

Abstract
Background:
Soccer has a high injury rate, with lateral ankle sprains being a common injury. Therefore, an approach to prevent or at least reduce the occurrence is warranted. Injury prevention can be improved by identifying specific risk factors and individuals at risk.
Purpose:
To assess drop-jump landing performance as a potential predictor of lateral ankle sprain within 3-year follow-up.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Single-legged drop-jump landing tests were performed by 190 elite soccer players. Based on ground-reaction forces, 6 outcome measures were calculated that aim to reflect the impact and stabilization phase. Lateral ankle sprains were registered during up to 3 years of follow-up. Following a z score correction for age, a multivariate regression analysis was performed.
Results:
During follow-up, 45 players (23.7%) suffered a primary lateral ankle sprain. Of those, 34 were regarded as severe (absence >7 days). Performance was related to increased risk of ankle sprain (P = .005 for all sprains and P = .001 for severe sprains). Low mediolateral stability for the first 0.4 seconds after landing (a larger value indicates more force exerted in the mediolateral direction, resulting in rapid lateral stabilization) and high horizontal ground-reaction force between 3.0 and 5.0 seconds (a smaller value indicates less sway in the stabilization phase) were identified as risk factors. A player that scored 2 SD below average for both risk factors had a 4.4-times-higher chance of sustaining an ankle sprain than a player who scored average.
Conclusion:
The current study showed that following a single-legged drop-jump landing, mediolateral force over 0 to 0.4 seconds and/or mean resultant horizontal ground-reaction force over 3 to 5 seconds has predictive value with regard to the occurrence of an ankle sprain among male elite soccer players within 3 years.
Keywords: injury, football, proprioception, balance, motor control
Soccer is the most popular sport worldwide.8 Top-level players (UEFA Champions League) sustain about 30 injuries per 1000 match hours, resulting in absence (mean, 18.5 days)32 and high costs (about €18,000 [US $21,000] a day).6 About 11% of soccer injuries are ankle ligament injuries36; therefore, an approach to prevent or at least reduce the occurrence of lateral ankle sprains is warranted.15
One way is to expose all players to a general injury prevention protocol, such as the FIFA 11+ program, which can be used as a warm-up routine.4,31 This reduced the occurrence of ankle injuries by 32%.31 Alternatively, one could opt for a more tailor-made approach by first identifying those players at risk for a certain injury and targeting them with an intervention. To validate a screening test to predict and prevent sports injuries, the test needs to show a strong relationship with injury risk in prospective studies.1 Some studies specifically identified risk factors for ankle sprains among male soccer players.5,7 However, to date there is no validated screening test available.1
Since exercises that focus on core stability, balance, and jumping help to reduce the incidence of ankle sprains, dynamic tests (eg, landing and stabilizing after a single-legged jump) may help to identify risk factors.13,22,23,33 Recently, it was shown that a selection of outcome measures based on ground-reaction force (GRF) could increase the usefulness of the single-legged drop-jump landing test (Huurnink A, Fransz DP, de Boode VA, Kingma I, van Dieën JH. “How Do Different Time Periods After Single-Leg Drop Jump Landing Affect Postural Stability Indices and Time to Stabilization? A Methodological Study,” 2018). Therefore, our goal is to assess the relationship between previously selected GRF outcome measures from single-legged drop-jump landing tests and the risk of sustaining a lateral ankle sprain. We hypothesize that the performance on a single-legged drop-jump landing test, accompanied by adequate outcome measure selection, will be related to injury risk.
Methods
Participants
A total of 190 highly talented male soccer players of the AFC Ajax Youth Academy (U13, U15, U17, U19, first, and second teams) participated in the current study. These players are regularly tested as part of a larger testing program developed to monitor player performance in a variety of motor tasks. The current performance data set was acquired at the start of the 2012-2013 (cohort 1, n = 138) and 2013-2014 (cohort 2, n = 52) seasons. At the time of measurements, all players were fit to perform at the highest standard of competitive soccer matches. Player characteristics are presented in Table 1. All participants were informed in advance of the procedures involved in the testing program. Parental consent and participant assent were collected, and approval was granted by the ethical review board of the Department of Human Movement Sciences, Vrije Universiteit Amsterdam (ECB 2014-80) in accordance with the Declaration of Helsinki.
Table 1.
Participant Characteristics, Arranged per Team Category a
| Age, y |
Height, cm |
Weight, kg |
Follow-up, y |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Team | n | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| U13 | 34 | 11.8 | 0.6 | 151.8 | 7.8 | 40.8 | 6.0 | 2.8 | 0.4 |
| U15 | 45 | 13.9 | 0.6 | 166.1 | 8.8 | 53.9 | 9.1 | 2.6 | 0.7 |
| U17 | 43 | 15.7 | 0.8 | 175.4 | 6.5 | 65.2 | 10.2 | 2.7 | 0.7 |
| U19 | 44 | 17.7 | 0.7 | 179.8 | 6.5 | 72.9 | 8.5 | 2.2 | 0.8 |
| First and second | 24 | 23.2 | 3.2 | 182.0 | 6.1 | 77.0 | 7.5 | 2.1 | 0.9 |
U13 to U19 are the youth teams under the age of 13, 15, 17, and 19 years. The first team played Eredivisie and Champions League (2012-2013 and 2013-2014) and the second team, Beloftencompetitie (2012-2013) and Jupiler League (2013-2014).
Performance
Test Procedures
The players were asked to perform a single-legged drop-jump landing by jumping from an aerobic step of 20-cm height, which was placed 5 cm behind a force plate covered with an antislip rubber surface and located 4 m from the wall. Players were instructed to take off with 2 feet, land on the testing leg, stabilize as quickly as possible, and subsequently balance for 15 seconds with their hands on their hips while keeping all other movement to a minimum and their eyes fixed on a visual target on the wall (Figure 1 and Appendix Video, available in the online version of this article). No instructions with regard to jump height were given. All players completed the regular warm-up as accustomed before a training session. This warm-up (about 15 minutes) consisted of jogging 2 laps around the field, followed by dynamic stretch exercises and subsequent 5 × 50–m runs at approximately 80% of maximum pace. One practice trial per leg was performed before actual testing commenced. Both legs were tested twice for cohort 1 and 3 times for cohort 2, owing to a change of protocol over time to improve reliability. To minimize the procedural burden, the order of legs was not randomized. Instead, the left leg was the initial testing leg. To avoid bias attributed to variation caused by shoe properties, all trials were performed without shoes but with socks. A trial was invalid, discarded, and repeated if a player touched the floor with the contralateral leg or if arm movement was used to regain balance.
Figure 1.

Stills from video registration (Appendix Video, available in the online version of this article). The images show a player just before impact on the force plate.
Instrumentation and Signal Processing
GRFs in the vertical, anteroposterior, and mediolateral directions were recorded at 1000 samples per second with a 40 × 60–cm AMTI force plate (type BP400600HF; Advanced Medical Technologies Inc). A custom MATLAB program (The Mathworks) was written for all data processing. The raw GRF data were cropped from time of impact (vertical GRF >10 N) to 12 seconds after impact. Subsequently, the GRF data were related to the participant’s body weight, which was calculated as the mean vertical GRF from 6 to 12 seconds. Data were low-pass filtered at 12 Hz with a bidirectional second-order Butterworth filter.18
Outcome Measures
Previous research showed that a time series following a single-legged drop-jump landing consists of 4 distinct phases, with each phase holding unique information.11 Since we aimed to identify potential information with regard to the risk of sustaining an ankle sprain, we selected only those outcome measures applicable to the impact and dynamic phases11-13 (Huurnink et al, unpublished data, 2018). Even more so, the selected outcome measures should form a representation of the different directions of force; hence, we selected 6 outcome measures:
Peak force V and peak force AP: Peak vertical GRF and peak anteroposterior GRF13—the maximum GRF per trial for vertical and anteroposterior directions (registered in Newton, corrected for body weight; Huurnink et al, unpublished data, 2018)
RMS ML 0.4: Root mean square of the GRF in the mediolateral direction with regard to the first 0.4 seconds after landing—the square root of the mean square of the first 400 samples of the mediolateral GRF (the root mean square is always larger than the mean value of a signal, since peak values are of greater influence; Huurnink et al, unpublished data, 2018)
Hor GRF dyn and Hor GRF late dyn: Mean resultant horizontal GRF during the dynamic phase (0.4-2.4 seconds) and the late dynamic phase (3.0-5.0 seconds)11—the mean resultant of the GRF in the anteroposterior and mediolateral directions for the identified phases
TTS VRAW 1.5: Time to stabilization with the raw signal in the vertical direction, the threshold set at ±5% body weight,24,27 and the signal to remain within threshold for 1.5 seconds (Huurnink et al, unpublished data, 2018)—time to stabilization is supposedly the time that it takes for an individual to return to a baseline or stable state after a perturbation.
The 6 selected outcome measures are illustrated in Figure 2.
Figure 2.

Illustration of the 6 selected outcome measures based on the ground-reaction forces (GRFs) (y-axis) and time series (x-axis): (A) peak force V and TTS VRAW 1.5, (B) Hor GRF dyn and Hor GRF late dyn, and (C) RMS ML 0.4 and peak force AP. See Outcome Measures section for definitions. BW, body weight.
Injuries
Club medical staff doctors and physical therapists documented all injuries that occurred from the 2012-2013 season to the 2015-2016 season. We considered injuries that occurred at the lateral ankle and were classified as “sprain” or “ligamentous injury” (thus including any diagnosis caused by the spraining mechanism). For those injuries, we recorded the number of days between testing and injury occurrence. Furthermore, we considered the number of days that the player was unfit to participate in training or matches after the sprain as a measure of injury severity. If a second sprain occurred within the observed seasons (either a recurrence in the initially sprained ankle or a first sprain in the contralateral ankle), this was recorded as well.9,10 We regarded an injury duration of more than a week a severe ankle sprain.26
We did not include each player’s medical history as a confounder. A recent study showed that past injury did not predict future injury in a multivariate analysis incorporating physical performance tests, whereas the univariate analysis did show predictive capacity.16 This implies that a possible effect of past injury on performance should affect physical performance testing and that performance on a physical test has a stronger relationship with future injury than past injury.16 As each player was fit to perform at the highest standard of competitive soccer matches at the time of performance testing, we expected no functional limitations.
Statistical Analysis
Statistical analysis was done with SPSS Statistics for Mac (v 21.0; IBM). Since performance on a single-legged drop-jump landing test is a measure of total-body sensorimotor function, we used the person, not the leg, as the unit of analysis.19,35 If a difference between legs exists, this would be very small.17 Furthermore, albeit in a static single-legged stance, previous research showed no difference between the kicking leg and stance leg.21 Therefore, results of all trials (for both legs) were averaged within players.
To control the outcome values for age, we calculated corresponding z scores. Calculations were done according to methods previously described (Huurnink et al, unpublished data, 2018).17 Age effects were assessed with linear regression between the (transformed) outcome values and age. Z scores were calculated with the following formula: (value – mean value) / SD. We used a Cox proportional hazards univariate regression analysis for the 6 GRF outcome measures as independent variables and (severe) injury as the dependent variable. Furthermore, we performed a multivariate regression analysis (forward conditional) with the 6 outcome measures as independent variables.2
Results
Participants
The numbers of players for both cohorts are shown in Tables 2 and 3 by season and follow-up duration. Each year, around 15% of the players left the club as a result of the ongoing selection process. None of these departures were injury related.
Table 2.
Number of Players for Each Cohort per Season: 2012-2016
| 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |
|---|---|---|---|---|
| Cohort 1 | 138 | 117 | 94 | |
| Cohort 2 | 52 | 42 | 35 |
Table 3.
Number of Players for Each Cohort per Follow-up Length: 1-3 Years
| 1 y | 2 y | 3 y | |
|---|---|---|---|
| Cohort 1 | 21 | 23 | 94 |
| Cohort 2 | 10 | 7 | 35 |
| Total | 31 | 30 | 129 |
Performance
The unstandardized GRF outcomes are shown in Table 4. Age-matched z scores were calculated and expressed in terms of SDs from their means. Consequently, these z scores have a distribution with a mean of 0 and an SD of 1.
Table 4.
Outcome Values for the Selected GRF Outcome Measures, Arranged per Team Category a
| U13 |
U15 |
U17 |
U19 |
First and Second |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Measure | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Peak force V | 279.94 | 28.43 | 270.75 | 25.13 | 270.99 | 27.39 | 261.28 | 24.23 | 267.09 | 17.86 |
| Peak force AP | 37.90 | 5.29 | 35.20 | 4.38 | 35.02 | 4.14 | 35.45 | 4.91 | 33.40 | 3.46 |
| RMS ML 0.4 | 4.26 | 0.74 | 4.48 | 0.90 | 4.41 | 0.77 | 4.69 | 0.99 | 4.22 | 0.82 |
| Hor GRF dyn | 1.79 | 0.57 | 1.69 | 0.45 | 1.57 | 0.38 | 1.59 | 0.39 | 1.35 | 0.22 |
| Hor GRF late dyn | 0.92 | 0.29 | 0.86 | 0.17 | 0.79 | 0.16 | 0.81 | 0.20 | 0.71 | 0.09 |
| TTS VRAW 1.5, s | 1.30 | 0.68 | 1.20 | 0.56 | 0.98 | 0.39 | 0.95 | 0.37 | 0.78 | 0.20 |
Values are presented as percentage body weight unless noted otherwise. See Outcome Measures section for definitions. GRF, ground-reaction force.
Injuries
In total, during 3 years of follow-up, 45 players (23.7%) suffered a primary lateral ankle sprain. Ten players experienced at least 1 second sprain. The mean ± SD number of days that a player was unfit to participate in training or matches was 17.7 ± 11.9 days (range, 3-54 days). A detailed overview is presented in Table 5.
Table 5.
Overview of the Occurrence of Ankle Sprains, Severity, and Reinjuries, Arranged per Team Category
| Sprains |
Severe |
Days |
Second Sprain |
|||||
|---|---|---|---|---|---|---|---|---|
| Team | n | % | Severe | % | Mean | Range | n | % |
| U13 a | 10 | 29 | 8 | 80 | 17.0 | 9-36 | 1 | 10 |
| U15 | 14 | 31 | 12 | 86 | 22.6 | 6-54 | 3 | 21 |
| U17 | 8 | 19 | 4 | 50 | 17.6 | 3-34 | 1 | 13 |
| U19 | 10 | 23 | 5 | 50 | 10.8 | 5-24 | 5 | 50 |
| First and second | 3 | 13 | 3 | 100 | 19.7 | 13-23 | 0 | 0 |
| Total | 45 | 32 | 10 | |||||
For 2 of the 10 sprains, the length of injury was unknown; therefore, the number of severe sprains and the number of days injured may be underestimated.
Since 20 to 50 injury cases are needed to detect moderate to strong associations,2 this sample size suffices for an analysis of the primary sprains. In contrast, the number of second sprains was too low to permit further analysis. We regarded an injury duration of more than a week as a severe ankle sprain, resulting in 34 sprains available for further analysis on severe injuries.
Statistical Analysis
The results of the Cox regression analyses are shown in Table 6 for all ankle sprains (n = 45) and for the severe ankle sprains (n = 32).
Table 6.
Univariate and Multivariate Analysis (Forward Model) for All Sprains and Severe Sprains a
| 95% CI for Exp(B) |
||||
|---|---|---|---|---|
| Risk Factor | P Value | Exp(B) | Lower | Upper |
| All sprains (n = 45) | ||||
| Univariate | ||||
| Peak force V | .149 | 0.802 | 0.594 | 1.082 |
| Peak force AP | .767 | 0.953 | 0.696 | 1.306 |
| RMS ML 0.4 | .017 | 0.680 | 0.496 | 0.933 |
| Hor GRF dyn | .747 | 1.051 | 0.776 | 1.424 |
| Hor GRF late dyn | .072 | 1.296 | 0.977 | 1.720 |
| TTS VRAW 1.5 | .763 | 0.954 | 0.705 | 1.292 |
| Multivariate b | ||||
| RMS ML 0.4 | .007 | 0.656 | 0.481 | 0.893 |
| Hor GRF late dyn | .029 | 1.377 | 1.034 | 1.834 |
| Severe sprains (n = 32) | ||||
| Univariate | ||||
| Peak force V | .026 | 0.678 | 0.481 | 0.955 |
| Peak force AP | .182 | 0.775 | 0.533 | 1.127 |
| RMS ML 0.4 | .012 | 0.613 | 0.419 | 0.898 |
| Hor GRF dyn | .362 | 1.183 | 0.824 | 1.699 |
| Hor GRF late dyn | .016 | 1.486 | 1.077 | 2.051 |
| TTS VRAW 1.5 | .426 | 1.168 | 0.797 | 1.711 |
| Multivariate c | ||||
| RMS ML 0.4 | .005 | 0.596 | 0.413 | 0.858 |
| Hor GRF late dyn | .006 | 1.573 | 1.135 | 2.178 |
Exp(B) is the ratio of the hazards between 2 players whose outcome value on the risk factor differs by 1 unit (z score) when all other covariates are held constant. Bold values indicate a significant effect (P < .05). See Outcome Measures section for definitions. GRF, ground-reaction force.
Forward step 2 (P = .005).
Forward step 2 (P = .001).
The univariate analyses for all ankle sprains showed that the RMS ML 0.4 holds a significant predictive capacity (P = .017) (Table 6, Figure 3). In the univariate analyses for severe ankle sprains, the RMS ML 0.4 and 2 other risk factors (peak force V and Hor GRF late dyn) had significant predictive capacity. A high peak force V reduces the chances of a severe ankle sprain, and a high value for Hor GRF late dyn increases this risk.
Figure 3.
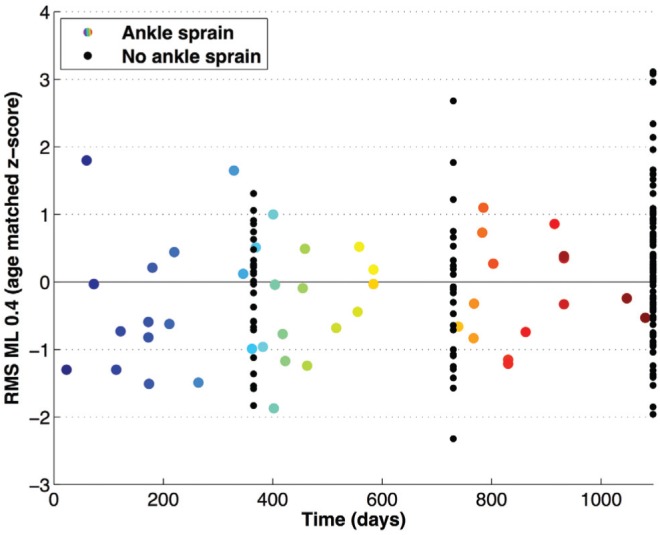
Scatterplot of all players regarding follow-up length and z score of RMS ML 0.4. The multicolored dots represent the corresponding RMS ML 0.4 z score (y-axis) for those players who sustained an ankle sprain at a certain moment in time (x-axis). The black dots signify the z scores at end of follow-up for the players who did not sustain an ankle sprain (hence, the vertical lines of dots at 1, 2, and 3 years). See Outcome Measures section for definitions.
In the multivariate analysis with regard to the prediction of all ankle sprains, the RMS ML 0.4 and Hor GRF late dyn combined into a significant risk factor model (P = .005), in which both outcome measures were significant as well (P = .007 and P = .029, respectively). For the severe ankle sprains (ie, absence >7 days), a similar model was significant (P = .001). Figure 4A shows the composed risk chart with the hazard ratio compared with the z scores in RMS ML 0.4 and Hor GRF late dyn with regard to all ankle sprains. A player that scored 2 SD below average for both risk factors had a 4.4-times-higher chance of sustaining an ankle sprain than a player who scored average (Figure 4B).
Figure 4.
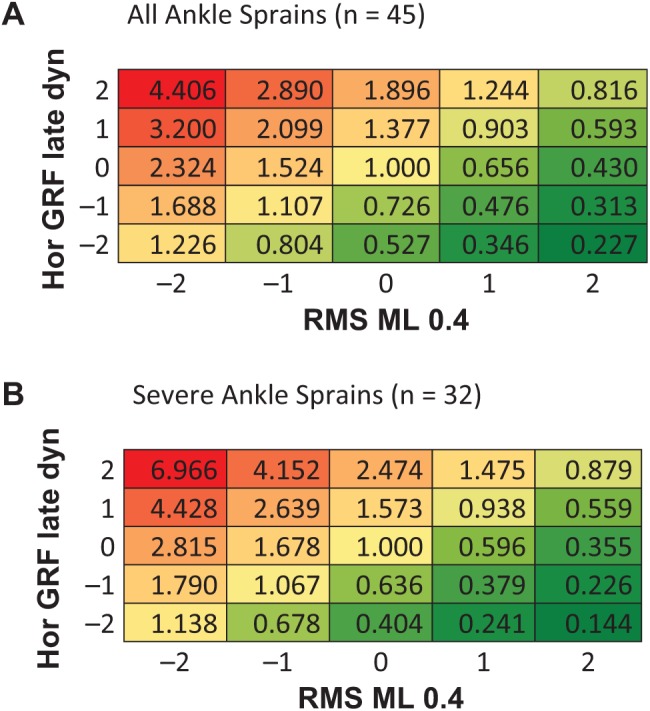
Risk chart with regard to (A) all ankle sprains and (B) the severe sprains; z scores of 0 for RMS ML 0.4 and Hor GRF late dyn mirror no change in risk (1.000). See Outcome Measures section for definitions.
Discussion
Our main finding was that following a single-legged drop-jump landing, 2 outcome measures were related to the occurrence of an ankle sprain among male elite soccer players within 3 years: RMS ML 0.4 (mediolateral stability for the first 0.4 seconds; a larger value indicates more force exerted in the mediolateral direction, resulting in rapid lateral stabilization) and Hor GRF late dyn (horizontal GRF between 3.0 and 5.0 seconds; a smaller value indicates less sway in the stabilization phase). A secondary finding is that, for only those sprains that prohibited participation for >7 days, the corresponding significance and hazard ratios of these outcome measures further increased.
Risk Factors
The few prospective studies that addressed risk factors for ankle sprains among soccer players reported that previous acute ankle injury and previous ankle sprain were significant predictors.7,20 In addition, a very recent study followed 133 male youth soccer players (U11-U17), of which 12 players sustained an ankle sprain during 3 years of follow-up (9.0%). In this small sample, the authors found low hip extension strength to be associated with lateral ankle sprains.5 Additional indications for risk factors can be found in more descriptive studies. For instance, most ankle sprains occurred with contact (59%), during matches (66%, with nearly 50% of these observed during the last third of each half), and during the first 3 months of the season (44%).36 Furthermore, in a sample of videotaped foot and ankle injuries (52 contusions, 20 sprains, 4 fractures), the majority was caused by tackles involving lateral or medial forces that created corresponding eversion or inversion.14
The current study showed that a higher RMS ML 0.4 coincided with a smaller risk, while a higher Hor GRF late dyn coincided with a greater risk. The fact that RMS ML 0.4 was larger for those at decreased risk might suggest that these players deal with the perturbation of a drop-jump landing by immediately (in the first 0.4 seconds) correcting in the mediolateral direction. Moreover, the univariate analysis for severe ankle sprains showed that a larger peak force V was associated with a lower risk as well. These 2 findings possibly point toward an optimized jump-landing strategy, which rapidly copes with the perturbation/impact and reduces injury risk. However, it is impossible to determine how exactly the jump-landing strategy differs among players solely on the basis of GRF. Combining kinetics with kinematics and electromyography might provide further insight.
The impact phase is followed by the dynamic, late dynamic, and static phases.11 Recent research showed that Hor GRF late dyn is related to static balance performance (Huurnink et al, unpublished data, 2018), and a meta-analysis revealed that participants (from varying sports and competitive levels) who injured their ankles had worse static balance performance.34 The early phase (Hor GRF dyn, 0.4-2.3 seconds) showed no predictive value, possibly because of the limited reliability of Hor GRF dyn when compared with Hor GRF late dyn (Huurnink et al, unpublished data, 2018).
To our knowledge, no previous studies targeted static balance and injury risk among soccer players. However, dynamic balance (eg, center of pressure measures) is impaired among young elite soccer players after a match.28 Since most ankle sprains during a match occur within the last 15 minutes of each half,36 this could be related to the current finding that an increase in Hor GRF late dyn is related to a higher risk of ankle sprains. Therefore, it would be interesting to perform the drop-jump landing test during halftime or directly after a match to confirm this possible association.
Note that in the subgroup of severe sprains (n = 32), all associations between risk factors and ankle sprains showed lower P values as compared with the entire group of ankle sprains (n = 45). It was previously shown that sprains were less severe when the injury mechanism involved contact with another player.20 The notion that noncontact trauma leads to more severe injuries perhaps explains that intrinsic risk factors are more significantly associated with severe ankle injuries than with all ankle injuries.
Injury Prevention
Prevention programs can either consist of a general protocol for the entire team or specifically target individuals at risk. To validate such a screening test, one would need to reproduce the current findings in relevant populations and develop an intervention program targeting athletes identified as high risk that is more beneficial than the same intervention program given to all athletes.1
However, one could also use findings from studies like the current one to try to understand why certain injury prevention programs work, such as the FIFA 11+.31 The more consistently this program was utilized, the greater the injury prevention benefit imparted to the athlete.29 Isolating underlying explanations is challenging; the program comprises lower limb muscular strength training (eg, Nordic hamstring exercises, plyometric jumping), balance training (eg, wobble board, balance exercises), and flexibility training (ie, functional dynamic stretching exercises).30 Therefore, one could hypothesize that the beneficial effect of the FIFA 11+ program on the occurrence of ankle sprains is partly due to improvement of balance (RMS ML 0.4 and Hor GRF late dyn, the current study) and to an increase in muscular strength and core stability (hip extension strength).5 In line with this, 1 study proved the effect of balance training on the recurrence of ankle sprains among male soccer players. The protocol consisted of daily exercises (20 minutes) on a wobble board and proved to be effective in reducing the recurrence rate of ankle sprains.25 It would be interesting to assess to what extent the aforementioned exercises improve the risk factors identified in the present study (RMS ML 0.4 and Hor GRF late dyn).
Limitations
It is likely that the multifactorial and complex nature of sports injuries arises not from the linear combination of isolated and predictive factors but from their interaction.3 However, to improve prediction capability1 and to understand injury mechanisms, the identification of possible risk factors is necessary.
The current study involved a limited number of repetitions of the test, chosen to limit the burden on players and coaches. Future studies might increase the number of repetitions to achieve better reliability. However, the testing protocol should remain feasible from a practical perspective. Furthermore, the study had a relatively long follow-up with regard to the initial testing moment. The predictive value of a performance test may decay over the follow-up period; hence, incorporating multiple tests over time might improve accuracy.
While we used a simple and verifiable criterion for injury severity in a way that matters most to the players (time lost/return to play), we acknowledge that this may not directly reflect severity of the injury from a medical/diagnostic perspective. A larger study would be needed to verify the relation between these factors.
We did not include other injuries to the lower extremity between testing and the occurrence of an ankle sprain in our analysis. Experiencing, for instance, an hamstring injury or Osgood-Schlatter disease could have an effect on the occurrence of an ankle sprain.9 Thus, related injuries could be an effect modifier. However, this would affect the interpretation on the causal pathway, not the risk factor as such.
As indicated in the Methods, we assumed that prior injury risk effects, where relevant, would show up as balance impairments. Regrettably, even though participants were young, they had careers at other clubs. Medical records on prior injuries were therefore not sufficiently reliable and complete to verify this. Note that young players are likely to honestly forget or simply ignore prior injury when they are allowed to enter an elite soccer club. Therefore, a retrospective questionnaire would also provide insufficient information. Furthermore, the current study is unable to explore any relations between the performance on a single-legged drop-jump landing and a second ankle sprain, given a small sample size.
Although we used z scores to correct for age, anthropometric characteristics, such body height, weight, and growth spurt, might still influence injury susceptibility. We ran an additional analysis to check for a relation between height/weight and injury and found no significant effect. This shows that our z score–based age correction appropriately corrected for such effects, if any. Assessing an effect of growth spurt would require long-term anthropometric data, which could be a topic for follow-up research. Furthermore, differentiation between contact and noncontact injuries would perhaps provide more insight into the intrinsic risk factors of ankle sprains. Finally, the current sample consisted of only male soccer players. The increasing popularity and level of international women’s soccer require validation of the current findings for female players.
Conclusion
The current study showed that the root mean square of the GRF in the mediolateral direction during the first 0.4 seconds after landing (RMS ML 0.4) and the mean resultant horizontal GRF during the late dynamic phase (3.0-5.0 seconds; Hor GRF late dyn) following a single-legged drop-jump landing are related to the occurrence of a lateral ankle sprain among male elite soccer players within 3 years.
Supplementary Material
Acknowledgments
The authors gratefully acknowledge Jeroen Eken, Liza Hallebeek, Lotte Jagtman, and Larissa Bonsen for their assistance in the data acquisition.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
A Video Supplement for this article is available online.
References
- 1. Bahr R. Why screening tests to predict injury do not work—and probably never will . . . : a critical review. Br J Sports Med. 2016;50:776-780. [DOI] [PubMed] [Google Scholar]
- 2. Bahr R, Holme I. Risk factors for sports injuries—a methodological approach. Br J Sports Med. 2003;37:384-392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Bittencourt NFN, Meeuwisse WH, Mendonça LD, Nettel-Aguiree A, Ocarino JM, Fonseca ST. Complex systems approach for sports injuries: moving from risk factor identification to injury pattern recognition—narrative review and new concept. Br J Sports Med. 2016;50:1309-1314. [DOI] [PubMed] [Google Scholar]
- 4. Bizzini M, Impellizzeri FM, Dvorak J, et al. Physiological and performance responses to the “FIFA 11+” (part 1): is it an appropriate warm-up? J Sport Sci. 2013;31(13):1481-1490. [DOI] [PubMed] [Google Scholar]
- 5. de Ridder R, Witvrouw E, Dolphens M, Roosen P, van Ginckel A. Hip strength as an intrinsic risk factor for lateral ankle sprains in youth soccer players: a 3-season prospective study. Am J Sports Med. 2017;45(2):410-416. [DOI] [PubMed] [Google Scholar]
- 6. Ekstrand J. Keeping your top players on the pitch: the key to football medicine at a professional level. Br J Sports Med. 2013;47(12):723-724. [Google Scholar]
- 7. Engebretsen AH, Myklebust G, Holme I, Engebretsen L, Bahr R. Intrinsic risk factors for acute ankle injuries among male soccer players: a prospective cohort study. Scand J Med Sci Sports. 2010;20:403-410. [DOI] [PubMed] [Google Scholar]
- 8. FIFA. Big count, 2006: 270 million people active in football. http://www.fifa.com/mm/document/fifafacts/bcoffsurv/bigcount.statspackage_7024.pdf. Accessed August 10, 2017.
- 9. Finch CF, Cook J. Categorising sports injuries in epidemiological studies: the subsequent injury categorisation (SIC) model to address multiple, recurrent and exacerbation of injuries. Br J Sports Med. 2014;48:1276-1280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Finch CF, Marshall SW. Let us stop throwing out the baby with the bathwater: towards better analysis of longitudinal injury data. Br J Sports Med. 2016;50(12):712-715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Fransz DP, Huurnink A, de Boode VA, Kingma I, van Dieën JH. Time series of ground reaction forces following a single leg drop jump landing in elite youth soccer players consist of four distinct phases. Gait Posture. 2016;50:137-144. [DOI] [PubMed] [Google Scholar]
- 12. Fransz DP, Huurnink A, Kingma I, van Dieën JH. How does postural stability following a single leg drop jump landing task relate to postural stability during a single leg stance balance task? J Biomech. 2014;47:3248-3253. [DOI] [PubMed] [Google Scholar]
- 13. Fransz DP, Huurnink A, Kingma I, Verhagen EALM, van Dieën JH. A systematic review and meta-analysis of dynamic tests and related force plate parameters used to evaluate neuromusculoskeletal function in foot and ankle pathology. Clin Biomech (Bristol, Avon). 2013;28(6):591-601. [DOI] [PubMed] [Google Scholar]
- 14. Giza E, Fuller C, Junge A, Dvorak J. Mechanisms of foot and ankle injuries in soccer. Am J Sports Med. 2003;31(4):550-554. [DOI] [PubMed] [Google Scholar]
- 15. Gribble PA, Bleakley CM, Caulfield BM, et al. 2016 consensus statement of the International Ankle Consortium: prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med. 2016;50:1493-1495. [DOI] [PubMed] [Google Scholar]
- 16. Hegedus EJ, McDonough S, Bleakley C, et al. Physical performance tests predict injury in National Collegiate Athletic Association athletes: a three-season prospective cohort study. Br J Sports Med. 2016;50:1333-1337. [DOI] [PubMed] [Google Scholar]
- 17. Huurnink A, Fransz DP, de Boode VA, Kingma I, van Dieën JH. Age-matched z-scores for longitudinal monitoring of center of pressure speed in single-leg balance performance in elite male youth football players [published online July 26, 2018]. J Strength Cond Res. doi: 10.1519/JSC.0000000000002765 [DOI] [PubMed] [Google Scholar]
- 18. Huurnink A, Fransz DP, Kingma I, van Dieën JH. Comparison of a laboratory grade force platform with a Nintendo Wii Balance Board on measurement of postural control in single-leg stance balance tasks. J Biomech. 2013;46(7):1392-1395. [DOI] [PubMed] [Google Scholar]
- 19. Huurnink A, Fransz DP, Kingma I, Verhagen EALM, van Dieën JH. Postural stability and ankle sprain history in athletes compared to uninjured controls. Clin Biomech (Bristol, Avon). 2014;29:183-188. [DOI] [PubMed] [Google Scholar]
- 20. Kofotolis ND, Kellis E, Vlachopoulos SP. Ankle sprain injuries and risk factors in amateur soccer players during a 2-year period. Am J Sports Med. 2007;35(3):458-466. [DOI] [PubMed] [Google Scholar]
- 21. McGuine TA, Greene JJ, Best T, Leverson G. Balance as predictor of ankle injuries in high school basketball players. Clin J Sport Med. 2000;10(4):239-244. [DOI] [PubMed] [Google Scholar]
- 22. McKay GD, Goldie PA, Payne WR, Oakes BW. Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med. 2001;35:103-108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. McKeon PO, Hertel J. Systematic review of postural control and lateral ankle instability, part I: can deficits be detected with instrumental testing? J Athl Training. 2008;43(3):293-304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. McKinley P, Pedotti A. Motor strategies in landing from a jump: the role of skill in task execution. Exp Brain Res. 1992;90:427-440. [DOI] [PubMed] [Google Scholar]
- 25. Mohammadi F. Comparison of 3 preventive methods to reduce the recurrence of ankle inversion sprains in male soccer players. Am J Sports Med. 2007;35(6):922-926. [DOI] [PubMed] [Google Scholar]
- 26. Nelson AJ, Collins CL, Yard EE, Fields SK, Comstock RD. Ankle injuries among United States high school sports athletes, 2005-2006. J Athl Training. 2007;42(3):381-387. [PMC free article] [PubMed] [Google Scholar]
- 27. Pau M, Arippa F, Leban B, et al. Relationship between static and dynamic balance abilities in Italian professional and youth league soccer players. Phys Ther Sport. 2015;16:235-241. [DOI] [PubMed] [Google Scholar]
- 28. Pau M, Mereu F, Melis M, Leban B, Corona F, Ibba G. Dynamic balance is impaired after a match in young elite soccer players. Phys Ther Sport. 2016;22:11-15. [DOI] [PubMed] [Google Scholar]
- 29. Silvers-Granelli H, Mandelbaum B, Adeniji O, et al. Efficacy of the FIFA 11+ injury prevention program in the collegiate male soccer player. Am J Sports Med. 2015;43(11):2628-2637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Soomro N, Sanders R, Hackett D, et al. The efficacy of injury prevention programs in adolescents team sports: a meta-analysis. Am J Sports Med. 2015;44(9):2415-2424. [DOI] [PubMed] [Google Scholar]
- 31. Thorborg K, Krommes KK, Esteve E, Clausen MB, Bartels EM, Rathleff MS. Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: a systematic review and meta-analysis of the FIFA 11 and 11+ programmes. Br J Sports Med. 2017;51:562-571. [DOI] [PubMed] [Google Scholar]
- 32. Waldén M, Hägglund M, Ekstrand J. UEFA Champions League study: a prospective study of injuries in professional footbal during the 2001-2002 season. Br J Sports Med. 2005;39:542-546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Wikstrom EA, Tillman MD, Chmielewski TL, Cauraugh JH, Naugle KE, Borsa PA. Dynamic postural control but not mechanical stability differs among those with and without chronic ankle instability. Scand J Med Sci Sports. 2010;20:e137-e144. [DOI] [PubMed] [Google Scholar]
- 34. Witchalls J, Blanch P, Waddington G, Adams R. Intrinsic functional deficitis associated with increased risk of ankle injuries: a systematic review with meta-analysis. Br J Sports Med. 2012;46:515-523. [DOI] [PubMed] [Google Scholar]
- 35. Witchalls JB, Newman P, Waddington G, Adams R, Blanch P. Functional performance deficits associated with ligamentous instability at the ankle. J Sci Med Sport. 2013;16:89-93. [DOI] [PubMed] [Google Scholar]
- 36. Woods C, Hawkins R, Hulse M, Hodson A. The Football Association Medical Research Programme: an audit of injuries in professional football. An analysis of ankle sprains. Br J Sports Med. 2003;37:233-238. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.