

Abstract
Background
In view of the reported increase in obstetric anal sphincter injuries, the objective of this study was to evaluate the incidence of such injuries over time and the associated risk and protective factors.
Methods
This was a retrospective cohort study from a national database of 168 137 primiparous women with term, singleton, cephalic, vaginal delivery between 2008 and 2014. The main outcome measure was obstetric anal sphincter injury. A multivariate regression model was used to identify risk and protective factors.
Results
Age >19 years, birthweight >4000 g, and operative vaginal delivery were independent risk factors for obstetric anal sphincter injuries. Mediolateral episiotomy increased the risk for obstetric anal sphincter injuries in spontaneous vaginal birth (number needed to harm 333), whereas it was protective in vacuum delivery (number needed to treat 50). From 2008 to 2014, there was an increase in the rate of obstetric anal sphincter injuries (2.1% vs 3.1%, P < .01), vacuum deliveries (12.1% vs 12.8%, P < .01), and cesarean delivery after labor (17.1% vs 19.4%, P < .01), while forceps deliveries (0.4% vs 0.1%, P < .01) and episiotomy rate decreased (35.9% vs 26.4%, P < .01).
Conclusions
Episiotomy may be a risk or protective factor depending on the type of episiotomy and the clinical setting in which it is used. Our study supports a restrictive use of mediolateral episiotomy in spontaneous vaginal deliveries. In vacuum deliveries mediolateral episiotomy may help prevent obstetric anal sphincter injuries.
Keywords: episiotomy, obstetric anal sphincter injury, risk factors
1. INTRODUCTION
Obstetric anal sphincter injuries include third degree lacerations, which involve the external and/or internal anal sphincter muscle, and fourth degree lacerations, which in addition to the anal sphincter muscles also involve the rectal mucosa.1 These injuries are associated with potential long‐term complications such as persistent sphincter dysfunction with anal and fecal incontinence, prolapse and perineal pain, and sexual dysfunction.2, 3 Established risk factors for obstetric anal sphincter injuries include high birthweight, operative vaginal delivery, and prolonged second stage of labor.4, 5 Furthermore, risk factors such as episiotomy, epidural analgesia, induction of labor, and advanced maternal age have also been associated with obstetric anal sphincter injuries, but not consistently.6, 7 Several population‐based studies have reported a gradual increase in obstetric anal sphincter injuries in the last decades with an incidence ranging from 4.1% to 16.0%.7, 8, 9 The exact reason for this increase remains unclear. Changes in demographic risk factors such as the rise in maternal age, higher fetal birthweight, improvement of diagnostic attention, and better documentation through national birth registries explain only part of the substantial increase in obstetric anal sphincter injuries.8 Interestingly, in some countries, the use of forceps at delivery, although one of the major risk factors, has risen in the past years and may have contributed to this trend.8, 10
Using the population‐based database from the Austrian national birth registry, the aim of this study was to analyze risk and protective factors for obstetric anal sphincter injuries in first births in Austria and to describe time trends about the incidence of these injuries and associated risk factors in a country with a long‐standing tradition of restricted use of forceps at delivery.
2. METHODS
We performed a nationwide study using data from the national birth registry of Austria, a database containing obstetrical data from all 82 (public and private) obstetric departments in Austria. Data are retrieved by the Austrian birth registry quarterly to constantly control and ensure adequate data quality.
In the database, we identified all primiparous women over a period of 7 years (January 2008 until December 2014) who underwent vaginal delivery of a live, term (≥37.0 weeks), singleton infant with cephalic presentation. Exclusion criteria included noncephalic presentation, multiple pregnancies, preterm delivery, multiparity, and planned cesarean delivery.
To examine a possible association between age and the frequency of obstetric anal sphincter injuries, 4 age groups were classified: 19 or below, 20‐30, 31‐40, and >40 years. The dependent variable, obstetric anal sphincter injury, was classified as third degree and fourth degree lacerations according to Sultan.1 Independent variables included year of delivery (2008, 2009, 2010, 2011, 2012, 2013, 2014), maternal age in years (19 and younger, 20‐30, 31‐40, 40 or older), birthweight in grams (<3000, 3000‐4000, >4000), mode of delivery (spontaneous delivery without episiotomy, spontaneous delivery with episiotomy, forceps delivery without episiotomy, forceps delivery with episiotomy, vacuum‐assisted delivery without episiotomy, vacuum‐assisted delivery with episiotomy), body mass index (BMI; <30 kg/m2, >30 kg/m2), epidural anesthesia (yes or no), birth position/type (recumbent on bed, squatting, water birth).
Statistical software SPSS 18.0 for Mac (SPSS 18.0, SPSS Inc., Chicago, IL, USA) was used for statistical analysis. We performed the Kolmogorov‐Smirnov test to verify the use of tests for normally distributed variables. Values are given as mean (standard deviation [SD]) when normally distributed or as median (interquartile range [IQR]) at presence of skewed distribution. Chi‐square tests and Student t tests were used to compare subgroup of patients and P‐values with odds ratios (95% confidence interval) and P‐values with mean values (SD) are provided, respectively. A multivariate binary logistic regression model was performed to identify independent risk factors for obstetric anal sphincter injuries, using the backward selection with likelihood ratio test with the covariates age group (≤19 vs 20‐30, 31‐40, >40), birth position, birthweight, BMI <30, epidural anesthesia, mediolateral episiotomy, and forceps or vacuum‐assisted delivery. The goodness quality of fit of models was assessed, using the Hosmer and Lemeshow test. In case of unknown distribution Mann‐Whitney U tests are used. Statistical significance is defined as P < .01.
The study was approved by the institutional review board of the Medical University of Vienna (IRB number: 2082/2015). As this study comprises retrospectively collected and analyzed data, the institutional review board approved the waiver of informed consent.
3. RESULTS
Data included 222 494 primiparous women who had a term, singleton, cephalic delivery. Among these, 13 864 (6.2%) had a planned cesarean section, 40 366 (18.1%) had a cesarean section after onset of labor, and for 127 (0.06%) the birth mode was not stated. This left a total of 168 137 (75.6%) women with a successful vaginal delivery, who were included in the analysis.
The overall obstetric anal sphincter injury rate was 2.6%. The mean birthweight was 3350 g, the mean age was 28 years, and the mean gestational age (weeks) was 39.4. A total of 6.1% women presented with a BMI ≥ 30. Blood loss >1000 mL occurred more often in patients with obstetric anal sphincter injuries (5.8% vs 2.7%, P < .001). The overall rate of operative vaginal delivery was 16.0%, 15.7% were vacuum‐assisted deliveries, and 0.3% forceps deliveries. In total, 30.3% women received a mediolateral episiotomy during delivery. Mediolateral episiotomy was performed in 22.4% of spontaneous vaginal deliveries, in 71.9% of vacuum‐assisted deliveries, and in 91.5% of forceps deliveries. The episiotomy rate was 30.0% when birthweight was <4000 g and 39.7% when birthweight was >4000 g. There were no cases of midline episiotomy reported.
Between 2008 and 2014, there was an increase in the rate of cesarean delivery performed after onset of labor (17.1% vs 19.4%), vacuum‐assisted delivery (12.1% vs 12.8%), and obstetric anal sphincter injury (2.1% vs 3.1%), and a decrease in forceps‐assisted delivery (0.4% vs 0.1%) and mediolateral episiotomy (35.9% vs 26.4%; Figure 1).
Figure 1.
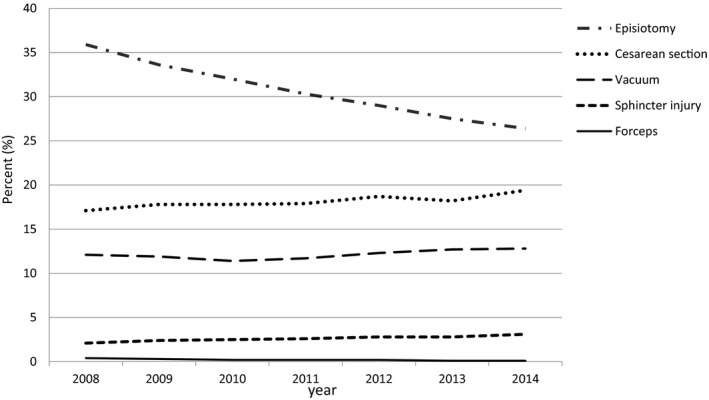
Trends in the rates of episiotomy, obstetric anal sphincter injury, cesarean delivery after labor, and forceps and vacuum‐assisted delivery, Austria, 2008‐2014
In univariate analysis, women with obstetric anal sphincter injuries were slightly older (28.7 years vs 28.0 years, P < .001) and had higher birthweight (3543 g vs 3344 g, P < .001). Women giving birth to a child of >4000 g sustained obstetric anal sphincter injuries in 6.1% of deliveries, compared with 2.4% when birthweight was below 4000 g (P < .001). Women who had forceps or vacuum‐assisted delivery were much more likely to have obstetric anal sphincter injuries compared with women giving birth spontaneously (9.9%, 5.1%, and 1.1%, P < .001, respectively). Furthermore, women who had a mediolateral episiotomy (3.3% vs 2.4%, P < .001), who had epidural anesthesia (3.2% vs 2.5%, P < .001), or had a BMI <30 (2.8% vs 2.4%, P = .04) were at higher risk for obstetric anal sphincter injuries compared with women without episiotomy, without epidural anesthesia, and with a BMI ≥30, respectively. Water births and squatting position were associated with a lower rate of sphincter injuries compared with giving birth in other positions (2.1%, 2.2%, and 2.7%, P < .001).
With respect to maternal age, the lowest rate of obstetric anal sphincter injuries, namely 1.1%, was seen in women who were 19 years or younger and this rate was significantly lower than in all other age groups (P < .001). Patients between 20 and 30 years, between 31 and 40 years, and older than 40 years were found to have an obstetric anal sphincter injury in 2.5%, 2.8%, and 2.5% of cases, respectively, which did not differ significantly.
In multivariate analysis, epidural analgesia, maternal BMI, and birth position were neither a risk nor a protective factor (Table 1). Age >19 years, birthweight >4000 g, and forceps or vacuum‐assisted delivery, were independently associated with increased risk for obstetric anal sphincter injuries (Table 1). Furthermore, mediolateral episiotomy significantly increased the risk for obstetric anal sphincter injuries with spontaneous vaginal delivery (OR 1.14 [CI 1.03‐126]), while it was protective with vacuum‐assisted vaginal delivery (OR 2.24 [CI 2.04‐2.47] vs OR 3.12 [CI 2.75‐3.55]). The protective effect of mediolateral episiotomy was not found with forceps‐assisted vaginal delivery (Table 1).
Table 1.
Rate of obstetric anal sphincter injury in singleton, term, cephalic, vaginal first births according to maternal and obstetric risk factors, Austria, 2008‐2014
| Variable | Prevalence of risk factor (%) | Rate of OASI per 100 births (%) | Crude OR (95% CI) | Adjusteda OR (95% CI) |
|---|---|---|---|---|
| Year of delivery | ||||
| 2008 | 2.1 | Reference | Reference | |
| 2009 | 2.4 | 1.14 (1.01‐1.29) | 1.01 (0.86‐1.19) | |
| 2010 | 2.5 | 1.16 (1.03‐1.31) | 1.14 (0.98‐1.33) | |
| 2011 | 2.6 | 1.23 (1.09‐1.38) | 1.12 (0.97‐1.31) | |
| 2012 | 2.8 | 1.34 (1.20‐1.51) | 1.24 (1.07‐1,45) | |
| 2013 | 2.8 | 1.30 (1.16‐1.43) | 1.16 (1.01‐1.34) | |
| 2014 | 3.1 | 1.49 (1.11‐1.67) | 1.37 (1.19‐1.57) | |
| Maternal age | ||||
| ≤19 | 2.4 | 1.1 | Reference | Reference |
| 20‐30 | 58.9 | 2.5 | 2.30 (1.71‐3.10) | 2.29 (1.57‐3.34) |
| 31‐40 | 36.8 | 2.9 | 2.64 (1.96‐3.56) | 2.54 (1.74‐3.71) |
| >40 | 1.8 | 2.5 | 2.24 (1.55‐3.26) | 1.95 (1.21‐3.15) |
| Birthweight | ||||
| <3000 | 20.4 | 1.2 | Reference | Reference |
| 3000‐4000 | 73.9 | 2.8 | 2.38 (2.14‐2.64) | 2.24 (1.98‐2.54) |
| >4000 | 5.6 | 6.1 | 5.43 (4.77‐6.17) | 5.05 (4.33‐5.89) |
| Mode of delivery | ||||
| Normal without episiotomy | 65.3 | 2.1 | Reference | Reference |
| Normal with episiotomy | 18.8 | 2.4 | 1.16 (1.06‐1.26) | 1.14 (1.03‐1.26) |
| Forceps without episiotomy | 0.1 | 12.5 | 6.76 (2.64‐17.23) | 6.04 (1.38‐26.42) |
| Forceps with episiotomy | 0.2 | 9.8 | 5.14 (3.73‐7.08) | 6.45 (4.53‐9.19) |
| Vacuum without episiotomy | 4.3 | 6.5 | 3.28 (2.96‐3.63) | 3.12 (2.75‐3.55) |
| Vacuum with episiotomy | 11.4 | 4.5 | 2.25 (2.07‐2.43) | 2.24 (2.04‐2.47) |
| BMI | ||||
| <30 | 93.9 | 2.8 | Reference | Reference |
| >30 | 6.1 | 2.4 | 0.85 (0.72‐0.99) | 0.79 (0.68‐1.18) |
| Epidural anesthesia | ||||
| No | 79.6 | 2.5 | Reference | Reference |
| Yes | 20.4 | 3.2 | 1.3 (1.22‐1.4) | 1.08 (0.99‐1.18) |
| Birth position/type | ||||
| Recumbent on bed | 89.7 | 2.7 | Reference | Reference |
| Water birth | 2.9 | 2.1 | 0.75 (0.62‐0.93) | 0.87 (0.64‐1.18) |
| Squatting | 4.1 | 2.2 | 0.82 (0.69‐0.97) | 0.89 (0.72‐1.1) |
| Other | 3.3 | 2.5 | 0.92 (0.77‐1.1) | 0.90 (0.66‐1.23) |
BMI, body mass index; CI, confidence interval; OASI, obstetric anal sphincter injury; OR, odds ratio.
Adjusted for: year of delivery, maternal age, birthweight, mode of delivery, BMI, epidural anesthesia, and birth position.
In vacuum‐assisted deliveries, the number needed to treat to prevent one case of obstetric anal sphincter injury with mediolateral episiotomy was found to be 50. The number needed to harm to produce one case of obstetric anal sphincter injury with mediolateral episiotomy during spontaneous vaginal delivery was found to be 333. If mediolateral episiotomy was performed in women with a child weighing >4000 g, the rate of obstetric anal sphincter injuries was 5.9% compared with 6.0% if no episiotomy was performed; the corresponding number needed to treat in these cases was found to be 1000.
4. DISCUSSION
This large population‐based study of the national birth registry of Austria outlines risk and protective factors associated with obstetric anal sphincter injuries. The overall incidence of obstetric anal sphincter injuries was 2.6%, which is low compared with other reports.8, 11 Similar to other European countries, there was an increase in the rate of obstetric anal sphincter injuries in primiparous women, from 2.1% in 2008 to 3.1% in 2014, which is possibly the result of improved awareness, diagnostic recognition, and documentation.12 In the same time period, the episiotomy rate decreased from 35.9% to 26.4%.
As supported by the literature, we found operative vaginal delivery7, 8, 13, 14, 15 to be an independent risk factor for sphincter damage. In particular, forceps delivery has consistently been shown to represent one of the major risk factors for obstetric anal sphincter injuries.16, 17, 18, 19 We found that the risk for obstetric anal sphincter injuries is increased by more than sixfold with the use of forceps delivery, with an incidence of 9.9%, and increased by more than twofold with the use of vacuum delivery (incidence 5.1%), respectively.
Episiotomy has previously been found to increase the risk for obstetric anal sphincter injuries.8, 20 However, looking at episiotomy as a single variable is insufficient and therefore we additionally analyzed the use of mediolateral episiotomy according to birth mode. Midline episiotomy has been abandoned in Austria because of the markedly increased risk of obstetric anal sphincter injuries, supported by several lines of evidence.21, 22, 23, 24 When it comes to mediolateral episiotomy, evidence is inconsistent as mediolateral episiotomy has previously been reported to be a risk,20 a protective,25, 26 or an insignificant factor.7, 27 We found that the use of mediolateral episiotomy increased the risk for obstetric anal sphincter injuries in spontaneous vaginal deliveries (number needed to harm 333), whereas it was protective in vacuum‐assisted deliveries. The number needed to treat to prevent one obstetric anal sphincter injury during vacuum‐assisted delivery was found to be 50. This finding is supported by previous studies, which reported a decrease in obstetric anal sphincter injuries when episiotomy was used in operative vaginal deliveries.8, 25, 28, 29 Jangö et al report a number needed to treat of 23 mediolateral episiotomies and Raisänen et al report a number needed to treat of 66 lateral episiotomies to prevent one case of obstetric anal sphincter injury in vacuum‐assisted deliveries, thus favoring more frequent use of episiotomy in such cases.28, 30 In forceps‐assisted vaginal delivery, we could not find a protective effect of mediolateral episiotomy. However, this must be interpreted carefully, since the number of patients who had forceps delivery without episiotomy was small (n = 40).
Other studies report a negative effect of a combined use of operative vaginal delivery and episiotomy, but solely with midline episiotomy.31, 32, 33 Kudish et al32 found a 20‐fold risk of anal sphincter injuries if a joint use of forceps and midline episiotomy was performed, and a 14‐fold increase in vacuum‐assisted delivery with midline episiotomy. Of prime consideration is the fact that in the published literature there is often a lack of description of the methodology of episiotomy, and a lack of proper identification of the incision actually made34; ie, in the practice of labeling an incision as mediolateral episiotomy there is in all probability a wide variation in the actual position and angle of the incision. However, this is of particular importance, since the type of episiotomy in use seems to influence the potentially protective effect.
Studies considering the question of whether maternal age is a risk factor for obstetric anal sphincter injuries yielded conflicting results.14, 35, 36 We found that the rate of obstetric anal sphincter injuries was significantly decreased in women of 19 years or younger, but subsequently remained stable in all age groups. Recent data from Sweden also demonstrated an age‐related risk of obstetric anal sphincter injuries starting at 25 years of age.37 Another population‐based study from the United States found a decreased risk of obstetric anal sphincter injuries in women 15‐19 years of age compared with women aged 20‐24 years.36 Our results likewise suggest a decreased risk of obstetric anal sphincter injuries only in very young women. The exact physiological effect of aging on the connective and muscular tissues in the perineal region is poorly researched. If these age‐related effects have an influence on lacerations during birth, then this risk seems to arise already at a relatively early age.
In line with most other reports, we found that high birthweight is a significant risk factor.7, 8, 13, 14, 15 Nevertheless, although the risk of obstetric anal sphincter injuries was 5 times higher when birthweight was >4000 g, the use of mediolateral episiotomy did not markedly reduce the risk, with a number needed to treat of 1000.
To be noted, in our study, epidural analgesia was neither protective nor a risk factor. This is supported by Loewenberg‐Weisband et al38 who also found that epidural analgesia is not associated with severe perineal lacerations, once confounding factors were controlled for. Other studies found a protective effect of epidural analgesia and therefore suggest epidural should not be considered an independent risk factor.28, 30
We further found that maternal BMI was an insignificant factor in the multivariate analysis. This is in accordance with recently published United Kingdom data, which report that higher BMI is protective for minor perineal trauma, but not for obstetric anal sphincter injuries.39 Other studies, however, suggest that higher BMI is protective for obstetric anal sphincter injuries.13, 40
Birth position did not influence the rate of obstetric anal sphincter injuries in our study. A Swedish study identified the lithotomy position to involve an increased risk of obstetric anal sphincter injuries, whilst a lateral position was protective.41 We were not able to identify a certain birth position to be a risk factor. However, it has to be noted that the lithotomy position is not a common position in Austria and that almost 90% in our cohort gave birth in a supine position, while in Sweden, the sitting position is the most common position to give birth.
Our study has several strengths including the population‐based design, resulting in a large sample size, and the prospective collection of data through the national birth registry. Limitations are the lack of data regarding other possible risk factors, including shoulder dystocia, gestational diabetes, duration of second‐stage labor, or information about perineal laceration protection techniques, or the experience of birth attendants, precluding further evaluation. Another limitation is that the majority of the study population is Caucasian and the percentage of obese patients was relatively low. This is representative for European countries, but may not be generalizable to other regions in the world.
In conclusion, we found that maternal age >19 years, birthweight >4000 g, and operative vaginal delivery are independent risk factors for obstetric anal sphincter injuries. Obstetricians should be aware that episiotomy may be a risk or protective factor depending on the type of episiotomy and the clinical setting in which it is used. Our study supports a restrictive use of mediolateral episiotomy in spontaneous vaginal deliveries. In vacuum deliveries, mediolateral episiotomy may help prevent obstetric anal sphincter injuries.
ACKNOWLEDGMENTS
The authors thank the Austrian Perinatal Registry for providing the data for this study and for their outstanding work in general.
Marschalek M‐L, Worda C, Kuessel L, et al. Risk and protective factors for obstetric anal sphincter injuries: A retrospective nationwide study. Birth. 2018;45:409‐415. 10.1111/birt.12346
REFERENCES
- 1. Sultan AH. Obstetric perineal injury and anal incontinence. Clin Risk. 1999;5:193‐196. [Google Scholar]
- 2. Vale de Castro Monteiro M, Pereira GM, Aguiar RA, Azevedo RL, Correia‐Junior MD, Reis ZS. Risk factors for severe obstetric perineal lacerations. Int Urogynecol J. 2016;27:61‐67. [DOI] [PubMed] [Google Scholar]
- 3. Fernando RJ, Sultan AH, Kettle C, Thakar R. Methods of repair for obstetric anal sphincter injury. Cochrane Database Syst Rev. 2013;(12):CD002866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Ott J, Gritsch E, Pils S, et al. A retrospective study on perineal lacerations in vaginal delivery and the individual performance of experienced midwives. BMC Pregnancy Childbirth. 2015;15:270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Low LK, Zielinski R, Tao Y, Galecki A, Brandon CJ, Miller JM. Predicting birth‐related levator ani tear severity in primiparous women: Evaluating Maternal Recovery from Labor and Delivery (EMRLD Study). Open J Obstet Gynecol. 2014;4:266‐278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Andrews V, Sultan AH, Thakar R, Jones PW. Risk factors for obstetric anal sphincter injury: a prospective study. Birth. 2006;33:117‐122. [DOI] [PubMed] [Google Scholar]
- 7. Baghestan E, Irgens LM, Bordahl PE, Rasmussen S. Trends in risk factors for obstetric anal sphincter injuries in Norway. Obstet Gynecol. 2010;116:25‐34. [DOI] [PubMed] [Google Scholar]
- 8. Gurol‐Urganci I, Cromwell DA, Edozien LC, et al. Third‐ and fourth‐degree perineal tears among primiparous women in England between 2000 and 2012: time trends and risk factors. BJOG. 2013;120:1516‐1525. [DOI] [PubMed] [Google Scholar]
- 9. Lowder JL, Burrows LJ, Krohn MA, Weber AM. Risk factors for primary and subsequent anal sphincter lacerations: a comparison of cohorts by parity and prior mode of delivery. Am J Obstet Gynecol. 2007;196:344.e1‐344.e5. [DOI] [PubMed] [Google Scholar]
- 10. Ampt AJ, Patterson JA, Roberts CL, Ford JB. Obstetric anal sphincter injury rates among primiparous women with different modes of vaginal delivery. Int J Gynaecol Obstet. 2015;131:260‐264. [DOI] [PubMed] [Google Scholar]
- 11. Meister MR, Cahill AG, Conner SN, Woolfolk CL, Lowder JL. Predicting obstetric anal sphincter injuries in a modern obstetric population. Am J Obstet Gynecol. 2016;215:310.e1‐310.e7. [DOI] [PubMed] [Google Scholar]
- 12. Andrews V, Sultan AH, Thakar R, Jones PW. Occult anal sphincter injuries—myth or reality? BJOG. 2006;113:195‐200. [DOI] [PubMed] [Google Scholar]
- 13. Blomberg M. Maternal body mass index and risk of obstetric anal sphincter injury. Biomed Res Int. 2014;2014:395803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Bowling CB, Wheeler Ii TL, Gerten KA, Chapman VR, Burgio KL, Richter HE. Sphincter tears in primiparous women: is age a factor? Int Urogynecol J Pelvic Floor Dysfunct. 2009;20:565‐569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Lagana AS, Terzic M, Dotlic J, et al. The role of episiotomy in prevention of genital lacerations during vaginal deliveries—results from two European centers. Ginekol Pol. 2015;86:168‐175. [DOI] [PubMed] [Google Scholar]
- 16. Kearney R, Miller JM, Ashton‐Miller JA, DeLancey JO. Obstetric factors associated with levator ani muscle injury after vaginal birth. Obstet Gynecol. 2006;107:144‐149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Combs CA, Robertson PA, Laros RK Jr. Risk factors for third‐degree and fourth‐degree perineal lacerations in forceps and vacuum deliveries. Am J Obstet Gynecol. 1990;163(1 Pt 1):100‐104. [DOI] [PubMed] [Google Scholar]
- 18. Hirayama F, Koyanagi A, Mori R, Zhang J, Souza JP, Gulmezoglu AM. Prevalence and risk factors for third‐ and fourth‐degree perineal lacerations during vaginal delivery: a multi‐country study. BJOG. 2012;119:340‐347. [DOI] [PubMed] [Google Scholar]
- 19. Caughey AB, Sandberg PL, Zlatnik MG, Thiet MP, Parer JT, Laros RK Jr. Forceps compared with vacuum: rates of neonatal and maternal morbidity. Obstet Gynecol. 2005;106(5 Pt 1):908‐912. [DOI] [PubMed] [Google Scholar]
- 20. Angioli R, Gomez‐Marin O, Cantuaria G, O'Sullivan MJ. Severe perineal lacerations during vaginal delivery: the University of Miami experience. Am J Obstet Gynecol. 2000;182:1083‐1085. [DOI] [PubMed] [Google Scholar]
- 21. Labrecque M, Baillargeon L, Dallaire M, Tremblay A, Pinault JJ, Gingras S. Association between median episiotomy and severe perineal lacerations in primiparous women. CMAJ. 1997;156:797‐802. [PMC free article] [PubMed] [Google Scholar]
- 22. Sagi‐Dain L, Sagi S. Morbidity associated with episiotomy in vacuum delivery: a systematic review and meta‐analysis. BJOG. 2015;122:1073‐1081. [DOI] [PubMed] [Google Scholar]
- 23. Bodner‐Adler B, Bodner K, Kaider A, et al. Risk factors for third‐degree perineal tears in vaginal delivery, with an analysis of episiotomy types. J Reprod Med. 2001;46:752‐756. [PubMed] [Google Scholar]
- 24. Coats PM, Chan KK, Wilkins M, Beard RJ. A comparison between midline and mediolateral episiotomies. Br J Obstet Gynaecol. 1980;87:408‐412. [DOI] [PubMed] [Google Scholar]
- 25. de Leeuw JW, de Wit C, Kuijken JP, Bruinse HW. Mediolateral episiotomy reduces the risk for anal sphincter injury during operative vaginal delivery. BJOG. 2008;115:104‐108. [DOI] [PubMed] [Google Scholar]
- 26. Handa VL, Danielsen BH, Gilbert WM. Obstetric anal sphincter lacerations. Obstet Gynecol. 2001;98:225‐230. [DOI] [PubMed] [Google Scholar]
- 27. Christianson LM, Bovbjerg VE, McDavitt EC, Hullfish KL. Risk factors for perineal injury during delivery. Am J Obstet Gynecol. 2003;189:255‐260. [DOI] [PubMed] [Google Scholar]
- 28. Jango H, Langhoff‐Roos J, Rosthoj S, Sakse A. Modifiable risk factors of obstetric anal sphincter injury in primiparous women: a population‐based cohort study. Am J Obstet Gynecol. 2014;210:59.e1‐59.e6. [DOI] [PubMed] [Google Scholar]
- 29. Bodner‐Adler B, Kimberger O, Kafer A, Husslein P, Bodner K. Management of the perineum during delivery with the Kiwi omnicup: effects of mediolateral episiotomy on anal sphincter tears in nulliparous women. Gynecol Obstet Invest. 2017; 10.1159/000478930. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 30. Raisanen SH, Vehvilainen‐Julkunen K, Gissler M, Heinonen S. Lateral episiotomy protects primiparous but not multiparous women from obstetric anal sphincter rupture. Acta Obstet Gynecol Scand. 2009;88:1365‐1372. [DOI] [PubMed] [Google Scholar]
- 31. Fitzgerald MP, Weber AM, Howden N, Cundiff GW, Brown MB, Pelvic Floor Disorders Network . Risk factors for anal sphincter tear during vaginal delivery. Obstet Gynecol. 2007;109:29‐34. [DOI] [PubMed] [Google Scholar]
- 32. Kudish B, Blackwell S, McNeeley SG, et al. Operative vaginal delivery and midline episiotomy: a bad combination for the perineum. Am J Obstet Gynecol. 2006;195:749‐754. [DOI] [PubMed] [Google Scholar]
- 33. Hudelist G, Gelle'n J, Singer C, et al. Factors predicting severe perineal trauma during childbirth: role of forceps delivery routinely combined with mediolateral episiotomy. Am J Obstet Gynecol. 2005;192:875‐881. [DOI] [PubMed] [Google Scholar]
- 34. Kalis V, Laine K, de Leeuw JW, Ismail KM, Tincello DG. Classification of episiotomy: towards a standardisation of terminology. BJOG. 2012;119:522‐526. [DOI] [PubMed] [Google Scholar]
- 35. Papamicheal E, Pillai R, Yoong W. Children having children: outcome of extreme teenage pregnancies (13‐15 years). Acta Obstet Gynecol Scand. 2009;88:1284‐1287. [DOI] [PubMed] [Google Scholar]
- 36. Torvie AJ, Callegari LS, Schiff MA, Debiec KE. Labor and delivery outcomes among young adolescents. Am J Obstet Gynecol. 2015;213:95.e1‐95.e8. [DOI] [PubMed] [Google Scholar]
- 37. Waldenstrom U, Ekeus C. Risk of obstetric anal sphincter injury increases with maternal age irrespective of parity: a population‐based register study. BMC Pregnancy Childbirth. 2017;17:306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Loewenberg‐Weisband Y, Grisaru‐Granovsky S, Ioscovich A, Samueloff A, Calderon‐Margalit R. Epidural analgesia and severe perineal tears: a literature review and large cohort study. J Matern Fetal Neonatal Med. 2014;27:1864‐1869. [DOI] [PubMed] [Google Scholar]
- 39. Durnea CM, Jaffery AE, Gauthaman N, Doumouchtsis SK. Effect of body mass index on the incidence of perineal trauma. Int J Gynaecol Obstet. 2017; 10.1002/ijgo.12403. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 40. Lindholm ES, Altman D. Risk of obstetric anal sphincter lacerations among obese women. BJOG. 2013;120:1110‐1115. [DOI] [PubMed] [Google Scholar]
- 41. Elvander C, Ahlberg M, Thies‐Lagergren L, Cnattingius S, Stephansson O. Birth position and obstetric anal sphincter injury: a population‐based study of 113 000 spontaneous births. BMC Pregnancy Childbirth. 2015;15:252. [DOI] [PMC free article] [PubMed] [Google Scholar]