

Abstract
Background and purpose
Creativity in Parkinson's disease (PD) is strongly related to dopaminergic activity and medication. We hypothesized that patients with PD, including those who are in the pre‐diagnostic phase of PD, are prone to choose highly structured ‘conventional’ professional occupations and avoid highly creative ‘artistic’ occupations.
Methods
At baseline of the population‐based Rotterdam Study, we asked 12 147 individuals aged ≥45 years about their latest occupation and categorized occupations according to the RIASEC model. Participants underwent baseline and follow‐up (median 11 years) examinations for PD. We determined associations of artistic (versus any other occupation) and conventional (versus any other occupation) occupations with PD. Additionally, we pooled our results with a recently published case–control study (Radboud Study).
Results
At baseline, conventional occupations were common [n = 4356 (36%)], whereas artistic occupations were rare [n = 137 (1%)]. There were 217 patients with PD, including 91 with prevalent PD and 126 with incident PD. The risk of PD varied substantially across occupational categories (chi‐square, 14.61; P = 0.01). The penalized odds ratio (OR) of artistic occupations for PD was 0.19 [95% confidence interval (CI), 0.00–1.31; P = 0.11], whereas the OR of conventional occupations for PD was 1.23 (95% CI, 0.95–1.66; P = 0.10). The direction and magnitude of ORs were similar in cross‐sectional and longitudinal subsamples. Pooled ORs across the Rotterdam and Radboud Studies were 0.20 (95% CI, 0.08–0.52; P < 0.001) for artistic and 1.23 (95% CI, 0.92–1.67; P = 0.08) for conventional occupations.
Conclusions
The risk of PD varies substantially by choice of professional occupation. Our findings suggest that dopaminergic degeneration affects choice of occupation, which may start in the pre‐diagnostic phase of PD.
Keywords: Parkinson's disease, professional occupation, risk factors
Introduction
In patients with Parkinson's disease (PD), low levels of dopamine and cortical dopamine receptor availability are associated with a lack of novelty seeking 1, 2. Furthermore, patients with PD may show changes in personality following initiation of dopaminergic treatment, progressively displaying traits such as novelty seeking 3. Given the remarkable link between dopaminergic state and creative behavior, patients with PD may be most comfortable in more structured jobs that do not require optimal dopamine levels, possibly leading to an over‐representation in highly structured ‘conventional’ occupations. In turn, patients with PD may be under‐represented in ‘artistic’ occupations, which are strongly correlated with high‐creativity traits such as ‘openness to new experience’ 4.
As clinical PD is preceded by a pre‐diagnostic phase during which dopaminergic degeneration leads to subtle cognitive and behavioral changes 5, 6, a distinct pattern of occupational preference may already be present in pre‐diagnostic patients with PD. Recent work from Radboud University Medical Center in Nijmegen (Radboud Study) showed that the distribution of occupational categories varied between patients with PD during their pre‐diagnostic phase and asymptomatic controls; most notably, patients with PD had a reduced prevalence of artistic occupations in late life prior to their PD diagnosis 7.
Here, we assessed the associations of artistic and conventional occupations with PD in a population‐based cohort and pooled estimates from this study and the recent Radboud Study to summarize all available evidence.
Methods
Study setting, population and design
The study was embedded in the population‐based Rotterdam Study 8, 9. A description of methods in the Rotterdam Study is provided in the next section. Furthermore, we pooled our results with a recently published case–control study (Radboud Study), which, unlike the Rotterdam Study, was a clinic‐based, case–control study 7. We note that there was a complementary element across both studies, each with their own strengths and weaknesses: one comprised a prospectively followed sample (no recall bias, but a low number of cases of PD) and the other comprised a retrospective case–control study (which may be affected by recall bias, but had a much larger number of cases of PD). A description of methods in the Radboud Study is provided at the end of the Methods.
Methods in the Rotterdam Study
The study was embedded in the Rotterdam Study, a prospective, population‐based study of individuals aged 45 years and older in the well‐defined Ommoord District in the city of Rotterdam comprising three subcohorts 8, 9. Baseline assessments of occupational status and prevalent parkinsonism or dementia took place in 1990 (first subcohort), 2000 (second subcohort) and 2006 (third subcohort), with a total study population of 14 926 individuals (overall response 72.0%) 8, 9. Follow‐up visits took place on average every 4 years and study follow‐up for incident parkinsonism was virtually complete (98%) 10 until 1 January 2015. For cross‐sectional analyses, in which the outcome was prevalent PD, we used data of participants who completed the baseline interview on occupational status and were screened for parkinsonism (n = 12 147). For longitudinal analyses, in which the outcome was incident PD, we excluded individuals with prevalent parkinsonism or dementia (n = 502).
During the interview on occupational status, participants who were still occupationally active were asked about their current occupation; retired or unemployed participants were asked about their last occupation. Subsequently, occupations were categorized according to the RIASEC model 11. Participants were also extensively screened for parkinsonism and dementia using several overlapping modalities, including serial in‐person examinations. The Rotterdam Study was approved by the medical ethics committee according to the Population Study Act Rotterdam Study, executed by the Ministry of Health, Welfare and Sports of the Netherlands. All participants provided written informed consent to participate in the study.
RIASEC model
To classify professional occupations, we used the RIASEC model, which is a previously validated method of classifying occupations into six categories linked to personality characteristics: realistic (R), investigative (I), artistic (A), social (S), enterprising (E) and conventional (C) 11. In Data S3, we present examples and characteristics of occupations in each category. The RIASEC model has previously been employed to assess occupational preference in Asperger's syndrome 12 and the association of occupational choice with brain hemisphere preference 13.
Although the influence of creativity on choice of professional occupation is probably not dichotomous, we focused on the two most contrasting RIASEC categories, i.e. ‘artistic’, which encompasses high creativity and novelty seeking, and ‘conventional’, which requires high levels of structure and routines. Occupational categories, based on professions reported by study participants at baseline, were assigned in 2016. The coder was blinded to participants’ prevalent or incident PD status.
Ascertainment of parkinsonism and Parkinson's disease
A detailed description of parkinsonism on PD assessment methods in the Rotterdam Study has been previously published 14. In short, we used four overlapping modalities to screen for potential parkinsonism: in‐person examinations, in‐person interviews, use of anti‐Parkinson medication and clinical monitoring alerts. In‐person examinations comprised two phases. In the first phase, participants underwent standardized assessments of the following Parkinsonian signs: tremor (resting, positional, intentional), hypokinesia and bradykinesia (including arm swing, gait, finger tapping, general impression), cogwheel rigidity and postural reflex. These screening assessments were conducted by research nurses who were repeatedly trained by an experienced neurologist (P.J.K.) during the study period. Individuals who screened positive were subsequently invited for a structured physical examination by a research physician who specialized in neurologic diseases.
For all individuals who screened positive in any of these methods, complete medical records (including letters from medical records of specialists and general practitioners) were studied and case reports were drawn up covering all potentially relevant information to establish the presence and cause of parkinsonism. These case reports were evaluated by a panel led by an experienced neurologist (P.J.K.). Parkinsonism was defined as at least one of: (i) the presence of hypokinesia or bradykinesia in combination with at least one other cardinal sign (resting tremor, rigidity or postural imbalance) as observed by any physician and (ii) a clinical diagnosis of parkinsonism by a neurologist or geriatrician (in the case that motor examination details were not available). PD was diagnosed after exclusion of parkinsonism associated with pre‐existent dementia, use of antidopaminergic drugs, cerebrovascular disease, multiple system atrophy, progressive supranuclear palsy and evidence of other rare causes (e.g. corticobasal degeneration). To diagnose PD, there also had to be at least one of: (i) a clinical PD diagnosis by a neurologist or geriatrician and (ii) positive response to dopaminergic treatment.
After initial diagnosis, medical records of all incident cases of parkinsonism (both PD and secondary) continued to be scrutinized until the end of the study period for new information that could lead to a revision of the diagnosis. Person‐time at risk of incident PD ended at the first of the following: diagnosis of incident parkinsonism (due to either PD or other causes), incident dementia, death or 1 January 2015.
Methods in the Radboud Study
A detailed description of methods used in the Radboud Study has previously been published 7. In short, the Radboud Study was a case–control study of 693 male patients with PD (defined using UK Brain Bank Criteria 15) and 1183 male community‐dwelling controls. Participants were asked about their most recent and first‐ever occupation before parkinsonism onset. Similar to the Rotterdam Study, occupations were categorized according to the RIASEC model 11. We only used data on the most recent occupation for meta‐analyses of the Rotterdam and Radboud Studies, as first‐ever occupation was not obtained from Rotterdam Study participants.
Statistical analysis
We separately analyzed the associations of artistic (versus any other occupation) and conventional (versus any other occupation) occupations with PD. We used Firth's penalized logistic regression models to account for the presence of statistical separation in our models, with adjustment for age, sex, education, subcohort and time at risk of PD (in longitudinal analyses) 16, 17. This method helps to avoid overestimation of the difference in PD risk across occupational categories. We constructed penalized regression models for ever‐PD (i.e. prevalent or incident PD) to meta‐analyze cross‐sectional and longitudinal data, and pooled results with the Radboud Study using inverse‐variance weighting or, in case of statistical separation, Mantel–Haenszel's method 7.
In post hoc sensitivity analyses on the link between artistic occupations and PD, we repeated the main analysis after simulating that one or two randomly selected individuals with an artistic occupation in the Rotterdam Study would have had PD. We performed 1000 simulations for each scenario and calculated mean odds ratios (ORs) of these simulations in the Rotterdam Study as well as corresponding pooled ORs across the Rotterdam and Radboud Studies.
Results
Baseline characteristics of the study population are shown in Table 1. Conventional occupations were common [4356 (36%)], whereas artistic occupations were rare [n = 137 (1%)] in this population. A total of 65% of individuals with conventional occupations were women, compared with only 27% of individuals with artistic occupations (P < 0.001). Among those with artistic occupations, 49% were still employed at study enrolment, which was distinctly higher than the 29% of individuals with a conventional occupation who were still employed (P < 0.001). Of individuals with artistic or conventional occupations who were not professionally active at baseline, most had retired, whereas <3% were unemployed (Data S2). The most common artistic occupation was musician, whereas the most common conventional occupation was shop employee. The median duration of latest occupation, which was available in 2373 individuals, was 12 years for conventional and 31 years for artistic occupations.
Table 1.
Characteristics of study population by occupation
| Characteristic | R | I | A | S | E | C | Total | P‐value for A vs. C* |
|---|---|---|---|---|---|---|---|---|
| No. of individuals | 3679 | 293 | 137 | 1771 | 1911 | 4356 | 12147 | |
| Age (years) | 68 (15) | 62 (12) | 64 (13) | 62 (10) | 64 (12) | 64 (12) | 65 (13) | 0.98 |
| Female sex | 1776 (48) | 59 (20) | 37 (27) | 1411 (80) | 678 (35) | 2850 (65) | 6811 (56) | <0.001 |
| Intermediate or higher education | 740 (21) | 98 (71) | 46 (55) | 487 (44) | 612 (40) | 1403 (36) | 3386 (33) | 0.08 |
| Smoking at baseline | 549 (15) | 19 (6) | 14 (10) | 141 (8) | 230 (12) | 491 (11) | 1444 (12) | 0.38 |
| Employed at baseline | 731 (20) | 141 (48) | 67 (49) | 701 (40) | 685 (36) | 1182 (27) | 3507 (29) | <0.001 |
A, artistic; C, conventional; E, enterprising; I, investigative; R, realistic; S, social; %, percentage of individuals with complete characteristics data. Intermediate or higher education includes intermediate vocational education or higher general education, higher vocational education or university. *P‐values for difference between individuals with artistic versus conventional occupations. Comparisons on age and sex were adjusted for each other; comparisons on education, smoking and employment were adjusted for age and sex. Data are given as median (interquartile range) and n (%).
There were 123 patients with prevalent parkinsonism, of whom 91 had prevalent PD. A total of 32 patients with prevalent PD (35%) and 4324 controls (35%) had held a conventional occupation, whereas no patients with prevalent PD and 137 controls (1%) had an artistic occupation. During follow‐up, 266 individuals were diagnosed with incident parkinsonism, including 126 with incident PD. A total of 51 (41%) patients with incident PD had a conventional occupation compared with 4194 controls (36%). No patients with incident PD and 132 controls (1%) had an artistic occupation. The full distribution of occupational categories by ever‐PD status is presented in Data S1.
In combined cross‐sectional and longitudinal analyses, the risk of ever‐PD varied substantially across occupational categories (chi‐square, 14.61; P = 0.01). Individuals with conventional occupations had an OR of 1.26 for PD [95% confidence interval (CI), 0.95–1.66; P = 0.10], whereas individuals with artistic occupations had an OR of 0.19 for PD (95% CI, 0.00–1.31; P = 0.11). In sensitivity analyses, exclusion of patients with prevalent PD who were still employed at study enrolment (n = 19) had virtually no effect on ORs of conventional (OR, 1.32; 95% CI, 0.98–1.77; P = 0.06) or artistic (OR, 0.21; 95% CI, 0.00–1.48; P = 0.15) professions for PD. Additional adjustment of the main analyses for smoking and employment status did somewhat attenuate the ORs of conventional (OR, 1.19; 95% CI, 0.88–1.77; P = 0.26) and artistic (OR, 0.28; 95% CI, 0.00–2.00; P = 0.26) occupations for PD.
In the Radboud Study, the risk of PD also varied distinctly across occupational categories (chi‐square, 41.41; P < 0.001). Pooled ORs for PD across the Rotterdam and Radboud Studies were 1.23 (95% CI, 0.92–1.67; P = 0.08) for conventional and 0.20 (95% CI, 0.08–0.52; P < 0.001) for artistic occupations. Separate ORs for cross‐sectional analyses, longitudinal analyses and ORs of the Radboud Study are presented in Fig. 1.
Figure 1.
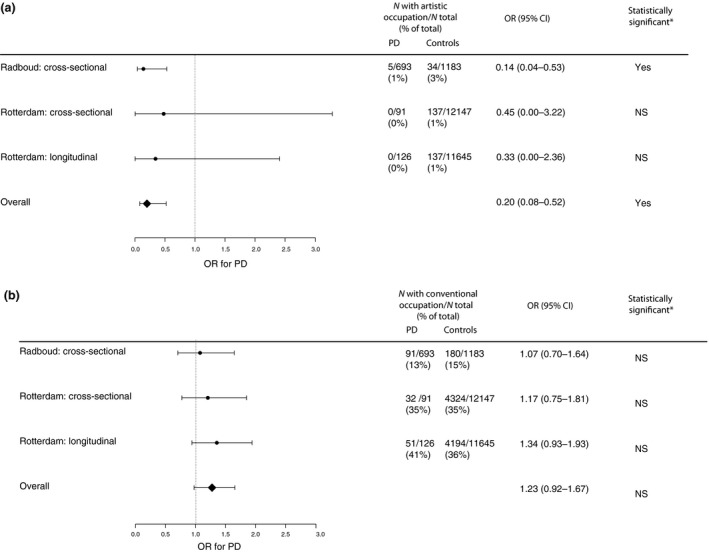
Odds ratios (ORs) of artistic and conventional occupations for Parkinson's disease (PD). (a) Artistic occupations. OR of artistic versus any other occupation for PD. (b) Conventional occupations. OR of conventional versus any other occupation for PD. CI, confidence interval; N, number; NS, not statistically significant. *Not statistically significant at α = 0.05. Analyses in the Rotterdam Study were adjusted for age, sex, education and study subcohort. Analyses in the male‐only Radboud Study were adjusted for age.
Although the protective effect of artistic occupation on risk of PD in the Rotterdam Study incrementally attenuated if one or two individuals with artistic occupation would have had PD, the overall association would have remained statistically robust in a pooled analysis of the Rotterdam and Radboud Studies (Table 2).
Table 2.
Sensitivity analyses: simulation of different Parkinson's disease (PD) distribution by artistic occupation
| N artistic individuals with PD | OR (95% CI) for PD in Rotterdam Study | OR (95% CI) for PD in pooled analysis |
|---|---|---|
| Observed | ||
| 0 | 0.19 (0.00–1.31) | 0.20 (0.08–0.52) |
| Simulated | ||
| 1 | 0.57 (0.06–2.11) | 0.28 (0.12–0.64) |
| 2 | 0.97 (0.20–2.83) | 0.34 (0.15–0.75) |
CI, confidence interval; N, number; OR, odds ratio.
Discussion
In this population‐based sample, choice of professional occupation in middle‐aged and older adults was associated with the risk of PD. This observation is in line with the recent Radboud Study 7. Taken together, these studies specifically show that individuals with highly creative artistic occupations have a reduced risk of PD, whereas individuals with highly structured conventional occupations may have an increased risk of PD, although this is not statistically significant.
As far as we know, farming is the only occupational group that has consistently been demonstrated to be associated with the risk of PD 18. In the current study, however, we used professional occupation as a proxy of personality. Individuals with artistic occupations have the most openness to new experiences, whereas those with conventional occupations have the least 4. In turn, dopamine levels and cortical D2 receptor availability are strongly associated with creativity in PD 1, 2, 3 and patients with PD who are being treated with dopaminergic medication can newly develop artistic expressions that they had not previously shown 4, 5, 6. Given the strong association between dopaminergic function and creative behavior in PD, we believe that the inverse association of artistic occupations with the risk of PD reflects a larger degree of dopaminergic degeneration in (pre‐diagnostic) patients with PD. Our study extends these findings by establishing an association between choice of professional occupation and the risk of PD.
We consider three alternative hypotheses that may explain our observations. First, the choice of professional occupation may be associated with addictive personality traits that predispose to substance use. For instance, individuals with artistic professions may have a higher prevalence of smoking, which may by itself affect (i.e. lower) the risk of PD 18. We note, however, that causality of the inverse association of addictive substances in general and of smoking in particular with the risk of PD remains highly contentious 19. Secondly, we cannot rule out that individuals with artistic occupations have a lower risk of PD because of non‐dopaminergic pathways, although we are unaware of consistent empirical evidence for a biological link of artistic or conventional occupations with serotonergic or noradrenergic pathways. Thirdly, high early‐life dopamine levels may increase the threshold for clinical parkinsonism to occur (higher dopamine reserve), even in the presence of PD pathology, similar to the observation that high education is associated with relative preservation of cognitive abilities in patients with PD with cortical β‐amyloid pathology 20.
The main strength of our study is its population‐based design, which ensures a representative sample of patients with PD and controls in the community. The main limitation of our study is the small number of participants with an artistic occupation (n = 137). Consequently, we were underpowered to restrict our analyses to patients with incident PD. Although the overall response figure of the study was high (72%) and ORs of the associations were similar in cross‐sectional and longitudinal subsamples, we cannot completely rule out that patients with PD with artistic occupations disproportionally more often changed their occupation due to onset of parkinsonism (or even due to subtle pre‐diagnostic motor features) than did patients with PD with other occupations. Also, although the association of artistic occupations with PD in our study is direction‐consistent and similar in magnitude to the recent Radboud Study 7, caution is warranted in interpreting the very low OR. Had a few more individuals with artistic occupations been diagnosed with PD in the Rotterdam Study, the association would have attenuated in the Rotterdam Study but would have remained robust in the pooled analysis.
In this study, the CI of the OR of conventional occupations for PD overlapped 1, even in the pooled analysis. This either suggests that there is no association between conventional occupations and PD or, alternatively, that this study was statistically insufficiently powered to detect a true association with a modest effect size that may be significant from a clinical perspective (i.e. OR ~1.2). To robustly determine whether there is an association between conventional occupations and PD, future studies with a larger sample size are warranted. Future studies should also focus on individuals with investigative occupations, which are characterized by traits that are often observed in patients with PD, such as precision, reason and independent work.
In conclusion, this population‐based study extends a recent case–control study and again suggests that the risk of PD varies substantially by choice of professional occupation in midlife. Although we interpret our findings cautiously, this converging evidence suggests that dopaminergic degeneration affects choice of occupation, which may start in the pre‐diagnostic phase of PD. Further large studies are warranted to robustly quantify the effect size of the associations of artistic and conventional occupations with incident PD.
Disclosure of conflicts of interest
The authors declare no financial or other conflicts of interest.
Supporting information
Data S1. Full distribution of occupational categories by Parkinson's disease status in the Rotterdam and Radboud Studies.
Data S2. Detailed employment status of individuals with artistic or conventional occupations in the Rotterdam Study.
Data S3. Examples and characteristics of occupations in each RIASEC category.
Acknowledgements
The contribution of the inhabitants, general practitioners and pharmacists of the Ommoord district to the Rotterdam Study is gratefully acknowledged. The authors also thank Dimitri van der Linden for his contribution to the Radboud Study. The Rotterdam Study is supported by the Erasmus MC University Medical Center and Erasmus University Rotterdam, the Netherlands Organization for Scientific Research (NWO), the Netherlands Organization for Health Research and Development (ZonMW), the Research Institute for Diseases in the Elderly (RIDE), the Ministry of Education, Culture and Science, the Ministry of Health, Welfare and Sport, The European Commission (DGXII), the Netherlands Genomics Initiative (NGI) and the Municipality of Rotterdam. The funders had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication. The authors have not been paid to write this article by a pharmaceutical company or other agency. S.K.L.D. takes full responsibility for the data, the analyses and interpretation, and the conduct of the research; had full access to all of the data; and has the right to publish any and all data separate and apart from any sponsor. M.A.I. had final responsibility for the decision to submit for publication.
References
- 1. Acosta LM. Creativity and neurological disease. Curr Neurol Neurosci Rep 2014; 14: 464. [DOI] [PubMed] [Google Scholar]
- 2. Inzelberg R. The awakening of artistic creativity and Parkinson's disease. Behav Neurosci 2013; 127: 256–261. [DOI] [PubMed] [Google Scholar]
- 3. Santangelo G, Garramone F, Baiano C, et al Personality and Parkinson's disease: a meta‐analysis. Parkinsonism Relat Disord 2018; 49: 67–74. [DOI] [PubMed] [Google Scholar]
- 4. Costa PT, Mccrae RR, Holland JL. Personality and vocational interests in an adult sample. J Appl Psychol 1984; 69: 390–400. [Google Scholar]
- 5. Noyce AJ, Lees AJ, Schrag AE. The prediagnostic phase of Parkinson's disease. J Neurol Neurosurg Psychiatry 2016; 87: 871–878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Darweesh SK, Verlinden VJ, Stricker BH, Hofman A, Koudstaal PJ, Ikram MA. Trajectories of prediagnostic functioning in Parkinson's disease. Brain 2017; 140: 429–441. [DOI] [PubMed] [Google Scholar]
- 7. Haaxma CA, Borm GF, van der Linden D, Kappelle AC, Bloem BR. Artistic occupations are associated with a reduced risk of Parkinson's disease. J Neurol 2015; 262: 2171–2176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Hofman A, Grobbee DE, de Jong PT, van den Ouweland FA. Determinants of disease and disability in the elderly: The Rotterdam Elderly Study. Eur J Epidemiol 1991; 7: 403–422. [DOI] [PubMed] [Google Scholar]
- 9. Hofman A, Brusselle GG, Darwish Murad S, et al The Rotterdam Study: 2016 objectives and design update. Eur J Epidemiol 2015; 30: 661–708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Clark TG, Altman DG, De Stavola BL. Quantification of the completeness of follow‐up. Lancet 2002; 359: 1309–1310. [DOI] [PubMed] [Google Scholar]
- 11. Holland JL. Making Vocational Choices: A Theory of Careers. Englewood Cliffs, NJ, USA: Prentice‐Hall, 1973. (Revised version: Holland JL. Making Vocational Choices: A Theory of Vocational Personalities and Work Environments, 3rd edn. Odessa, FL, USA: Psychological Assessment Resources, 1997.)
- 12. Lorenz T, Heinitz K. Aspergers – different, not less: occupational strengths and job interests of individuals with Asperger's Syndrome. PLoS ONE 2014; 9: e100358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Szirony GM, Pearson LC, Burgin JS, Murray GC, Elrod LM. Brain hemisphere dominance and vocational preference: a preliminary analysis. Work 2007; 29: 323–329. [PubMed] [Google Scholar]
- 14. Darweesh SK, Koudstaal PJ, Stricker BH, Hofman A, Ikram MA. Trends in the incidence of Parkinson Disease in the general population: The Rotterdam Study. Am J Epidemiol 2016; 183: 1018–1026. [DOI] [PubMed] [Google Scholar]
- 15. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico‐pathological study of 100 cases. J Neurol Neurosurg Psychiatry 1992; 55: 181–184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Firth D. Bias reduction of maximum‐likelihood‐estimates. Biometrika 1993; 80: 27–38. [Google Scholar]
- 17. Heinze G, Schemper M. A solution to the problem of separation in logistic regression. Stat Med 2002; 21: 2409–2419. [DOI] [PubMed] [Google Scholar]
- 18. Noyce AJ, Bestwick JP, Silveira‐Moriyama L, et al Meta‐analysis of early nonmotor features and risk factors for Parkinson disease. Ann Neurol 2012; 72: 893–901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hershey LA, Perlmutter JS. Smoking and Parkinson disease: where there is smoke there may not be fire. Neurology 2014; 83: 1392–1393. [DOI] [PubMed] [Google Scholar]
- 20. Lucero C, Campbell MC, Flores H, Maiti B, Perlmutter JS, Foster ER. Cognitive reserve and beta‐amyloid pathology in Parkinson disease. Parkinsonism Relat Disord 2015; 21: 899–904. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1. Full distribution of occupational categories by Parkinson's disease status in the Rotterdam and Radboud Studies.
Data S2. Detailed employment status of individuals with artistic or conventional occupations in the Rotterdam Study.
Data S3. Examples and characteristics of occupations in each RIASEC category.