

Abstract
Background:
Multiple sclerosis (MS) is an autoimmune disease associated with inflammation of the central nervous system in humans. This disease is the most common neurological disease, especially in young people. Various factors, including biological, genetic, and environmental factors, are effective on the prevalence of MS disease. This study intends to determine the relationship between geographical factors, and the prevalence of MS disease was performed.
Methods:
This ecological study was carried out on 2000 patients with diagnosis of MS during the years 2001–2014 in Isfahan province. All patients’ data including age, sex, marital status, year, and location of patients were extracted from the files. Arc geographic information systems version 10.3 software was used for geographical maps, and for statistical analysis of data, SPSS.16 software ANOVA tests, independent t-test, and Kruskal–Wallis were used.
Results:
Based on recorded cases of MS, the highest and lowest cumulative incidence of diseases was related to the city of Isfahan (75.92 in one hundred thousand) and Aran Bidgol (1.16 in one hundred thousand), respectively. A significant relationship was observed between the incidence and height above sea level (P = 0.001), the average annual rainfall (P = 0.001), and land use (P = 0.001). With increase in the height above sea level and the average annual precipitation, the incidence of disease decreased.
Conclusions:
MS disease incidence is high in Isfahan province. The distribution of the disease is not the same in the cities of this province, and some cities have a higher incidence. Furthermore, the incidence of the disease is influenced by geographical factors such as height above sea level, average annual rainfall, and land use. Therefore, it is recommended that relevant authorities by the implementation of screening programs in high-risk areas take action to identify and treat patients in the early stages.
Keywords: Geographic information systems, geographical factors, Isfahan, multiple sclerosis, prevalence
Introduction
Multiple sclerosis (MS) is the most common disease of the central nervous system that causes destruction of the myelin sheath of nerve cells and the most common cause of disability in adolescents and young adults.[1] From etiology, probably, the destruction of myelin tissue is due to nerve tissue sporadic attacks on the immune system that were caused by an abnormal immune response.[2] The process of disease is variable so that about 90% of patients that their disease have arisen before 40, shows the periods of gain to health and reappear and 10%–20% of them was progressive.[3] This disease is the most common neurological disorder in young adults, and depending on the geographic region, the incidence is between“5.3-47 per hundred thousand people.”[4]
According to the World Atlas of MS in 2008, the prevalence of the disease was estimated to be 30 and its incidence is 2.5 per hundred thousand people, in which Europe, Eastern Mediterranean, America, Southeast Asia, and Africa, respectively, accounted for the highest rates, and also, in a report published in 2013, America, Europe, and the West Pacific had the highest prevalence.[5,6] The highest prevalence of the disease is in the UK, with more than 85 thousand patients with MS.[7]
In the Seventh International Congress of MS, the number of patients in Iran was reported to be about 40 thousand, and in 2013, the prevalence of MS in the country is between 20 and 60 in one hundred thousand.[6,8] Among the provinces, a prevalence of 15–30 in one hundred thousand is accounted for the highest rate.[9] Although the cause of MS is unknown, some sources know the common role of genetic and immune system diseases effective in catching it.[10] Various factors including immune deficiency, genetic predisposition, infectious disease, mental stress, environmental factors, and geographic area can be involved in its creation.[11,12] Geographic and environmental factors such as sunlight and climatic zones have been effective in MS so that the prevalence of diseases in the tropics is low.[13,14] Distribution and publication of many diseases is related to geographical conditions, with natural obstacles, such as mountains and rivers, on the one hand, and the dependence of some pathogenic factors on climatic conditions, on the other hand, restricting some of the diseases to specific areas; therefore, geography and location are very important in the study of diseases.[15]
Geographic information system (GIS) is one of the most useful and important softwares in epidemiology, distribution, publication, and identification of the geographical areas and population groups at high risk of catching diseases.[16] In fact, the accumulation of patients at a particular location can be obtained using a GIS, and spatial analysis of diseases and its relationship to environmental factors can be studied in GIS by capabilities of this site.[15] As a result, in the provision of prevention services, health information and surveillance in places and times have paramount importance.[16]
By the high prevalence of MS in Isfahan Province[9] and the effect of geographical and environmental factors on the pathogenesis of the disease[12] as well as study on the relationship between geography and spatial analysis, MS disease was not observed in Isfahan province; the determination of incidence based on geographical conditions helps in identifying the relationship between geographic regions in the development of the disease. The aim of this study was to determine the incidence of MS and its relationship with geographical factors: climatic conditions, rainfall, and height above sea level and mapping of MS to the general awareness of the incidence of the disease in Isfahan province.
Methods
Participants
The present ecological study was performed in Isfahan province during the years 2001–2014. Isfahan province with an area of 107,029 km2 and occupying a 6.57% of the total area of the country is one of the largest and most important provinces in the central part of Iran. According to the latest population and housing census in the year 1985, the population of Isfahan was announced to be about 4 million and 560 thousand. During the mentioned years, 2000 patients were registered in Al-Zahra hospital and martyr Ayatollah Kashani Isfahan that are main centers in at treatment for MS patients and all patients refer to treatment centers, participated in the study. All patients that were identified during 2001–2014 years, They disease by a neurologist based on clinical and laboratory diagnosis was given, a resident of Isfahan province have met the inclusion criteria to study and were enrolled.
The required information was collected based on questionnaires from patients’ files and using a questionnaire that its validity and reliability was approved. MS patients for complete and continued treatment in specialized centers have treatment file. During a visit to these centers informed consent was obtained from patients to take action to collect data on the patient's file. In this questionnaire, required information including age, sex, marital status, place of residence of the disease, and so on were extracted.
Statistical analysis
To estimate the cumulative incidence in the population studied was calculated in the beginning of 2001, then, the number of patients in each area in the numerator and the denominator was the resident population in each region and by a coefficient of a hundred thousand people in the regions studied was calculated cumulative incidence. To determine the relationship between the incidence of MS in different sectors and environmental factors, including climate conditions and height above sea level, the rain from the chart means plot, scatter plot, and Kruskal–Wallis were used. Statistical analysis was performed using software SPSS Inc. Released 2007. SPSS for Windows, Version 16.0. Chicago, SPSS Inc. ESRI 2011. Map of climatic factors including state map, height above sea level, land use, and average annual rainfall was performed using the software ArcGIS Desktop: Release 10.3. Redlands, CA: Environmental Systems Research Institute.
Results
Based on the data of 2000 patients registered in the MS specialized centers in Isfahan, the mean age was 30.15 ± 9.7 and the median age was 29 ± 9.4 years. Female to male sex ratio was 3.53. About 69.2% of patients were married, 27.3% were unmarried, 2.6% were divorced, and 1% of their husbands were dead.
The highest cumulative incidence in the province Isfahan was related to Isfahan city with 75.92 in hundred thousand, and the least in the Aran Bidgol, with 1.16 in hundred thousands. There was a significant correlation between cumulative incidence and city of residence (P = 0.0001) [Figure 1].
Figure 1.

The incidence of multiple sclerosis in the cities of Esfahan province by using GIS during the years from 2001 to 2014
The highest cumulative incidence of disease based on the height above sea level of patients’ location was 900–1600 m (59.25 in hundreds of thousands), and the lowest related to altitudes above 3000 m (0.0001 in hundreds of thousands) shows that with the increasing height above sea level incidence rate increase that this relationship was statistically significant (P: 0.0001) [Figure 2]. Patients’ location study showed patients on the basis of land use show the highest incidence rate of 98.39 in residential areas with hundreds of thousands, and the least was mountainous areas with hundreds of thousands of 1.01, in that, the relationship was statistically significant (P = 0.0001) [Figure 3].
Figure 2.
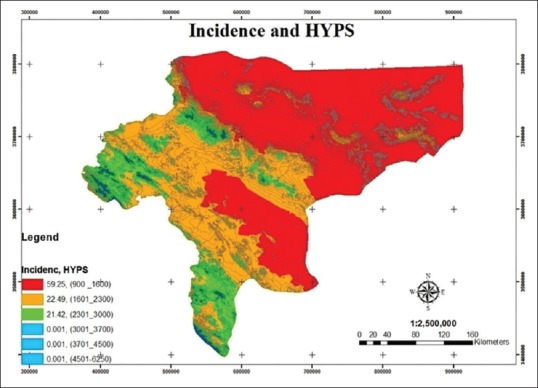
The incidence of multiple sclerosis based on the height above sea level in Esfahan province by using GIS during the years from 2001 to 2014
Figure 3.
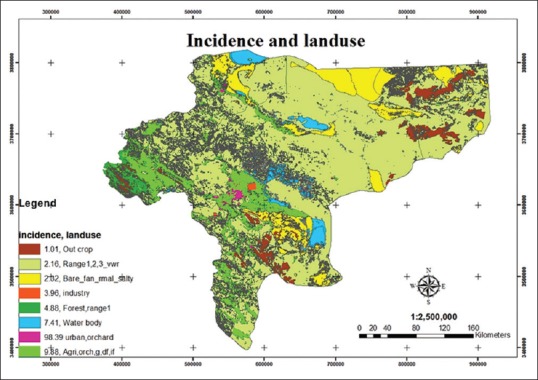
The incidence of multiple sclerosis disease-based land use in Isfahan province by using GIS during the years from 2001 to 2014
The findings showed that the average annual rainfall associated with the disease so that by increasing the average annual rainfall, the incidence of disease is decreased [Chart 1]. The highest incidence rate is based on the average annual rainfall in the region and occurs in regions with an average annual rainfall 0–100 mm (55.17 in hundreds of thousands) and lowest occurs in the region with an average annual rainfall of over 1000 mm (0.001 in hundreds of thousands); this relationship was statistically significant (P = 0.0001) [Figure 4].
Chart 1.
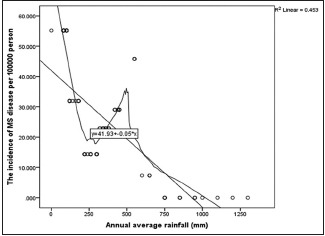
The relationship between the cumulative incidence of multiple sclerosis and the average annual rainfall in Isfahan province during the years from 2001 to 2014
Figure 4.

The incidence of multiple sclerosis based on the average annual rainfall in Isfahan province by using GIS during the years from 2001 to 2014
Discussion
The present study was performed on 2000 patients with MS registered in the specialized centers of Isfahan province to investigate the relationship between climate factors and the disease. In this study, the mean age of the patients was 30.15 ± 9.7 years – that of male patients is 31.7 ± 9.7 years and that of female patients is 29.72 ± 9.22 years. About 77.9% of the patients were women and 22.1% of the patients were men. Female to male sex ratio was 3.53. About 69.2% of patients were married, 27.3% were unmarried, 2.6% were divorced, and 1% of their husbands were dead. In the study of Izadi et al. in Fars Province in 2013, the mean age was 32/94 ± 9 years; in men, it was 33.24 ± 8.9 years, and in women, it was 32.86 ± 9.5 years. Women were 80.2% and men were 19.8% and female to male ratio was 4.04.[17] In Saei et al.'s study in Tehran in 2012, 75.99% of patients were women and 24.1% of them were men. The highest prevalence had occurred among married couples (57.22%),[18] which is consistent with our results. In the study of Balbuena et al. in the UK, the average age of patients with MS in men was 52.95 ± 19.94 and in women was 50.47 ± 18.32 years. The proportion of female to male gender was equal to 1.86.[19] Based on the results of studies, MS disease occurs more in young people and the average age of patients is far lower than developed countries.
The highest cumulative incidence was in the province of Isfahan and the lowest was in Bidgol Aran. In the study of Raiesi et al. in the Chaharmahal and Bakhtiari province in 2011, most cases of disease were related to Shahrekord and the lowest belonged to the Koohrang. Cumulative distribution of disease focused more in East and North-East of the Province.[20] In the study of Saei et al., the incidence of MS based on 22 areas of Tehran, the cumulative incidence of the disease in the north of Tehran (101.73 in one hundred thousand) far more than the south (53.79 in one hundred thousand), respectively. The highest incidence was in Region 2 and Region 6 and the lowest was in Region 17 and Region 19.[18]
The findings of our study showed the highest incidence of the disease based on the average annual precipitation were related to the region by 0–100 mm with and the lowest in the region with average rainfall of over 1000 mm. So that by increasing the average annual rainfall, the incidence of disease decreased. In relation to altitude, the highest incidence was related to altitudes 900–1600 m and the lowest incidence was related to altitude above 3000 m. Also according to land use in residential areas, the highest and lowest incidence belonged to the mountain areas. In the study of Pugliatti et al. that examines the MS disease incidence rate in 30 years in Europe, the incidence rate in Northern Europe was far more than other regions.[21] In a study of Fromont et al. in France Incidence rate in the North and North East of France was top and in South-West France has a low incidence.[22] In a study by Vukusic et al. in French on farmers, the disease rate in North East France is much higher than farmers in the South West. MS disease in farmers had a high prevalence.[23] In the study of Balbuena et al. in England, Wales, there is relation between height above sea level, length of coastline, light exposure time, and disease so that by increasing the hours of sunlight and the length of coastline, the incidence is decreased.[19] The results of these studies indicated a relationship between geographic and climatic conditions and the prevalence of the disease and by change in the status of these factors diseases will change. Although other factors such as lack of vitamin D,[24] nutrition, lifestyle, infectious diseases (Epstein–Barr virus), stress, exposure to soil and water pollution,[25] and cigarettes, genetic factors[26] are also effective in diseases. To compare the results of this study, similar studies that examine the relationship between these factors and the prevalence of the disease was not observed. But the increase in rainfall and increase in height above sea level can decrease exposure to related factors with MS-like disease, air pollution, soil etc., and vice versa in residential areas with concentration of population and pollution agents’ environment such as infectious diseases, smoking and stress can increase the risk of this disease.
Although the sample size in this study is relatively large, it has a few limitations. The study is ecological and it is not possible to assess risk factors individually, patient information has not recorded in the medical records for research purposes and may be biased information, some cases lack the required information to evaluate patients’ proprietary factors and it is possible population in the years before diagnosis has fled the province.
Conclusions
MS is a disease that has a high incidence in the province. This amount was not distributed in different regions same and some areas are more at risk. The disease is influenced by geographical factors such as height above sea level, land use, and average annual rainfall. Therefore, it is suggested to carry out longitudinal studies at the individual level and to have a closer examination of these factors; also the relevant authorities concerned with the implementation of screening programs in high-risk areas should take action to identify and treat patients in the early stages.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Bradley W, Daroff R, Fenichel G, Jankovic J. Neurology in Clinical Practice. 4th ed. Vol. 3. New York: Butterworth & Heinemnn; 2004. pp. 4–9. [Google Scholar]
- 2.Frankel J. Neurological Rehabilitation. Vol. 2. Philadelphia: Rh Publications Service; 1995. pp. 17–26. [Google Scholar]
- 3.Ling ND, Selby MJ. Assessment of memory in multiple sclerosis patients using the memory assessment scale. Percept Mot Skills. 1998;86:987–98. doi: 10.2466/pms.1998.86.3.987. [DOI] [PubMed] [Google Scholar]
- 4.Rosati G. The prevalence of multiple sclerosis in the world: An update. Neurol Sci. 2001;22:117–39. doi: 10.1007/s100720170011. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. Atlas multiple sclerosis resources in the world. Switzerland: WHO: World Health Organization; 2008. p. 53. [Google Scholar]
- 6.Aarli JA, Abramsky O. Atlas of multiple sclerosis 2013: A growing global problem with widespread in equity. Am Acad Neurol. 2014;83:81–9. doi: 10.1212/WNL.0000000000000768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Vazirinejad R, Lilley J, Ward C. A health profile of adults with multiple sclerosis living in the community. Mult Scler. 2008;14:1099–105. doi: 10.1177/1352458508092264. [DOI] [PubMed] [Google Scholar]
- 8.Shahbeigi S. 7th International Congress of Multiple Sclerosis Tehran. Iran: Medial News; 2010. [Google Scholar]
- 9.Masoodi R, Mohammadi E, Nabavi M, Ahmadi F. The effect of Orem based self-care program on physical quality of life in multiple sclerosis patients. J Shahrekord Univ Med Sci. 2008;10:44–53. [Google Scholar]
- 10.Allen I. Aetiological hypothesis for multiple sclerosis: Evidence from human and experimental diseases. In: Matthews WB, editor. McAlpines Multiple Sclerosis. 2nd ed. New York: Churchill Livingstone; 1991. pp. 379–90. [Google Scholar]
- 11.Karimi A, Delpisheh A, Ashtari F, Sayehmiri K, Meamar R. The relationship between the amount of radiation, relative humidity, and temperature with the risk of multiple sclerosis in Isfahan Province, Iran, during the years 2001-2014. J Isfahan Med Sch. 2017;35:434–9. [Google Scholar]
- 12.Rezaei A, Panahi M. Descriptive cross sectional study of clinical manifestation and MRI finding in 60 multiple sclerosis patients. J Hamadan Univ Med Sci. 2005;12:38–45. [Google Scholar]
- 13.Ebers GC. Environmental factors and multiple sclerosis. Lancet Neurol. 2008;7:268–77. doi: 10.1016/S1474-4422(08)70042-5. [DOI] [PubMed] [Google Scholar]
- 14.Marrie RA. Environmental risk factors in multiple sclerosis aetiology. Lancet Neurol. 2004;3:709–18. doi: 10.1016/S1474-4422(04)00933-0. [DOI] [PubMed] [Google Scholar]
- 15.Masoumi Z, Mesgari MS. Vol. 3. Tehran, Iran: National Cartographic Center; 2006. Fitting a Model in Place-for Statistics on Skin Cancer Decision Support, Geomatics 85 National Cartographic Center; pp. 87–96. [Google Scholar]
- 16.Bastida AZ, Hernández Tellez M, Montes LB, Torres IM, Paniagua JJ, Martínez GM. Spatial and temporal distribution of tuberculosis in the State of Mexico, Mexico 2012. Sci World J. 2012;4:72–9. doi: 10.1100/2012/570278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Izadi S Md, Nikseresht AR Md, Poursadeghfard M Md, Borhanihaghighi A Md, Heydari ST., PhD Prevalence and incidence of multiple sclerosis in Fars province, Southern Iran. Iran J Med Sci. 2015;40:390–5. [PMC free article] [PubMed] [Google Scholar]
- 18.Saei M, Holakouie-Naieni K, Mostafavi E, Sahraian MA, Mahmoodi M, Mansournia MA, et al. Spatial analysis of multiple sclerosis disease in Tehran Metropolitan Zone, Iran, 2001-2012. Iran J Public Health. 2014;43:621–9. [PMC free article] [PubMed] [Google Scholar]
- 19.Balbuena LD, Middleton RM, Tuite-Dalton K, Pouliou T, Williams KE, Noble GJ, et al. Sunshine, sea, and season of birth: MS incidence in Wales. PLoS One. 2016;11:e0155181. doi: 10.1371/journal.pone.0155181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Raiesi R, Baiati A, Karami J, Sarkaregar-ardakani A, Katorani S, Ramezaninezhad P. Patial distribution of multiple sclerosis disease in Chaharmahal va Bakhtiari province in 20-year period. J Shahrekord Univ Med Sci. 2013;15:73–82. [Google Scholar]
- 21.Pugliatti M, Rosati G, Carton H, Riise T, Drulovic J, Vécsei L, et al. The epidemiology of multiple sclerosis in Europe. Eur J Neurol. 2006;13:700–22. doi: 10.1111/j.1468-1331.2006.01342.x. [DOI] [PubMed] [Google Scholar]
- 22.Fromont A, Binquet C, Sauleau EA, Fournel I, Bellisario A, Adnet J, et al. Geographic variations of multiple sclerosis in France. Brain. 2010;133:1889–99. doi: 10.1093/brain/awq134. [DOI] [PubMed] [Google Scholar]
- 23.Vukusic S, Bockstael VV, Gosselin S, Confavreux C. Regional variations in the prevalence of multiple sclerosis in French farmers. J Neurol Neurosurg Psychiatry. 2007;78:1–4. doi: 10.1136/jnnp.2006.101196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Summerday NM, Brown SJ, Allington DR, Rivey MP. Vitamin D and multiple sclerosis: Review of a possible association. J Pharm Pract. 2012;25:75–84. doi: 10.1177/0897190011421839. [DOI] [PubMed] [Google Scholar]
- 25.Pugliatti M. Vol. 5. The University of Bergen; 2007. Epidemiological Studies of Multiple Sclerosis in a Sardinian Population, Insular Italy: Cluster Studies and Health Status [Phd Thesis] pp. 88–96. [Google Scholar]
- 26.Wingerchuk DM. Environmental factors in multiple sclerosis: Epstein-Barr virus, vitamin D, and cigarette smoking. Mt Sinai J Med. 2011;78:221–30. doi: 10.1002/msj.20240. [DOI] [PubMed] [Google Scholar]