51) | ||
| IL-10 | |||
| Normal (≤7.8 pg/mL) | 0 (0%) | 24 (48%) | .016 |
| Elevated (>7.8 pg/mL) | 8 (100%) | 27 (52%) | |
| TNF-α | |||
| Normal (≤2.8 pg/mL) | 2 (25%) | 26 (51%) | .259 |
| Elevated (>2.8 pg/mL) | 6 (75%) | 25 (49%) | |
| IL-1β | |||
| Normal (≤0.45 pg/mL) | 0 (0%) | 5 (10%) | .998 |
| Elevated (>0.45 pg/mL) | 8 (100%) | 46 (90%) | |
| Complement C5b-9b | |||
| ≤6440 ng/mL | 5 (63%) | 25 (49%) | .707 |
| >6440 ng/mL | 3 (37%) | 26 (51%) | |
Abbreviations: IL, interleukin; TNF, tumor necrosis factor.
a Fisher exact test.
b Cohorts for complement are derived from the patient median in this study, because C5b-9 concentrations in healthy patients are undetectable.
CART Analysis Comparing of Duration of Bacteremia and Mortality
CART identified the duration of bacteremia threshold for predicting mortality at 4.5 days, establishing our definition of prolonged bacteremia as >4 days duration. Of note, 2 of the patients who died had relapsing bacteremia with 64 and 65 days between positive cultures, which were included in the duration analysis. Sources of infection were similar between both duration groups, and neither methicillin resistance nor vancomycin MIC had an impact on duration of bacteremia.
Association of Cytokine Concentrations at Clinical Presentation to Duration of Bacteremia
In comparing the serum cytokine concentrations between those patients with bacteremia ≤4 days versus >4 days, lower concentrations of C5b-9 were noted in cases of prolonged bacteremia (P = .08; Table 3). Conversely, elevated serum concentrations of IL-1β appeared to be highly protective against prolonged bacteremia (P < .001). Univariate analysis examining the association of complement C5b-9 serum concentration to duration of bacteremia did not reach statistical significance (OR 1.00, 95% CI 0.99–1.01; P = .306). Failure to achieve statistical significance may have been due to the high variability in C5b–9 concentrations in the 2 duration cohorts and relatively low prevalence of prolonged bacteremia in our study, with only 10 patients with >4 days’ bacteremia duration.
Table 3.
Duration of Bacteremia, ≤4 d Versus >4 d Duration, in Patients With S. aureus Bacteremia Stratified by Normal or Elevated Cytokine Concentrations
| Cytokine Concentration | Outcome |
P Valuea | |
|---|---|---|---|
| Bacteremia ≤4 d (n = 49) | Bacteremia >4 d (n = 10) | ||
| IL-10 | |||
| Normal (≤7.8 pg/mL) | 21 (43%) | 3 (30%) | .506 |
| Elevated (>7.8 pg/mL) | 28 (57%) | 7 (70%) | |
| TNF-α | |||
| Normal (≤2.8 pg/mL) | 24 (49%) | 4 (40%) | .734 |
| Elevated (>2.8 pg/mL) | 25 (51%) | 6 (60%) | |
| IL-1β | |||
| Normal (≤0.45 pg/mL) | 0 (0%) | 5 (50%) | <.001 |
| Elevated (>0.45 pg/mL) | 49 (100%) | 5 (50%) | |
| Complement C5b-9b | |||
| ≤6440 ng/mL | 22 (45%) | 8 (80%) | .080 |
| >6440 ng/mL | 27 (55%) | 2 (20%) | |
Abbreviations: IL, interleukin; TNF, tumor necrosis factor.
a Fisher exact test.
b Cohorts for complement are derived from the patient median in this study, because C5b-9 concentrations in healthy patients are undetectable.
Multivariate Analysis and ROC Analysis for Predicting Patient Mortality in S. aureus Bacteremia
Multivariate logistic regression analysis was conducted to evaluate the association between the cytokine markers, duration of bacteremia and mortality. Stepwise analysis was used to identify a parsimonious logistic regression model. The results of the final parsimonious multivariate logistic regression model for mortality are presented in Table 4. In the 59 patients with S. aureus bacteremia, 3 independent predictors of patient mortality were identified: (1) duration of bacteremia >4 days (OR 1.159; P = .031); (2) increased patient age (OR 1.158; P = .022); and (3) elevated serum concentrations of IL-10 (OR 1.050; P = .014). These results show that each day of bacteremia raises the probability of death by 15.9%, each year increase in age raises the probability of death by 15.8%, and every 1 pg/mL increase in serum IL-10 concentration raises the probability of death by 5%. The ROCs for predicting mortality with duration of bacteremia, age, TNF-α, and IL-10 are shown in Figure 1.
Table 4.
Multivariate Logistic Regression Model With Independent Predictors of Mortality
| Variable | OR | 95% CI | P value |
|---|---|---|---|
| Bacteremia duration, per day | 1.16 | 1.01–1.32 | .031 |
| Age, per year | 1.16 | 1.02–1.31 | .022 |
| IL-10, per pg/mL | 1.05 | 1.01–1.08 | .014 |
Abbreviations: CI, confidence interval; IL, interleukin; OR, odds ratio.
Figure 1.
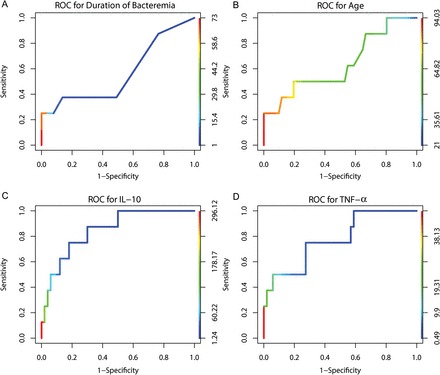
Receiver operating characteristic (ROC) curve for duration of bacteremia for predicting mortality. A, Duration of bacteremia (days). B, Age (years). C, IL-10 (pg/mL). D, TNF-α (pg/mL). Abbreviations: IL, interleukin; TNF, tumor necrosis factor.
DISCUSSION
Despite the high prevalence of SaB, the host innate immune response as it relates to clinical presentation and outcome remains poorly characterized in humans. This study attempted for the first time to integrally evaluate certain key parameters of the immunologic host response alongside clinical and pathogen characteristics with patient outcome. As anticipated, a highly heterogeneous host immune response in SaB was observed, with variable serum concentrations of (1) the anti-inflammatory cytokine IL-10, (2) proinflammatory cytokines TNF-α and IL-1β, and (3) terminal complement components C5b-9 complex.
Nevertheless, some very significant novel findings emerged from this analysis, with the most notable being that: (1) a normal serum IL-10 serum concentration, found in 48% of patients with SaB, represented a sine qua non for patient survival; (2) the lack of an IL-1β response was pathognomonic among patients with a bacteremia of >4 days. The same 4-day breakpoint was identified by regression tree modeling as predictive of mortality. We propose that >4 days be considered the definition of “prolonged” SaB based on the fact that this breakpoint was derived from both clinical and immunologic data in this study. While duration of SaB has been one of the strongest predictors of patient mortality, the components of the immune response driving mortality and duration appear separate. It is worth re-emphasizing that these cytokine concentrations were sampled at the same point in time for all patients—the time of clinical presentation and before the institution of antimicrobial therapy. This eliminates the variables of antimicrobial selection and other differences in clinical management (eg, timing of surgical intervention, infectious disease consultation, etc.) in influencing the host immune response and clinical outcome.
Our results suggest that patient outcomes in SaB rest heavily upon, or are reflected meaningfully in, the innate immune response of the host, in addition to well-established factors such as bacteremia duration and patient age (Table 4). The finding that induction of an anti-inflammatory cytokine (IL-10) and lack of induction of a proinflammatory cytokine (IL-1β) appear clinically detrimental underscore the importance of host cytokine modulation by S. aureus in the pathogenesis of invasive disease.
Elevated IL-10 concentration may signal an important marker of immune response dysregulation or “immunoparalysis” via induction of apoptosis of antigen-presenting cells [2]. Potentially significant insights as to the detrimental effect of IL-10 on the immune response to S. aureus are presented recently by Froderman et al [3], which suggest that S. aureus peptidoglycan may play an important role in increasing IL-10 concentrations. Toll-like receptor (TLR) 2 on antigen-presenting cells enables recognition of peptidoglycan-embedded lipopeptides and glycopolymers in the staphylococcal cell wall and can induce either an inflammatory or immunomodulatory (IL-10) response. These investigators showed that the IL-10 response preferentially occurs upon CD14- and CD36-independent TLR2 signaling, triggering phosphoinositide 3-kinase activation in monocytes and monocyte-derived macrophages. In contrast, monocyte-derived dendritic cells produce mostly IL-12 and IL-23, triggering a proinflammatory T-helper response. TLR2 signaling by S. aureus may explain the variable immune response and consequence clinical outcomes in S. aureus infection [3]. Other explanations to the variable IL-10 and other cytokine responses could include differences in peptidoglycan burden (bacterial inoculum). This may be the reason for the higher mortality observed in this study and others previously in primary endovascular SaB-like endocarditis. Finally, an anti-inflammatory effect by a heightened IL-10 response may dampen clinical symptoms and thus delay patients' seeking medical attention. While our analysis of patients on the day of clinical presentation eliminated confounders of medical care heterogeneity, there is no way for investigators to control the time to seek medical attention by patients.
Our present data are consistent with prior work demonstrating higher mortality with an increased anti-inflammatory immune response in patients with fever [1]. It remains unclear if this increased IL-10 response is directly responsible for increased risk of death or if it is a marker of a host characteristic, pathogen virulence factor, or host–pathogen interaction that is the culprit. At the onset of the study, we wished to examine the vancomycin and methicillin susceptibility of S. aureus and their relationship to the immune response. We did not find any significant differences in IL-10 serum concentrations or mortality between patients with MSSA versus MRSA. We were unable to examine the impact of reduced susceptibility to vancomycin phenotype on the host inflammatory response as only 19% of the isolates had vancomycin Etest MICs >1 mg/L. However, the finding that nonelevated serum concentrations of IL-1β track with survival and prolonged bacteremia provide a potential underlying reason for the recent finding that heteroresistant VISA bacteremia does not alter mortality despite persisting in the bloodstream, and VISA is less capable of inducing IL-1β in mouse macrophages [8].
Recent data from animal models suggest an association between complement activation and protection from S. aureus bacteremia and associated septic complications [5, 6]. C5 deficiency results in impairment of bacterial clearance, increased metastatic complications, and death [6]. We hypothesized that complement function on initial presentation might influence duration of bacteremia and, consequently, mortality. Although the number of patients with prolonged bacteremia in our study was low, a significant inverse association between C5b-9 and duration was observed, indicating that patients with low complement levels during the induction of the infection are at risk for prolonged duration or relapse of bacteremia.
Additional studies are needed to further investigate the impact of C5a and C5b-9 response, not only at the onset, but also throughout the infection course in patients with bacteremia. The possibility exists that complement concentrations may have been low prior to bacteremia, either through physiologic or pathologic conditions. For example, a host whose serum complement proteins are depleted at baseline prior to the onset of S. aureus bacteremia (as may occur in hemodialysis patients) [15, 16] may be at increased risk for a prolonged bacteremia.
Some limitations of our study warrant discussion. First, the small sample size, resulting in a relatively low absolute number of patients who died or who had prolonged bacteremia, posed limitations on the ability to demonstrate significance for some of the characteristic trends noted in logistic regression. Additional studies with larger cohorts will help to determine the significance of these trends. Secondly, our analysis of the host immune response was prioritized to only a few key factors, which have been shown in previous studies to be significant in sepsis outcome. Similar analyses are needed for other components of the host cytokine and complement systems. There were other confounding factors that were not controlled in this study, mainly intensive care unit stay and infection source control, and antibiotic therapy. Finally, although our study was observational, molecular typing revealed considerable heterogeneity in organism genetic background. Furthermore, data acquisition was obtained at a sharply defined microbiological and clinical point in the illness (the day of clinical presentation) and therefore did not hinge on more diffuse clinical definitions characteristic of many clinical observational studies, allowing for elimination of the confounders of heterogeneity in treatment that may influence outcome (eg, antimicrobial therapy, infectious disease consultant management bias).
One of the most interesting observations regarding vancomycin therapy for MRSA bacteremia is the discrepancy between clinician dissatisfaction with its performance and the lack of data to show superiority of any alternative new agent. Given the exclusionary criteria of many registry clinical trials, we hypothesize that many of the exclusionary criteria are confining analysis of patients to the immunologically low-risk patients with respect to cytokine response. We would greatly anticipate any future studies to examine differences in efficacy of antibiotics among patients stratified by immune response (eg, serum concentrations of IL-10, IL-1β).
In conclusion, this study identified host response characteristics that may be significant in determining patient outcome in SaB, both in terms of patient mortality and duration. While bacteremia >4 days and increased patient age were significant and previously established predictors of patient death, elevated IL-10 serum concentrations were independently highly predictive of death. An elevated IL-1β response precisely defined the subset of patients (49 of 59) who subsequently cleared SaB in 4 days or less. Patient screening for abnormally elevated IL-10 serum concentrations upon presentation to the hospital on the initial day of SaB may improve effective triage and treatment of those with a high risk of mortality. We propose that immunologic stratification of patients with SaB using ELISA to measure IL-10 and IL-1β serum concentrations be used to select antibiotic therapy and to perform clinical trials in evaluating future therapies. Further studies of the host immune response in SaB may provide insights into novel immunotherapies for this disease.
Supplementary Material
Notes
Acknowledgments. We thank the Toni Ziegler and University of Wisconsin clinical laboratories and for assistance with patient sample collection and cytokine assays.
Financial support. This work was supported by the Sharp Healthcare Foundation (San Diego, CA) for laboratory analyses performed in this study. The funding source was not involved in the design and conduct of the study; data analysis and interpretation; or preparation, review, and approval of the manuscript.
Potential conflicts of interest. W. E. R. received grant funding and is speaker honoraria for Cubist, received grant funding from Astellas, and consults for The Medicines Company and Visante; G. S. consults, received grant funding, and is speaker honoraria for Cubist; consults and is speaker honoraria for Astellas; and is speaker honoraria for Pfizer. All other authors report no potential conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
References
- 1.van Dissel JT, van Langevelde P, Westendorp RG, Kwappenberg K, Frolich M. Anti-inflammatory cytokine profile and mortality in febrile patients. Lancet. 1998;351:950–3. doi: 10.1016/S0140-6736(05)60606-X. [DOI] [PubMed] [Google Scholar]
- 2.Chau TA, McCully ML, Brintnell W, et al. Toll-like receptor 2 ligands on the staphylococcal cell wall downregulate superantigen-induced T cell activation and prevent toxic shock syndrome. Nat Med. 2009;15:641–8. doi: 10.1038/nm.1965. [DOI] [PubMed] [Google Scholar]
- 3.Frodermann V, Chau TA, Sayedyahossein S, Toth JM, Heinrichs DE, Madrenas J. A modulatory interleukin-10 response to staphylococcal peptidoglycan prevents Th1/Th17 adaptive immunity to Staphylococcus aureus. J Infect Dis. 2011;204:253–62. doi: 10.1093/infdis/jir276. [DOI] [PubMed] [Google Scholar]
- 4.Jongerius I, Kohl J, Pandey MK, et al. Staphylococcal complement evasion by various convertase-blocking molecules. J Exp Med. 2007;204:2461–71. doi: 10.1084/jem.20070818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cerquetti MC, Sordelli DO, Ortegon RA, Bellanti JA. Impaired lung defenses against Staphylococcus aureus in mice with hereditary deficiency of the fifth component of complement. Infect Immun. 1983;41:1071–6. doi: 10.1128/iai.41.3.1071-1076.1983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.von Kockritz-Blickwede M, Konrad S, Foster S, Gessner JE, Medina E. Protective role of complement C5a in an experimental model of Staphylococcus aureus bacteremia. J Innate Immun. 2009;2:87–92. doi: 10.1159/000247157. [DOI] [PubMed] [Google Scholar]
- 7.Spika JS, Peterson PK, Wilkinson BJ, et al. Role of peptidoglycan from Staphylococcus aureus in leukopenia, thrombocytopenia, and complement activation associated with bacteremia. J Infect Dis. 1982;146:227–34. doi: 10.1093/infdis/146.2.227. [DOI] [PubMed] [Google Scholar]
- 8.Howden BP, Smith DJ, Mansell A, et al. Different bacterial gene expression patterns and attenuated host immune responses are associated with the evolution of low-level vancomycin resistance during persistent methicillin-resistant Staphylococcus aureus bacteraemia. BMC Microbiol. 2008;8:39. doi: 10.1186/1471-2180-8-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Soriano A, Marco F, Martinez JA, et al. Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Clin Infect Dis. 2008;46:193–200. doi: 10.1086/524667. [DOI] [PubMed] [Google Scholar]
- 10.Holmes NE, Turnidge JD, Munckhof WJ, et al. Antibiotic choice may not explain poorer outcomes in patients with Staphylococcus aureus bacteremia and high vancomycin minimum inhibitory concentrations. J Infect Dis. 2011;204:340–7. doi: 10.1093/infdis/jir270. [DOI] [PubMed] [Google Scholar]
- 11.Clinical and Laboratory Standards Institute. Wayne, PA: Clinical and Laboratory Standards Institute; 2010. 20th informational supplement (M100-S20) Performance standards for antimicrobial susceptibility testing. [Google Scholar]
- 12.Koreen L, Ramaswamy SV, Graviss EA, Naidich S, Musser JM, Kreiswirth BN. spa typing method for discriminating among Staphylococcus aureus isolates: implications for use of a single marker to detect genetic micro- and macrovariation. J Clin Microbiol. 2004;42:792–9. doi: 10.1128/JCM.42.2.792-799.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mellmann A, Weniger T, Berssenbrugge C, et al. Based Upon Repeat Pattern (BURP): an algorithm to characterize the long-term evolution of Staphylococcus aureus populations based on spa polymorphisms. BMC Microbiol. 2007;7:98. doi: 10.1186/1471-2180-7-98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Breiman L, Friedman J, Stone CJ, Olshen RA. Classification and regression tress. Monterey, CA: Wadsworth International Group; 1984. [Google Scholar]
- 15.Gasche Y, Pascual M, Suter PM, Favre H, Chevrolet JC, Schifferli JA. Complement depletion during haemofiltration with polyacrilonitrile membranes. Nephrol Dial Transpl. 1996;11:117–9. [PubMed] [Google Scholar]
- 16.Koller H, Hochegger K, Zlabinger GJ, Lhotta K, Mayer G, Rosenkranz AR. Apoptosis of human polymorphonuclear neutrophils accelerated by dialysis membranes via the activation of the complement system. Nephrol Dial Transpl. 2004;19:3104–11. doi: 10.1093/ndt/gfh500. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.